
A QoS-Aware IoT Edge Network for Mobile Telemedicine Enabling In-Transit Monitoring of Emergency Patients
 ,
,
Abstract
1. Introduction
1.1. Key Contributions of the Paper
- To address the needs of the resource-constrained environment, this work proposes an IoT edge algorithm integrated with a wearable-device-based monitoring algorithm for edge (WDMA-Edge).
- Currently, a standardized health score to assess patients’ risk levels is lacking. We propose an on-the-fly emergency health score (OFEHS) to monitor emergency patients during transit.
- An adaptive QoS-aware packet transmission for fog (AQPT-Fog) algorithm is designed and implemented to prioritize patient mobilization.
- A simulation study is performed based on real-world traffic data collected from the stretch of road in Mysuru, India. The results showcase the need to have a dynamic communication architecture integrating V2I and show that deploying stationary units greatly improves QoS.
1.2. Paper Outline
2. Literature Review
3. Proposed Research Framework
- RO1: Designing a common standard for patient risk scoring during traversal to the hospital;
- RO2: Hybrid communication architecture for transmitting delay-intolerant health risk data;
- RO3: Traffic-aware real-time routing of health risk data to the selected hospital.
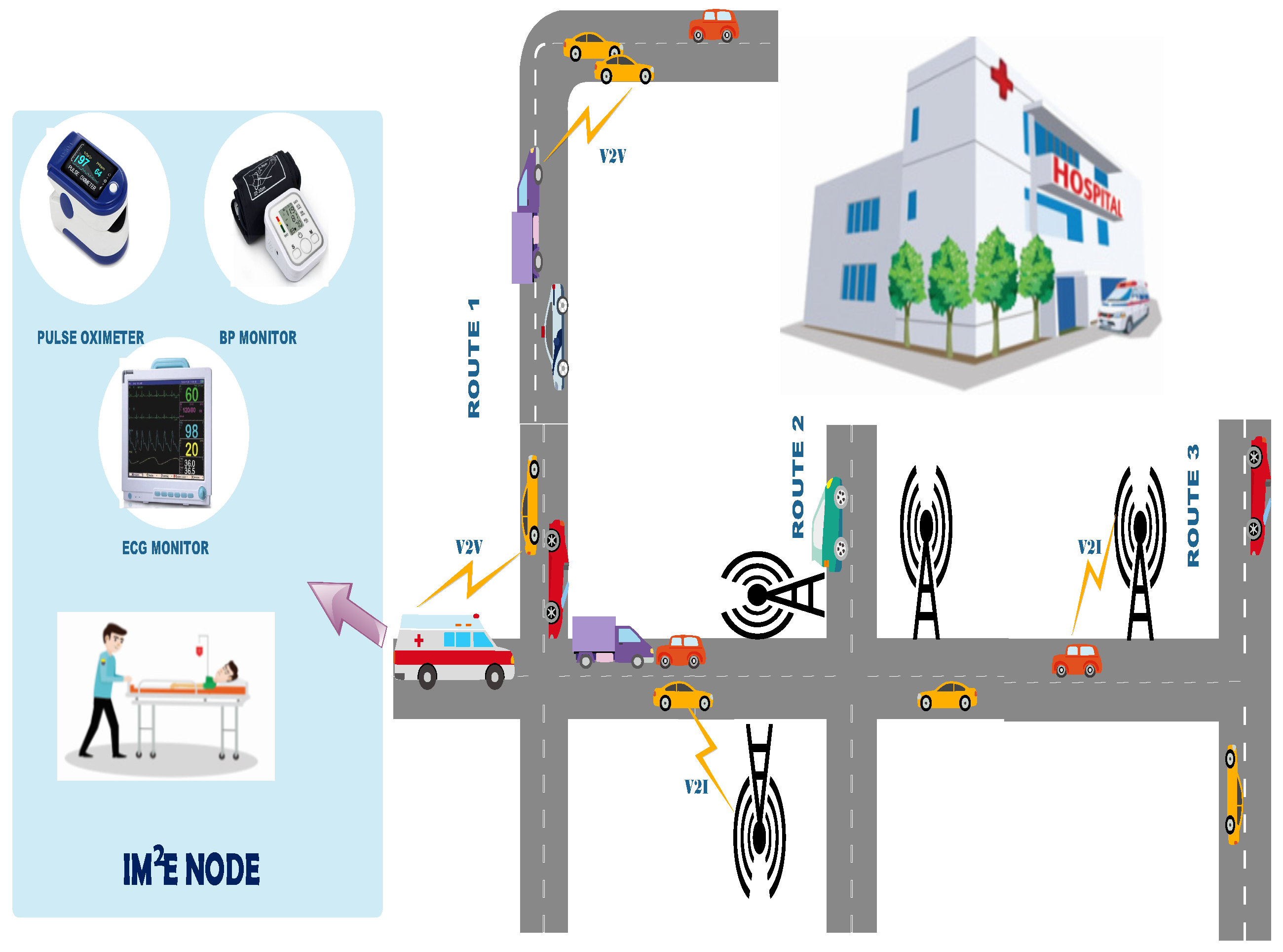
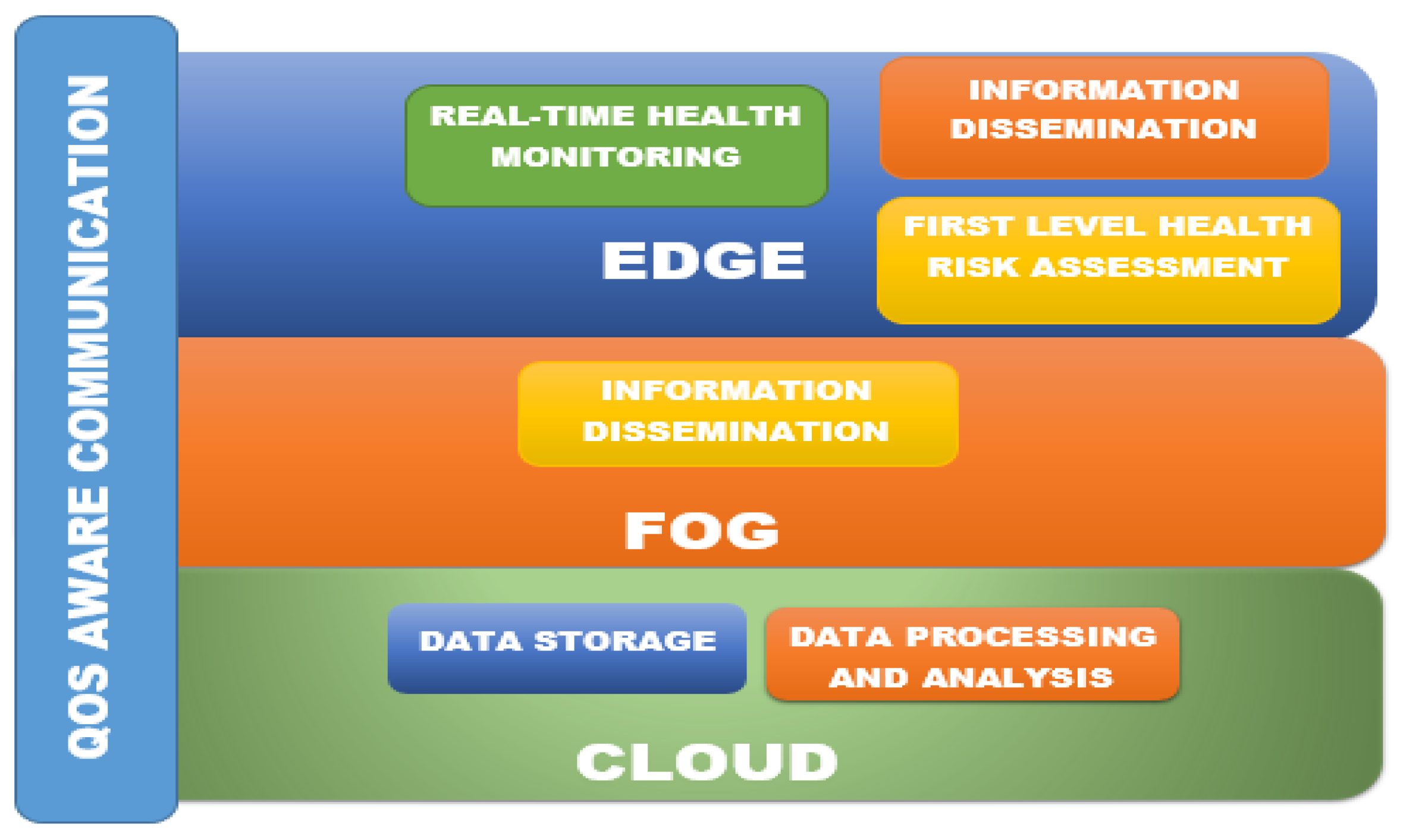
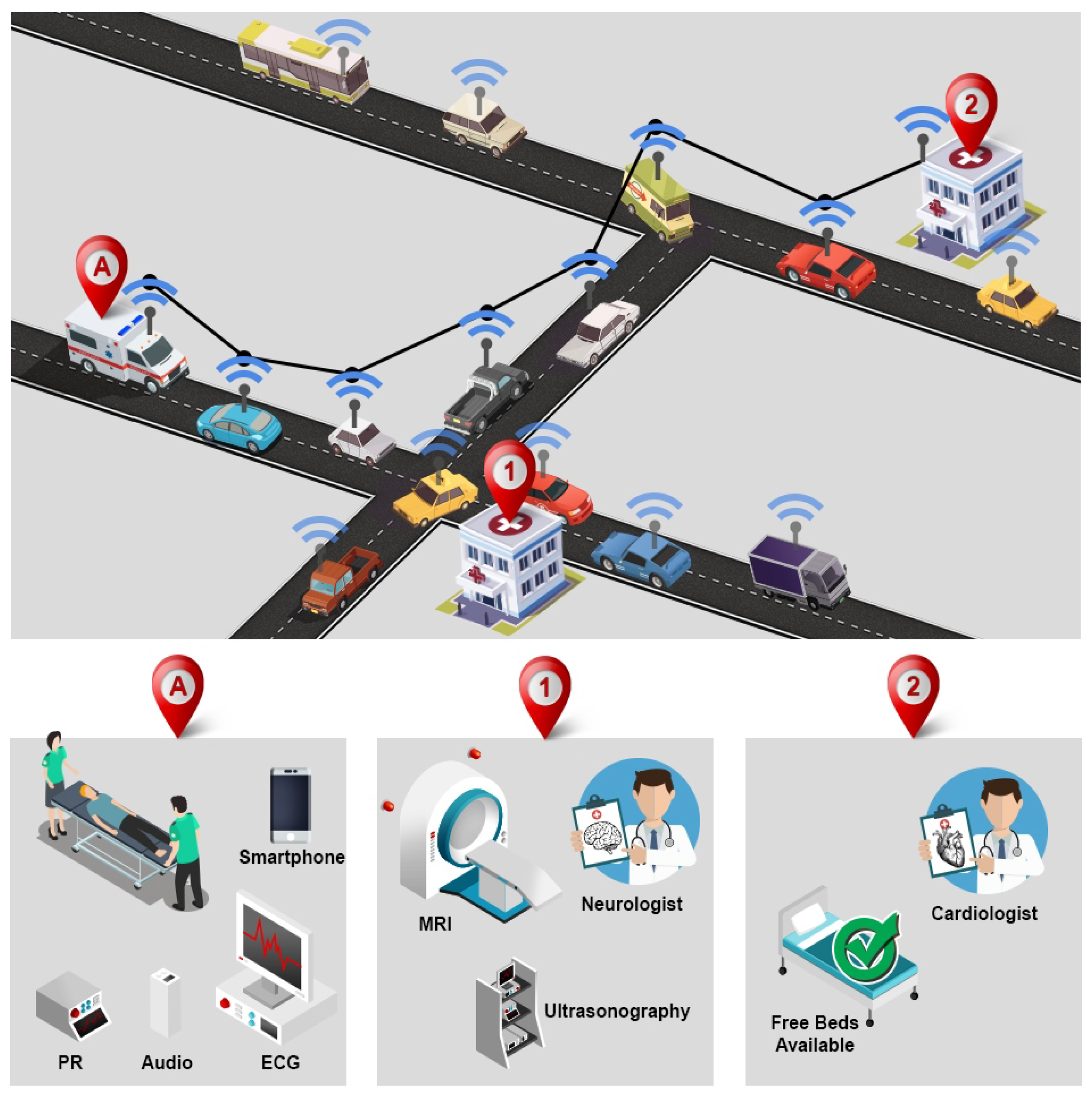
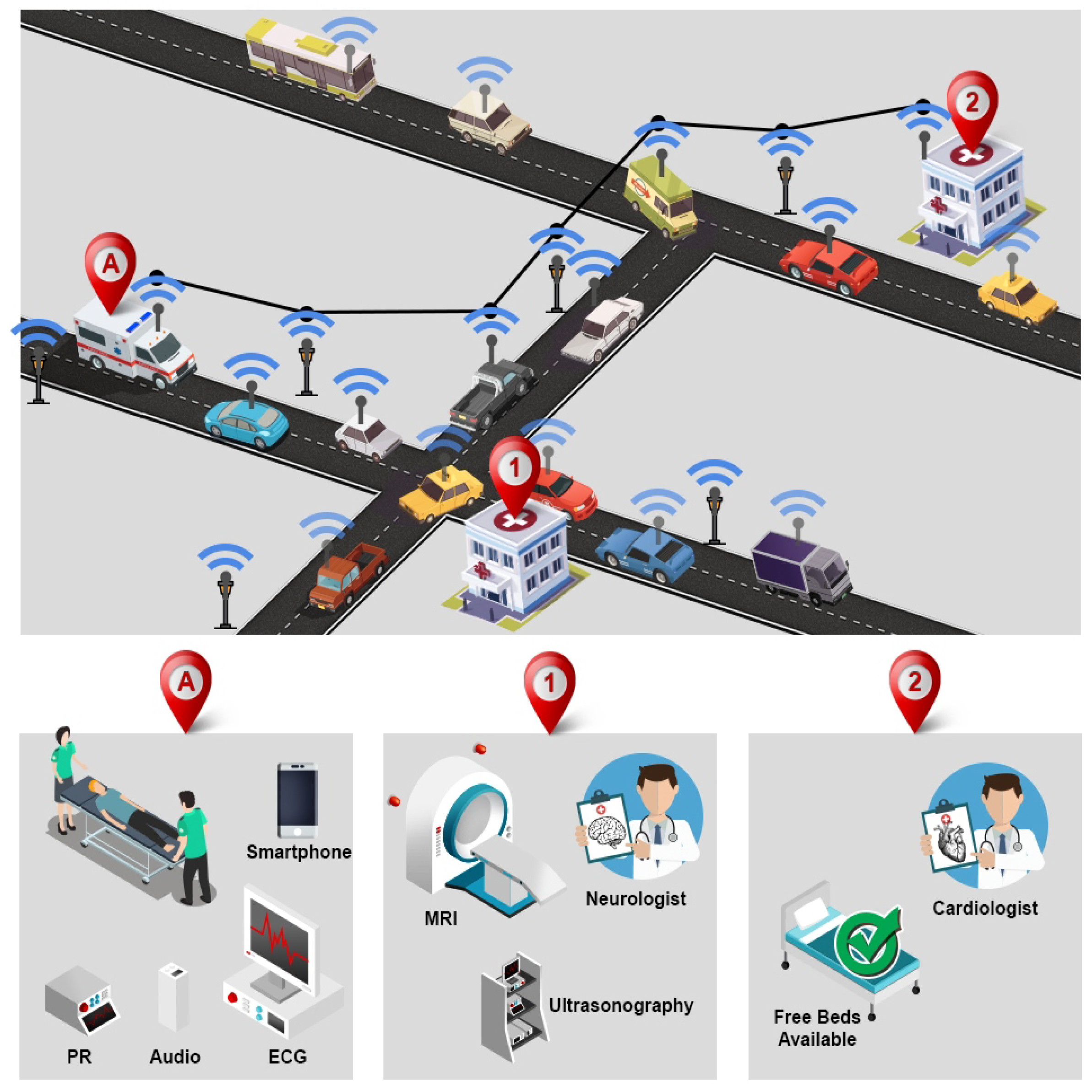
4. IoT-Enabled Traffic-Aware Telemedicine Architecture (ITTA)
4.1. IoT-Based Telemedicine Services Framework (ITSF)
4.2. Wearable-Device-Based Monitoring Algorithm for Edge Device (WDMA-Edge)
| Algorithm 1 Wearable- device-based monitoring algorithm for edge device (WDMA-Edge) |
|
4.3. Algorithm
4.4. Adaptive QoS-Aware Packet Transmission for Fog (AQPT-Fog)
| Algorithm 2 Adaptive QoS-Aware Packet Transmission for fog (AQPT-Fog) |
Input: data, route, link Output: packet
|
- Location-based services (LBS): GPS-based tracking and navigation assistance for ambulances can be of immense assistance to both ambulance operators as well as healthcare practitioners.
- Real-time health monitoring: Monitoring the dynamically changing health parameters of the patients being transported is necessary since the risk level of the patient will vary with the change in the level of vital parameters.
- Multi-level health risk assessments: Just as monitoring the vital parameters is important, it is equally important to ensure that the criticality or risk level of the patient is monitored.
- Data transmission from mobile ambulance: After measuring the level of vital parameters, it is necessary to transmit the same to the doctor at the remote hospital.
- QoS: While transmitting the data to the remote hospital, it is important to ensure that requisite QoS parameters are considered. Healthcare data, being very critical in nature, have stringent QoS parameters.
- Availability of V2V/V2I communication: During the data communication, as VANETs are considered in the current work, we verify what type of network topology is possible/available in the respective road link.
- Adaptive routing: Based on the type of network topology found on the road link, the routing protocol is selected dynamically.
- Cloud storage or processing: All the data need to be transmitted to the doctor in the remote hospital. However, since the doctor is not present on the same network, cloud storage is required as an intermediary. The processing of the criticality analysis is also performed on the cloud.
- Medical scoring for patients during transit: Categorizing the risk level of the patients cannot happen randomly and requires a methodical analysis. The same is also required for triaging of the patient.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Research Works | LBS | A | B | C | QoS | V2V/ V2I | D | E | F |
|---|---|---|---|---|---|---|---|---|---|
| [29] | ✔ | ✔ | ✔ | ||||||
| [48] | ✔ | ✔ | ✔ | ||||||
| [49] | ✔ | ✔ | |||||||
| [50] | |||||||||
| [30] | ✔ | ✔ | ✔ | ||||||
| [31] | ✔ | ✔ | ✔ | ||||||
| [51] | ✔ | ✔ | |||||||
| [52] | ✔ | ✔ | ✔ | ||||||
| ITTA | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
5. Simulation Study for Edge-to-Fog Communication Service Analysis
5.1. Simulation Scenarios
5.2. Experimental Design and Performance Analysis
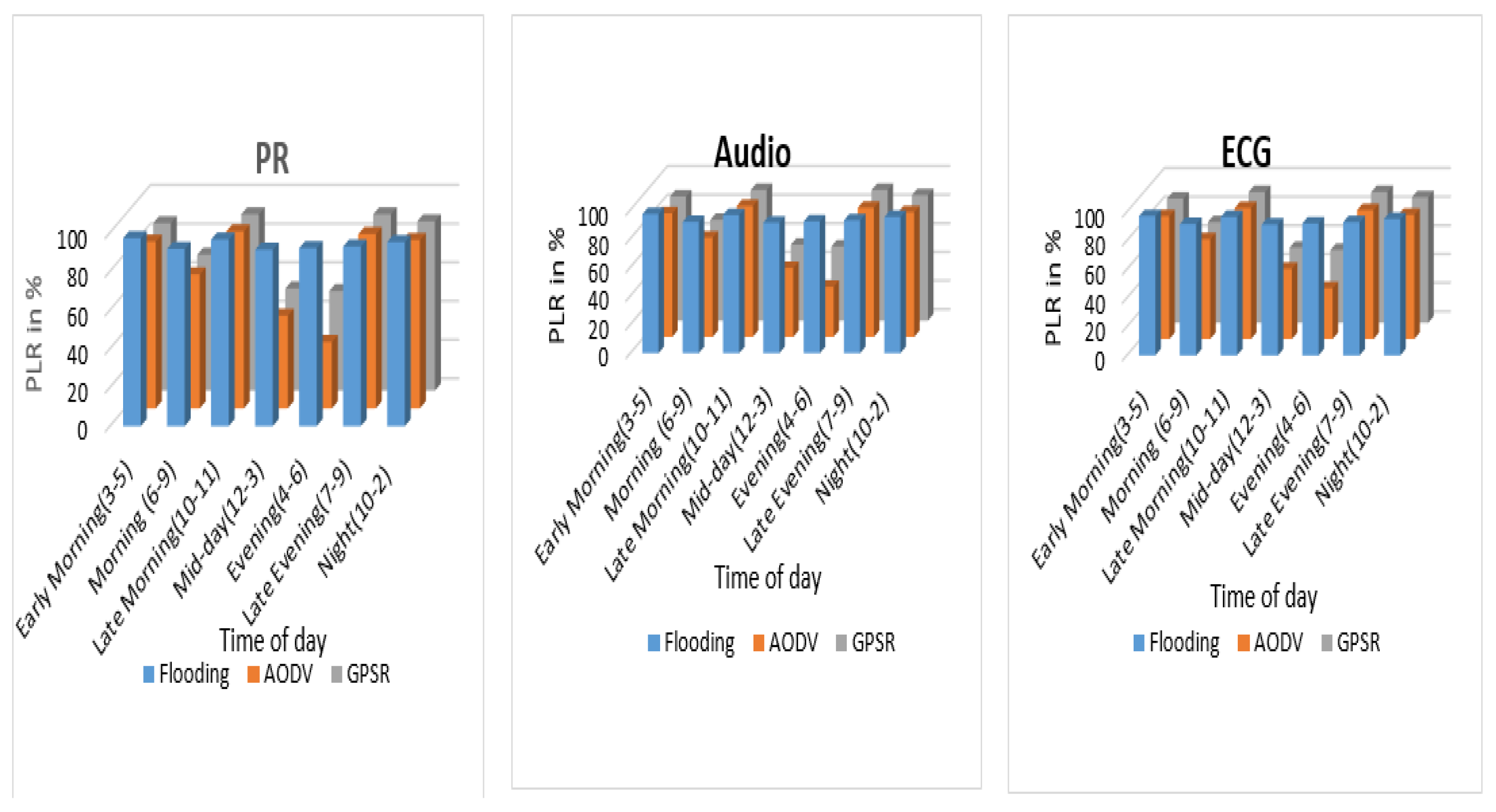
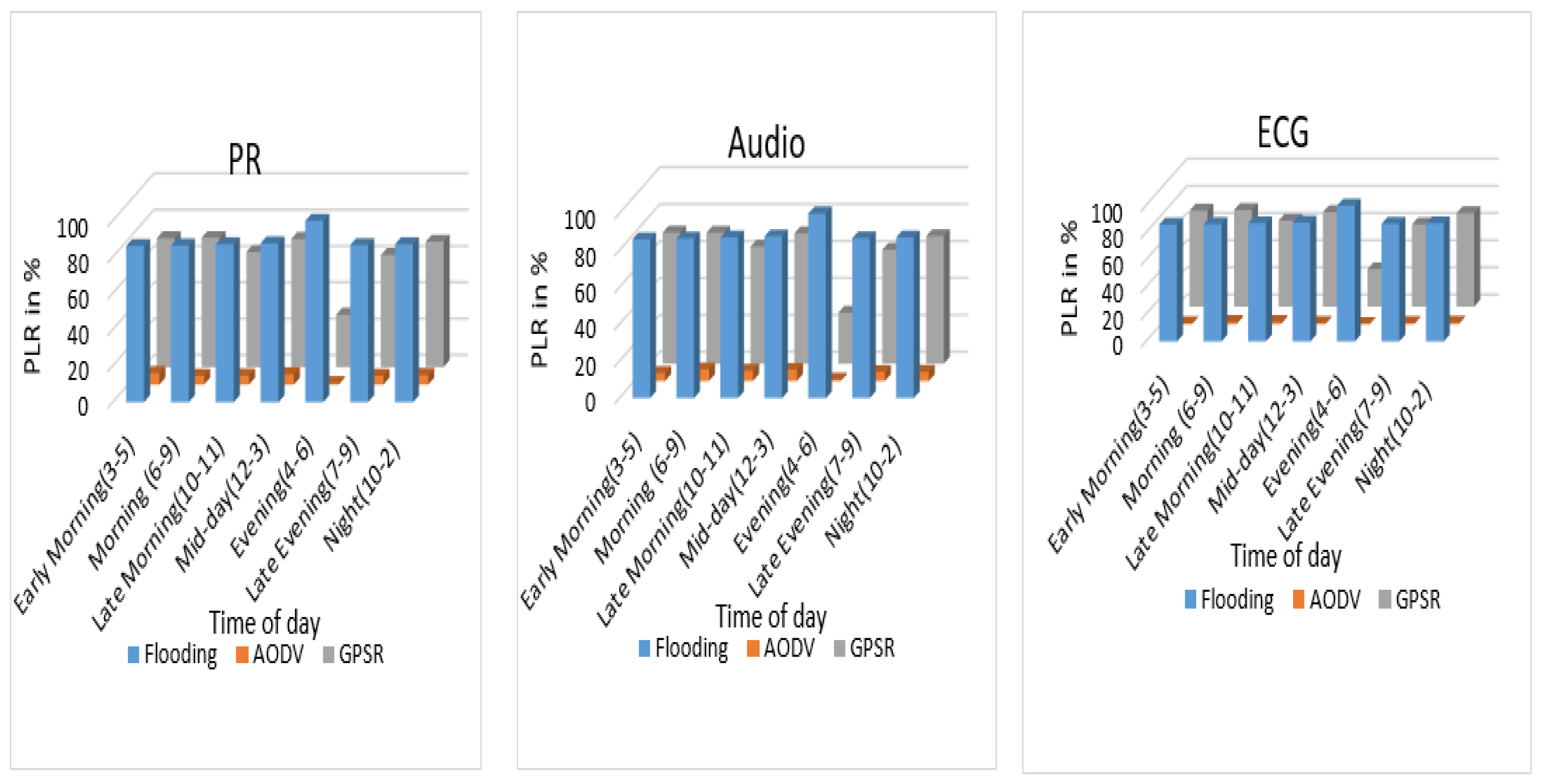
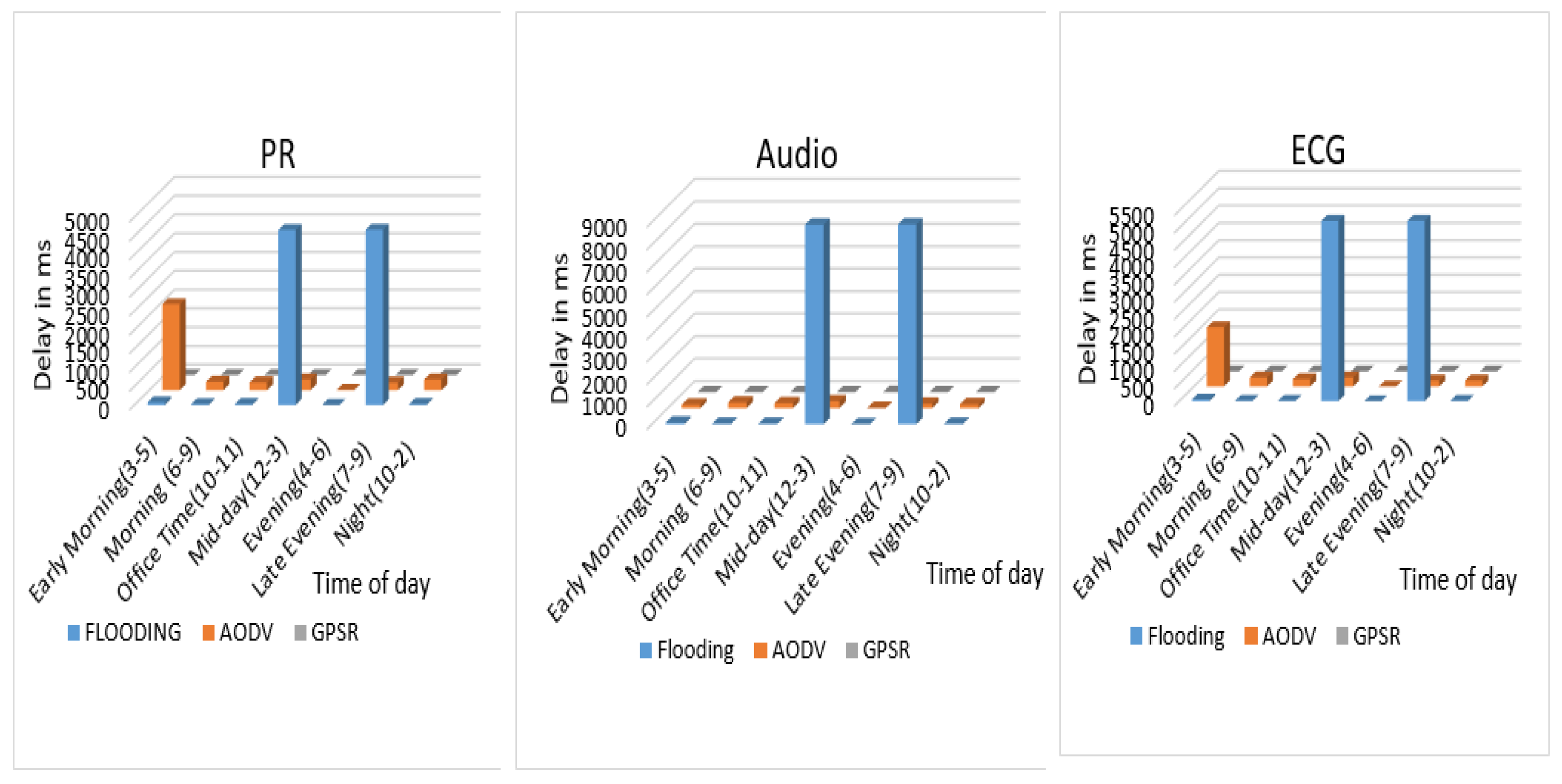
5.2.1. Performance Analysis of Healthcare VANET
5.2.2. Summary of Performance Analysis of Healthcare VANET
5.2.3. Performance Analysis of AQPT-Fog
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| IoT | Internet of Things |
| AODV | Ad Hoc On-demand Distance Vector |
| GPSR | Greedy Perimeter Stateless Routing |
| VANET | Vehicular Ad Hoc Network |
| QoS | Quality of Service |
| PLR | Packet Loss Ratio |
References
- Ting, D.S.W.; Carin, L.; Dzau, V.; Wong, T.Y. Digital technology and COVID-19. Nat. Med. 2020, 26, 459–461. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Murthy, S.; Webb, S. COVID-19: A novel coronavirus and a novel challenge for critical care. Intensive Care Med. 2020, 46, 833–836. [Google Scholar] [CrossRef]
- Smith, A.C.; Thomas, E.; Snoswell, C.L.; Haydon, H.; Mehrotra, A.; Clemensen, J.; Caffery, L.J. Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J. Telemed. Telecare 2020, 26, 309–313. [Google Scholar] [CrossRef]
- Istepanian, R.S.; Lacal, J.C. Emerging mobile communication technologies for health: Some imperative notes on m-health. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (IEEE Cat. No. 03CH37439), Cancun, Mexico, 17–21 September 2003; IEEE: New York, NY, USA, 2003; Volume 2, pp. 1414–1416. [Google Scholar]
- Chandwani, R.K.; Dwivedi, Y.K. Telemedicine in India: Current state, challenges and opportunities. Transform. Gov. People Process. Policy 2015, 9, 393–400. [Google Scholar] [CrossRef]
- Lee, J.S.; Su, Y.W.; Shen, C.C. A Comparative Study of Wireless Protocols: Bluetooth, UWB, ZigBee, and Wi-Fi. In Proceedings of the IECON 2007—33rd Annual Conference of the IEEE Industrial Electronics Society, Taipei, Taiwan, 5–8 November 2007; IEEE: New York, NY, USA, 2007; pp. 46–51. [Google Scholar] [CrossRef]
- Batistatos, M.C.; Tsoulos, G.V.; Athanasiadou, G.E.; Science, T. Mobile Telemedicine for Moving Vehicle Scenarios: Wireless Technology Options and Challenges. J. Netw. Comput. Appl. 2012, 35, 1140–1150. [Google Scholar] [CrossRef]
- Niyato, D.; Hossain, E.; Diamond, J. IEEE 802.16/WiMAX-based broadband wireless access and its application for telemedicine/e-health services. IEEE Wirel. Commun. 2007, 14, 72–83. [Google Scholar] [CrossRef]
- Mercer, T.R.; Salit, M. Testing at scale during the COVID-19 pandemic. Nat. Rev. Genet. 2021, 22, 415–426. [Google Scholar] [CrossRef]
- Wood, R.M.; McWilliams, C.J.; Thomas, M.J.; Bourdeaux, C.P.; Vasilakis, C. COVID-19 scenario modelling for the mitigation of capacity-dependent deaths in intensive care. Health Care Manag. Sci. 2020, 23, 315–324. [Google Scholar] [CrossRef]
- Subhan, I.; Jain, A. Emergency care in India: The building blocks. Int. J. Emerg. Med. 2010, 3, 207–211. [Google Scholar] [CrossRef]
- Das, S.; Desai, R. Emergence of {EMS} in India. Available online: https://www.jems.com/international/emergence-of-ems-in-india/ (accessed on 25 January 2024).
- Williams, T.A.; Tohira, H.; Finn, J.; Perkins, G.D.; Ho, K.M. The ability of early warning scores (EWS) to detect critical illness in the prehospital setting: A systematic review. Resuscitation 2016, 102, 35–43. [Google Scholar] [CrossRef]
- Droogh, J.M.; Smit, M.; Absalom, A.R.; Ligtenberg, J.; Zijlstra, J.G. Transferring the critically ill patient: Are we there yet? Crit. Care 2015, 19, 62. [Google Scholar] [CrossRef]
- Nasiri, S.; Sadoughi, F.; Tadayon, M.H.; Dehnad, A. Security requirements of internet of things-based healthcare system: A survey study. Acta Inform. Med. 2019, 27, 253. [Google Scholar] [CrossRef]
- Gupta, K. Mobile Internet Penetration in Rural India Is Just 18%: Report. 2004. Available online: https://www.livemint.com/Technology/OBZOWMvu6CXHMPCdplDYfM/Mobile-internet-penetration-in-rural-India-is-just-18-repo.html (accessed on 2 November 2022).
- Agarwal, S. Internet and Mobile Association of India: Internet Users in India Expected to Reach 500 Million by June: IAMAI—The Economic Times. 2018. Available online: https://economictimes.indiatimes.com/tech/internet/internet-users-in-india-expected-to-reach-500-million-by-june-iamai/articleshow/63000198.cms?from=mdr (accessed on 2 November 2022).
- Firstpost. Rural India Has a Mere 17 Percent Internet Penetration due to Challenges in Deployment of Fixed Broadband Networks: Report-Technology News, Firstpost. 2018. Available online: https://www.firstpost.com/tech/news-analysis/rural-india-has-a-mere-17-percent-internet-penetration-due-to-challenges-in-deployment-of-fixed-broadband-networks-report-4306853.html (accessed on 2 November 2022).
- Sondi, P.; Wahl, M.; Rivoirard, L.; Cohin, O. Performance Evaluation of 802.11p-Based Ad Hoc Vehicle-to-Vehicle Communications for Usual Applications Under Realistic Urban Mobility. Int. J. Adv. Comput. Sci. Appl. 2016, 7, 221–230. [Google Scholar] [CrossRef]
- Nedungadi, P.; Jayakumar, A.; Raman, R. Personalized Health Monitoring System for Managing Well-Being in Rural Areas. J. Med. Syst. 2018, 42, 22. [Google Scholar] [CrossRef]
- Misic, J.; Misic, V. Bridge performance in a multitier wireless network for healthcare monitoring. IEEE Wirel. Commun. 2010, 17, 90–95. [Google Scholar] [CrossRef]
- Pavlopoulos, S.; Kyriacou, E.; Berler, A.; Dembeyiotis, S.; Koutsouris, D. A novel emergency telemedicine system based on wireless communication technology—AMBULANCE. IEEE Trans. Inf. Technol. Biomed. 1998, 2, 261–267. [Google Scholar] [CrossRef]
- Jin, Z.; Chen, Y. Telemedicine in the cloud era: Prospects and challenges. arXiv 2015, arXiv:1011.1669v3. [Google Scholar] [CrossRef]
- Lee, S.; Lim, A. Reliability and performance of IEEE 802.11n for vehicle networks with multiple nodes. In Proceedings of the 2012 International Conference on Computing, Networking and Communications (ICNC), Maui, HI, USA, 30 January–2 February 2012; IEEE: New York, NY, USA, 2012; pp. 252–256. [Google Scholar] [CrossRef]
- Shivaldova, V.; Mecklenbrauker, C.F. Real-world measurements-based evaluation of IEEE 802.11p system performance. In Proceedings of the 2013 IEEE 5th International Symposium on Wireless Vehicular Communications (WiVeC), Dresden, Germany, 2–3 June 2013; IEEE: New York, NY, USA, 2013; pp. 1–5. [Google Scholar] [CrossRef]
- Bala, R.; Krishna, C.R. Scenario Based Performance Analysis of AODV and GPSR Routing Protocols in a VANET. In Proceedings of the 2015 IEEE International Conference on Computational Intelligence & Communication Technology, Ghaziabad, India, 13–14 February 2015; IEEE: New York, NY, USA, 2015; pp. 432–437. [Google Scholar] [CrossRef]
- Goel, N.; Sharma, G.; Dhyani, I. A study of position based VANET routing protocols. In Proceedings of the 2016 International Conference on Computing, Communication and Automation (ICCCA), Greater Noida, India, 29–30 April 2016; IEEE: New York, NY, USA, 2016; pp. 655–660. [Google Scholar] [CrossRef]
- Dinu, R.; Veeraragavan, A. Random parameter models for accident prediction on two-lane undivided highways in India. J. Saf. Res. 2011, 42, 39–42. [Google Scholar] [CrossRef]
- Sonnis, O.; Sunka, A.; Singh, R.; Agarkar, T. IoT based telemedicine system. In Proceedings of the 2017 IEEE International Conference on Power, Control, Signals and Instrumentation Engineering (ICPCSI), Chennai, India, 21–22 September 2017; IEEE: New York, NY, USA, 2017; pp. 2840–2842. [Google Scholar]
- Raj, S. An efficient IoT-based platform for remote real-time cardiac activity monitoring. IEEE Trans. Consum. Electron. 2020, 66, 106–114. [Google Scholar] [CrossRef]
- Pathinarupothi, R.K.; Durga, P.; Rangan, E.S. IoT-based smart edge for global health: Remote monitoring with severity detection and alerts transmission. IEEE Internet Things J. 2018, 6, 2449–2462. [Google Scholar] [CrossRef]
- Ghazal, T.M.; Hasan, M.K.; Alshurideh, M.T.; Alzoubi, H.M.; Ahmad, M.; Akbar, S.S.; Al Kurdi, B.; Akour, I.A. IoT for smart cities: Machine learning approaches in smart healthcare—A review. Future Internet 2021, 13, 218. [Google Scholar] [CrossRef]
- Selvaraj, S.; Sundaravaradhan, S. Challenges and opportunities in IoT healthcare systems: A systematic review. Appl. Sci. 2020, 2, 139. [Google Scholar] [CrossRef]
- Saeik, F.; Avgeris, M.; Spatharakis, D.; Santi, N.; Dechouniotis, D.; Violos, J.; Leivadeas, A.; Athanasopoulos, N.; Mitton, N.; Papavassiliou, S. Task offloading in Edge and Cloud Computing: A survey on mathematical, artificial intelligence and control theory solutions. Comput. Netw. 2021, 195, 108177. [Google Scholar] [CrossRef]
- Khaliq, K.A.; Chughtai, O.; Qayyum, A.; Pannek, J. An emergency alert system for elderly/special people using VANET and WBAN. In Proceedings of the 2017 13th International Conference on Emerging Technologies (ICET), Islamabad, Pakistan, 27–28 December 2017; IEEE: New York, NY, USA, 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Nasajpour, M.; Pouriyeh, S.; Parizi, R.M.; Dorodchi, M.; Valero, M.; Arabnia, H.R. Internet of Things for current COVID-19 and future pandemics: An exploratory study. J. Healthc. Inform. Res. 2020, 4, 325–364. [Google Scholar] [CrossRef]
- Kelly, J.T.; Campbell, K.L.; Gong, E.; Scuffham, P. The Internet of Things: Impact and implications for health care delivery. J. Med. Internet Res. 2020, 22, e20135. [Google Scholar] [CrossRef]
- Tamilselvi, V.; Sribalaji, S.; Vigneshwaran, P.; Vinu, P.; GeethaRamani, J. IoT based health monitoring system. In Proceedings of the 2020 6th International Conference on Advanced Computing and Communication Systems (ICACCS), Coimbatore, India, 6–7 March 2020; IEEE: New York, NY, USA, 2020; pp. 386–389. [Google Scholar]
- Ahmed, S.T.; Basha, S.M.; Ramachandran, M.; Daneshmand, M.; Gandomi, A.H. An Edge-AI enabled Autonomous Connected Ambulance Route Resource Recommendation Protocol (ACA-R3) for eHealth in Smart Cities. IEEE Internet Things J. 2023, 10, 11497–11506. [Google Scholar] [CrossRef]
- Bouras, M.A.; Lu, Q.; Dhelim, S.; Ning, H. A lightweight blockchain-based IoT identity management approach. Future Internet 2021, 13, 24. [Google Scholar] [CrossRef]
- Aung, N.; Zhang, W.; Dhelim, S.; Ai, Y. T-Coin: Dynamic traffic congestion pricing system for the Internet of Vehicles in smart cities. Information 2020, 11, 149. [Google Scholar] [CrossRef]
- Imhoff, B.F.; Thompson, N.J.; Hastings, M.A.; Nazir, N.; Moncure, M.; Cannon, C.M. Rapid Emergency Medicine Score (REMS) in the trauma population: A retrospective study. BMJ Open 2014, 4, e004738. [Google Scholar] [CrossRef]
- Mukhopadhyay, A.; Sreekumar, S.; Xavier, B.; Suraj, M. A cloud-based smartphone solution for transmitting bio-signals from an emergency response vehicle. In Research Anthology on Telemedicine Efficacy, Adoption, and Impact on Healthcare Delivery; IGI Global: Pennsylvania, PA, USA, 2021; pp. 429–446. [Google Scholar]
- Mukhopadhyay, A.; Nishin, S. An IoT and Smartphone-Based Real-Time Analysis on Pulse Rate and Spo2 using Fog-to-cloud Architecture. In Proceedings of the 2021 International Conference on Computer Communication and Informatics (ICCCI), Coimbatore, India, 27–29 January 2021; IEEE: New York, NY, USA, 2021; pp. 1–7. [Google Scholar]
- Mukhopadhyay, A.; Xavier, B.; Sreekumar, S.; Suraj, M. Real-time ecg monitoring over multi-tiered telemedicine environment using firebase. In Proceedings of the 2018 International Conference on Advances in Computing, Communications and Informatics (ICACCI), Bangalore, India, 19–22 September 2018; IEEE: New York, NY, USA, 2018; pp. 631–637. [Google Scholar]
- Mukhopadhyay, A. QoS based telemedicine technologies for rural healthcare emergencies. In Proceedings of the 2017 IEEE Global Humanitarian Technology Conference (GHTC), San Jose, CA, USA, 19–22 October 2017; IEEE: New York, NY, USA, 2017; pp. 1–7. [Google Scholar] [CrossRef]
- Skorin-Kapov, L.; Matijasevic, M. Analysis of QoS requirements for e-health services and mapping to evolved packet system QoS classes. Int. J. Telemed. Appl. 2010, 2010, 628086. [Google Scholar] [CrossRef]
- Devigayathri, P.; Varshini, R.A.; Pooja, M.; Subbulakshmi, S. Mobile ambulance management application for critical needs. In Proceedings of the 2020 Fourth International Conference on Computing Methodologies and Communication (ICCMC), Erode, India, 11–13 March 2020; IEEE: New York, NY, USA, 2020; pp. 319–323. [Google Scholar]
- Usman, M.A.; Philip, N.Y.; Politis, C. 5G enabled mobile healthcare for ambulances. In Proceedings of the 2019 IEEE Globecom Workshops (GC Wkshps), Waikoloa, HI, USA, 9–13 December 2019; IEEE: New York, NY, USA, 2019; pp. 1–6. [Google Scholar]
- Albahri, A.S.; Alwan, J.K.; Taha, Z.K.; Ismail, S.F.; Hamid, R.A.; Zaidan, A.; Albahri, O.S.; Zaidan, B.; Alamoodi, A.H.; Alsalem, M. IoT-based telemedicine for disease prevention and health promotion: State-of-the-Art. J. Netw. Comput. Appl. 2021, 173, 102873. [Google Scholar] [CrossRef]
- Cancela, J.; Pastorino, M.; Arredondo, M.T.; Hurtado, O. A telehealth system for Parkinson’s disease remote monitoring. The PERFORM approach. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; IEEE: New York, NY, USA, 2013; pp. 7492–7495. [Google Scholar]
- Lehocki, F.; Kossaczky, I.; Homola, M.; Skalicky, D.; Mydliar, M.; Thurzo, A. Yet another hypertension telehealth solution? The rules will tell you. In Proceedings of the 2014 IEEE Conference on Biomedical Engineering and Sciences (IECBES), Miri, Malaysia, 8–10 December 2014; IEEE: New York, NY, USA, 2014; pp. 510–515. [Google Scholar]
- Ftaimi, S.; Mazri, T. A comparative study of Machine learning algorithms for VANET networks. In Proceedings of the 3rd International Conference on Networking, Information Systems & Security, Marrakech, Morocco, 31 March–2 April 2020; pp. 1–8. [Google Scholar]
- Zhang, D.; Yu, F.R.; Yang, R. A machine learning approach for software-defined vehicular ad hoc networks with trust management. In Proceedings of the 2018 IEEE Global Communications Conference (GLOBECOM), Abu Dhabi, United Arab Emirates, 9–13 December 2018; IEEE: New York, NY, USA, 2018; pp. 1–6. [Google Scholar]
- Phull, N.; Singh, P.; Shabaz, M.; Sammy, F. Enhancing vehicular ad hoc networks’ dynamic behavior by integrating game theory and machine learning techniques for reliable and stable routing. Secur. Commun. Netw. 2022, 2022, 4108231. [Google Scholar] [CrossRef]
- Kandali, K.; Bennis, L.; El Bannay, O.; Bennis, H. An Intelligent Machine Learning Based Routing Scheme for VANET. IEEE Access 2022, 10, 74318–74333. [Google Scholar] [CrossRef]
- Dawood, A. Cars in Delhi Move at Highest Speed as Bengaluru and Kolkata Remain Slowest Moving Metros. Available online: https://www.scoopwhoop.com/news/cars-in-delhi-move-at-highest-speed-as-bengaluru-and-kolkata-remain-slowest-moving-metros/ (accessed on 6 February 2023).
- Yona, M.; Klein, I. Compensating for Partial Doppler Velocity Log Outages by Using Deep- Learning Approaches. In Proceedings of the 2021 IEEE International Symposium on Robotic and Sensors Environments (ROSE), Virtual, 28–29 October 2021; pp. 1–5. [Google Scholar] [CrossRef]
- Pulse Transit Time PPG Dataset v1.1.0. Available online: https://physionet.org/content/pulse-transit-time-ppg/1.1.0/ (accessed on 2 November 2022).
- Simultaneous Physiological Measurements with Five Devices at Different Cognitive and Physical Loads v1.0.2. Available online: https://physionet.org/content/simultaneous-measurements/1.0.2/ (accessed on 2 November 2022).
- Pattern Analysis of Oxygen Saturation Variability v1.0.0. Available online: https://physionet.org/content/osv/1.0.0/ (accessed on 2 November 2022).








| 6 | 5 | 4 | 3 | 2 | 1 | 0 | 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Systolic (mmHg) | ≥170 | 160–169 | 150–159 | 140–149 | 130–139 | 124–129 | 119–123 | 109–118 | 99–108 | 79–98 | 70–78 | 60–69 | 50–59 |
| Diastolic (mmHg) | >130 | 120–129 | 110–119 | 100–109 | 90–99 | 80–89 | 75–79 | 70–74 | 50–69 | 40–49 | 30–39 | 20–29 | <20 |
| Heart rate | 160–200 | 140–159 | 120–139 | 100–119 | 70–99 | ||||||||
| SPO2 (%) | <84 | 84–90 | 91–94 | ≥ 95 |
| Notation | Meaning |
|---|---|
| Sysi | Systolic score at ith instance |
| Diai | Diastolic score at ith instance |
| PRi | PR score at ith instance |
| Oxyi | Oxygen Saturation score at ith instance |
| RStoti | Total risk score at ith instance |
| RStot | Total risk score |
| RStot | Mean risk score |
| j | Total time instances of measuring values |
| A | denotes the received power |
| I | approximates the fading effect of each transmission channel |
| C | The power required to transmit each packet. |
| i | Data instance |
| Received signal strength | |
| N | Maximum nodes in the topology of the selected path |
| T | System throughput |
| S | Path selection parameter |
| Data Type | Required Data Rate | Max Delay Allowed | Maximum Packet Loss Allowed (%) |
|---|---|---|---|
| Voice | 4–25 Kbps | 150–400 ms | 3 |
| ECG | 24 Kbps | 1 s | 0 |
| PR | 2–5 Kbps | 1 s | 0 |
| BP | 2–5 Kbps | 1 s | 0 |
| Features | Simulation Parameter Specifics |
|---|---|
| Communication Technology | WiFi (802.11) |
| Length of Road Stretch | 6 km |
| Geographic and Spatial Division (km) | Rural-2, Sub Urban-2, Urban-2 |
| Temporal Slots | Details in Table 6 |
| Speed | 60 kmph (rural), 40 kmph (suburban), 20 kmph (urban) |
| QoS Parameters | Details in Table 3 |
| Inter-packet interval | 1 s/0.1 s |
| Data type and Packet Size in Bytes | PR—250; Audio—500; ECG—300 |
| Routing mechanisms | Flooding, AODV, GPSR |
| Time of Day | Rural | Suburban | Urban | Total (in 6 km) |
|---|---|---|---|---|
| Early Morning (3–5) | 8 | 28 | 68 | 104 |
| Morning (6–9) | 36 | 205 | 276 | 517 |
| Late Morning (10–11) | 28 | 164 | 176 | 368 |
| Mid-day (12–3) | 50 | 302 | 312 | 664 |
| Evening (4–6) | 60 | 324 | 342 | 726 |
| Late Evening (7–9) | 30 | 94 | 170 | 294 |
| Night (10–2) | 14 | 46 | 84 | 144 |
| Timings | Vehicular Density | PR | Audio | ECG | Total | ||||
|---|---|---|---|---|---|---|---|---|---|
| Low | High | Low | High | Low | High | Low | High | ||
| Early Morning | 104 | AODV (86%) | Flooding (97%) | AODV (86%) | Flooding (97% ) | GPSR (85%) | Flooding (97%) | AODV (86%) | Flooding (97%) |
| Morning | 517 | AODV (69%) | Flooding (91%) | AODV (69%) | Flooding (91%) | AODV (69%) | Flooding (91%) | AODV (69%) | Flooding (91%) |
| Late Morning | 368 | GPSR (91%) | Flooding (96%) | GPSR (91%) | Flooding (96%) | GPSR (91%) | Flooding (96%) | AODV and GPSR (91%) | Flooding (96%) |
| Mid-day | 664 | AODV (47%) | Flooding (91%) | AODV (48%) | Flooding (91%) | AODV (49%) | Flooding (91%) | AODV (47%) | Flooding (91%) |
| Evening | 726 | AODV (34%) | Flooding (92%) | AODV (34%) | Flooding (92%) | AODV (35%) | Flooding (92%) | AODV (34%) | Flooding (92%) |
| Late Evening | 294 | AODV (90%) | Flooding (92%) | AODV (90%) | Flooding (92%) | AODV (89%) | Flooding (92%) | AODV (90%) | Flooding (90%) |
| Night | 144 | AODV (87%) | Flooding (95%) | AODV (87%) | Flooding (95%) | AODV (86%) | Flooding (95%) | AODV (41%) | Flooding (89%) |
| Timings | Vehicular Density | PR | Audio | ECG | Total | ||||
|---|---|---|---|---|---|---|---|---|---|
| Low | High | Low | High | Low | High | Low | High | ||
| Early Morning | 104 | GPSR (1 ms) | Flooding (36 ms) | GPSR (1 ms) | Flooding (36 ms) | GPSR (1 ms) | Flooding (20 ms) | GPSR (1 ms) | Flooding (36 ms) |
| Morning | 517 | GPSR (1 ms) | Flooding (4653 ms) | GPSR (2 ms) | Flooding (8881 ms) | GPSR (1 ms) | Flooding (5209 ms) | GPSR (1 ms) | Flooding (4653 ms) |
| Late Morning | 368 | GPSR (1 ms) | Flooding (136 ms) | GPSR (1 ms) | Flooding (137 ms) | GPSR (1 ms) | Flooding (96 ms) | GPSR (1 ms) | Flooding (136 ms) |
| Mid-day | 664 | GPSR (15 ms) | Flooding (4632 ms) | GPSR (4 ms) | Flooding (8857 ms) | GPSR (13 ms) | Flooding (5206 ms) | GPSR (15 ms) | Flooding (4632 ms) |
| Evening | 726 | GPSR (3 ms) | AODV (343 ms) | GPSR (9 ms) | AODV (459 ms) | GPSR (5 ms) | AODV (5355 ms) | GPSR (3 ms) | AODV (343 ms) |
| Late Evening | 294 | AODV (16) | GPSR (7560 ms) | GPSR (1 ms) | Flooding (22 ms) | Flooding (12 ms) | GPSR (8252 ms) | GPSR (1 ms) | GPSR (8252 ms) |
| Night | 144 | GPSR (1 ms) | Flooding (65 ms) | GPSR (2 ms) | Flooding (66 ms) | GPSR (1 ms) | Flooding (46 ms) | GPSR (1 ms) | Flooding (65 ms) |
| Timings | Vehicular Density | PR | Audio | ECG | Total | ||||
|---|---|---|---|---|---|---|---|---|---|
| Low | High | Low | High | Low | High | Low | High | ||
| Early Morning | 104 | AODV (6%) | Flooding (86%) | AODV (4%) | Flooding (86%) | AODV (0.5%) | Flooding (86%) | AODV (0.5%) | Flooding (86%) |
| Morning | 517 | AODV (4%) | Flooding (86%) | AODV (6%) | Flooding (86%) | AODV (1%) | Flooding (86%) | AODV (1%) | Flooding (86%) |
| Late Morning | 368 | AODV (4%) | Flooding (87%) | AODV (5%) | Flooding (87%) | AODV (1%) | Flooding (87%) | AODV (1%) | Flooding (87%) |
| Mid-day | 664 | AODV (5%) | Flooding (87%) | AODV (6%) | Flooding (87%) | AODV (0.7%) | Flooding (87%) | AODV (0.7%) | Flooding (87%) |
| Evening | 726 | AODV (0.7%) | Flooding (100%) | AODV (0.7%) | Flooding (100%) | AODV (0.07%) | Flooding (100%) | AODV (0.07%) | Flooding (100%) |
| Late Evening | 294 | AODV (4%) | Flooding (86%) | AODV (4%) | Flooding (86%) | AODV (0.6%) | Flooding (86%) | AODV (0.6%) | Flooding (86%) |
| Night | 144 | AODV (5%) | Flooding (87%) | AODV (4%) | Flooding (87%) | AODV (0.8%) | Flooding (87%) | AODV (0.8%) | Flooding (87%) |
| Timings | Vehicular Density | PR | Audio | ECG | Total | ||||
|---|---|---|---|---|---|---|---|---|---|
| Low | High | Low | High | Low | High | Low | High | ||
| Early Morning | 104 | GPSR (1 ms) | AODV (2287 ms) | GPSR (2 ms) | AODV (158 ms) | GPSR (1 ms) | AODV (1707 ms) | GPSR (1 ms) | AODV (2287 ms) |
| Morning | 517 | GPSR (1 ms) | AODV (224 ms) | GPSR (2 ms) | AODV (252 ms) | GPSR (1 ms) | AODV (258 ms) | GPSR (1 ms) | AODV (258 ms) |
| Late Morning | 368 | GPSR (2 ms) | AODV (207ms) | GPSR (3 ms) | AODV (224 ms) | GPSR (1 ms) | AODV (209 ms) | GPSR (1 ms) | AODV (224 ms) |
| Mid-Day | 664 | GPSR (1 ms) | Flooding (4661 ms) | GPSR (2 ms) | Flooding (8887 ms) | GPSR (1 ms) | Flooding (5206 ms) | GPSR (1 ms) | Flooding (4661 ms) |
| Evening | 726 | GPSR (1 ms) | AODV (11 ms) | GPSR (8 ms) | AODV (12 ms) | GPSR (1 ms) | AODV (8 ms) | GPSR (1 ms) | AODV (12 ms) |
| Late Evening | 294 | GPSR (2 ms) | Flooding (4668 ms) | GPSR (3 ms) | Flooding (8891 ms) | GPSR (1 ms) | Flooding (5207 ms) | GPSR (1 ms) | Flooding (8891 ms) |
| Night | 144 | GPSR (1 ms) | AODV (282 ms) | GPSR (2 ms) | AODV (176 ms) | GPSR (1 ms) | AODV (175 ms) | GPSR (1 ms) | AODV (282 ms) |
| Patient | Systolic | Diastolic | HR | SpO2 | Patient Risk Score |
|---|---|---|---|---|---|
| patient1 | 120 | 92 | 72 | 98 | 2 |
| patient2 | 122 | 73 | 74 | 96 | 3 |
| patient3 | 133 | 76 | 80 | 96 | 2 |
| patient4 | 135 | 93 | 74 | 99 | 4 |
| patient5 | 80 | 55 | 75 | 98 | 5 |
| patient6 | 92 | 56 | 81 | 96 | 5 |
| patient7 | 100 | 73 | 85 | 95 | 3 |
| patient8 | 121 | 76 | 75 | 92 | 2 |
| patient9 | 132 | 75 | 112 | 96 | 4 |
| patient10 | 120 | 78 | 122 | 85 | 5 |
| Route | Links | V2V/V2I |
|---|---|---|
| r1 | l1.1, l1.3, l1.4 | V2V |
| l1.2 | V2V/V2I | |
| r2 | l2.1, l2.2 | V2V |
| l2.3 | V2V/V2I | |
| r3 | l3.1, l3.4, l3.5 | V2V |
| l3.2, l3.3, l3.6 | V2I | |
| r4 | l4.1 | V2I |
| l4.2 | V2V |
| Patient ID | Route | Links | V2V/V2I | Routing Protocol |
|---|---|---|---|---|
| patient1 | r3 | l3.1, l3.4, l3.5 | V2V | GPSR |
| l3.2, l3.3, l3.6 | V2I | AODV | ||
| patient2 | r1 | l1.1, l1.3, l1.4 | V2V | GPSR |
| l1.2 | V2I | AODV | ||
| patient3 | r3 | l3.1, l3.4, l3.5 | V2V | GPSR |
| l3.2, l3.3, l3.6 | V2I | AODV | ||
| patient4 | r1 | l1.1, l1.3, l1.4 | V2V | GPSR |
| l1.2 | V2I | AODV | ||
| patient5 | r4 | l4.1 | V2I | AODV |
| l4.2 | V2V | GPSR | ||
| patient6 | r4 | l4.1 | V2I | AODV |
| l4.2 | V2V | GPSR | ||
| patient7 | r1 | l1.1, l1.3, l1.4 | V2V | GPSR |
| l1.2 | V2I | AODV | ||
| patient8 | r3 | l l3.1, l3.4, l3.5 | V2V | GPSR |
| l3.2, l3.3, l3.6 | V2I | AODV | ||
| patient9 | r2 | l2.1, l2.2 | V2V | GPSR |
| l2.3 | V2I | AODV | ||
| patient10 | r4 | l4.1 | V2I | AODV |
| l4.2 | V2V | GPSR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mukhopadhyay, A.; Remanidevi Devidas, A.; Rangan, V.P.; Ramesh, M.V. A QoS-Aware IoT Edge Network for Mobile Telemedicine Enabling In-Transit Monitoring of Emergency Patients. Future Internet 2024, 16, 52. https://doi.org/10.3390/fi16020052
Mukhopadhyay A, Remanidevi Devidas A, Rangan VP, Ramesh MV. A QoS-Aware IoT Edge Network for Mobile Telemedicine Enabling In-Transit Monitoring of Emergency Patients. Future Internet. 2024; 16(2):52. https://doi.org/10.3390/fi16020052
Chicago/Turabian StyleMukhopadhyay, Adwitiya, Aryadevi Remanidevi Devidas, Venkat P. Rangan, and Maneesha Vinodini Ramesh. 2024. "A QoS-Aware IoT Edge Network for Mobile Telemedicine Enabling In-Transit Monitoring of Emergency Patients" Future Internet 16, no. 2: 52. https://doi.org/10.3390/fi16020052
APA StyleMukhopadhyay, A., Remanidevi Devidas, A., Rangan, V. P., & Ramesh, M. V. (2024). A QoS-Aware IoT Edge Network for Mobile Telemedicine Enabling In-Transit Monitoring of Emergency Patients. Future Internet, 16(2), 52. https://doi.org/10.3390/fi16020052