
Development of Co-Amorphous Systems for Inhalation Therapy—Part 1: From Model Prediction to Clinical Success †

 , , ,
, , ,
Abstract

1. Introduction
2. Material and Methods
2.1. Materials
2.2. Model Validation
2.3. Preparation of COAMS
2.4. Particle Characterization
2.4.1. Particle Size Measurements—LiteSizer
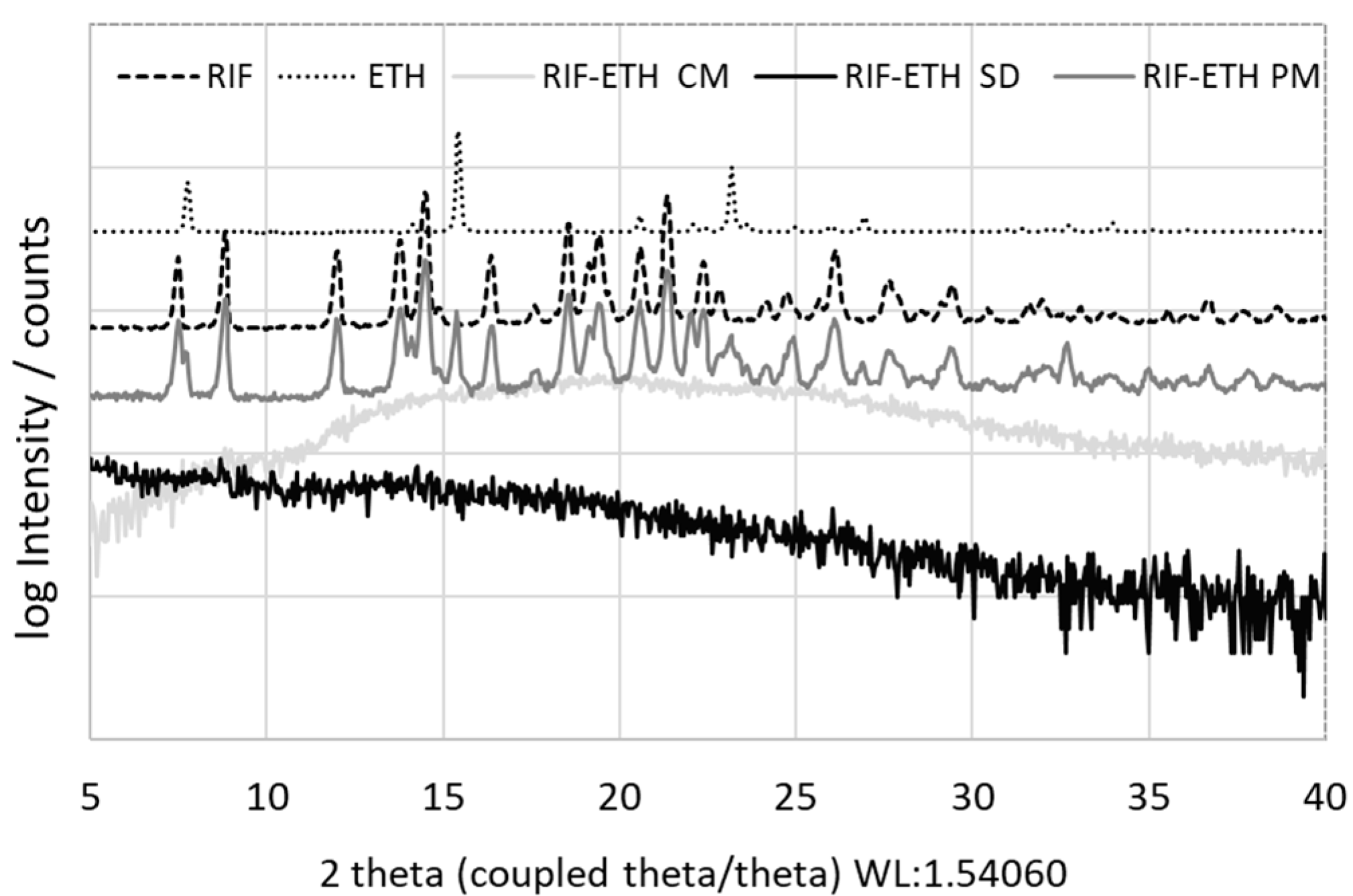
2.4.2. Solid-State—Powder X-Ray Diffraction (XRD) Measurements
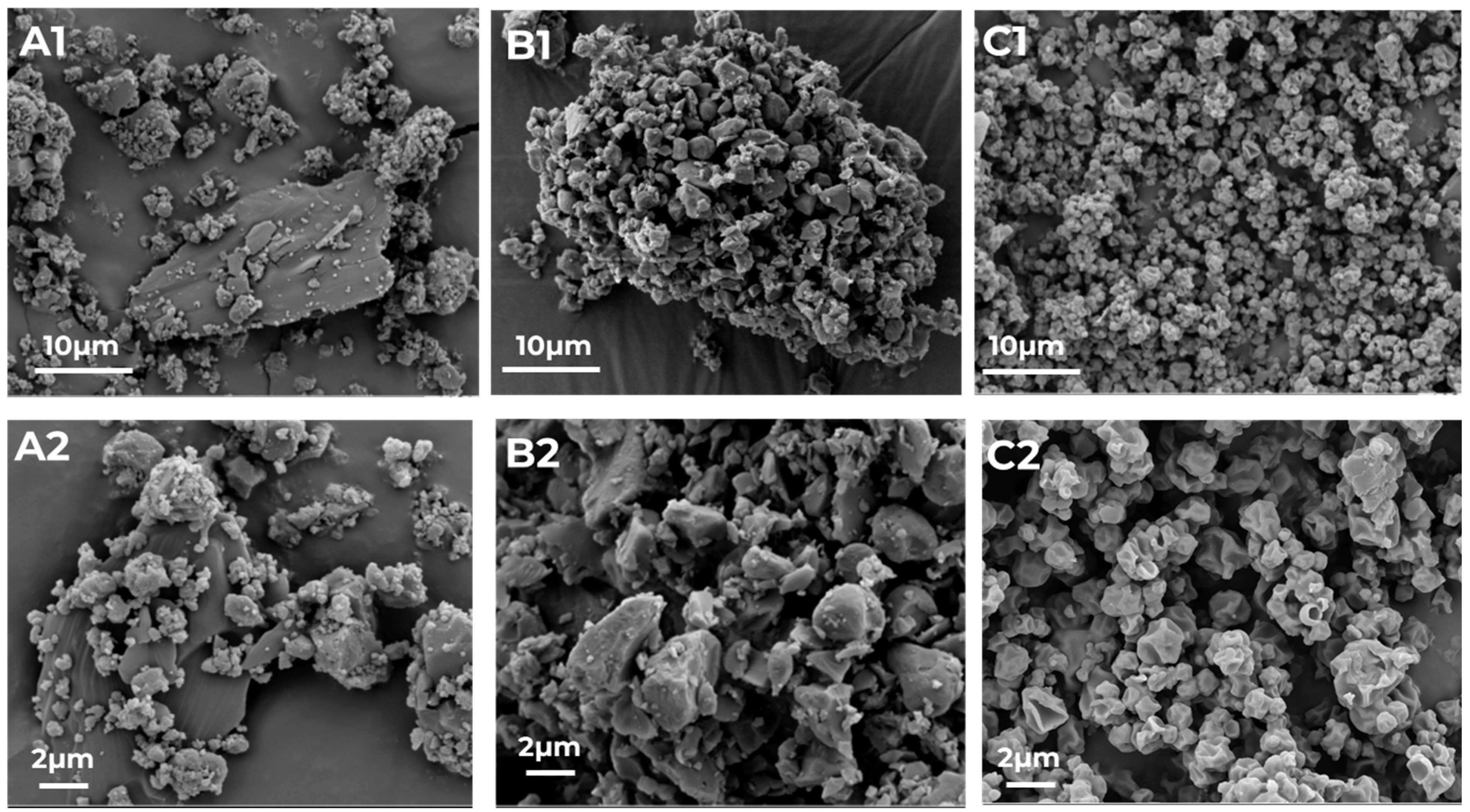
2.4.3. Particle Morphology—SEM Images
2.5. Formulation Preparation
2.6. Analytics
2.7. API Distribution/API Content
2.8. Aerosolization Performance
2.9. Dissolution
2.10. Stability Study
2.11. Statistical Analysis
3. Results and Discussion
3.1. Detailed Model Validation
3.2. Particle Characteristics
3.3. COAMS Stability
3.4. Particle Performance
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Javid, S.; Rahmanulla, A.; Ahmed, M.G.; sultana, R.; Prashantha Kumar, B.R. Machine Learning & Deep Learning Tools in Pharmaceutical Sciences: A Comprehensive Review. Intell. Pharm. 2025, 3, 167–180. [Google Scholar]
- Huanbutta, K.; Burapapadh, K.; Kraisit, P.; Sriamornsak, P.; Ganokratanaa, T.; Suwanpitak, K.; Sangnim, T. Artificial Intelligence-Driven Pharmaceutical Industry: A Paradigm Shift in Drug Discovery, Formulation Development, Manufacturing, Quality Control, and Post-Market Surveillance. Eur. J. Pharm. Sci. 2024, 203, 106938. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Ding, J.; Pan, L.; Cao, D.; Jiang, H.; Ding, X. Artificial Intelligence Facilitates Drug Design in the Big Data Era. Chemom. Intell. Lab. Syst. 2019, 194, 103850. [Google Scholar] [CrossRef]
- Rehman, A.U.; Li, M.; Wu, B.; Ali, Y.; Rasheed, S.; Shaheen, S.; Liu, X.; Luo, R.; Zhang, J. Role of Artificial Intelligence in Revolutionizing Drug Discovery. Fundam. Res. 2025, 5, 1273–1287. [Google Scholar] [CrossRef] [PubMed]
- Chopra, H.; Annu; Shin, D.K.; Munjal, K.; Priyanka; Dhama, K.; Emran, T.B. Revolutionizing Clinical Trials: The Role of AI in Accelerating Medical Breakthroughs. Int. J. Surg. 2023, 109, 4211–4220. [Google Scholar] [CrossRef] [PubMed]
- Serrano, D.R.; Luciano, F.C.; Anaya, B.J.; Ongoren, B.; Kara, A.; Molina, G.; Ramirez, B.I.; Sánchez-Guirales, S.A.; Simon, J.A.; Tomietto, G.; et al. Artificial Intelligence (AI) Applications in Drug Discovery and Drug Delivery: Revolutionizing Personalized Medicine. Pharmaceutics 2024, 16, 1328. [Google Scholar] [CrossRef] [PubMed]
- Pantanowitz, L.; Hanna, M.; Pantanowitz, J.; Lennerz, J.; Henricks, W.H.; Shen, P.; Quinn, B.; Bennet, S.; Rashidi, H.H. Regulatory Aspects of Artificial Intelligence and Machine Learning. Mod. Pathol. 2024, 37, 100609. [Google Scholar] [CrossRef] [PubMed]
- Ali, K.A.; Mohin, S.; Mondal, P.; Goswami, S.; Ghosh, S.; Choudhuri, S. Influence of Artificial Intelligence in Modern Pharmaceutical Formulation and Drug Development. Futur. J. Pharm. Sci. 2024, 10, 53. [Google Scholar] [CrossRef]
- Gilpin, L.H.; Bau, D.; Yuan, B.Z.; Bajwa, A.; Specter, M.; Kagal, L. Explaining Explanations: An Overview of Interpretability of Machine Learning. In Proceedings of the 2018 IEEE 5th International Conference on Data Science and Advanced Analytics (DSAA), Turin, Italy, 1–3 October 2018; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2018; pp. 80–89. [Google Scholar]
- Pillai, N.; Dasgupta, A.; Sudsakorn, S.; Fretland, J.; Mavroudis, P.D. Machine Learning Guided Early Drug Discovery of Small Molecules. Drug Discov. Today 2022, 27, 2209–2215. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Shah, M. Artificial Intelligence and Machine Learning in Drug Discovery and Development. Intell. Med. 2022, 2, 134–140. [Google Scholar] [CrossRef]
- Djuris, J.; Cirin-Varadjan, S.; Aleksic, I.; Djuris, M.; Cvijic, S.; Ibric, S. Application of Machine-Learning Algorithms for Better Understanding of Tableting Properties of Lactose Co-Processed with Lipid Excipients. Pharmaceutics 2021, 13, 663. [Google Scholar] [CrossRef] [PubMed]
- Jones-Salkey, O.; Windows-Yule, C.R.K.; Ingram, A.; Stahler, L.; Nicusan, A.L.; Clifford, S.; Martin de Juan, L.; Reynolds, G.K. Using AI/ML to Predict Blending Performance and Process Sensitivity for Continuous Direct Compression (CDC). Int. J. Pharm. 2024, 651, 123796. [Google Scholar] [CrossRef] [PubMed]
- Fröhlich, E.; Mercuri, A.; Wu, S.; Salar-Behzadi, S. Measurements of Deposition, Lung Surface Area and Lung Fluid for Simulation of Inhaled Compounds. Front. Pharmacol. 2016, 7, 181. [Google Scholar] [CrossRef] [PubMed]
- Fink, E.; Brunsteiner, M.; Mitsche, S.; Schröttner, H.; Paudel, A.; Zellnitz-Neugebauer, S. Data-Driven Prediction of the Formation of Co-Amorphous Systems. Pharmaceutics 2023, 15, 347. [Google Scholar] [CrossRef] [PubMed]
- National Asthma Council. Asthma Management Handbook; National Asthma Campaign: South Melbourne, Australia, 2013; Volume 53, ISBN 9788578110796. [Google Scholar]
- Global Initiative for Asthma. Global Innitiative for Asthma GINA-2024-Strategy-Report-24_05_22_WMS; Global Initiative for Asthma: Fontana, WI, USA, 2024. [Google Scholar]
- World Health Organization. Treatment of Tuberculosis; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- COPD Health Center. GOLD COPD Guidelines, Classifications, and Staging. 2025. Available online: http://www.webmd.com/lung/copd/gold-criteria-for-copd (accessed on 2 February 2025).
- Han, J.; Wei, Y.; Lu, Y.; Wang, R.; Zhang, J.; Gao, Y.; Qian, S. Co-Amorphous Systems for the Delivery of Poorly Water-Soluble Drugs: Recent Advances and an Update. Expert Opin. Drug Deliv. 2020, 17, 1411–1435. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Grohganz, H.; Löbmann, K.; Rades, T.; Hempel, N.J. Co-Amorphous Drug Formulations in Numbers: Recent Advances in Co-Amorphous Drug Formulations with Focus on Co-Formability, Molar Ratio, Preparation Methods, Physical Stability, in Vitro and in Vivo Performance, and New Formulation Strategies. Pharmaceutics 2021, 13, 389. [Google Scholar] [CrossRef] [PubMed]
- Tobin, E.H.; Tristram, D. Tuberculosis Overview. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar] [PubMed]
- Falzon, D.; Zignol, M.; Bastard, M.; Floyd, K.; Kasaeva, T. The Impact of the COVID-19 Pandemic on the Global Tuberculosis Epidemic. Front. Immunol. 2023, 14, 1234785. [Google Scholar] [CrossRef] [PubMed]
- Hickey, A.J.; Durham, P.G.; Dharmadhikari, A.; Nardell, E.A. Inhaled Drug Treatment for Tuberculosis: Past Progress and Future Prospects. J. Control. Release 2016, 240, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Misra, A.; Hickey, A.J.; Rossi, C.; Borchard, G.; Terada, H.; Makino, K.; Fourie, P.B.; Colombo, P. Inhaled Drug Therapy for Treatment of Tuberculosis. Tuberculosis 2011, 91, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Pham, D.-D.; Fattal, E.; Tsapis, N. Pulmonary Drug Delivery Systems for Tuberculosis Treatment. Int. J. Pharm. 2015, 478, 517–529. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Tucker, I.; Stewart, P. Inhaled Dry Powder Formulations for Treating Tuberculosis. Curr. Drug Deliv. 2015, 12, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Khadka, P.; Dummer, J.; Hill, P.C.; Katare, R.; Das, S.C. A Review of Formulations and Preclinical Studies of Inhaled Rifampicin for Its Clinical Translation. Drug Deliv. Transl. Res. 2023, 13, 1246–1271. [Google Scholar] [CrossRef] [PubMed]
- Courrier, H.M.; Butz, N.; Vandamme, T.F. Pulmonary Drug Delivery Systems: Recent Developments and Prospects. Crit. Rev. Ther. Drug Carr. Syst. 2002, 19, 425–498. [Google Scholar] [CrossRef] [PubMed]
- Healy, A.M.; Amaro, M.I.; Paluch, K.J.; Tajber, L. Dry Powders for Oral Inhalation Free of Lactose Carrier Particles. Adv. Drug Deliv. Rev. 2014, 75, 32–52. [Google Scholar] [CrossRef] [PubMed]
- Zellnitz, S.; Roblegg, E.; Pinto, J.; Fröhlich, E. Delivery of Dry Powders to the Lungs: Influence of Particle Attributes from a Biological and Technological Point of View. Curr. Drug Deliv. 2019, 16, 180–194. [Google Scholar] [CrossRef] [PubMed]
- Tamadondar, M.R.; Rasmuson, A. The Role of Fine Excipient Particles in Adhesive Mixtures for Inhalation. AIChE J. 2021, 67, e17150. [Google Scholar] [CrossRef]
- Radivojev, S.; Zellnitz, S.; Paudel, A.; Fröhlich, E. Searching for Physiologically Relevant in Vitro Dissolution Techniques for Orally Inhaled Drugs. Int. J. Pharm. 2018, 556, 45–56. [Google Scholar] [CrossRef] [PubMed]
- The United States Pharmacopeial Convention, General Chapter <711>: Dissolution; United States Pharmacopeia 47—National Formulary 42 (USP 47–NF 42): Rockville, MD, USA, 2024.
- Alderborn, G. Aulton’s Pharmaceutics, Chapter 30, Tablets and Compaction. In Aulton’s Pharmaceutics, the Design and Manufacture of Medicines; Elsevier: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Kissi, E.O.; Khorami, K.; Rades, T. Determination of Stable Co-Amorphous Drug–Drug Ratios from the Eutectic Behavior of Crystalline Physical Mixtures. Pharmaceutics 2019, 11, 628. [Google Scholar] [CrossRef] [PubMed]
- Chavan, R.B.; Thipparaboina, R.; Kumar, D.; Shastri, N.R. Co Amorphous Systems: A Product Development Perspective. Int. J. Pharm. 2016, 515, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Carter, H.E.; Clark, R.K.; Dickman, S.R.; Loo, Y.H.; Skell, P.S.; Strong, W.A. Isolation and Purification of Streptomycin. J. Biol. Chem. 1945, 160, 337–342. [Google Scholar] [CrossRef]
- Lu, W.; Rades, T.; Rantanen, J.; Yang, M. Inhalable Co-Amorphous Budesonide-Arginine Dry Powders Prepared by Spray Drying. Int. J. Pharm. 2019, 565, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Huntington, D.H. The Influence of the Spray Drying Process on Product Properties. Dry. Technol. 2004, 22, 1261–1287. [Google Scholar] [CrossRef]
- Liu, H.; He, Z.Z.; Yu, L.; Ma, J.; Jin, X.P. Improved Solubility and Stability of Rifampicin as an Inclusion Complex of Acyclic Cucurbit[n]Uril. J. Incl. Phenom. Macrocycl. Chem. 2021, 101, 111–120. [Google Scholar] [CrossRef]
- Meirelles, L.; Carazo, E.; Borrego-Sánchez, A.; Barbosa, R.; Moura, T.; Aguzzi, C.; Sainz-Diaz, C.I.; Viseras, C.; Raffin, F. Design and Characterization of a Tuberculostatic Hybrid Based on Interaction of Ethambutol with a Raw Palygorskite. Appl. Clay Sci. 2019, 181, 105213. [Google Scholar] [CrossRef]
- Simon, A.; Velloso-Junior, S.O.; Mesquita, R.D.; Fontao, A.P.G.A.; Costa, T.E.M.M.; Honorio, T.S.; Guimaraes, T.F.; Sousa, E.G.R.; Viçosa, A.L.; Sampaio, A.L.F.; et al. Development of Inhaled Moxifloxacin-Metformin Formulation as an Alternative for Pulmonary Tuberculosis Treatment. Int. J. Pharm. 2024, 666, 124740. [Google Scholar] [CrossRef] [PubMed]
- Nokhodchi, A.; Ghafourian, T. Future of Carrier-Free Dry Powder Inhaler Formulations. Pharm. Sci. 2024, 30, 279–281. [Google Scholar] [CrossRef]
- Kaialy, W. On the Effects of Blending, Physicochemical Properties, and Their Interactions on the Performance of Carrier-Based Dry Powders for Inhalation—A Review. Adv. Colloid Interface Sci. 2016, 235, 70–89. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Ema Guideline on the Pharmaceutical Quality of Inhalation and Nasal Medicinal Products; European Medicines Agency: Amsterdam, The Netherlands, 2024. [Google Scholar]
- Magramane, S.; Vlahović, K.; Gordon, P.; Kállai-Szabó, N.; Zelkó, R.; Antal, I.; Farkas, D. Inhalation Dosage Forms: A Focus on Dry Powder Inhalers and Their Advancements. Pharmaceuticals 2023, 16, 1658. [Google Scholar] [CrossRef] [PubMed]
- Steckel, H.; Mü, B.W. In Vitro Evaluation of Dry Powder Inhalers I: Drug Deposition of Commonly Used Devices. Int. J. Pharm. 1997, 154, 19–29. [Google Scholar] [CrossRef]
- Dengale, S.J.; Grohganz, H.; Rades, T.; Löbmann, K. Recent Advances in Co-Amorphous Drug Formulations. Adv. Drug Deliv. Rev. 2016, 100, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Takayama, T.; Kaneko, S.; Palanisamy, V.; Ono, M.; Titapiwatanakun, V.; Higashi, K.; Fukami, T. Physical Properties for Novel Cilostazol Co-Amorphous; Effect of Preparation Method and Molar Ratio on the Co-Amorphous. Chem. Pharm Bull. 2025, 73, 318–326. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| API 1 | API 2 | Prediction | Distance | Therapeutic Relevance | XRPD Results | Validation Success |
|---|---|---|---|---|---|---|
| MOM | BAM | 1 | 57 | IGC + LAMA | amorphous both | yes |
| SBS | RIF | 1 | 184 | amorphous both | yes | |
| RIF | GB | 1 | 253 | amorphous both | yes | |
| GB | STR | 1 | 411 | amorphous both | yes | |
| RIF | ETH | 1 | 361 | Two first-line drugs | amorphous both | yes |
| MOM | SBS | 1 | 117 | amorphous both | yes | |
| PYR | ISO | 1 | 55 | Two first-line drugs | crystalline both | no |
| MOM | GB | 0.98 | 58 | IGC + LABA | amorphous both | yes |
| RIF | PYR | 0.98 | 394 | Two first-line drugs | amorphous both | yes |
| BUD | GB | 0.98 | 74 | IGC + LABA | amorphous both | yes |
| ETH | PYR | 0.96 | 44 | Two first-line drugs | crystalline both | no |
| SBS | GB | 0.94 | 90 | amorphous both | yes | |
| ETH | ISO | 0.9 | 57 | Two first-line drugs | crystalline both | no |
| BAM | PYR | 0.26 | 78 | crystalline both | yes | |
| BAM | ISO | 0.22 | 65 | crystalline both | yes | |
| BUD | STR | 0.14 | 187 | amorphous STR | no | |
| MOM | STR | 0.12 | 212 | amorphous STR | no | |
| ETH | GB | 0 | 89 | crystalline both | yes |
| Formulation | D10 Intensity/µm | D50 Intensity/µm | D90 Intensity/µm | Undersize SPAN |
|---|---|---|---|---|
| RIF JM | 0.91 ± 0.51 | 1.49 ± 1.08 | 2.54 ± 1.30 | 1.08 ± 0.79 |
| ETH JM | 0.85 ± 0.46 | 1.38 ± 0.83 | 2.40 ± 1.23 | 2.01 ± 0.27 |
| RIF + ETH PM | 1.61 ± 0.48 | 2.13 ± 0.64 | 2.87 ± 0.82 | 0.94 ± 0.70 |
| RIF + ETH CM | 2.02 ± 0.48 | 2.78 ± 0.95 | 3.83 ± 1.04 | 0.71 ± 0.50 |
| RIF + ETH SD | 1.59 ± 0.50 | 2.01 ± 0.65 | 2.84 ± 0.86 | 0.85 ± 0.74 |
| Formulation | Mean Drug Content RIF/% | Mixing Homogeneity RIF/% | Mean Drug Content ETH/% | Mixing Homogeneity ETH/% |
|---|---|---|---|---|
| RIF + ETH PM | 104.7 | 6.0 | 81.2 | 10.2 |
| RIF + ETH CM | 96.8 | 4.5 | 96.2 | 1.6 |
| RIF + ETH SD | 96.1 | 2.3 | 92.0 | 3.6 |
| Formulation | EF RIF/% | FPM RIF/µg | FPF RIF/% |
|---|---|---|---|
| RIF + ETH PM | 72.7 ± 28.2 | 6291.3 ± 1522.0 | 48.78 ± 13.1 |
| RIF + ETH CM | 93.1 ± 2.0 | 5450.2 ± 214.2 | 38.54 ± 2.3 |
| RIF + ETH SD | 71.0 ± 11.8 | 3592.12 ± 705.8 | 32.38 ± 2.8 |
| Formulation | EF ETH/% | FPM ETH/µg | FPF ETH/% |
|---|---|---|---|
| RIF + ETH PM | 90.2 ± 0.5 | 3097.8 ± 210.4 | 40.46 ± 1.4 |
| RIF + ETH CM | 95.9 ± 0.6 | 3810.8 ± 224.4 | 40.20 ± 0.2 |
| RIF + ETH SD | 66.2 ± 14.9 | 1713.0 ± 629.8 | 38.27 ± 14.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fröhlich, E.; Bordoni, A.; Mohsenzada, N.; Mitsche, S.; Schröttner, H.; Zellnitz-Neugebauer, S. Development of Co-Amorphous Systems for Inhalation Therapy—Part 1: From Model Prediction to Clinical Success. Pharmaceutics 2025, 17, 922. https://doi.org/10.3390/pharmaceutics17070922
Fröhlich E, Bordoni A, Mohsenzada N, Mitsche S, Schröttner H, Zellnitz-Neugebauer S. Development of Co-Amorphous Systems for Inhalation Therapy—Part 1: From Model Prediction to Clinical Success. Pharmaceutics. 2025; 17(7):922. https://doi.org/10.3390/pharmaceutics17070922
Chicago/Turabian StyleFröhlich, Eleonore, Aurora Bordoni, Nila Mohsenzada, Stefan Mitsche, Hartmuth Schröttner, and Sarah Zellnitz-Neugebauer. 2025. "Development of Co-Amorphous Systems for Inhalation Therapy—Part 1: From Model Prediction to Clinical Success" Pharmaceutics 17, no. 7: 922. https://doi.org/10.3390/pharmaceutics17070922
APA StyleFröhlich, E., Bordoni, A., Mohsenzada, N., Mitsche, S., Schröttner, H., & Zellnitz-Neugebauer, S. (2025). Development of Co-Amorphous Systems for Inhalation Therapy—Part 1: From Model Prediction to Clinical Success. Pharmaceutics, 17(7), 922. https://doi.org/10.3390/pharmaceutics17070922