

Migraine Disability Improvement during Treatment with Galcanezumab in Patients with Chronic and High Frequency Episodic Migraine
Abstract
1. Introduction
2. Methods
2.1. Standard Protocol Approvals and Patient Consents
2.2. Study Design and Participants
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders. Cephalalgia 2018, 38, 1–211. [Google Scholar]
- Burch, R.C.; Buse, D.C.; Lipton, R.B. Migraine: Epidemiology, Burden, and Comorbidity. Neurol. Clin. 2019, 37, 631–649. [Google Scholar] [CrossRef]
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Culpepper, W.J.; Dorsey, E.R.; Elbaz, A.; Ellenbogen, R.G.; et al. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [PubMed]
- Stovner, L.J.; Nichols, E.; Steiner, T.J.; Abd-Allah, F.; Abdelalim, A.; Al-Raddadi, R.M.; Ansha, M.G.; Barac, A.; Bensenor, I.; Doan, L.P.; et al. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 954–976. [Google Scholar] [CrossRef] [PubMed]
- Buse, D.C.; Scher, A.I.; Dodick, D.W.; Reed, M.L.; Fanning, K.M.; Adams, A.M.; Lipton, R.B. Impact of Migraine on the Family: Perspectives of People with Migraine and Their Spouse/Domestic Partner in the CaMEO Study. Mayo Clin. Proc. 2016, 91, 596–611. [Google Scholar] [CrossRef]
- Ashkenazi, A.; Mushtaq, A.; Yang, I.; Oshinsky, M. Ictal and Interictal Phonophobia in Migraine—A Quantitative Controlled Study. Cephalalgia 2009, 29, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Lovati, C.; D’Amico, D.; Bertora, P.; Rosa, S.D.S.R.F.; Suardelli, M.; Mailland, E.; Mariani, C.; Bussone, G. Acute and Interictal Allodynia in Patients With Different Headache Forms: An Italian Pilot Study. Headache 2007, 48, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Gossrau, G.; Frost, M.; Klimova, A.; Koch, T.; Sabatowski, R.; Mignot, C.; Haehner, A. Interictal osmophobia is associated with longer migraine disease duration. J. Headache Pain 2022, 23, 81. [Google Scholar] [CrossRef]
- Main, A.; Dowson, A.; Gross, M. Photophobia and phonophobia in migraineurs between attacks. Headache 1997, 37, 492–495. [Google Scholar] [CrossRef]
- Giffin, N.; Ruggiero, L.; Lipton, R.; Silberstein, S.; Tvedskov, J.F.; Olesen, J.; Altman, J.; Goadsby, P.; Macrae, A. Premonitory symptoms in migraine: An electronic diary study. Neurology 2003, 60, 935–940. [Google Scholar] [CrossRef]
- Blau, J.N. Resolution of migraine attacks: Sleep and the recovery phase. J. Neurol. Neurosurg. Psychiatry 1982, 45, 223–226. [Google Scholar] [CrossRef]
- Giffin, N.J.; Lipton, R.B.; Silberstein, S.D.; Olesen, J.; Goadsby, P.J. The migraine postdrome: An electronic diary study. Neurology 2016, 87, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Camarda, C.; Monastero, R.; Pipia, C.; Recca, D.; Camarda, R. Interictal Executive Dysfunction in Migraineurs Without Aura: Relationship with Duration and Intensity of Attacks. Cephalalgia 2007, 27, 1094–1100. [Google Scholar] [CrossRef] [PubMed]
- Meylakh, N.; Henderson, L.A. Exploring alterations in sensory pathways in migraine. J. Headache Pain 2022, 23, 5. [Google Scholar] [CrossRef]
- Filippi, V.; Steiger, R.; Beliveau, V.; Frank, F.; Kaltseis, K.; Gizewski, E.R.; Broessner, G. Investigating the Migraine Cycle over 21 Consecutive Days Using Proton Magnetic Resonance Spectroscopy and Resting-State fMRI: A Pilot Study. Brain Sci. 2022, 12, 646. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.F.; Lipton, R.B.; Kolodner, K.; Liberman, J.; Sawyer, J. Reliability of the Migraine Disability Assessment Score in A Population-Based Sample of Headache Sufferers. Cephalalgia 1999, 19, 107–114. [Google Scholar] [CrossRef]
- D’Amico, D.; Mosconi, P.; Genco, S.; Usai, S.; Prudenzano, A.; Grazzi, L.; Leone, M.; Puca, F.M.; Bussone, G. The Migraine Disability Assessment (MIDAS) Questionnaire: Translation and Reliability of the Italian Version. Cephalalgia 2001, 21, 947–952. [Google Scholar] [CrossRef]
- Stewart, W.F.; Lipton, R.B.; Kolodner, K.B.; Sawyer, J.; Lee, C.; Liberman, J.N. Validity of the Migraine Disability Assessment (MIDAS) score in comparison to a diary-based measure in a population sample of migraine sufferers. Pain 2000, 88, 41–52. [Google Scholar] [CrossRef]
- Kosinski, M.; Bayliss, M.S.; Bjorner, J.B.; Ware, J.E., Jr.; Garber, W.H.; Batenhorst, A.; Cady, R.; Dahlöf, C.G.H.; Dowson, A.; Tepper, S. A six-item short-form survey for measuring headache impact: The HIT-6™. Qual. Life Res. 2003, 12, 963–974. [Google Scholar] [CrossRef]
- Bayliss, M.S.; Batenhorst, A.S. The HIT-6™: A User’s Guide; QualityMetric Incorporated: Lincoln, RI, USA, 2002. [Google Scholar]
- Society, A.H. The American Headache Society Position Statement on Integrating New Migraine Treatments into Clinical Practice. Headache 2019, 59, 1–18. [Google Scholar] [CrossRef]
- Aurora, S.K.; Dodick, D.W.; Diener, H.; DeGryse, R.E.; Turkel, C.C.; Lipton, R.B.; Silberstein, S.D. OnabotulinumtoxinA for chronic migraine: Efficacy, safety, and tolerability in patients who received all five treatment cycles in the PREEMPT clinical program. Acta Neurol. Scand. 2014, 129, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Rosen, N.L.; Ailani, J.; DeGryse, R.E.; Gillard, P.J.; Varon, S.F. OnabotulinumtoxinA improves quality of life and reduces impact of chronic migraine over one year of treatment: Pooled results from the PREEMPT randomized clinical trial program. Cephalalgia 2016, 36, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Matharu, M.; Halker, R.; Pozo-Rosich, P.; DeGryse, R.; Adams, A.M.; Aurora, S.K. The impact of onabotulinumtoxinA on severe headache days: PREEMPT 56-week pooled analysis. J. Headache Pain 2017, 18, 78. [Google Scholar] [CrossRef] [PubMed]
- Blumenfeld, A.M.; Stark, R.J.; Freeman, M.C.; Orejudos, A.; Adams, A.M. Long-term study of the efficacy and safety of OnabotulinumtoxinA for the prevention of chronic migraine: COMPEL study. J. Headache Pain 2018, 19, 13. [Google Scholar] [CrossRef]
- Ashina, M.; Dodick, D.; Goadsby, P.J.; Reuter, U.; Silberstein, S.; Zhang, F.; Gage, J.R.; Cheng, S.; Mikol, D.D.; Lenz, R.A. Erenumab (AMG 334) in episodic migraine: Interim analysis of an ongoing open-label study. Neurology 2017, 89, 1237–1243. [Google Scholar] [CrossRef]
- Gaul, C.; Diener, H.-C.; Danesch, U.; on behalf of the Migravent® Study Group. Improvement of migraine symptoms with a proprietary supplement containing riboflavin, magnesium and Q10: A randomized, placebo-controlled, double-blind, multicenter trial. J. Headache Pain 2015, 16, 32. [Google Scholar] [CrossRef]
- Rendas-Baum, R.; Yang, M.; Varon, S.F.; Bloudek, L.M.; DeGryse, R.E.; Kosinski, M. Validation of the Headache Impact Test (HIT-6) in patients with chronic migraine. Health Qual. Life Outcomes 2014, 12, 117. [Google Scholar] [CrossRef]
- Houts, C.; Wirth, R.; McGinley, J.S.; Gwaltney, C.; Kassel, E.; Snapinn, S.; Cady, R. Content Validity of HIT-6 as a Measure of Headache Impact in People with Migraine: A Narrative Review. Headache 2020, 60, 28–39. [Google Scholar] [CrossRef]
- Russell, F.A.; King, R.; Smillie, S.-J.; Kodji, X.; Brain, S.D.; Pressly, J.D.; Soni, H.; Jiang, S.; Wei, J.; Liu, R.; et al. Calcitonin Gene-Related Peptide: Physiology and Pathophysiology. Physiol. Rev. 2014, 94, 1099–1142. [Google Scholar] [CrossRef]
- Goadsby, P.J.; Edvinsson, L. The trigeminovascular system and migraine: Studies characterizing cerebrovascular and neuropeptide changes seen in humans and cats. Ann. Neurol. 1993, 33, 48–56. [Google Scholar] [CrossRef]
- Edvinsson, L.; Ekman, R.; Goadsby, P.J. Measure-ment of vasoactive neuropeptides in biologicalmaterials: Problems and pitfalls from 30 years ofexperience and novel future approaches. Cephalalgia 2010, 30, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Hansen, J.M.; Hauge, A.W.; Olesen, J.; Ashina, M. Calcitonin gene-related peptide triggers migraine-like attacks in patients with migraine with aura. Cephalalgia 2010, 30, 1179–1186. [Google Scholar] [CrossRef]
- Benschop, R.J.; Collins, E.C.; Darling, R.J.; Allan, B.; Leung, D.; Conner, E.; Nelson, J.; Gaynor, B.; Xu, J.; Wang, X.-F.; et al. Development of a novel antibody to calcitonin gene-related peptide for the treatment of osteoarthritis-related pain. Osteoarthr. Cartil. 2014, 22, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Monteith, D.; Collins, E.C.; Vandermeulen, C.; Van Hecken, A.; Raddad, E.; Scherer, J.C.; Grayzel, D.; Schuetz, T.J.; De Hoon, J. Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of the CGRP Binding Monoclonal Antibody LY2951742 (Galcanezumab) in Healthy Volunteers. Front. Pharmacol. 2017, 8, 740. [Google Scholar] [CrossRef]
- Eli Lilly and Company. EMGALITY (galcanezumab-gnlm) Injection, for Subcutaneous Use: US Prescribing Information. 2018. Available online: http://pi.lilly.com/ (accessed on 11 October 2018).
- Kielbasa, W.; O’Brien, L.; Moser, B.; Quinlan, T. Assessment of pharmacokinetics, target engagement and immunogenicity in patients with migraine administered galcanezumab, an anti-CGRP antibody [abstract no. IOR09]. Headache 2018, 58 (Suppl. S2), 77–78. [Google Scholar]
- Vermeersch, S.; Benschop, R.J.; Van Hecken, A.; Monteith, D.; Wroblewski, V.J.; Grayzel, D.; de Hoon, J.; Collins, E.C. Translational Pharmacodynamics of Calcitonin Gene-Related Peptide Monoclonal Antibody LY2951742 in a Capsaicin-Induced Dermal Blood Flow Model. Experiment 2015, 354, 350–357. [Google Scholar] [CrossRef]
- Skljarevski, V.; Matharu, M.; Millen, B.A.; Ossipov, M.H.; Kim, B.-K.; Yang, J.Y. Efficacy and safety of galcanezumab for the prevention of episodic migraine: Results of the EVOLVE-2 Phase 3 randomized controlled clinical trial. Cephalalgia 2018, 38, 1442–1454. [Google Scholar] [CrossRef]
- Stauffer, V.L.; Dodick, D.W.; Zhang, Q.; Carter, J.N.; Ailani, J.; Conley, R.R. Evaluation of Galcanezumab for the Prevention of Episodic Migraine: The EVOLVE-1 Randomized Clinical Trial. JAMA Neurol. 2018, 75, 1080–1088, Erratum in: JAMA Neurol. 2019, 76, 872. [Google Scholar] [CrossRef]
- Detke, H.C.; Goadsby, P.J.; Wang, S.; Friedman, D.I.; Selzler, K.J.; Aurora, S.K. Galcanezumab in chronic migraine: The randomized, double-blind, placebo-controlled REGAIN study. Neurology 2018, 91, e2211–e2221. [Google Scholar] [CrossRef]
- Vernieri, F.; Altamura, C.; Brunelli, N.; Costa, C.M.; Aurilia, C.; Egeo, G.; Fofi, L.; Favoni, V.; Pierangeli, G.; Lovati, C.; et al. Galcanezumab for the prevention of high frequency episodic and chronic migraine in real life in Italy: A multicenter prospective cohort study (the GARLIT study). J. Headache Pain 2021, 22, 35. [Google Scholar] [CrossRef]
- Vernieri, F.; Altamura, C.; Brunelli, N.; Costa, C.M.; Aurilia, C.; Egeo, G.; Fofi, L.; Favoni, V.; Lovati, C.; Bertuzzo, D.; et al. Rapid response to galcanezumab and predictive factors in chronic migraine patients: A 3-month observational, longitudinal, cohort, multicenter, Italian real-life study. Eur. J. Neurol. 2022, 29, 1198–1208. [Google Scholar] [CrossRef]
- Martin, V.; Samaan, K.H.; Aurora, S.; Pearlman, E.M.; Zhou, C.; Li, X.; Pallay, R. Efficacy and Safety of Galcanezumab for the Preventive Treatment of Migraine: A Narrative Review. Adv. Ther. 2020, 37, 2034–2049. [Google Scholar] [CrossRef]
- Silvestro, M.; Tessitore, A.; Orologio, I.; De Micco, R.; Tartaglione, L.; Trojsi, F.; Tedeschi, G.; Russo, A. Galcanezumab effect on “whole pain burden” and multidimensional outcomes in migraine patients with previous unsuccessful treatments: A real-world experience. J. Headache Pain 2022, 23, 69. [Google Scholar] [CrossRef] [PubMed]
- Vernieri, F.; Altamura, C.; Aurilia, C.; Brunelli, N.; Egeo, G.; Fofi, L.; Costa, C.M.; Fallacara, A.; Favoni, V.; Pierangeli, G.; et al. Effectiveness, safety, and tolerability of galcanezumab in a real-life setting in patients with migraine in Italy (the GARLIT study). Neurol. Sci. 2020, 41, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Altamura, C.; Brunelli, N.; Marcosano, M.; Aurilia, C.; Egeo, G.; Lovati, C.; Favoni, V.; Perrotta, A.; Maestrini, I.; Schiano Di Cola, F.; et al. Conversion from chronic to episodic migraine in patients treated with galcanezumab in real life in Italy: The 12-month observational, longitudinal, cohort multicenter GARLIT experience. J. Neurol. 2022, 269, 5848–5857. [Google Scholar] [CrossRef] [PubMed]
- Vernieri, F.; Brunelli, N.; Marcosano, M.; Aurilia, C.; Egeo, G.; Lovati, C.; Favoni, V.; Perrotta, A.; Maestrini, I.; Rao, R.; et al. Maintenance of response and predictive factors of 1-year GalcanezumAb treatment in real-life migraine patients in Italy: The multicenter prospective cohort GARLIT study. Eur. J. Neurol. 2023, 30, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.F.; Lipton, R.B.; Dowson, A.J.; Sawyer, J. Development and testing of the Migraine Disability Assessment (MIDAS) Questionnaire to assess headache-related disability. Neurology 2001, 56 (Suppl. S1), S20–S28. [Google Scholar] [CrossRef]
- Ford, J.H.; Stauffer, V.L.; McAllister, P.; Akkala, S.; Sexson, M.; Ayer, D.W.; Wang, S. Functional impairment and disability among patients with migraine: Evaluation of galcanezumab in a long-term, open-label study. Qual. Life Res. 2021, 30, 455–464, Erratum in: Qual. Life Res. 2020. [Google Scholar] [CrossRef]
- Ayer, D.W.; Skljarevski, V.; Ford, J.H.; Nyhuis, A.W.; Lipton, R.B.; Aurora, S.K. Measures of Functioning in Patients With Episodic Migraine: Findings From a Double-Blind, Randomized, Placebo-Controlled Phase 2b Trial With Galcanezumab. Headache 2018, 58, 1225–1235. [Google Scholar] [CrossRef]
- Buse, D.C.; Bigal, M.; Rupnow, M.; Reed, M.; Serrano, D.; Lipton, R. Development and validation of the migraine Interictal burden scale (MIBS): A self-administered instrument for measuring the burden of migraine between attacks. Neurology 2007, 68, A89. [Google Scholar]
- Buse, D.C.; Rupnow, M.F.T.; Lipton, R.B. Assessing and managing all aspects of migraine: Migraine attacks, migraine-related functional impairment, common comorbidities, and quality of life. Mayo Clin. Proc. 2009, 84, 422–435. [Google Scholar] [CrossRef] [PubMed]
- Ailani, J.; Andrews, J.S.; Rettiganti, M.; Nicholson, R.A. Impact of galcanezumab on total pain burden: Findings from phase 3 randomized, double-blind, placebo-controlled studies in patients with episodic or chronic migraine (EVOLVE-1, EVOLVE-2, and REGAIN trials). J. Headache Pain 2020, 21, 123. [Google Scholar] [CrossRef] [PubMed]
- Ailani, J.; Andrews, J.S.; Tockhorn-Heidenreich, A.; Wenzel, R.; Rettiganti, M. Effect of Galcanezumab on Total Pain Burden in Patients Who Had Previously Not Benefited from Migraine Preventive Medication (CONQUER Trial): A Post Hoc Analysis. Adv. Ther. 2022, 39, 4544–4555. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 54) | HFEM (n = 17) | CM (n = 37) | p | |
|---|---|---|---|---|
| Age (years) mean, SD | 46.2 (9.5) | 47.2 (11.3) | 45.7 (8.6) | 0.1 # |
| Female, n (%) | 50 (92.5) | 15 (88.2) | 35 (93.5) | 0.9 § |
| Medication overuse, n (%) | 40 (74.1) | 7 (41.1) | 34 (91.8) | 0.0001 § |
| Disease duration (years) mean, SD | 30.1 (10.6) | 33.4 (10.6) | 28.4 (10.3) | 0.8 # |
| Allodynia, n (%) | 29 (53.7) | 9 (52.9) | 20 (54) | 1.0 § |
| Previous failed prophylaxis mean, SD | 4.4 (2.1) | 3.7 (2.3) | 4.8 (2) | 0.2 # |
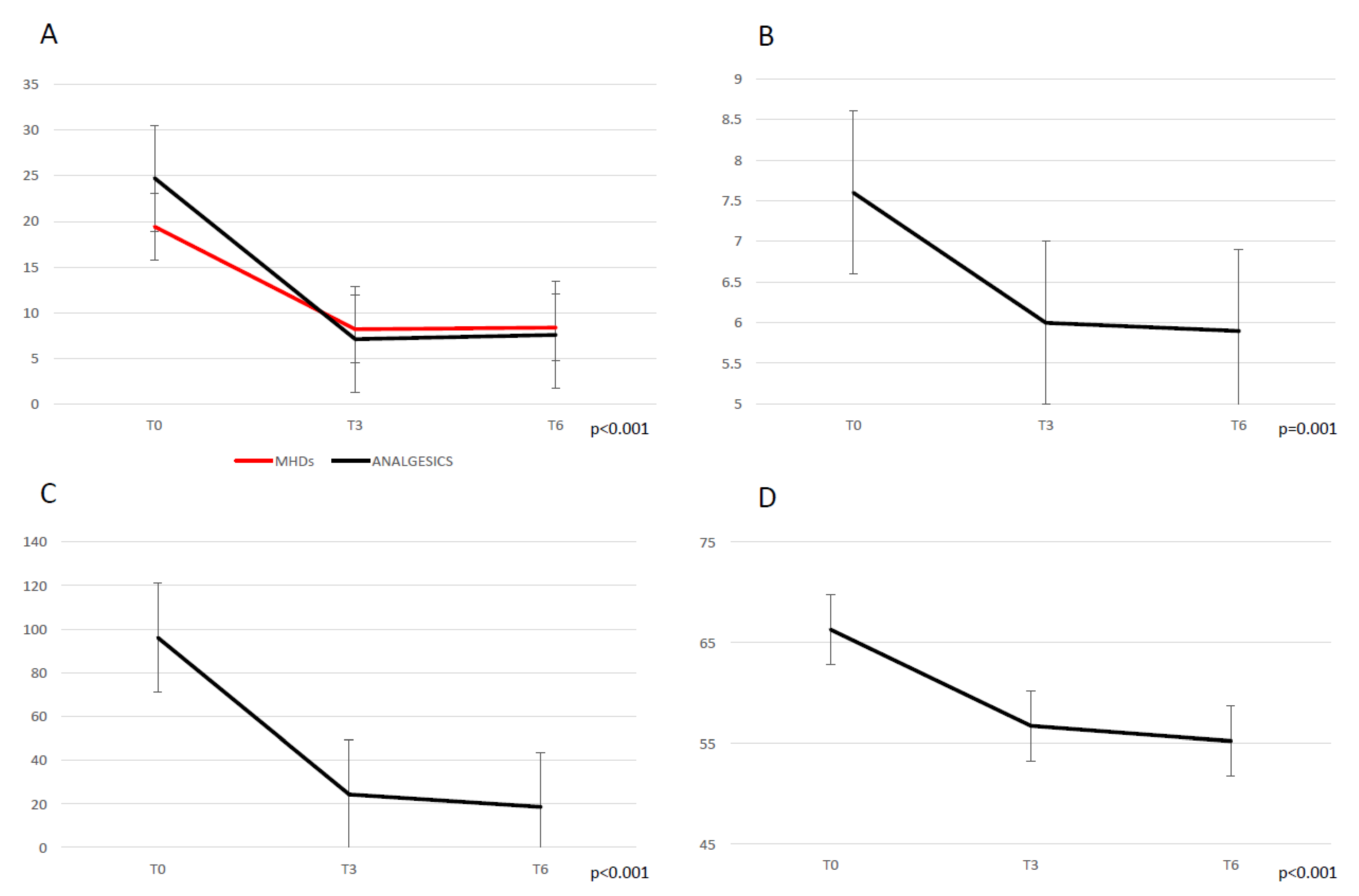
| MHDs T0 mean, SD | 19.4 (7.5) | 12.4 (5.3) | 22.8 (5.9) | 0.04 # |
| MMDs T0 Mean, SD | 11.2 (7.3) | 8.6 (3.1) | 12.1 (8.1) | 0.02 # |
| Monthly total analgesics consumption T0 mean, SD | 24.7 (14.7) | 13.2 (7.5) | 30.3 (28.4) | 0.02 # |
| - NSAIDs | 6.7 (12.1) | 4.2 (8.9) | 7.8 (13.5) | 0.3 # |
| - Triptans | 11.5 (8.9) | 8.9 (5.3) | 12.8 (8.1) | 0.03 # |
| - Combination | 6.5 (25.8) | 0 (0) | 9.6 (30.2) | 0.02 # |
| Pain intensity-NRS T0 mean, SD | 7.6 (1.1) | 7.6 (0.9) | 7.7 (1.2) | 0.7 # |
| MIDAS score T0 mean, SD | 96.1 (70.8) | 65 (38) | 111.1 (78.3) | 0.01 # |
| HIT-6 score T0 mean, SD | 66.3 (5.1) | 65.3 (3.7) | 66.8 (5.6) | 0.3 # |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
di Cola, F.S.; Bolchini, M.; Caratozzolo, S.; Ceccardi, G.; Cortinovis, M.; Liberini, P.; Rao, R.; Padovani, A. Migraine Disability Improvement during Treatment with Galcanezumab in Patients with Chronic and High Frequency Episodic Migraine. Neurol. Int. 2023, 15, 273-284. https://doi.org/10.3390/neurolint15010017
di Cola FS, Bolchini M, Caratozzolo S, Ceccardi G, Cortinovis M, Liberini P, Rao R, Padovani A. Migraine Disability Improvement during Treatment with Galcanezumab in Patients with Chronic and High Frequency Episodic Migraine. Neurology International. 2023; 15(1):273-284. https://doi.org/10.3390/neurolint15010017
Chicago/Turabian Styledi Cola, Francesca Schiano, Marco Bolchini, Salvatore Caratozzolo, Giulia Ceccardi, Matteo Cortinovis, Paolo Liberini, Renata Rao, and Alessandro Padovani. 2023. "Migraine Disability Improvement during Treatment with Galcanezumab in Patients with Chronic and High Frequency Episodic Migraine" Neurology International 15, no. 1: 273-284. https://doi.org/10.3390/neurolint15010017
APA Styledi Cola, F. S., Bolchini, M., Caratozzolo, S., Ceccardi, G., Cortinovis, M., Liberini, P., Rao, R., & Padovani, A. (2023). Migraine Disability Improvement during Treatment with Galcanezumab in Patients with Chronic and High Frequency Episodic Migraine. Neurology International, 15(1), 273-284. https://doi.org/10.3390/neurolint15010017