Detecting Incident Delirium within Routinely Collected Inpatient Rehabilitation Data: Validation of a Chart-Based Method

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source and Study Design
2.2. Study Population
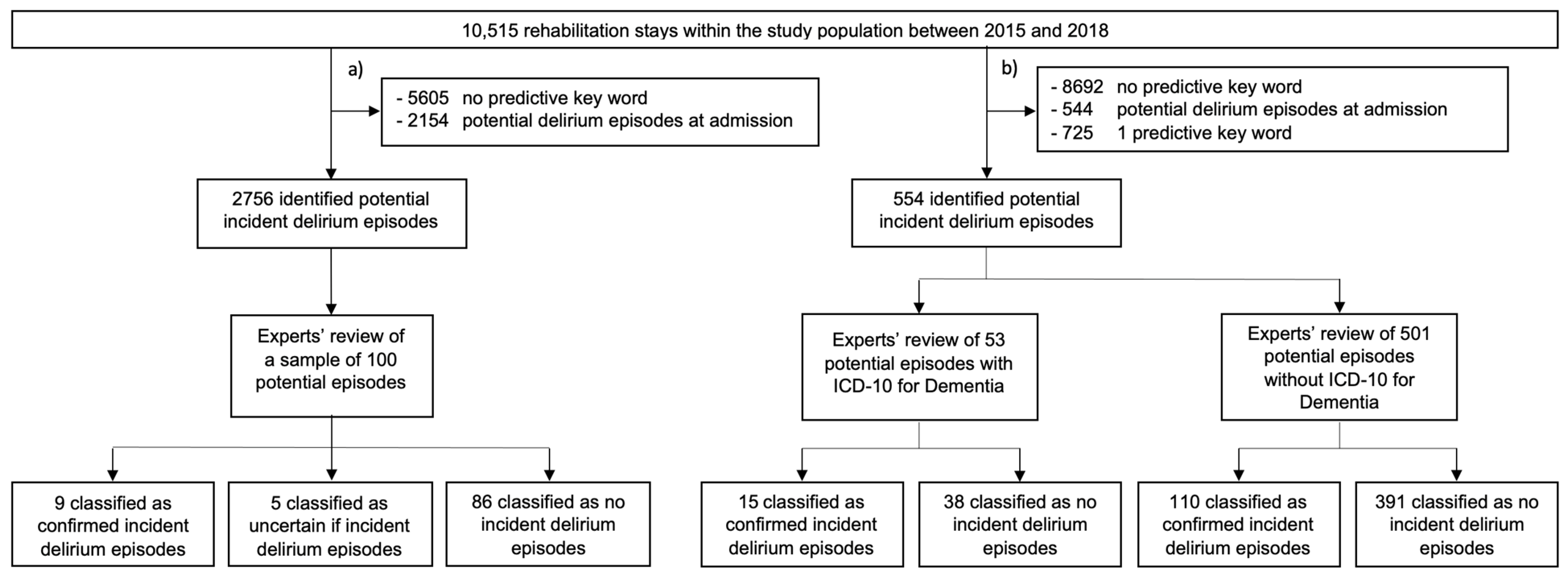
2.3. Identification and Classification of Potential Incident Delirium Episodes
2.3.1. Sample Review
2.3.2. Main Review
2.4. Identification of Recorded Delirium Discharge Diagnoses within the Claims Data
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th Revision, 5th ed.; World Health Organization: Geneva, Switzerland, 2016; Available online: https://apps.who.int/iris/handle/10665/246208 (accessed on 1 September 2021).
- Rudolph, J.L.; Inouye, S.K.; Jones, R.; Yang, F.M.; Fong, T.G.; Levkoff, S.E.; Marcantonio, E.R. Delirium: An Independent Predictor of Functional Decline After Cardiac Surgery. J. Am. Geriatr. Soc. 2010, 58, 643–649. [Google Scholar] [CrossRef]
- Davis, D.H.J.; Terrera, G.M.; Keage, H.; Rahkonen, T.; Oinas, M.; Matthews, F.; Cunningham, C.; Polvikoski, T.; Sulkava, R.; MacLullich, A.; et al. Delirium is a strong risk factor for dementia in the oldest-old: A population-based cohort study. Brain 2012, 135, 2809–2816. [Google Scholar] [CrossRef]
- Marcantonio, E.R.; Flacker, J.M.; Michaels, M.; Resnick, N.M. Delirium Is Independently Associated with Poor Functional Recovery After Hip Fracture. J. Am. Geriatr. Soc. 2000, 48, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Bellelli, G.; Frisoni, G.B.; Turco, R.; Lucchi, E.; Magnifico, F.; Trabucchi, M. Delirium Superimposed on Dementia Predicts 12-Month Survival in Elderly Patients Discharged from a Postacute Rehabilitation Facility. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2007, 62, 1306–1309. [Google Scholar] [CrossRef][Green Version]
- Jang, S.; Jung, K.-I.; Yoo, W.-K.; Jung, M.H.; Ohn, S.H. Risk Factors for Delirium During Acute and Subacute Stages of Various Disorders in Patients Admitted to Rehabilitation Units. Ann. Rehabil. Med. 2016, 40, 1082–1091. [Google Scholar] [CrossRef] [PubMed]
- McCusker, J.; Cole, M.; Abrahamowicz, M.; Primeau, F.; Belzile, E. Delirium Predicts 12-Month Mortality. Arch. Intern. Med. 2002, 162, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Kotfis, K.; Szylińska, A.; Listewnik, M.; Strzelbicka, M.; Brykczyński, M.; Rotter, I.; Żukowski, M. Early delirium after cardiac surgery: An analysis of incidence and risk factors in elderly (≥65 years) and very elderly (≥80 years) patients. Clin. Interv. Aging 2018, 13, 1061–1070. [Google Scholar] [CrossRef]
- Szylińska, A.; Rotter, I.; Listewnik, M.; Lechowicz, K.; Brykczyński, M.; Dzidek, S.; Żukowski, M.; Kotfis, K. Postoperative Delirium in Patients with Chronic Obstructive Pulmonary Disease after Coronary Artery Bypass Grafting. Medicina 2020, 56, 342. [Google Scholar] [CrossRef]
- Inouye, S.K.; Westendorp, R.G.; Saczynski, J.S. Delirium in elderly people. Lancet 2014, 383, 911–922. [Google Scholar] [CrossRef]
- Rudolph, J.L.; Doherty, K.; Kelly, B.; Driver, J.A.; Archambault, E. Validation of a Delirium Risk Assessment Using Electronic Medical Record Information. J. Am. Med. Dir. Assoc. 2016, 17, 244–248. [Google Scholar] [CrossRef]
- Leonard, M.M.; Agar, M.; Spiller, J.A.; Davis, B.; Mohamad, M.M.; Meagher, D.J.; Lawlor, P.G. Delirium Diagnostic and Classification Challenges in Palliative Care: Subsyndromal Delirium, Comorbid Delirium-Dementia, and Psychomotor Subtypes. J. Pain Symptom Manag. 2014, 48, 199–214. [Google Scholar] [CrossRef] [PubMed]
- Inouye, S.K.; Van Dyck, C.H.; Alessi, C.A.; Balkin, S.; Siegal, A.P.; Horwitz, R.I. Clarifying Confusion: The Confusion Assessment Method. Ann. Intern. Med. 1990, 113, 941–948. [Google Scholar] [CrossRef]
- Grover, S. Assessment scales for delirium: A review. World J. Psychiatry 2012, 2, 58–70. [Google Scholar] [CrossRef] [PubMed]
- De, B.J.; Wand, B.A.P.F. Delirium Screening: A Systematic Review of Delirium Screening Tools in Hospitalized Patients. Gerontoogy 2015, 55, 1079–1099. [Google Scholar] [CrossRef] [PubMed]
- Oh-Park, M.; Chen, P.; Romel-Nichols, V.; Hreha, K.; Boukrina, O.; Barrett, A. Delirium Screening and Management in Inpatient Rehabilitation Facilities. Am. J. Phys. Med. Rehabil. 2018, 97, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Inouye, S.K.; Leo-Summers, L.; Zhang, Y.; Bogardus, S.T.; Leslie, D.; Agostini, J.V. A Chart-Based Method for Identification of Delirium: Validation Compared with Interviewer Ratings Using the Confusion Assessment Method. J. Am. Geriatr. Soc. 2005, 53, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Fong, T.G.; Jones, R.; Marcantonio, E.R.; Tommet, D.; Gross, A.L.; Habtemariam, D.; Schmitt, E.; Yap, L.; Inouye, S.K. Adverse Outcomes After Hospitalization and Delirium in Persons with Alzheimer Disease. Ann. Intern. Med. 2012, 156, 848–856. [Google Scholar] [CrossRef]
- Fong, T.G.; Jones, R.N.; Shi, P.; Marcantonio, E.R.; Yap, L.; Rudolph, J.L.; Yang, F.M.; Kiely, D.K.; Inouye, S.K. Delirium accelerates cognitive decline in Alzheimer disease. Neurology 2009, 72, 1570–1575. [Google Scholar] [CrossRef] [PubMed]
- Saczynski, J.S.; Ma, C.M.K.; Xu, G.; Bs, M.R.P.; Schmitt, E.; Jones, R.; Marcantonio, E.R.; Wong, B.; Isaza, I.; Inouye, S.K. A Tale of Two Methods: Chart and Interview Methods for Identifying Delirium. J. Am. Geriatr. Soc. 2014, 62, 518–524. [Google Scholar] [CrossRef]
- Puelle, M.R.; Kosar, C.M.; Xu, G.; Schmitt, E.; Jones, R.; Marcantonio, E.R.; Cooper, Z.; Inouye, S.K.; Saczynski, J.S. The Language of Delirium: Keywords for Identifying Delirium from Medical Records. J. Gerontol. Nurs. 2015, 41, 34–42. [Google Scholar] [CrossRef]
- Ford, E.; Sheppard, J.; Oliver, S.; Rooney, P.; Banerjee, S.; Cassell, J.A. Automated detection of patients with dementia whose symptoms have been identified in primary care but have no formal diagnosis: A retrospective case–control study using electronic primary care records. BMJ Open 2021, 11, e039248. [Google Scholar] [CrossRef] [PubMed]
- WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC Classification and DDD Assignment; WHO Collaborating Centre for Drug Statistics Methodology: Oslo, Norway, 2019. [Google Scholar]
- Morandi, A.; Davis, D.; Bellelli, G.; Arora, R.C.; Caplan, G.A.; Kamholz, B.; Kolanowski, A.; Fick, D.; Kreisel, S.; MacLullich, A.; et al. The Diagnosis of Delirium Superimposed on Dementia: An Emerging Challenge. J. Am. Med. Dir. Assoc. 2017, 18, 12–18. [Google Scholar] [CrossRef]
- Voyer, P.; Richard, S.; Doucet, L.; Carmichael, P.-H. Detecting Delirium and Subsyndromal Delirium Using Different Diagnostic Criteria among Demented Long-Term Care Residents. J. Am. Med. Dir. Assoc. 2009, 10, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, N.; House, A.O.; Holmes, J.D. Occurrence and outcome of delirium in medical in-patients: A systematic literature review. Age Ageing 2006, 35, 350–364. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Lee, J.; Kim, C.A.; Huybrechts, K.F.; Bateman, B.T.; Patorno, E.; Marcantonio, E.R. Evaluation of algorithms to identify delirium in administrative claims and drug utilization database. Pharmacoepidemiol. Drug Saf. 2017, 26, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Infante, M.T.; Pardini, M.; Balestrino, M.; Finocchi, C.; Malfatto, L.; Bellelli, G.; Mancardi, G.L.; Gandolfo, C.; Serrati, C. Delirium in the acute phase after stroke: Comparison between methods of detection. Neurol. Sci. 2017, 38, 1101–1104. [Google Scholar] [CrossRef]
- Hope, C.; Estrada, N.; Weir, C.; Teng, C.-C.; Damal, K.; Sauer, B.C. Documentation of delirium in the VA electronic health record. BMC Res. Notes 2014, 7, 208. [Google Scholar] [CrossRef]


{kind=link}
| (A) | (B) |
| agress * | agress * |
| aggress * | aggress * |
| delir * | delir * |
| desorient * | desorient * |
| durcheinand * | durcheinand * |
| halluzin * | halluzin * |
| klingelmatte | klingelmatte |
| konfus * | konfus * |
| unkoperat * | unkoperat * |
| unkooperat * | unkooperat * |
| nestel | nestel |
| orient * | nicht (…) orient * |
| koperat * | nicht (…) koperat * |
| kooperat * | nicht (…) kooperat * |
| unruh * | |
| verwirr * | verwirr * |
| Study Population (n = 10,515) | |
|---|---|
| Male | 4683 (44.54%) |
| Median length of stay in days (IQR) | 22 (10) |
| Median age at admission in years (IQR) | 70 (23) |
| Age at admission, years | |
| <40 | 700 (6.66%) |
| 40–49 | 822 (7.82%) |
| 50–59 | 1684 (16.02%) |
| 60–69 | 1925 (18.31%) |
| 70–79 | 2913 (27.70%) |
| 80–89 | 2238 (21.28%) |
| >90 | 233 (2.22%) |
| Rehabilitation discipline | |
| Angiology | 631 (6.00%) |
| Cardiology | 1127 (10.72%) |
| Headache program | 450 (4.28%) |
| Neurology | 3458 (32.89%) |
| Orthopedics | 2964 (28.19%) |
| Pain program | 510 (4.85%) |
| Rheumatology | 1095 (10.41%) |
| Others | 280 (2.66%) |
| Number of Delirium-Predictive Key Words | ≥1 Antipsychotic Drug after Index Date | Potential Incident Delirium Episodes | Classified Incident Delirium Episodes | PPV (95% CI) |
|---|---|---|---|---|
| ≥2 | No | 554 | 125 | 0.23 (0.19–0.26) |
| Yes | 152 | 80 | 0.53 (0.45–0.61) | |
| ≥3 | No | 312 | 100 | 0.32 (0.27–0.37) |
| Yes | 110 | 63 | 0.57 (0.48–0.67) | |
| ≥4 | No | 197 | 85 | 0.43 (0.36–0.50) |
| Yes | 88 | 57 | 0.65 (0.55–0.75) | |
| ≥5 | No | 141 | 68 | 0.48 (0.40–0.57) |
| Yes | 68 | 46 | 0.68 (0.56–0.79) | |
| ≥6 | No | 105 | 58 | 0.55 (0.46–0.65) |
| Yes | 61 | 42 | 0.69 (0.57–0.81) | |
| ≥7 | No | 78 | 43 | 0.55 (0.44–0.66) |
| Yes | 51 | 33 | 0.65 (0.51–0.78) | |
| ≥8 | No | 61 | 33 | 0.54 (0.41–0.67) |
| Yes | 42 | 27 | 0.64 (0.49–0.79) | |
| ≥9 | No | 53 | 29 | 0.55 (0.41–0.69) |
| Yes | 38 | 24 | 0.63 (0.47–0.79) | |
| ≥10 | No | 42 | 22 | 0.52 (0.37–0.68) |
| Yes | 30 | 18 | 0.60 (0.41–0.79) |
| Rehabilitation Discipline | Rehabilitation Stays | Potential Incident Delirium Episodes | Classified Incident Delirium Episodes | Cumulative Delirium Incidence | PPV (95% CI) |
|---|---|---|---|---|---|
| Cardiology | 1127 | 31 | 6 | 0.53% | 0.19 (0.04–0.35) |
| Neurology | 3458 | 343 | 89 | 2.57% | 0.26 (0.21–0.31) |
| Orthopedics | 2964 | 111 | 19 | 0.64% | 0.17 (0.10–0.24) |
| Others ** | 2966 | 69 | 11 | 0.37% | 0.16 (0.07–0.25) |
| 10,515 | 554 | 125 | 1.19% | 0.23 (0.19–0.26) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceppi, M.G.; Rauch, M.S.; Sándor, P.S.; Gantenbein, A.R.; Krishnakumar, S.; Albert, M.; Meier, C.R. Detecting Incident Delirium within Routinely Collected Inpatient Rehabilitation Data: Validation of a Chart-Based Method. Neurol. Int. 2021, 13, 701-711. https://doi.org/10.3390/neurolint13040067
Ceppi MG, Rauch MS, Sándor PS, Gantenbein AR, Krishnakumar S, Albert M, Meier CR. Detecting Incident Delirium within Routinely Collected Inpatient Rehabilitation Data: Validation of a Chart-Based Method. Neurology International. 2021; 13(4):701-711. https://doi.org/10.3390/neurolint13040067
Chicago/Turabian StyleCeppi, Marco G., Marlene S. Rauch, Peter S. Sándor, Andreas R. Gantenbein, Shyam Krishnakumar, Monika Albert, and Christoph R. Meier. 2021. "Detecting Incident Delirium within Routinely Collected Inpatient Rehabilitation Data: Validation of a Chart-Based Method" Neurology International 13, no. 4: 701-711. https://doi.org/10.3390/neurolint13040067
APA StyleCeppi, M. G., Rauch, M. S., Sándor, P. S., Gantenbein, A. R., Krishnakumar, S., Albert, M., & Meier, C. R. (2021). Detecting Incident Delirium within Routinely Collected Inpatient Rehabilitation Data: Validation of a Chart-Based Method. Neurology International, 13(4), 701-711. https://doi.org/10.3390/neurolint13040067