
An Overview of Energy Access Solutions for Rural Healthcare Facilities

 ,
,  ,
,  ,
,  ,
,  ,
,
Abstract
1. Introduction
1.1. Background
1.2. Theoretical Analysis
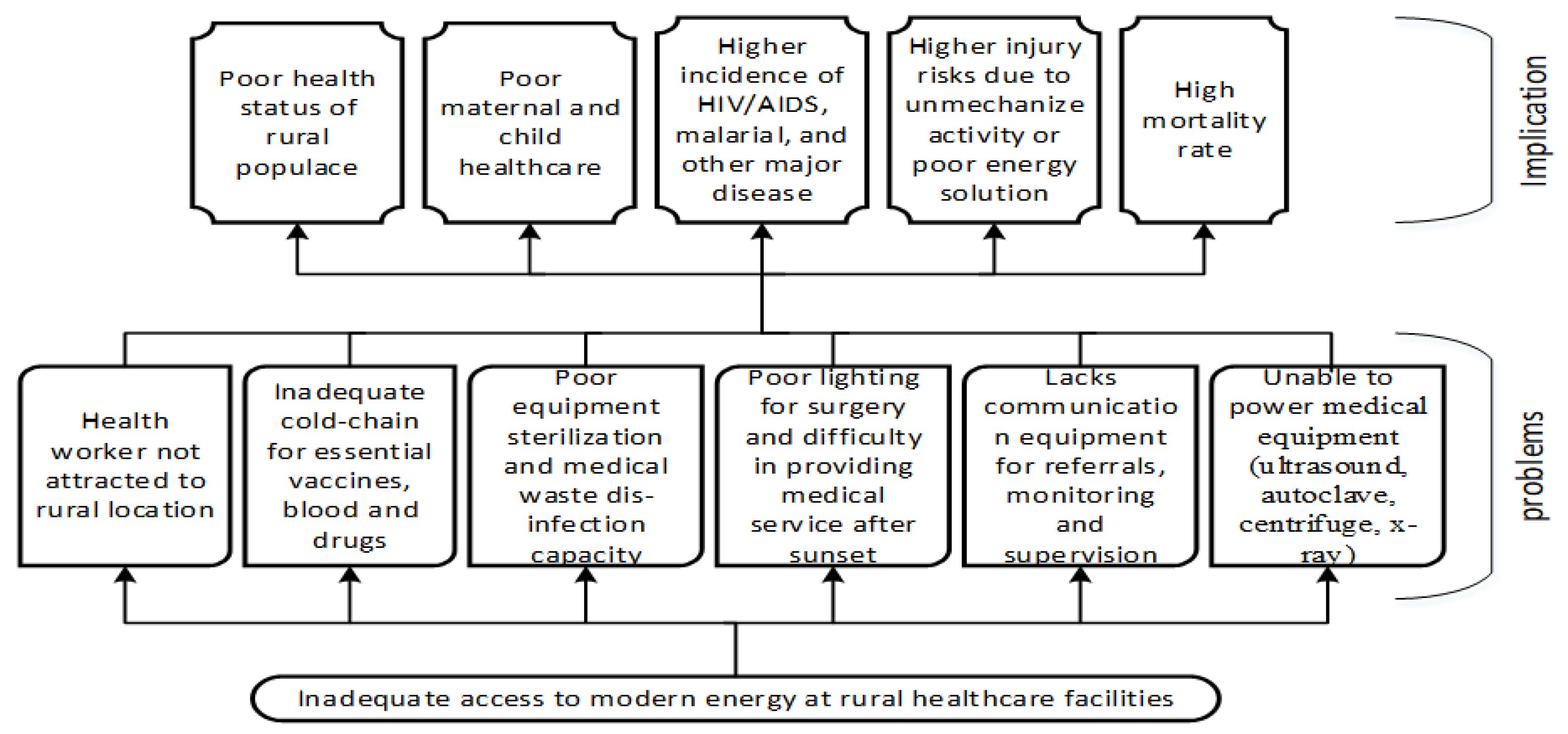
1.2.1. Effects of No Access to Reliable Energy Sources in Rural Healthcare Centres
1.2.2. Significance of Accessing Reliable Electricity in Rural Healthcare Centres
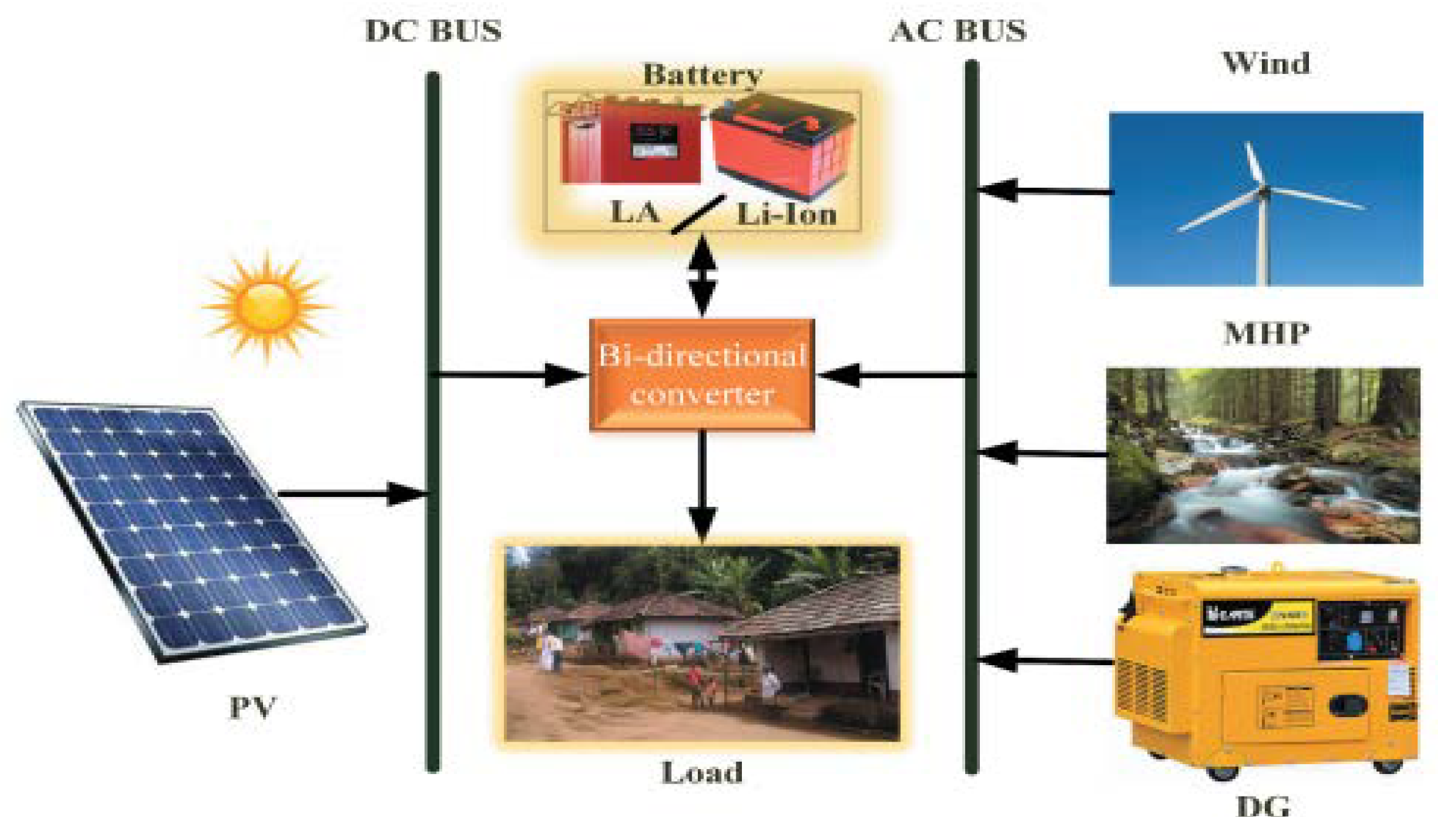
1.2.3. Rural Healthcare Centre Power Supply Alternative the Off-Grid Renewable Energy Systems
- Strategic conservation: this is simply an energy conservation method where high-power-consuming electrical appliances are replaced with low-rated appliances with similar functionality. This approach ensures less power consumption and a reduction in load demand. Appliances such as DC lighting, low-wattage lamps, and replacing Cathode Ray Tube (CRT) TV sets with Plasma or Liquide Crystal Display (LCD) are typical strategic conservation which increase the HRES performance.
- Peak shifting: This approach allows the operation of non-priority loads during off-peak periods. The operation of a shiftable peak load is suspended till an off-peak period when the demand is adequately low [37].
2. Methodology/Procedure
2.1. Energy Access Solutions and Demand-Side Management Strategies
2.2. Social and Economic Sustainability of HRES
2.3. Modelling Tools for Hybrid Energy Access Solutions
3. Conclusions and Policy Directions
- Initially, electrification is identified as a primary factor in improving the standard of healthcare administration in Sub-Saharan Africa and attracting healthcare personnel into rural areas for quality services.
- Available natural and renewable resources were identified as optimal approaches to powering rural healthcare centres. The deployment of mini-grids powered primarily by renewable energy sources and associated technologies is a solution to energy accessibility for healthcare facilities in rural or urban areas with low power supply.
- Small-scale hydropower via mini-grid or off-grid is an energy provision solution in rural areas, which possess the potential to serve healthcare facilities and provide nearby communities with sustainable energy. However, the small-scale hydropower may require modification to suit the local situation and grid size. Thus, higher and more reliable energy access in rural healthcare centres can be achieved through Hybrid Renewable Energy Sources (HRES) microsystems, such as Microgrids incorporated with solar panels and battery storage.
- Providing backup with solar panels and battery storage systems to healthcare facilities and households in urban or rural areas is considered a better, cost-effective, and operationally less-burden alternative than small-scale hydropower. Furthermore, the HRES can be aided by implementing intelligent devices developed from artificial intelligence and internet of things technologies; this allows for combining solar and wind in energy production.
- Technical maintenance of renewable energy microsystems is a necessary procedure to avoid breakdown. Therefore, as a policy measure, the benefitting communities should carry out preventive and corrective maintenance of the system. This approach ensures ownership and responsibility; the preliminary instruction given to the user will help them perform elementary maintenance, such as periodically adding distilled water to the battery.
- Since the local council, which owned the rural healthcare centre, has an insufficient budgetary allocation for the maintenance of HRES, providing funding through public-private-partnership to maintain HRES is a sure approach to prevent the early breakdown of the system. Additionally, the course of installation, training, and enlightenment of the healthcare staff on the usage and maintenance of the HRES can reduce the maintenance cost of the system. One critical component of the HRES is using an energy storage device. The storage system enhances the utilisation of the renewable energy system, reduces the need for a generator set and reduces fuel consumption.
- The adoption of DSM strategies in the HRES deployment in rural healthcare facilities is seen to lessen the start-up cost of installation and improve efficiency. In addition, DSM strategy through an energy management system can be adapted to meet the energy needs of a rural health care centre by minimising carbon emissions and guaranteeing low-cost energy.
- The financial burden of the HRES–DSM system procurement can be limited by leasing the system to the beneficiary. Alternatively, the project can be contracted out to the system operator for continuous energy system operation. As for the rural community, where the finance might be huge to handle or meet the vendor’s requirement, the government can intervene to execute the project as a national development program.
- Lastly, in improving energy access, rural electrification planning is achieved through modelling tools related to energy access modelling. A careful assessment of the features of various tools offers an easy means of identifying and choosing a tool that can give perceptions of the particular research question, adequately model the processes, and retain the indispensable technological and economic properties.
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Nomenclature
| HRES | Hybrid Renewable Energy Sources | CRT | TV Cathode Ray Tube Television |
| DSM | Demand Side Management | LCD | Liquid Crystal Display |
| SDG | Sustainable Development Goal | LRHC | Low Rating High Cost |
| ECE | Economic Computable Equilibrium | MRMC | Medium Rating Medium Cost |
| PHCs | Primary Health Centres | HRLC | High Rating Low-Cost |
| WHO | World Health Organisation | kW | KiloWatt |
| HRES | Renewable Energy System | NGOs | Non Governmental Organisations |
| PV | Photo Voltaic | ARE | Alliance for Rural Electrification |
| UN | United Nation | DRE | Decentralised Renewable Energy |
| AC | Alternating Current | PPA | Power Purchasing Agreement |
| DC | Direct Current | RE | Renewable Energy |
| DG | Distributed Generation | RES | Renewable Energy System |
| CO2 | Carbon dioxide | UPS | Uninterruptible Power Supply |
| RHU | Rural Health Units | LCOE | Levelized cost of energy: LCOE |
| PSAT | Power Systems Analysis | COVID-19 | Corona Virus |
| HO | Heuristic Optimisation | I & ODS Investment & Operation Support | |
| CGE | Computable General Equilibrium | MIP | Mix Integer Programming |
| LP | Linear Programming | ABS | Agent Based Simulation |
| HOMER | Hybrid Optimisation of Multiple Electric Renewable Energy | ||
| CMA-ES | Covariance Matrix Adaptation Evolution Strategy | ||
| TETFund | Tertiary Education Trust Fund, Nigeria | ||
| NPHCDA | National Primary Health Care Development Agency | ||
| NREL | National Renewable Energy Laboratory | ||
| REA | Rural Electrification Agency | ||
References
- Franco, A.; Shaker, M.; Kalubi, D.; Hostettler, S. A review of sustainable energy access and technologies for healthcare facilities in the Global South. Sustain. Energy Technol. Assess. 2017, 22, 92–105. [Google Scholar] [CrossRef]
- Oladigbolu, J.O.; Al-Turki, Y.A.; Olatomiwa, L. Comparative study and sensitivity analysis of a standalone hybrid energy system for electrification of rural healthcare facility in Nigeria. Alex. Eng. J. 2021, 60, 5547–5565. [Google Scholar] [CrossRef]
- Adair-Rohani, H.; Zukor, K.; Bonjour, S.; Wilburn, S.; Kuesel, A.C.; Hebert, R.; Fletcher, E.R. Limited electricity access in health facilities of sub-Saharan Africa: A systematic review of data on electricity access, sources, and reliability. Glob. Health Sci. Pract. 2013, 1, 249–261. [Google Scholar] [CrossRef]
- Akinyele, D.O.; Rayudu, R.K. Community-based hybrid electricity supply system: A practical and comparative approach. Appl. Energy 2016, 171, 608–628. [Google Scholar] [CrossRef]
- Ikenna, D.; Salman, T.; Okoye, T.T. Improving Access to Clean Reliable Energy for Primary Health Care Centres in Nigeria: Situation Analysis of PHCs in the Federal Capital Territory. In Heinrich Boell Stiftung Nigeria; Heinrich Boell Stiftung Nigeria: Abuja, Nigeria, 2018. [Google Scholar]
- Olatomiwa, L.; Blanchard, R.E.; Mekhilef, S.; Akinyele, D. Hybrid renewable energy supply for rural healthcare facilities: An approach to quality healthcare delivery. Sustain. Energy Technol. Assess. 2018, 30, 121–138. [Google Scholar] [CrossRef]
- Akinyele, D.O.; Nair, N.K.C.; Rayudu, R.K.; Chakrabarti, B. Decentralised energy generation for end-use applications: Economic, social and environmental benefits assessment. In Proceedings of the IEEE Innovative Smart Grid Technologies Asia (ISGT ASIA), Kuala Lumpur, Malaysia, 20–23 May 2014; pp. 84–89. [Google Scholar]
- Energypedia. Access to Modern Energy and the Impact on Health. 2018. Available online: https://energypedia.info/wiki/Access_to_modern_energy_and_the_impact_on_health (accessed on 23 June 2022).
- Uzoma, C.C.; Amadi, K.C. Energy access: A key to rural development in Nigeria. J. Soc. Sci. 2019, 5, 452–456. [Google Scholar]
- Welland, A. Electrification of Health Clinics in Rural Areas: Challenges and Opportunities; CMEDT-Smart Villages Initiative, c/o Trinity College: Cambridge, UK, 2017. [Google Scholar]
- Aemro, Y.B.; Moura, P.; De Almeida, A.T. Energy access during and post-COVID-19 pandemic in sub-Saharan countries: The case of Ethiopia. In Environment, Development and Sustainability; Springer: Berlin/Heidelberg, Germany, 2022; pp. 1–22. [Google Scholar]
- Chen, Y.J.; Chindarkar, N.; Xiao, Y. Effect of reliable electricity on health facilities, health information, and child and maternal health services utilisation: Evidence from rural Gujarat, India. J. Health Popul. Nutr. 2019, 38, 1–16. [Google Scholar] [CrossRef]
- Kaygusuz, K. Energy services and energy poverty for sustainable rural development. Renew. Sustain. Energy Rev. 2011, 15, 936–947. [Google Scholar] [CrossRef]
- Rabetanetiarimanana, J.C.I.; Radanielina, M.H.; Rakotondramiarana, H.T. PV-Hybrid Off-Grid and Mini-Grid Systems for Rural Electrification in Sub-Saharan Africa. Smart Grid Renew. Energy 2018, 9, 171. [Google Scholar] [CrossRef]
- Babatunde, O.M.; Adedoja, O.S.; Babatunde, D.E.; Denwigwe, I.H. Off-grid hybrid renewable energy system for rural healthcare centers: A case study in Nigeria. Energy Sci. Eng. 2019, 7, 676–693. [Google Scholar] [CrossRef]
- Kolhe, M.L.; Ranaweera, K.I.U.; Gunawardana, A.S. Techno-economic sizing of off-grid hybrid renewable energy system for rural electrification in Sri Lanka. Sustain. Energy Technol. Assess. 2015, 11, 53–64. [Google Scholar] [CrossRef]
- Moner-Girona, M.; Kakoulaki, G.; Falchetta, G.; Weiss, D.J.; Taylor, N. Achieving universal electrification of rural healthcare facilities in sub-Saharan Africa with decentralised renewable energy technologies. Joule 2021, 5, 2687–2714. [Google Scholar] [CrossRef]
- Akinyele, D.O.; Rayudu, R.K. Strategy for developing energy systems for remote communities: Insights to best practices and sustainability. Sustain. Energy Technol. Assess. 2016, 16, 106–127. [Google Scholar] [CrossRef]
- Ohunakin, O.S.; Adaramola, M.S.; Oyewola, O.M.; Fagbenle, R.O. Solar energy applications and development in Nigeria: Drivers and barriers. Renew. Sustain. Energy Rev. 2014, 32, 294–301. [Google Scholar] [CrossRef]
- Olatomiwa, L.; Mekhilef, S.; Huda, A.S.N.; Ohunakin, O.S. Economic evaluation of hybrid energy systems for rural electrification in six geopolitical zones of Nigeria. Renew. Energy 2015, 83, 435–446. [Google Scholar] [CrossRef]
- Chowdhury, T.; Chowdhury, H.; Hasan, S.; Rahman, M.S.; Bhuiya, M.; Chowdhury, P. Design of a standalone energy hybrid system for a makeshift health care center: A case study. J. Build. Eng. 2021, 40, 102346. [Google Scholar] [CrossRef]
- Akinyele, D.; Rayudu, R.; Blanchard, R.E. Sustainable Microgrids for Energy-Poor Communities: A Spotlight on the Planning Dimensions; IEEE: Piscataway, NJ, USA, 2016. [Google Scholar]
- Asian Development Bank. Improving Lives of Rural Communities Through Developing Small Hybrid Renewable Energy Systems; Asian Development Bank: Mandaluyong, Philippines, 2017. [Google Scholar]
- Olatomiwa, L.; Mekhilef, S.; Ohunakin, O.S. Hybrid renewable power supply for rural health clinics (RHC) in six geo-political zones of Nigeria. Sustain. Energy Technol. Assess. 2016, 13, 1–12. [Google Scholar] [CrossRef]
- Ighravwe, D.E.; Babatunde, M.O. Determination of a suitable renewable energy source for mini-grid business: A risk-based multicriteria approach. J. Renew. Energy 2018, 2018, 2163262. [Google Scholar] [CrossRef]
- Irena, R.E.S. Renewable Energy Target Setting; International Renewable Energy Agency: Abu Dhabi, United Arab Emirates, 2015. [Google Scholar]
- Javadi, D.; Ssempebwa, J.; Isunju, J.B.; Yevoo, L.; Amu, A.; Nabiwemba, E.; Severi, L. Implementation research on sustainable electrification of rural primary care facilities in Ghana and Uganda. Health Policy Plan. 2020, 35, 124–136. [Google Scholar] [CrossRef]
- Olatomiwa, L. Optimal configuration assessments of hybrid renewable power supply for rural healthcare facilities. Energy Rep. 2016, 2, 141–146. [Google Scholar] [CrossRef]
- Uamusse, M.M.; Tussupova, K.; Persson, K.M.; Bengtsson, L.; Berndtsson, R.; Zobaa, A. Access to sustainable electrification: Possibilities for rural Mozambique. Cogent Eng. 2020, 7, 1765688. [Google Scholar] [CrossRef]
- Dávalos, A.; De Jesús Gil Herrera, R.; Colmenares, R.F.A. Comprehensive solution approach to the sustainability problem of photovoltaic systems: The Bolivian case. Cogent Eng. 2019, 6, 1691314. [Google Scholar] [CrossRef]
- Maggio, G.; Squadrito, G.; Nicita, A. Hydrogen and medical oxygen by renewable energy based electrolysis: A green and economically viable route. Appl. Energy 2022, 306, 117993. [Google Scholar] [CrossRef]
- Olsen, K.; Jimenez, A. Renewable Energy for Rural Health Clinics; National Renewable Energy Laboratory Publishing: Golden, CO, USA, 1998. [Google Scholar]
- Akinyele, D.; Olatomiwa, L.; Ighravwe, D.E.; Babatunde, M.O.; Monyei, C.; Aikhuele, D. Optimal planning and electricity sharing strategy of hybrid energy system for remote communities in Nigeria. Sci. Afr. 2020, 10, e00589. [Google Scholar] [CrossRef]
- Salisu, S.; Mustafa, M.W.; Olatomiwa, L.; Mohammed, O.O. Assessment of technical and economic feasibility for a hybrid PV-wind-diesel-battery energy system in a remote community of north-central Nigeria. Alex. Eng. J. 2019, 58, 1103–1118. [Google Scholar] [CrossRef]
- Pittalis, M.; Kyriakarakos, G.; Moner-Girona, M. The role of photovoltaics in Clean Energy Access Business Models for Social Infrastructure in Sub-Saharan Africa—Existing Models and Emerging Trends. In Encyclopedia of Sustainability Science and Technology Second Edition; Springer: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Watson, J.; Johnson, O. Renewable Energy Technologies for Rural Development. 2010. Available online: https://policycommons.net/artifacts/100912/renewable-energy-technologies-for-rural-development/ (accessed on 23 June 2022).
- Ramesh, M.; Saini, R.P. Demand Side Management based techno-economic performance analysis for a standalone hybrid renewable energy system of India. Energy Sources Part A Recovery Util. Environ. Eff. 2021, 43, 1–29. [Google Scholar] [CrossRef]
- Ayodele, T.R.; Mosetlhe, T.C.; Yusuff, A.A.; Ogunjuyigbe, A.S.O. Off-grid hybrid renewable energy system with hydrogen storage for South African rural community health clinic. Int. J. Hydrogen Energy 2021, 46, 19871–19885. [Google Scholar] [CrossRef]
- Lemence, A.L.G.; Tamayao, M.-A.M. Energy consumption profile estimation and benefits of hybrid solar energy system adoption for rural health units in the Philippines. Renew. Energy 2021, 178, 651–668. [Google Scholar] [CrossRef]
- Lemence, A.L.G.; Tamayao, M.A.M. Techno-Economic Potential of Hybrid Renewable Energy Systems for Rural Health Units in the Philippines. World Med. Health Policy 2021, 13, 97–125. [Google Scholar] [CrossRef]
- Kyriakarakos, G.; Dounis, A. Intelligent Management of Distributed Energy Resources for Increased Resilience and Environmental Sustainability of Hospitals. Sustainability 2020, 12, 7379. [Google Scholar] [CrossRef]
- WHO; World Bank. Access to Modern Energy Services for Health Facilities in Resource-Constrained Settings—A Review of Status, Significance, Challenges and Measurement. 2015. Available online: https://apps.who.int/iris/handle/10665/156847 (accessed on 30 June 2022).
- Porcaro, J.; Severi, L.; Mcgregor, C. Lasting Impact: Sustainable Off-Grid Solar Delivery Models to Power Health and Education; UN Foundation and SEforALL: Vienna, Austria, 2019. [Google Scholar]
- Ramesh, M.; Saini, R.P. Optimisation of a Standalone Hybrid Renewable Energy System Using Demand-Side Management for a Remote Rural Area in India. In Proceedings of the Second International Conference on Smart Energy and Communication, Jaipur, India, 20–21 March 2020; Springer: Singapore, 2021. [Google Scholar]
- Taddonio, K. Renewable Energy Facts Sheet: Renewables Make a Powerful Case as Hospital Energy Source; U.S. Department of Energy: Washington, DC, USA, 2011. [Google Scholar]
- Soler, A.; Jæger, J.; Lecoque, D. Best Practices for Electrifying Rural Health Facilities with Decentralised Renewables. 2020, pp. 1–54. Available online: https://www.ruralelec.org/sites/default/files/2020-08-31%20-%20Best%20Practices%20for%20Electrifying%20Rural%20Health%20Facilities_Final.pdf (accessed on 30 June 2022).
- WHO. Strategic Roadmap on Health and Energy. 2022. Available online: https://www.who.int/initiatives/health-and-energy-platform-of-action/high-level-coalition-on-health-and-energy/strategic-roadmap-on-health-and-energy (accessed on 1 December 2022).
- Ringkjøb, H.K.; Haugan, P.M.; Solbrekke, I.M.A. Review of modelling tools for energy and electricity systems with large shares of variable renewables. Renew. Sustain. Energy Rev. 2018, 96, 440–459. [Google Scholar] [CrossRef]
- Logan, T.M.J.; Blair, N.; Sullivan, P.; Bazilian, M. RE-ASSUME: A Decision Maker’s Guide to Evaluating Energy Scenarios, Modeling, and Assumptions. 2013; Available online: http://iea-retd.org/wp-content/uploads/2013/07/RE-Assume_IEA-RETD_2013.pdf (accessed on 23 August 2022).
- Després, J.; Hadjsaid, N.; Criqui, P.; Noirot, I. Modelling the impacts of variable renewable sources on the power sector: Reconsidering the typology of energy modelling tools. Energy 2015, 80, 486–495. [Google Scholar] [CrossRef]
- Kumar, P.; Deokar, S. Optimal Design Configuration Using HOMER; Springer: Berlin/Heidelberg, Germany, 2017; p. 442. [Google Scholar]
- Olatomiwa, L.; Blanchard, R.E.; Uligwe, J. Demand side management strategies for solar-PV penetration in powering rural healthcare centre in Africa. In the IAPE ’19; University of Oxford: Oxford, UK, 2019; Available online: https://hdl.handle.net/2134/37301 (accessed on 30 June 2022).
- Beitelmal, W.H.; Okonkwo, P.C.; Al Housni, F.; Grami, S.; Emori, W.; Uzoma, P.C.; Das, B.K. Renewable energy as a source of electricity for Murzuq health clinic during COVID-19. MRS Energy Sustain. 2022, 9, 79–93. [Google Scholar] [CrossRef]
- Vishnupriyan, J.; Manoharan, P.S. Prospects of hybrid photovoltaic–diesel standalone system for six different climate locations in Indian state of Tamil Nadu. J. Clean. Prod. 2018, 185, 309–321. [Google Scholar] [CrossRef]
- Longe, O.M.; Ouahada, K.; Rimer, S.; Ferreira, H.C.; Han Vinck, A.J. Distributed Optimisation Algorithm for Demand Side Management in a Grid-Connected Smart Microgrid. Sustainability 2017, 9, 1088. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
INPUT: Increased financing for energy interventions, including:
| IMPACT OF FINANCING RENEWABLE SOLUTIONS |
OUTPUT: Enhanced elements of energy supply ecosystem
| ENHANCED ENERGY PERFORMANCE |
INTERMEDIATE OUTCOME: Healthcare facility access to modern energy services for electricity and thermal requirements.
| ENERGY ACCESS |
| RE Solutions | Modularity & Scalability | Application Services | Deployment Area | Operations & Maintenance Cost | CO2 & Emission? | Seasonal Output? | Backup Available? | Technical Maintenance | Safety & Environ. | Investment Cost/Capital |
|---|---|---|---|---|---|---|---|---|---|---|
| Natural and Renewable resources [8,14,21,25,33]. | Y | All | U, R | Medium/High | N | Y—Solar, Wind & Hydro | Y | Scheduled & Periodical | H-SL | Medium & High |
| Off-grid Installations [26,37] | Y | All | R | Medium | Y/N | Y—Solar, Wind & Hydro | Y | Minimal & Periodical | M-SL | Medium & High |
| Fossil Fuel-based [26] | Y | All | U, R | High | Y | N | N | Scheduled & Periodical | L-SL | Medium |
| Solar PV with or without Storage, [12,27,34] | Y | All, may exclude HC. | U, R | Low | N | Y | Y | Minimal & Periodical | H-SL | High |
| Solar PV Home Systems [23] | Y | Exclude HC | U, R | Low | N | Y | Y | Minimal & Periodical | H-SL | High |
| Lithium-ion batteries & Other Storage. [23] | Y | Exclude HC | U, R | Low | N | N | -- | Minimal & Periodical | M-SL | Medium & High |
| Hybrid storage units. [23] | Y | Exclude HC | U, R | Low | N | N | -- | Minimal & Periodical | M-SL | Medium & High |
| Wind Turbine. [34] | Y | All | R | Low | N | Y | N | Scheduled & Periodical | M-SL | Medium |
| Mini-grids. [3,11,26]. | N | All | U, R | Medium | Y—fossil fuel based | Y—Night hours | Y/N | Scheduled & Periodical | M-SL | Medium & High |
| Small & Micro Hydro. [29] | Y | All | R | Medium/High | N | Y—Low water heads | N | Scheduled & Periodical | M-SL | Medium & High |
| Hybrid RE & Fossil Fuel Systems. [15,26,37,38,48,49] | Y | All | U, R | Medium/High | Y—Minimal | Y | Y | Minimal & Periodical | M-SL | High |
| Hybrid Solar PV/Wind/DG/Battery and Wind (HRES). [2,21,36,40,49] | Y | All | U, R | Medium/High | N | Y | Y | Minimal & Periodical | M-SL | High |
| Microgrids- Solar PV and Battery storage. [11,15,37]. | Y | All, may exclude HC. | U, R | Low | N | Y | Y | Minimal & Periodical | H-SL | High |
| Demand Side Management (DSM). [36,40] | -- | All | U, R | -- | -- | -- | -- | -- | H-SL | Low |
| HRES & DSM [36,40] | Y | All | U, R | Medium/High | Y—Minimal | Y | Y | Minimal & Periodical | M-SL | Low & Medium |
| S/N | Model | Full Name | Purpose | Developer | Available | Software Type | Method/ Solver | Temporal Resolution | Modelling Horizon |
|---|---|---|---|---|---|---|---|---|---|
| 1 | COMPETES | Comprehensive Market Power in Electricity Transmission and Energy Simulator | I & ODDS | Energy Research Centre of the Netherlands | Only ECA and Partners | AIMMS/GUROBI | Simulation | Hourly | User Define |
| 2 | COMPOSE | Compare Options for Sustainable Energy | ODS & S | Morten Blarke, ENERGIANALYSE.DK | AC | Standalone, CPLEX or GUROBI | MAP | User Define | User Define |
| 3 | DER-CAM | Distributed Energy Resources Customer Adoption Model | I & ODDS | Lawrence Berkeley National Laboratory | F | Online:-None Licensed:-GAMS | MAP | Minutes & Hourly | |
| 4 | DESSTinEE | Demand for Energy Services, Supply and Transmission in Europe | S, I & ODDS | Imperial College London—Iain Staffell, Richard Green | OS | VBA/Excel | Simulation | Hourly | 2050 |
| 5 | DIETER | Dispatch and Investment Evaluation Tool with Endogenous Renewables | I & ODDS | DIW Berlin—Alexander Zerrahn & Wolf-Peter Schill | OS | Solver + GAMS | LP | Hourly | 1 yr |
| 6 | EMLab- Generation | Energy Modelling Laboratory—Generation | IDS | TU Delft—Richstein, Chappin, Bhagwat & de Vries | OS | Maven JAVA | ABS | Yearly | 2050 |
| 7 | EMPIRE | European Model for Power system Investment with Renewable Energy | IDS | NTNU—Christian Skar et al. | UN | Xpress-Mosel | LP | User Define | 40–50 yrs |
| 8 | EnergyPlan | Sustainable Energy Planning Research Group | S, DIS | Aalborg University | F | Standalone | Simulation | Hourly | 1 yr |
| 9 | energyPro | energyPro | I & ODDS | EMD International A/S | C | Standalone | AO | Minutes | 40 yrs Max |
| 10 | ITEM | Energy Transition Model | S | Quintel Intelligence | OS | Online tool | Simulation | 15 min, hr & yr | 2050 |
| 11 | GEM-E3 | General Equilibrium Model for Economy-Energy-Environment | S | European Commission Funded Multinational Collaboration | GAMS (Solved with PATH) | CGI | 5 yrs | 2030 & 2050 | |
| 12 | GENESYS | Genetic Optimisation of a European Energy Supply System | IDS | RWTH-Aachen University—Alvarez, Bussar, Cai, Chen, Moraes, etc. | OS | Stand-alone | CMA-ES & HO | Hourly | 2050 |
| 13 | GridLAB-D | PSAT | US Department of Energy | OS | Standalone | ABS | Seconds | 3–5 yrs | |
| 14 | HOMER | Hybrid Optimisation of Multiple Energy Resources | I & ODDS | NREL—Peter Lilienthal | C | Standalone | Simulation | Minutes | Multi-year |
| 15 | HYPERSIM | PSAT | Opal-RT | C | Stand-alone | Simulation | 10 micr sec | User Define | |
| 16 | iHOGA | Improved Hybrid Optimisation by Genetic Algorithms | I & ODDS | Dr. Rodolfo Dufo-López—University of Zaragoza | ED | Standalone | HO | Hourly | Yearly |
| 17 | LEAP | Long-range Energy Alternatives Planning | S | Stockholm Environment Institute | AS | Simulation & LP | Yearly | 20–30 Yrs | |
| 18 | LIBEMOD | Liberalisation MODel for the European Energy Markets | S | Frisch Centre & the Research Department at Statistics Norway | GAMS | ECE | Yearly | 1–2-yrs | |
| 19 | MESSAGE | Model for Energy Supply Strategy Alternatives and their General Environmental Impact | S, IDS | IIASA | UR | GAMS & ORACLE | LP | User Define | 50–100 yrs |
| 20 | NEMS | National Energy Modelling System | S | US Energy Information Administration (EIA) | Free & Commercial Veriosn | Simulation | Yearly | 2050 | |
| 21 | Remove (SOLPH) | Open Energy Modelling Framework | S, I & ODDS | Remove developing group (Reiner Lemoine Institut/ZNES Flensburg/OVGU) | OS | Solver + Python | LP, MIP | Sec to yrs | User Define |
| 22 | OSeMOSYS | The Open Source Energy Modelling System | IDS | KTH—Howells et al. | OS | GNU MathProg | LP | User Define | User Define |
| 23 | PLEXUS | PLEXOS Integrated Energy Model | I & ODS, S, | Energy Exemplar—Glenn Drayton | C | Standalone | User Define | User Define | |
| 24 | POLES | Prospective Outlook on Long-term Energy Systems | S, I & ODDS | CNRS (GAEL Energy), Enerdata, JRC-IPTS | Simulations | Yearly | 2050 | ||
| 25 | RAPSim | Renewable Alternative Power systems Simulation | PSAT | NES, AUU—Pöchacker, Khatib, Elmenreich et al. | OS | Standalone | Simulations | Minutes | Multi days |
| 26 | ReEDS | Regional Energy Deployment System | S (& IDS) | NREL | GAMS (Excel & R) | LP | 2 yr period | 2050 | |
| 27 | REMix | Renewable Energy Mix | I & ODS | DLR | GAMS | LP | Hourly | 2 yrs | |
| 28 | renpass | Renewable Energy Pathways Simulation System | ODS, S | Frauke Wiese & Gesine Bökenkamp | OS | MySQL, R, RMySQL | Simulations | Hourly | 1 yr |
| 29 | RETScreen | The RETSCreen Clean Energy Project Analysis Software | IDS, S | Natural Resources Canada | F | Windows with .NET | Simulation | Year/Month/Day | 100 yrs |
| 30 | SIREN | Sustainable Energy Now Integrated Renewable Energy Network | S | Sustainable Energy Now Inc.—Angus King | OS | Standalone | Simulation | Hourly | 1 yr |
| 31 | SWITCH | Solar, Wind, Transmission, Conventional Generation & Hydroelectricity | I & Odds | Fripp, Johnston & Maluenda | OS | Python | Map | Hourly | User Define |
| 32 | Temora | Tools For Energy Model Optimisation & Analysis | S | NC State University—K. Hunter et al. | OS | Solver + Python | LP | Yearly | User Define |
| 33 | WEM | World Energy Model | S | International Energy Agency | others + Vensim | Simulations | Yearly | 2040 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olatomiwa, L.; Sadiq, A.A.; Longe, O.M.; Ambafi, J.G.; Jack, K.E.; Abd'azeez, T.A.; Adeniyi, S. An Overview of Energy Access Solutions for Rural Healthcare Facilities. Energies 2022, 15, 9554. https://doi.org/10.3390/en15249554
Olatomiwa L, Sadiq AA, Longe OM, Ambafi JG, Jack KE, Abd'azeez TA, Adeniyi S. An Overview of Energy Access Solutions for Rural Healthcare Facilities. Energies. 2022; 15(24):9554. https://doi.org/10.3390/en15249554
Chicago/Turabian StyleOlatomiwa, Lanre, Ahmad A. Sadiq, Omowunmi Mary Longe, James G. Ambafi, Kufre Esenowo Jack, Toyeeb Adekunle Abd'azeez, and Samuel Adeniyi. 2022. "An Overview of Energy Access Solutions for Rural Healthcare Facilities" Energies 15, no. 24: 9554. https://doi.org/10.3390/en15249554
APA StyleOlatomiwa, L., Sadiq, A. A., Longe, O. M., Ambafi, J. G., Jack, K. E., Abd'azeez, T. A., & Adeniyi, S. (2022). An Overview of Energy Access Solutions for Rural Healthcare Facilities. Energies, 15(24), 9554. https://doi.org/10.3390/en15249554