
Application of Natural Products in Neurodegenerative Diseases by Intranasal Administration: A Review


Abstract

1. Introduction
2. NDs
2.1. AD
2.2. PD
2.3. HD
2.4. Other NDs
3. Pathway of Drug Delivery via IN
4. IN of Natural Products for NDs Treatment
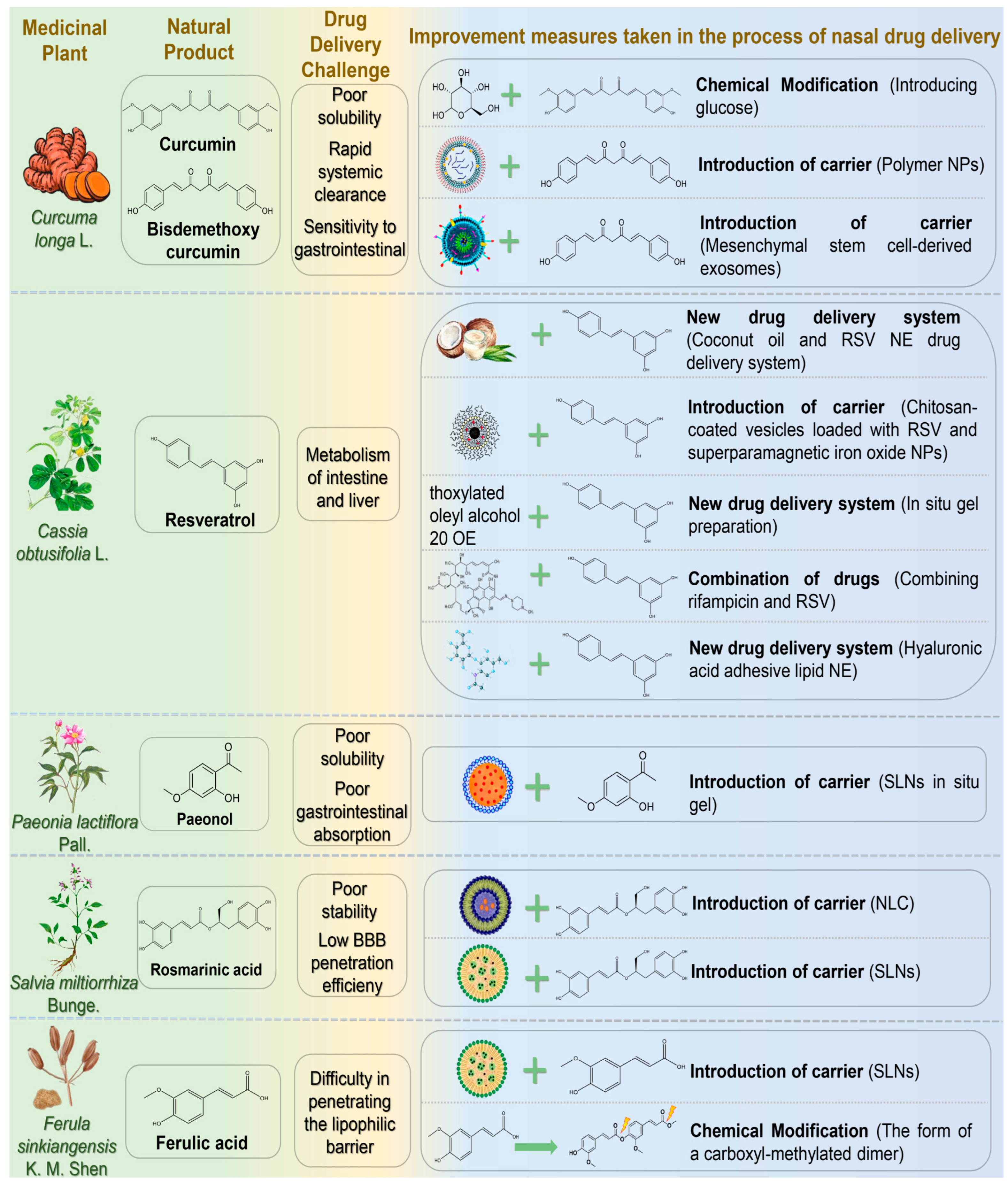
4.1. Phenols and Phenolic Acids
4.1.1. Curcumin
4.1.2. Resveratrol
4.1.3. Paeonol
4.1.4. Rosmarinic Acid
4.1.5. Ferulic Acid

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Natural Products | Diseases | Experimental Animal Model/Cell Model | Drug Delivery Systems | Formulation Optimization Effects | Pharmacological Effects | Reference |
|---|---|---|---|---|---|---|
| Curcumin | AD | Intraperitoneal injection of scopolamine induced AD in model rats | Curcumin α- and β-d-glucoside isomers | Glutathione and acetylcholine levels↑; Lipid peroxidation and protein carbonyl levels ↓ | [55] | |
| Mimicking mucin in amyloid peptide plaques | Curcumin/Demethoxycurcumin Polymer Nanoparticles | Good capture and released stability | Curcumin had a better affinity for pathological products | [56] | ||
| PD | in vitro: α-syn-mCherry overexpression in SH-SY5Y cells; in vivo: MPTP-induced PD rats | Exosome self-directed nanoparticles | Penetrates nasal mucosal barrier and cell membrane barrier ↑; Brain targeting ↑ | Aggregation of α-syn ↓; Neuronal synapse growth, remodelling and functional recovery ↑ | [57] | |
| Resveratrol | AD | in vitro: goat nasal mucosa; in vivo: rat | Coconut oil resveratrol nanoemulsion | in vitro drug release: 92.66 ± 3.45%; in vitro permeability of nasal mucosa: 88.54 ± 2.67%; AUC brain: 30,049.63 ± 1652.8; Cmax brain: 5762.30 ± 316.9 ng/mL | [62] | |
| AD model mice were induced by intracerebroventricular injection of lipopolysaccharide | Chitosan-coated RES and superparamagnetic iron oxide nanoparticle-loaded vesicles | Brain targeting ↑; Slow-release performance ↑, Extend resveratrol release for 24 h; Burst effect slightly decreased to 9.6% | Memory and cognitive function ↑; The levels of pro-inflammatory markers, NF-κB and p38 protein ↓; Improved the brain parenchyma and limited the activation of astrocytes in brain tissue. | [63] | ||
| Intracerebroventricular injection of streptozotocin induced an AD model in Swiss female mice | RES nasal in situ gelling system | Blocking property ↑ | Spatial memory level ↑; IL-1β, Neuroinflammation ↓ | [64] | ||
| APP-, tau-, and α-synuclein-transgenic mice | Combination drugs of rifampicin and resveratrol | Concentrations of brain-derived neurotrophic factor (BDNF) and its precursor, pro-BDNF, in hippocampus ↑; Rifampicin-induced liver injury ↓; Accumulation of amyloid oligomers ↓ | [65] | |||
| in vitro: sheep nasal mucosa; in vivo: rat | Hyaluronic acid-adhesive lipid NE encapsulating RSV and Curcumin | Nasal retention time ↑; Mucociliary clearance ↓; Stability of NE↑; AUCbrain increased 7 times | [66] | |||
| Paeonol | NDs | Goat nasal mucosa; RPMI2650 cells | Paeonol SLNs in situ gel | Nasal mucosa adhesion ↑; Nasal mucosa irritation ↓; Nasal-brain transport efficiency ↑; Sustained release capacity ↑ (72 h sustained release drug 64.89% ± 3.14%) | [70] | |
| Rosmarinic acid | AD | hCMEC/D3 cells | NLC carrying Rosmarinic acid | Drug sustained release time ↑; Transmembrane permeability in vitro ↑ | Antioxidant activity ↑ | [75] |
| HD | HD model rats induced by 3-nitropropionic acid | Rosmarinic acid SLNs | AUCbrain ↑; Duration of drug release ↑ (drug concentration is maintained to 14 h) | Lipid peroxidation, nitrite concentration ↓; antioxidant enzyme activity ↑ | [76] | |
| Ferulic acid | AD | Goat nasal mucosa; AD model rats were induced by streptozotocin injection | Ferulic acid-loaded chitosan-coated SLNs | In vitro mucosal adhesion and permeability ↑; the drug release rate in vitro increased to 72%; Brain drug levels ↑ | Improvement of cognitive ability ↑ | [80] |
| NDs | in vitro: PC12 cells; in vivo: rat | Dimeric ferulic acid conjugate as prodrug loaded ferulic acid solid lipid microparticles | The drug retention time in cerebrospinal fluid was prolonged and could be detected after 120 min; Bioavaolability ↑; Drug entering brain time was shortened, reaching Cmax in 20 min; The brain targeting was 7 times higher than monomer | [81] |
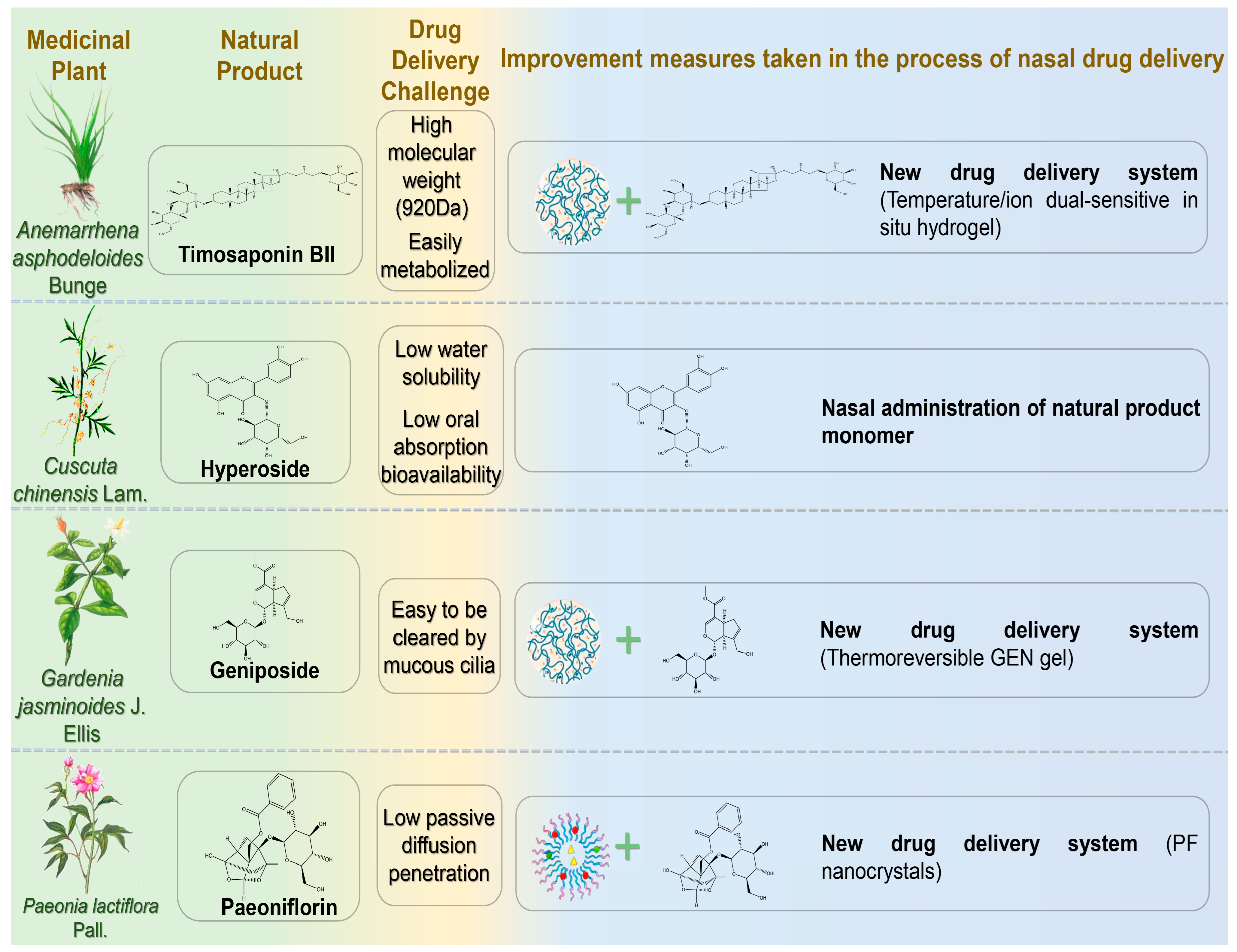
4.2. Glucosides
4.2.1. Timosaponin BII
4.2.2. Hyperoside
4.2.3. Geniposide
4.2.4. Paeoniflorin
| Natural Products | Diseases | Experimental Animal Model/Cell Model | Drug Delivery Systems | Formulation Optimization Effects | Pharmacological Effects | Reference |
|---|---|---|---|---|---|---|
| Timosaponin BII | AD | in vitro: Sheep nasal septum mucosa; Lipopolysaccharide damaged PC12 cells; in vivo: AD model mice were induced by injection of lipopolysaccharide | Temperature/ion sensitive in situ hydrogel of Timosaponin BII | Brain targeting ↑ (concentrated in brain at 5 min after IN, brain fluorescence intensity was the highest at 90 min after administration); Nasal mucosal retention time ↑ | iNOS ↓; Inflammatory cytokines TNF-α and IL-1β ↓ | [87] |
| Hyperin | APP/PSEN1 double transgenic AD mouse model | Hyperin | The drug elimination half-life was 7 times longer than that of intravenous administration (iv); Bioavaolability ↑ | Spatial learning and memory ability ↑; Aβ plaques and GFAP levels in cortex and hippocampus ↓ | [91] | |
| Geniposide | Goat nasal mucosa | Geniposide thermoreversible in situ gel | Nasal mucosa adhesion ↑; Nasal residence time ↑; Thermal reversibility ↑; The prescription drug content can reach 97 –101%; Gel strength 25–50 s | [95] | ||
| Paeoniflorin | PD | in vitro: porcine nasal mucosa; calu-3 cells; SH-SY5Y cells; in vivo: SD rats | Paeoniflorin nanocrystal preparation | AUCbrain ↑(AUCbrain 0–8h(IN)(230.86 ± 18.56 ng.h/g) > AUCbrain 0–8h(iv)(94.11 ± 10.37 ng.h/g)); Nasal permeability ↑; The cumulative release rate of the drug in 24 h: 87.14% ± 5.34%; Brain targeting ↑ (The Cmax IN (108.47 ± 9.51 ng/g) was significantly higher than that after IV (47.19 ± 5.69 ng/g)) | Neuroprotective effects ↑ | [98] |
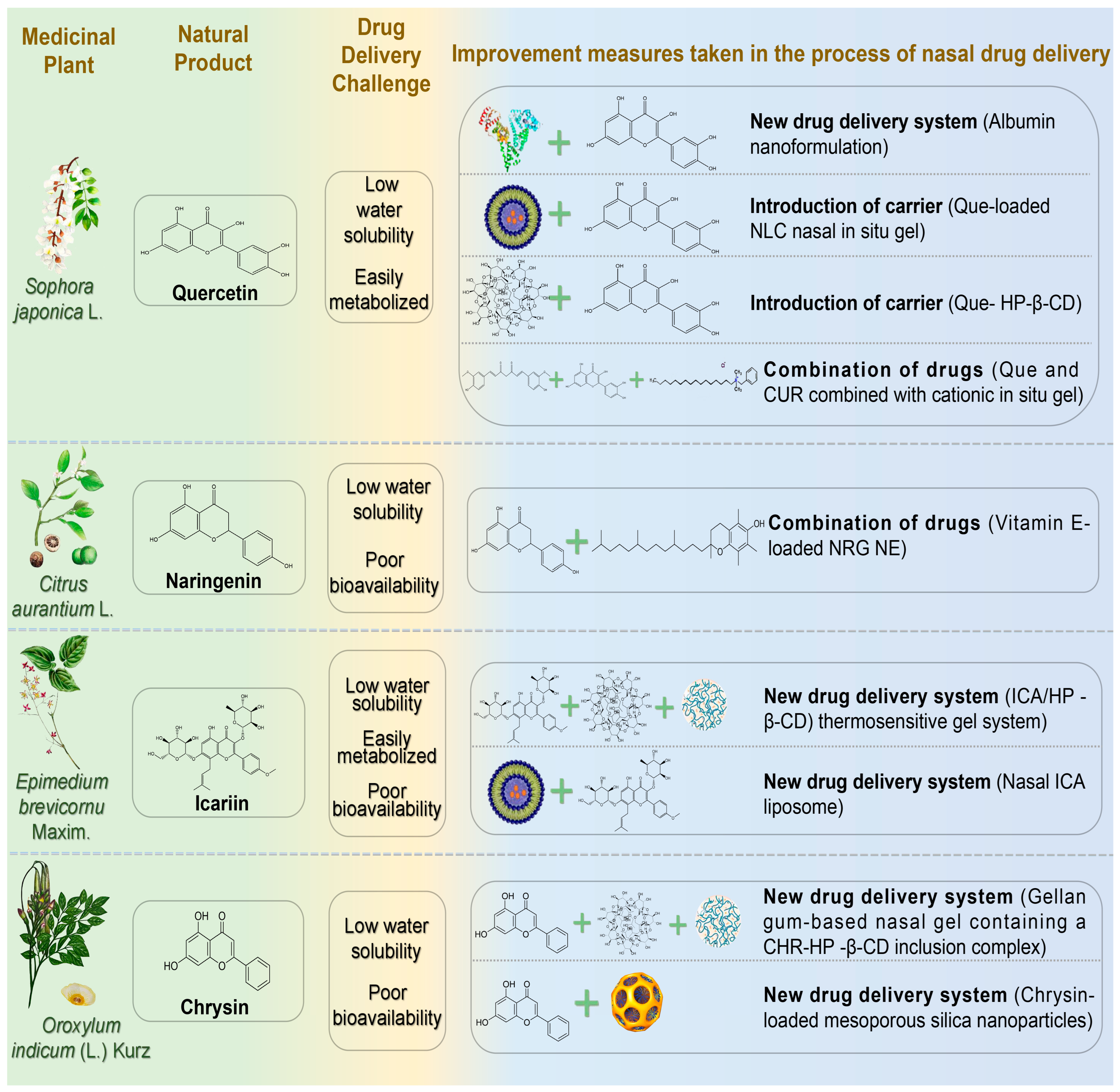
4.3. Flavonoids
4.3.1. Quercetin
4.3.2. Naringenin
4.3.3. Icariin
4.3.4. Chrysin
| Natural Products | Diseases | Experimental Animal Model/Cell Model | Drug Delivery Systems | Formulation Optimization Effects | Pharmacological Effects | Reference |
|---|---|---|---|---|---|---|
| Quercetin | AD | in vitro: H2O2-induced oxidative damage in PC12 cells; in vivo: APP/PS1 AD model mice | Que-coated human serum albumin NPs | Sustained release capacity ↑ (24 h can reach 99% release rate) | Oxidative stress ↓; Aβ aggregation ↓; Neuronal apoptosis ↓; synaptic damage in brain ↓ | [103] |
| in vitro: Goat nasal mucosa; in vivo: Trimethyltin-induced NDs rats | Quercetin NLC in situ gel | Brain targeting ↑ (drug targeting efficiency: 117.47%); Brain drug accumulation ↑ (Cmax: 183.41 ± 11.76 ng/mL); In vitro drug release ↑ (in vitro drug release rate: 83.74 ± 1.40%); Drug solubility ↑; Nasal mucosal retention time ↑ | [104] | |||
| Rabbit nasal mucosa | β-cyclodextrin derivative Que inclusion complex | The solubility of Que was 50 times higher than monomer; Nasal mucosal barrier permeability ↑ | [105] | |||
| NDs | RPMI2650 cells | Quercetin NE | Drug loading ↑; Gel-modified NE particle size increased to 244 nm, the entrapment efficiencyvalues were higher than 99%; Stability ↑ | Antioxidant activity ↑ | [106] | |
| Naringenin | PD | in vitro: Goat nasal mucosa; in vivo: 6-OHDA-induced PD rat model | Vitamin E-loaded naringenin NE | The drug release rate was 3 times higher than monomer; The permeability of nasal mucosa increased by 3 times; Cbrain↑ (394.33 ± 80.83 ng/mL); Brain bioavailability: 334.20 ± 8.91% | Antioxidant activity ↑ | [109] |
| Icariin | PD | Paraquat-induced PD mouse model | Icariin/hydroxypropyl-β-cyclodextrin inclusion complex controlled-release thermosensitive gel | Duration of drug release ↑ (the cumulative release of 24 h reached 98.64 ± 1.08%); Drug stability, solubility ↑; Bioavailability, brain targeting ↑ | Antioxidant activity ↑ | [113] |
| 6-OHDA-induced PD rat model | Icariin liposome | Necrosis and apoptosis of dopaminergic neurons in substantia nigra ↓ | [114] | |||
| Chrysin | PD | Sheep nasal mucosa; SH-SY5Y cell model induced by H2O2 | Gellan gum nasal gel loaded with chrysin/HP-β-CD inclusion complex | Sustained release capacity ↑ (12 h can reach 78.27 ± 3.81% accumulated release rate); The permeability of nasal mucosa ↑ (accumulative permeability reached 78.73 ± 0.37%); Stability ↑ (The drug content remained 97.49 ± 0.34% within 3 months) | Cell viability ↑ (p < 0.05); Superoxide dismutase (SOD) enzymatic activity ↑ | [119] |
| NDs | OBGF400cells | mesoporous silica nanoparticles based delivery system | Drug loading ↑ (11.49 ± 1.19% w/w); PH-responsive sustained release; Stability ↑ | Regulating oxidative stress pathway; cytotoxicity ↓ | [120] |
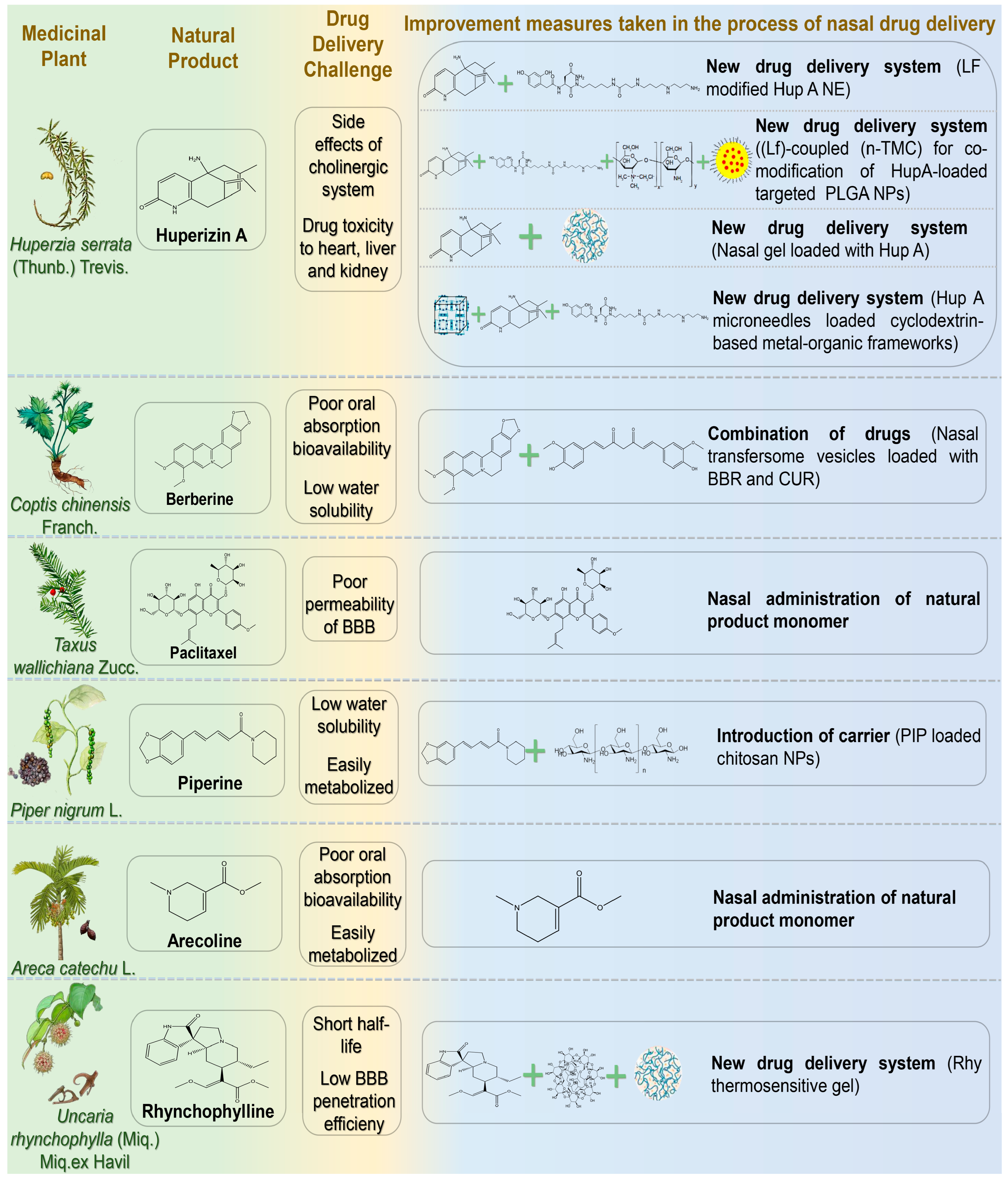
4.4. Alkaloid
4.4.1. Huperizin A
4.4.2. Berberine
4.4.3. Paclitaxel
4.4.4. Piperine
4.4.5. Arecoline
4.4.6. Rhynchophylline
| Natural Products | Diseases | Experimental Animal Model/Cell Model | Drug Delivery Systems | Formulation Optimization Effects | Pharmacological Effects | Reference |
|---|---|---|---|---|---|---|
| Huperzine A | AD | in vitro: Human cerebral microvascular endothelial cells/D3; in vivo: Wistar rats | LF modified Hup A NE | Drug solubility ↑; Stability ↑; Sustained release capacity ↑ (24 h release rate of 85%); Brain targeting ↑ (Drug targeting indexes (DTI) in brain (3.2 ± 0.75) showed effective targeting) | [124] | |
| in vitro: Human bronchial epithelial cell line 16HBE cells and SH-SY5Y cells; in vivo: Kunming mice | LF-coupled n-TMC was used to co-modify targeted PLGA NPs loaded with Hup A | Sustained release ability ↑ (48 h release rate: 74.5% ± 4.5%); Adhesion ↑ (the adhesion of NPs modified by TMC increased by nearly three times); Brain targeting ↑; Cytotoxicity ↓ | [125] | |||
| in vitro: SH-SY5Y cells in vivo: APP/PS1 double transgenic mice | Hup A nasal gel | Antioxidant enzyme activity ↑; Inhibition of acetylcholinesterase activity ↑; Aβ aggregation ↓ | [126] | |||
| in vitro: 16HBE cells, PC12 cells; Pig nasal mucosa; in vivo: AD model rats induced by hyoscyamine and d-galactose | Cyclodextrin-based metal-organic framework-mediated Hup A nanomicroneedles | Administration time ↓; Physical stability ↑; Nasal mucosal penetration ability ↑ (the amount of nasal penetration of the drug was 1.7 times higher than free); Brain uptake rate ↑; Brain targeting ↑ | Neuronal cell injury ↓; Spatial memory improvement ability ↑ | [127] | ||
| Berberine | AD | AD mice were induced by intranasal administration of scopolamine | Nasal transfersome vesicles loaded with berberine and curcumin | Sustained release ability ↑ (60 h release saturation); Hemolytic toxicity ↓; The average residence time in brain was 7 times than pure drug group | Inhibition of Acetylcholinesterase ↑; Spatial memory improvement ability ↑; Antioxidant enzyme activity ↑ | [132] |
| Paclitaxel | AD | in vitro: Primary hippocampal neurons of E18 embryonic rats; in vivo: 3XTg-AD mice; | Paclitaxel | AD model mice cognitive impairment ↓; Hyperphosphorylation of tau protein and abnormal proliferation of glial cells ↓; Axonal transport in body ↑ | [135] | |
| Piperine | AD | Intraventricular injection of colchicine-induced SD model rats | PIP-loaded chitosan NPs | Brain targeting ↑; Nasal mucosa irritation ↓; The dose was reduced by 20 times compared with oral administration ↓; Sustained release time ↑ (24 h cumulative release rate of 92%) | Acetylcholinesterase inhibition and antioxidant effect ↑ | [139] |
| Arecoline | AD | Male Lewis rats | Arecoline | Drug absorption rate ↑ (t = 3 ± 1.6 min); Drug elimination half-life ↑ | [143] | |
| Rhynchophylline | PD | in vitro: SH-SY5Y cells; in vivo: MPTP+ induced PD model mice | Rhy thermosensitive gel | Nasal mucosal permeability ↑; Nasal mucosa adhesion ↑; Slow-release performance ↑; Bioavailability ↑; Brain targeting ↑ (DTI is 2.1 times higher than oral administration) | Abnormal expression of oxidative stress factors, neurons positive damage, and dopamine in substantia nigra ↓ | [146] |
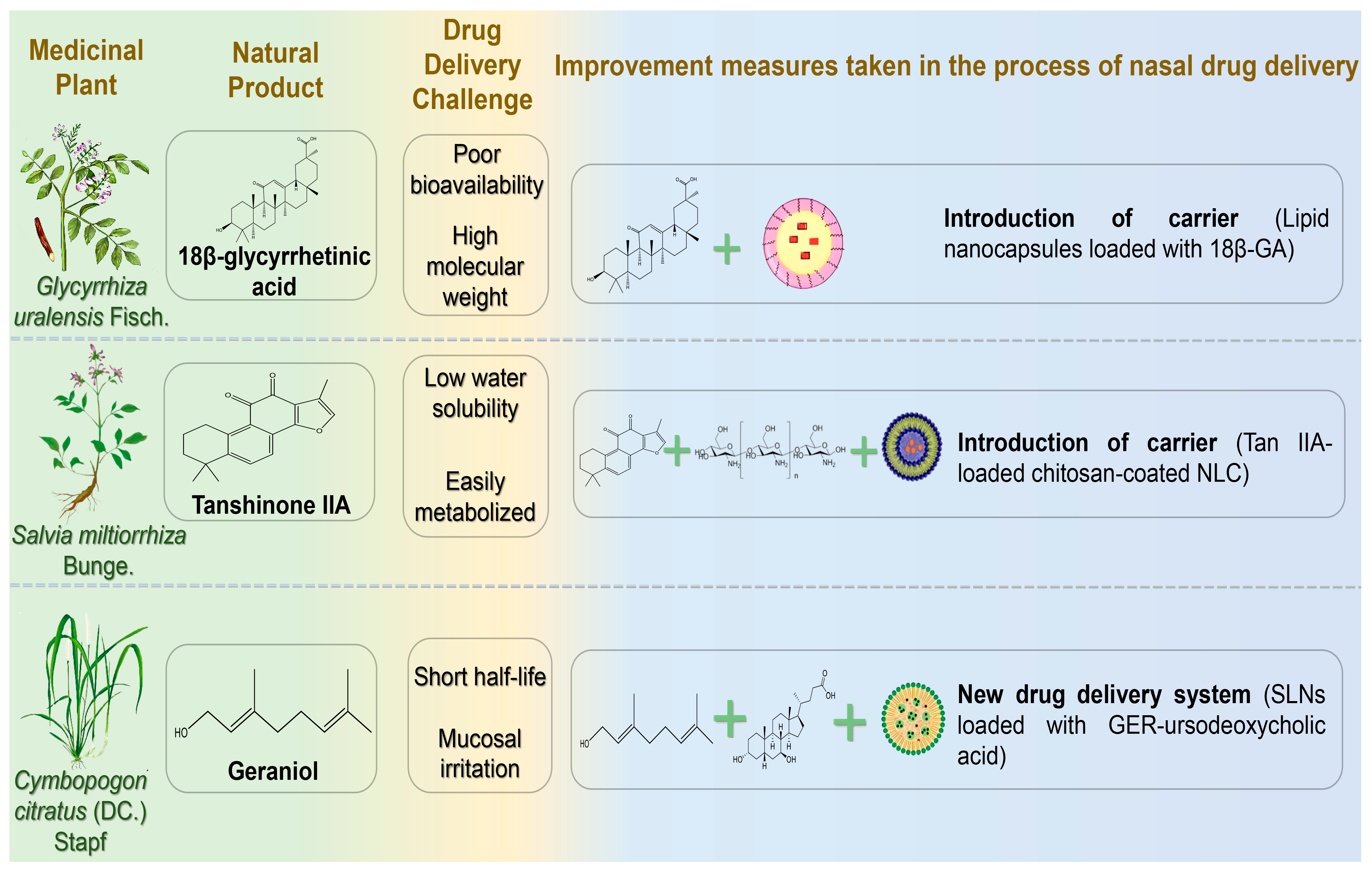
4.5. Terpenoids
4.5.1. 18β-Glycyrrhetinic Acid
4.5.2. Tanshinone IIA
4.5.3. Geraniol
| Natural Products | Diseases | Experimental Animal Model/Cell Model | Drug Delivery Systems | Formulation Optimization Effects | Pharmacological Effects | Reference |
|---|---|---|---|---|---|---|
| 18β-glycyrrhetinic acid | AD | in vitro: Sheep nasal mucosa; in vivo: scopolamine-induced AD model Wister mice | LNCs coated with 18β-glycyrrhetinic acid | Nasal mucosal permeability ↑; Drug sustained release time 24 h ↑; Brain bioavailability ↑; Nasal brain targeting ↑ | [150] | |
| Tanshinone IIA | PD | Rotenone-induced PD rat model | Tan IIA chitosan-coated nano-lipid carrier | Drug solubility ↑; Drug sustained release time 24 h ↑; Nasal mucosal retention time ↑; Brain targeting ↑ | Anti-PD activity ↑ (striatal dopamine level ↑; Neuroinflammation and oxidative stress level ↓) | [153] |
| Geraniol | PD | in vitro: Nasal mucosa of Wistar rats; in vivo: SD rats | Geraniol β-cyclodextrin/hydroxypropyl β-cyclodextrin inclusion complex | Drug solubility ↑ (HP-β-CDs increased the solubilization of GER nearly threefold to 14.73 ± 0.07); Drug stability ↑; Nasal mucosal penetration ability ↑; Brain targeting ↑ (C(CSF)GER-HP-β-CD: 1.25 ± 0.03~0.26 ± 0.03 μg/mL; C(CSF)GER-β-CD: 119.0 ± 8.6 to 12.6 ± 3.3 μg/mL) | [157] |
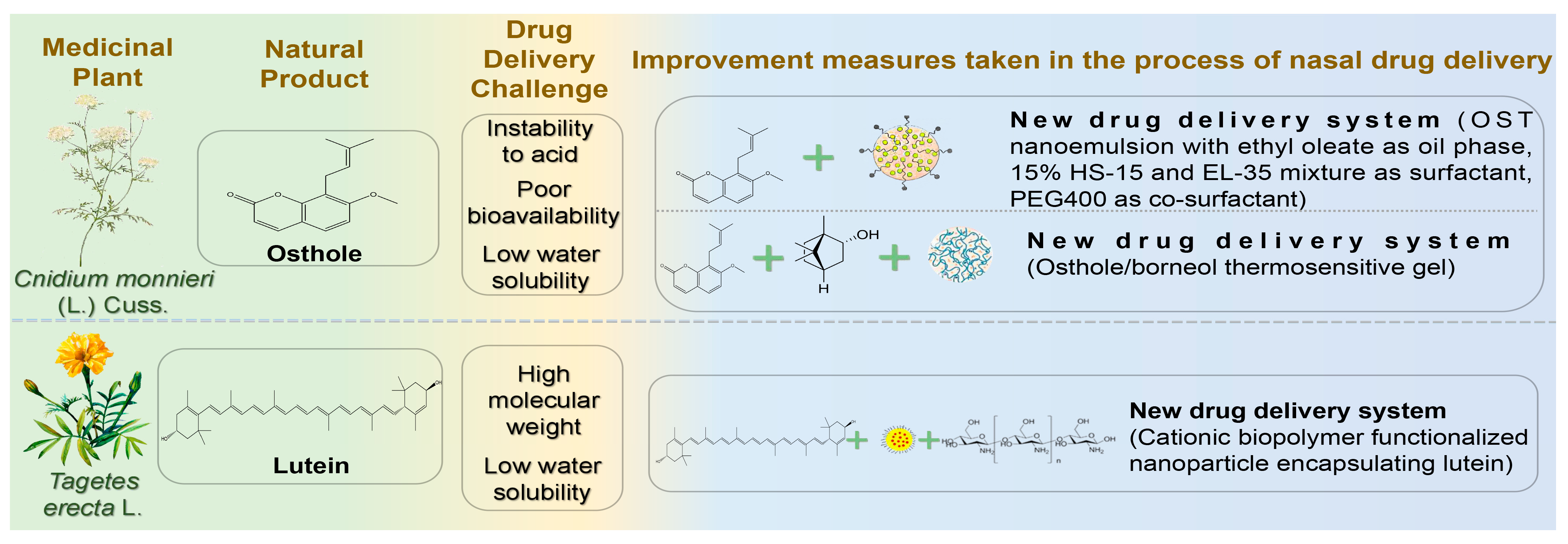
4.6. Others
4.6.1. Osthole
4.6.2. Lutein
| Natural Products | Diseases | Experimental Animal Model/Cell Model | Drug Delivery Systems | Formulation Optimization Effects | Pharmacological Effects | Reference |
|---|---|---|---|---|---|---|
| Osthole | AD | in vitro: L-glutamic acid-induced excitotoxic SH-SY5Y cells; in vivo: Scopolamine induced AD mice | Osthole NE | Slow-release performance ↑ (72 h release 80% OST); AUC brain ↑; Brain targeting ↑ (1.73 times higher than IV infusion); The brain clearance rate was 7.08 times lower than IV. | Antioxidant enzyme (superoxide dismutase and glutathione) activity ↑ | [163] |
| in vitro: Nasal mucosa from SD rats and APP/PS1 mice; in vivo: APP/PS1 transgenic mice | OST/Borneol thermosensitive gel | Intercellular space of nasal mucosa ↑; The drug release performance was good (the total dissolution rate of OST exceeded 95% within 300 min.); Brain bioavailability ↑; AUCbrain ↑ (Cbrain is nearly 10 times higher than oral administration) | Clearance of Aβ ↑ | [164] | ||
| Lutein | AD | in vitro: Goat nasal mucosa; SH-SY5Y cells; U-373MG cells; in vivo: SD rats | Cationic polymer-functionalized NPs carrying LT | Sustained drug release ability ↑ (drug release after 96 h was 70.12 ± 1.25%); Nasal mucosa permeability ↑ (24 h permeability 87.01%); BBB permeability ↑; Brain targeting ↑ (the Cmax of LT coated with chitosan in brain was 1.7 times higher than uncoated LT) | [167] |
5. Conclusions and Future Perspectives
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Katsuno, M.; Sahashi, K.; Iguchi, Y.; Hashizume, A. Preclinical progression of neurodegenerative diseases. Nagoya J. Med. Sci. 2018, 80, 289–298. [Google Scholar] [PubMed]
- Perneczky, R. Dementia prevention and reserve against neurodegenerative disease. Dialogues Clin. Neurosci. 2019, 21, 53–60. [Google Scholar] [CrossRef]
- Torres, J.; Costa, I.; Peixoto, A.F.; Silva, R.; Sousa, L.J.; Silva, A.C. Intranasal Lipid Nanoparticles Containing Bioactive Compounds Obtained from Marine Sources to Manage Neurodegenerative Diseases. Pharmaceuticals 2023, 16, 311. [Google Scholar] [CrossRef] [PubMed]
- Scheltens, P.; De Strooper, B.; Kivipelto, M.; Holstege, H.; Chetelat, G.; Teunissen, C.E.; Cummings, J.; van der Flier, W.M. Alzheimer’s disease. Lancet 2021, 397, 1577–1590. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Sherer, T.; Okun, M.S.; Bloem, B.R. The Emerging Evidence of the Parkinson Pandemic. J. Park. Dis. 2018, 8, S3–S8. [Google Scholar] [CrossRef]
- Jiang, A.; Handley, R.R.; Lehnert, K.; Snell, R.G. From Pathogenesis to Therapeutics: A Review of 150 Years of Huntington’s Disease Research. Int. J. Mol. Sci. 2023, 24, 13021. [Google Scholar] [CrossRef]
- Hardiman, O.; Al-Chalabi, A.; Chio, A.; Corr, E.M.; Logroscino, G.; Robberecht, W.; Shaw, P.J.; Simmons, Z.; van den Berg, L.H. Amyotrophic lateral sclerosis. Nat. Rev. Dis. Primers 2017, 3, 17071. [Google Scholar] [CrossRef]
- Yeo, C.; Tizzano, E.F.; Darras, B.T. Challenges and opportunities in spinal muscular atrophy therapeutics. Lancet Neurol. 2024, 23, 205–218. [Google Scholar] [CrossRef]
- Harding, A.E. Classification of the hereditary ataxias and paraplegias. Lancet 1983, 1, 1151–1155. [Google Scholar] [CrossRef]
- Wallin, M. Diagnosis of multiple sclerosis: Challenges and opportunities. Lancet Neurol. 2024, 23, 958–960. [Google Scholar] [CrossRef]
- Jin, X.; Liu, M.Y.; Zhang, D.F.; Zhong, X.; Du, K.; Qian, P.; Gao, H.; Wei, M.J. Natural products as a potential modulator of microglial polarization in neurodegenerative diseases. Pharmacol. Res. 2019, 145, 104253. [Google Scholar] [CrossRef] [PubMed]
- Ying, C.M.; Liu, F.X.; Pan, X.L.; Fan, F.Y.; Chen, N.; Zhang, Y.K. Research progress on traditional Chinese medicine in treatment of neurodegenerative diseases by delaying neurovascular unit aging. China J. Chin. Mater. Medica 2023, 48, 4060–4071. [Google Scholar]
- Bitter, C.; Suter-Zimmermann, K.; Surber, C. Nasal drug delivery in humans. Curr. Probl. Dermatol. 2011, 40, 20–35. [Google Scholar]
- Cunha, S.; Amaral, M.H.; Lobo, J.M.; Silva, A.C. Therapeutic Strategies for Alzheimer’s and Parkinson’s Diseases by Means of Drug Delivery Systems. Curr. Med. Chem. 2016, 23, 3618–3631. [Google Scholar] [CrossRef]
- Passeri, E.; Elkhoury, K.; Morsink, M.; Broersen, K.; Linder, M.; Tamayol, A.; Malaplate, C.; Yen, F.T.; Arab-Tehrany, E. Alzheimer’s Disease: Treatment Strategies and Their Limitations. Int. J. Mol. Sci. 2022, 23, 13954. [Google Scholar] [CrossRef]
- Patel, D.; Thakkar, H. Formulation considerations for improving intranasal delivery of CNS acting therapeutics. Ther. Deliv. 2022, 13, 371–381. [Google Scholar] [CrossRef]
- GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2133–2161. [Google Scholar]
- Rostagno, A.A. Pathogenesis of Alzheimer’s Disease. Int. J. Mol. Sci. 2022, 24, 107. [Google Scholar] [CrossRef]
- Hardy, J.A.; Higgins, G.A. Alzheimer’s disease: The amyloid cascade hypothesis. Science 1992, 256, 184–185. [Google Scholar] [CrossRef]
- Zhang, H.; Wei, W.; Zhao, M.; Ma, L.; Jiang, X.; Pei, H.; Cao, Y.; Li, H. Interaction between Abeta and Tau in the Pathogenesis of Alzheimer’s Disease. Int. J. Biol. Sci. 2021, 17, 2181–2192. [Google Scholar] [CrossRef]
- Hampel, H.; Mesulam, M.M.; Cuello, A.C.; Farlow, M.R.; Giacobini, E.; Grossberg, G.T.; Khachaturian, A.S.; Vergallo, A.; Cavedo, E.; Snyder, P.J.; et al. The cholinergic system in the pathophysiology and treatment of Alzheimer’s disease. Brain 2018, 141, 1917–1933. [Google Scholar] [CrossRef]
- Khan, S.; Barve, K.H.; Kumar, M.S. Recent Advancements in Pathogenesis, Diagnostics and Treatment of Alzheimer’s Disease. Curr. Neuropharmacol. 2020, 18, 1106–1125. [Google Scholar] [CrossRef] [PubMed]
- Berk, C.; Paul, G.; Sabbagh, M. Investigational drugs in Alzheimer’s disease: Current progress. Expert Opin. Investig. Drugs 2014, 23, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Galimberti, D.; Scarpini, E. Old and new acetylcholinesterase inhibitors for Alzheimer’s disease. Expert Opin. Investig. Drugs 2016, 25, 1181–1187. [Google Scholar] [CrossRef]
- GBD 2021 Nervous System Disorders Collaborators. Global, regional, and national burden of disorders affecting the nervous system, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol. 2024, 23, 344–381. [Google Scholar] [CrossRef] [PubMed]
- Erkkinen, M.G.; Kim, M.O.; Geschwind, M.D. Clinical Neurology and Epidemiology of the Major Neurodegenerative Diseases. Cold Spring Harb. Perspect. Biol. 2018, 10, a033118. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Constantinescu, R.; Thompson, J.P.; Biglan, K.M.; Holloway, R.G.; Kieburtz, K.; Marshall, F.J.; Ravina, B.M.; Schifitto, G.; Siderowf, A.; et al. Projected number of people with Parkinson disease in the most populous nations, 2005 through 2030. Neurology 2007, 68, 384–386. [Google Scholar] [CrossRef]
- Ye, H.; Robak, L.A.; Yu, M.; Cykowski, M.; Shulman, J.M. Genetics and Pathogenesis of Parkinson’s Syndrome. Annu. Rev. Pathol. 2023, 18, 95–121. [Google Scholar] [CrossRef]
- Hirsch, E.C.; Jenner, P.; Przedborski, S. Pathogenesis of Parkinson’s disease. Mov. Disord. 2013, 28, 24–30. [Google Scholar] [CrossRef]
- Hansen, C.A.; Miller, D.R.; Annarumma, S.; Rusch, C.T.; Ramirez-Zamora, A.; Khoshbouei, H. Levodopa-induced dyskinesia: A historical review of Parkinson’s disease, dopamine, and modern advancements in research and treatment. J. Neurol. 2022, 269, 2892–2909. [Google Scholar] [CrossRef]
- Aghaei, D.N.; Kheiri, R.; Ghorbani, N.B.; Sheikhi, M.; Razavi, M.S.; Rahimzadegan, M.; Salmasi, Z. Recent progress in the intranasal PLGA-based drug delivery for neurodegenerative diseases treatment. Iran. J. Basic Med. Sci. 2023, 26, 1107–1119. [Google Scholar]
- Aron, B.R. Nonhuman Primate Models of Huntington’s Disease and Their Application in Translational Research. Methods Mol. Biol. 2018, 1780, 267–284. [Google Scholar]
- Pringsheim, T.; Wiltshire, K.; Day, L.; Dykeman, J.; Steeves, T.; Jette, N. The incidence and prevalence of Huntington’s disease: A systematic review and meta-analysis. Mov. Disord. 2012, 27, 1083–1091. [Google Scholar] [CrossRef] [PubMed]
- An, P.; Lu, B.X. Current Research Status of Huntington’s Disease. Chin. J. Cell Biol. 2018, 40, 1621–1632. [Google Scholar]
- Shannon, K.M.; Fraint, A. Therapeutic advances in Huntington’s Disease. Mov. Disord. 2015, 30, 1539–1546. [Google Scholar] [CrossRef]
- Roos, R.A. Huntington’s disease: A clinical review. Orphanet. J. Rare Dis. 2010, 5, 40. [Google Scholar] [CrossRef]
- Yang, S.; Cheng, P.; Banta, H.; Piotrowska-Nitsche, K.; Yang, J.; Cheng, E.C.H.; Snyder, B.; Larkin, K.; Liu, J.; Orkin, J.; et al. Towards a transgenic model of Huntington’s disease in a non-human primate. Nature 2008, 453, 921–924. [Google Scholar] [CrossRef]
- Jimenez-Sanchez, M.; Licitra, F.; Underwood, B.R.; Rubinsztein, D.C. Huntington’s Disease: Mechanisms of Pathogenesis and Therapeutic Strategies. Cold Spring Harb. Perspect. Med. 2017, 7, a024240. [Google Scholar] [CrossRef]
- Feldman, E.L.; Goutman, S.A.; Petri, S.; Mazzini, L.; Savelieff, M.G.; Shaw, P.J.; Sobue, G. Amyotrophic lateral sclerosis. Lancet 2022, 400, 1363–1380. [Google Scholar] [CrossRef]
- Mercuri, E.; Sumner, C.J.; Muntoni, F.; Darras, B.T.; Finkel, R.S. Spinal muscular atrophy. Nat. Rev. Dis. Primers 2022, 8, 52. [Google Scholar] [CrossRef]
- Koch-Henriksen, N.; Magyari, M. Apparent changes in the epidemiology and severity of multiple sclerosis. Nat. Rev. Neurol. 2021, 17, 676–688. [Google Scholar] [CrossRef] [PubMed]
- Meyyazhagan, A.; Orlacchio, A. Hereditary Spastic Paraplegia: An Update. Int. J. Mol. Sci. 2022, 23, 1697. [Google Scholar] [CrossRef]
- Zhang, M.; Li, L.; Yang, Y. Exploration and analysis of Traditional Chinese Medicine books on nasal twitching therapy. China J. Chin. Ophthalmol. 2021, 31, 425–427. [Google Scholar]
- Jensen, J.P. Vasopressin therapy in Parkinson’s disease. Acta Neurol. Scand. 1980, 62, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Vaka, S.R.; Murthy, S.N. Enhancement of nose-brain delivery of therapeutic agents for treating neurodegenerative diseases using peppermint oil. Pharmazie 2010, 65, 690–692. [Google Scholar] [PubMed]
- Erdo, F.; Bors, L.A.; Farkas, D.; Bajza, A.; Gizurarson, S. Evaluation of intranasal delivery route of drug administration for brain targeting. Brain Res. Bull. 2018, 143, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Crowe, T.P.; Greenlee, M.; Kanthasamy, A.G.; Hsu, W.H. Mechanism of intranasal drug delivery directly to the brain. Life Sci. 2018, 195, 44–52. [Google Scholar] [CrossRef]
- Yasuda, M.; Inui, T.A.; Hirano, S.; Asano, S.; Okazaki, T.; Inui, T.; Marunaka, Y.; Nakahari, T. Intracellular Cl− Regulation of Ciliary Beating in Ciliated Human Nasal Epithelial Cells: Frequency and Distance of Ciliary Beating Observed by High-Speed Video Microscopy. Int. J. Mol. Sci. 2020, 21, 4052. [Google Scholar] [CrossRef]
- Wu, H.; Hu, K.; Jiang, X. From nose to brain: Understanding transport capacity and transport rate of drugs. Expert Opin. Drug Deliv. 2008, 5, 1159–1168. [Google Scholar] [CrossRef]
- Keller, L.A.; Merkel, O.; Popp, A. Intranasal drug delivery: Opportunities and toxicologic challenges during drug development. Drug Deliv. Transl. Res. 2022, 12, 735–757. [Google Scholar] [CrossRef]
- Zhang, Y.; Yu, W.; Zhang, L.; Wang, M.; Chang, W. The Interaction of Polyphenols and the Gut Microbiota in Neurodegenerative Diseases. Nutrients 2022, 14, 5373. [Google Scholar] [CrossRef] [PubMed]
- Yavarpour-Bali, H.; Ghasemi-Kasman, M.; Pirzadeh, M. Curcumin-loaded nanoparticles: A novel therapeutic strategy in treatment of central nervous system disorders. Int. J. Nanomed. 2019, 14, 4449–4460. [Google Scholar] [CrossRef]
- Zang, W.B.; Wei, H.L.; Zhang, W.W.; Ma, W.; Li, J.; Yao, Y. Curcumin hybrid molecules for the treatment of Alzheimer’s disease: Structure and pharmacological activities. Eur. J. Med. Chem. 2024, 265, 116070. [Google Scholar] [CrossRef] [PubMed]
- Anand, P.; Kunnumakkara, A.B.; Newman, R.A.; Aggarwal, B.B. Bioavailability of curcumin: Problems and promises. Mol. Pharm. 2007, 4, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, N.; Hosseini, M.J.; Rostamizadeh, K.; Anoush, M. Investigation of therapeutic effect of curcumin alpha and beta glucoside anomers against Alzheimer’s disease by the nose to brain drug delivery. Brain Res. 2021, 1766, 147517. [Google Scholar] [CrossRef]
- Hathout, R.M.; El-Ahmady, S.H.; Metwally, A.A. Curcumin or bisdemethoxycurcumin for nose-to-brain treatment of Alzheimer disease? A bio/chemo-informatics case study. Nat. Prod. Res. 2018, 32, 2873–2881. [Google Scholar] [CrossRef]
- Peng, H.; Li, Y.; Ji, W.; Zhao, R.; Lu, Z.; Shen, J.; Wu, Y.; Wang, J.; Hao, Q.; Wang, J.; et al. Intranasal Administration of Self-Oriented Nanocarriers Based on Therapeutic Exosomes for Synergistic Treatment of Parkinson’s Disease. ACS Nano 2022, 16, 869–884. [Google Scholar] [CrossRef]
- Katila, N.; Duwa, R.; Bhurtel, S.; Khanal, S.; Maharjan, S.; Jeong, J.H.; Lee, S.; Choi, D.Y.; Yook, S. Enhancement of blood-brain barrier penetration and the neuroprotective effect of resveratrol. J. Control. Release 2022, 346, 1–19. [Google Scholar] [CrossRef]
- Rege, S.D.; Geetha, T.; Griffin, G.D.; Broderick, T.L.; Babu, J.R. Neuroprotective effects of resveratrol in Alzheimer disease pathology. Front. Aging Neurosci. 2014, 6, 218. [Google Scholar] [CrossRef]
- Walle, T. Bioavailability of resveratrol. Ann. N. Y. Acad. Sci. 2011, 1215, 9–15. [Google Scholar] [CrossRef]
- Chimento, A.; De Amicis, F.; Sirianni, R.; Sinicropi, M.S.; Puoci, F.; Casaburi, I.; Saturnino, C.; Pezzi, V. Progress to Improve Oral Bioavailability and Beneficial Effects of Resveratrol. Int. J. Mol. Sci. 2019, 20, 1381. [Google Scholar] [CrossRef] [PubMed]
- Kotta, S.; Aldawsari, H.M.; Badr-Eldin, S.M.; Alhakamy, N.A.; Md, S. Coconut oil-based resveratrol nanoemulsion: Optimization using response surface methodology, stability assessment and pharmacokinetic evaluation. Food Chem. 2021, 357, 129721. [Google Scholar] [CrossRef] [PubMed]
- Abbas, H.; Refai, H.; El, S.N.; Rashed, L.A.; Mousa, M.R.; Zewail, M. Superparamagnetic iron oxide loaded chitosan coated bilosomes for magnetic nose to brain targeting of resveratrol. Int. J. Pharm. 2021, 610, 121244. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Santos, B.; Cazarin, C.A.; Da, S.P.; Dos, S.K.; Da, R.M.; Bao, S.N.; De-Souza, M.M.; Chorilli, M. Intranasal in situ gelling liquid crystal for delivery of resveratrol ameliorates memory and neuroinflammation in Alzheimer’s disease. Nanomedicine 2023, 51, 102689. [Google Scholar] [CrossRef]
- Umeda, T.; Sakai, A.; Shigemori, K.; Yokota, A.; Kumagai, T.; Tomiyama, T. Oligomer-Targeting Prevention of Neurodegenerative Dementia by Intranasal Rifampicin and Resveratrol Combination—A Preclinical Study in Model Mice. Front. Neurosci. 2021, 15, 763476. [Google Scholar] [CrossRef]
- Nasr, M. Development of an optimized hyaluronic acid-based lipidic nanoemulsion co-encapsulating two polyphenols for nose to brain delivery. Drug Deliv. 2016, 23, 1444–1452. [Google Scholar] [CrossRef]
- Shi, X.; Chen, Y.H.; Liu, H.; Qu, H.D. Therapeutic effects of paeonol on methyl-4-phenyl-1,2,3,6-tetrahydropyridine/probenecid-induced Parkinson’s disease in mice. Mol. Med. Rep. 2016, 14, 2397–2404. [Google Scholar] [CrossRef]
- Shen, B.; Wen, Y.; Li, S.; Zhou, Y.; Chen, J.; Yang, J.; Zhao, C.; Wang, J. Paeonol ameliorates hyperlipidemia and autophagy in mice by regulating Nrf2 and AMPK/mTOR pathways. Phytomedicine 2024, 132, 155839. [Google Scholar] [CrossRef]
- Adki, K.M.; Kulkarni, Y.A. Chemistry, pharmacokinetics, pharmacology and recent novel drug delivery systems of paeonol. Life Sci. 2020, 250, 117544. [Google Scholar] [CrossRef]
- Sun, Y.; Li, L.; Xie, H.; Wang, Y.; Gao, S.; Zhang, L.; Bo, F.; Yang, S.; Feng, A. Primary Studies on Construction and Evaluation of Ion-Sensitive in situ Gel Loaded with Paeonol-Solid Lipid Nanoparticles for Intranasal Drug Delivery. Int. J. Nanomed. 2020, 15, 3137–3160. [Google Scholar] [CrossRef]
- Wang, Z.Y.; Liu, J.G.; Li, H.; Yang, H.M. Pharmacological Effects of Active Components of Chinese Herbal Medicine in the Treatment of Alzheimer’s Disease: A Review. Am. J. Chin. Med. 2016, 44, 1525–1541. [Google Scholar] [CrossRef]
- Wang, S.; Jing, H.; Yang, H.; Liu, Z.; Guo, H.; Chai, L.; Hu, L. Tanshinone I selectively suppresses pro-inflammatory genes expression in activated microglia and prevents nigrostriatal dopaminergic neurodegeneration in a mouse model of Parkinson’s disease. J. Ethnopharmacol. 2015, 164, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Ma, J.; Xu, Z.; Chen, L.; Sun, B.; Shi, Y.; Miao, Y.; Wu, T.; Qin, M.; Zhang, Y.; et al. Rosmarinic Acid Inhibits Platelet Aggregation and Neointimal Hyperplasia In Vivo and Vascular Smooth Muscle Cell Dedifferentiation, Proliferation, and Migration In Vitro via Activation of the Keap1-Nrf2-ARE Antioxidant System. J. Agric. Food Chem. 2022, 70, 7420–7440. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Becker, J.; Ong, J.; Ciaghi, S.; Guldin, L.S.; Savastano, S.; Fukumitsu, S.; Kuwata, H.; Szele, F.G.; Isoda, H. Rosemary extract activates oligodendrogenesis genes in mouse brain and improves learning and memory ability. Biomed. Pharmacother. 2024, 179, 117350. [Google Scholar] [CrossRef] [PubMed]
- Markova, E.; Taneska, L.; Kostovska, M.; Shalabalija, D.; Mihailova, L.; Dodov, M.G.; Makreski, P.; Geskovski, N.; Petrushevska, M.; Taravari, A.N.; et al. Design and evaluation of nanostructured lipid carriers loaded with Salvia officinalis extract for Alzheimer’s disease treatment. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 1368–1390. [Google Scholar] [CrossRef]
- Bhatt, R.; Singh, D.; Prakash, A.; Mishra, N. Development, characterization and nasal delivery of rosmarinic acid-loaded solid lipid nanoparticles for the effective management of Huntington’s disease. Drug Deliv. 2015, 22, 931–939. [Google Scholar] [CrossRef]
- Neto-Neves, E.M.; Da, S.M.B.F.; Dejani, N.N.; de Sousa, D.P. Ferulic Acid and Cardiovascular Health: Therapeutic and Preventive Potential. Mini Rev. Med. Chem. 2021, 21, 1625–1637. [Google Scholar] [CrossRef]
- Bramanti, E.; Fulgentini, L.; Bizzarri, R.; Lenci, F.; Sgarbossa, A. beta-Amyloid amorphous aggregates induced by the small natural molecule ferulic acid. J. Phys. Chem. B 2013, 117, 13816–13821. [Google Scholar] [CrossRef]
- Sgarbossa, A.; Giacomazza, D.; di Carlo, M. Ferulic Acid: A Hope for Alzheimer’s Disease Therapy from Plants. Nutrients 2015, 7, 5764–5782. [Google Scholar] [CrossRef]
- Saini, S.; Sharma, T.; Jain, A.; Kaur, H.; Katare, O.P.; Singh, B. Systematically designed chitosan-coated solid lipid nanoparticles of ferulic acid for effective management of Alzheimer’s disease: A preclinical evidence. Colloids Surf. B Biointerfaces 2021, 205, 111838. [Google Scholar] [CrossRef]
- Botti, G.; Bianchi, A.; Dalpiaz, A.; Tedeschi, P.; Albanese, V.; Sorrenti, M.; Catenacci, L.; Bonferoni, M.C.; Beggiato, S.; Pavan, B. Dimeric ferulic acid conjugate as a prodrug for brain targeting after nasal administration of loaded solid lipid microparticles. Expert Opin. Drug Deliv. 2023, 20, 1657–1679. [Google Scholar] [CrossRef] [PubMed]
- Sun, A.; Xu, X.; Lin, J.; Cui, X.; Xu, R. Neuroprotection by saponins. Phytother. Res. 2015, 29, 187–200. [Google Scholar] [CrossRef]
- Guo, C.; Li, L.; Yang, X.; Meng, Z.; Li, F.; Zhang, C.; Yang, Z. Protective effects of timosaponin B-II on high glucose-induced apoptosis in human umbilical vein endothelial cells. Environ. Toxicol. Pharmacol. 2014, 37, 37–44. [Google Scholar] [CrossRef]
- Lu, W.Q.; Qiu, Y.; Li, T.J.; Tao, X.; Sun, L.N.; Chen, W.S. Timosaponin B-II inhibits pro-inflammatory cytokine induction by lipopolysaccharide in BV2 cells. Arch. Pharm. Res. 2009, 32, 1301–1308. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Liu, C.; Qi, Y.; Fang, L.; Luo, J.; Bi, K.; Jia, Y. Timosaponin B-II ameliorates scopolamine-induced cognition deficits by attenuating acetylcholinesterase activity and brain oxidative damage in mice. Metab. Brain Dis. 2016, 31, 1455–1461. [Google Scholar] [CrossRef]
- Wang, H.Q.; Lan, F.; Zhang, Y.H.; Xia, J.E.; Gong, X.M.; Liu, M. Identification and pharmacokinetics of saponins in Rhizoma Anemarrhenae after oral administration to rats by HPLC-Q-TOF/MS and HPLC-MS/MS. Acta Pharm. 2021, 71, 567–585. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Li, R.; Zhu, S.; Ma, J.; Pang, L.; Ma, B.; Du, L.; Jin, Y. Nasal timosaponin BII dually sensitive in situ hydrogels for the prevention of Alzheimer’s disease induced by lipopolysaccharides. Int. J. Pharm. 2020, 578, 119115. [Google Scholar] [CrossRef]
- Yi, J.H.; Moon, S.; Cho, E.; Kwon, H.; Lee, S.; Jeon, J.; Park, A.Y.; Lee, Y.H.; Kwon, K.J.; Ryu, J.H.; et al. Hyperoside improves learning and memory deficits by amyloid β1–42 in mice through regulating synaptic calcium-permeable AMPA receptors. Eur. J. Pharmacol. 2022, 931, 175188. [Google Scholar] [CrossRef]
- Chen, L.; Zhou, Y.P.; Liu, H.Y.; Gu, J.H.; Zhou, X.F.; Yue-Qin, Z. Long-term oral administration of hyperoside ameliorates AD-related neuropathology and improves cognitive impairment in APP/PS1 transgenic mice. Neurochem. Int. 2021, 151, 105196. [Google Scholar] [CrossRef]
- Qian, F.; Zhang, Q. Determination of Equilibrium Solubility and Apparent Oil/water Partition Coefficients of Hyperin in Total Flavones from Abelmoschus Manihot. China Pharm. 2016, 19, 2222–2224. [Google Scholar]
- Song, L.L.; Qu, Y.Q.; Tang, Y.P.; Chen, X.; Lo, H.H.; Qu, L.Q.; Yun, Y.X.; Wong, V.; Zhang, R.L.; Wang, H.M.; et al. Hyperoside alleviates toxicity of beta-amyloid via endoplasmic reticulum-mitochondrial calcium signal transduction cascade in APP/PS1 double transgenic Alzheimer’s disease mice. Redox. Biol. 2023, 61, 102637. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Wu, Q.; Chen, Y.; Gu, G.; Gao, R.; Peng, B.; Wang, Y.; Li, A.; Guo, J.; Xu, X.; et al. Updated Pharmacological Effects, Molecular Mechanisms, and Therapeutic Potential of Natural Product Geniposide. Molecules 2022, 27, 3319. [Google Scholar] [CrossRef]
- Liu, W.; Li, G.; Holscher, C.; Li, L. Neuroprotective effects of geniposide on Alzheimer’s disease pathology. Rev. Neurosci. 2015, 26, 371–383. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, K.; Shi, M.; Xie, L.; Deng, M.; Chen, H.; Li, X. Therapeutic potential of catalpol and geniposide in Alzheimer’s and Parkinson’s diseases: A snapshot of their underlying mechanisms. Brain Res. Bull. 2021, 174, 281–295. [Google Scholar] [CrossRef]
- Wang, Y.; Jiang, S.; Wang, H.; Bie, H. A mucoadhesive, thermoreversible in situ nasal gel of geniposide for neurodegenerative diseases. PLoS ONE 2017, 12, e189478. [Google Scholar] [CrossRef]
- Gong, X.; Tan, Z.; Xu, H.; Jiang, X.; Chen, L. Paeoniflorin Attenuates Oxidative Stress and Inflammation in Parkinson’s Disease by Activating the HSF1-NRF1 Axis. Am. J. Chin. Med. 2024, 52, 2131–2159. [Google Scholar] [CrossRef]
- Shen, C.; Shen, B.; Zhu, J.; Wang, J.; Yuan, H.; Li, X. Glycyrrhizic acid-based self-assembled micelles for improving oral bioavailability of paeoniflorin. Drug Dev. Ind. Pharm. 2021, 47, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Li, B.; Zhang, Y.; Chen, T.; Chen, C.; Jiang, W.; Wang, Q.; Chen, T. Intranasal delivery of paeoniflorin nanocrystals for brain targeting. Asian J. Pharm. Sci. 2020, 15, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Inagaki, Y.; Liu, Y. Research progress on flavonoids isolated from traditional Chinese medicine in treatment of Alzheimer’s disease. Intractable Rare Dis. Res. 2013, 2, 3–10. [Google Scholar]
- Agrawal, K.; Chakraborty, P.; Dewanjee, S.; Arfin, S.; Das, S.S.; Dey, A.; Moustafa, M.; Mishra, P.C.; Jafari, S.M.; Jha, N.K.; et al. Neuropharmacological interventions of quercetin and its derivatives in neurological and psychological disorders. Neurosci. Biobehav. Rev. 2023, 144, 104955. [Google Scholar] [CrossRef]
- Sabogal-Guaqueta, A.M.; Munoz-Manco, J.I.; Ramirez-Pineda, J.R.; Lamprea-Rodriguez, M.; Osorio, E.; Cardona-Gomez, G.P. The flavonoid quercetin ameliorates Alzheimer’s disease pathology and protects cognitive and emotional function in aged triple transgenic Alzheimer’s disease model mice. Neuropharmacology 2015, 93, 134–145. [Google Scholar] [CrossRef]
- Sood, S.; Jain, K.; Gowthamarajan, K. Intranasal therapeutic strategies for management of Alzheimer’s disease. J. Drug Target. 2014, 22, 279–294. [Google Scholar] [CrossRef] [PubMed]
- Dou, Y.; Zhao, D.; Yang, F.; Tang, Y.; Chang, J. Natural Phyto-Antioxidant Albumin Nanoagents to Treat Advanced Alzheimer’s Disease. ACS Appl. Mater. Interfaces 2021, 13, 30373–30382. [Google Scholar] [CrossRef] [PubMed]
- Sonawane, D.; Pokharkar, V. Quercetin-Loaded Nanostructured Lipid Carrier In Situ Gel for Brain Targeting Through Intranasal Route: Formulation, In Vivo Pharmacokinetic and Pharmacodynamic Studies. AAPS PharmSciTech 2024, 25, 30. [Google Scholar] [CrossRef]
- Manta, K.; Papakyriakopoulou, P.; Chountoulesi, M.; Diamantis, D.A.; Spaneas, D.; Vakali, V.; Naziris, N.; Chatziathanasiadou, M.V.; Andreadelis, I.; Moschovou, K.; et al. Preparation and Biophysical Characterization of Quercetin Inclusion Complexes with beta-Cyclodextrin Derivatives to be Formulated as Possible Nose-to-Brain Quercetin Delivery Systems. Mol. Pharm. 2020, 17, 4241–4255. [Google Scholar] [CrossRef] [PubMed]
- Vaz, G.; Clementino, A.; Mitsou, E.; Ferrari, E.; Buttini, F.; Sissa, C.; Xenakis, A.; Sonvico, F.; Dora, C.L. In Vitro Evaluation of Curcumin- and Quercetin-Loaded Nanoemulsions for Intranasal Administration: Effect of Surface Charge and Viscosity. Pharmaceutics 2022, 14, 194. [Google Scholar] [CrossRef]
- Rani, N.; Bharti, S.; Krishnamurthy, B.; Bhatia, J.; Sharma, C.; Kamal, M.A.; Ojha, S.; Arya, D.S. Pharmacological Properties and Therapeutic Potential of Naringenin: A Citrus Flavonoid of Pharmaceutical Promise. Curr. Pharm. Des. 2016, 22, 4341–4359. [Google Scholar] [CrossRef]
- Wang, G.Q.; Zhang, B.; He, X.M.; Li, D.D.; Shi, J.S.; Zhang, F. Naringenin targets on astroglial Nrf2 to support dopaminergic neurons. Pharmacol. Res. 2019, 139, 452–459. [Google Scholar] [CrossRef]
- Gaba, B.; Khan, T.; Haider, M.F.; Alam, T.; Baboota, S.; Parvez, S.; Ali, J. Vitamin E Loaded Naringenin Nanoemulsion via Intranasal Delivery for the Management of Oxidative Stress in a 6-OHDA Parkinson’s Disease Model. BioMed Res. Int. 2019, 2019, 2382563. [Google Scholar] [CrossRef]
- He, C.; Wang, Z.; Shi, J. Pharmacological effects of icariin. Adv. Pharmacol. 2020, 87, 179–203. [Google Scholar]
- Chen, W.F.; Wu, L.; Du, Z.R.; Chen, L.; Xu, A.L.; Chen, X.H.; Teng, J.J.; Wong, M.S. Neuroprotective properties of icariin in MPTP-induced mouse model of Parkinson’s disease: Involvement of PI3K/Akt and MEK/ERK signaling pathways. Phytomedicine 2017, 25, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Yu, J.; Zhan, J.; Yang, L.; Guo, L.; Xu, Y. Pharmacokinetics, Tissue Distribution, and Metabolism Study of Icariin in Rat. BioMed Res. Int. 2017, 2017, 4684962. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y. Therapeutic Effect of Nasal Administration of Controlled-Release Icariin Temperature-Sensitive Gel on Mouse Model of Parkinson’s Disease. Master’s Thesis, Tianjin University of Traditional Chinese Medicine, Tianjin, China, 2020. [Google Scholar]
- Cheng, Z.; Huang, J.; Zhu, W.; Zhi, Y.; Zhao, Y. Effect of intranasal administration of icariin liposome on behavior and neurotransmitter in rats with Parkinson’s disease. China Mod. Dr. 2019, 57, 43–47. [Google Scholar]
- Moghadam, E.R.; Ang, H.L.; Asnaf, S.E.; Zabolian, A.; Saleki, H.; Yavari, M.; Esmaeili, H.; Zarrabi, A.; Ashrafizadeh, M.; Kumar, A.P. Broad-Spectrum Preclinical Antitumor Activity of Chrysin: Current Trends and Future Perspectives. Biomolecules 2020, 10, 1374. [Google Scholar] [CrossRef]
- Talebi, M.; Talebi, M.; Farkhondeh, T.; Kopustinskiene, D.M.; Simal-Gandara, J.; Bernatoniene, J.; Samarghandian, S. An updated review on the versatile role of chrysin in neurological diseases: Chemistry, pharmacology, and drug delivery approaches. Biomed. Pharmacother. 2021, 141, 111906. [Google Scholar] [CrossRef]
- Guo, B.; Zheng, C.; Cai, W.; Cheng, J.; Wang, H.; Li, H.; Sun, Y.; Cui, W.; Wang, Y.; Han, Y.; et al. Multifunction of Chrysin in Parkinson’s Model: Anti-Neuronal Apoptosis, Neuroprotection via Activation of MEF2D, and Inhibition of Monoamine Oxidase-B. J. Agric. Food Chem. 2016, 64, 5324–5333. [Google Scholar] [CrossRef] [PubMed]
- Stompor-Goracy, M.; Bajek-Bil, A.; Machaczka, M. Chrysin: Perspectives on Contemporary Status and Future Possibilities as Pro-Health Agent. Nutrients 2021, 13, 2038. [Google Scholar] [CrossRef]
- Lavania, K.; Garg, A. Ion-activated In Situ Gel of Gellan Gum Containing Chrysin for Nasal Administration in Parkinson’s Disease. Recent Adv. Drug Deliv. Formul. 2024, 18, 35–49. [Google Scholar] [CrossRef]
- Lungare, S.; Hallam, K.; Badhan, R.K. Phytochemical-loaded mesoporous silica nanoparticles for nose-to-brain olfactory drug delivery. Int. J. Pharm. 2016, 513, 280–293. [Google Scholar] [CrossRef]
- Rezaul, I.M.; Akash, S.; Murshedul, I.M.; Sarkar, N.; Kumer, A.; Chakraborty, S.; Dhama, K.; Ahmed, A.M.; Anwar, Y.; Wilairatana, P.; et al. Alkaloids as drug leads in Alzheimer’s treatment: Mechanistic and therapeutic insights. Brain Res. 2024, 1834, 148886. [Google Scholar] [CrossRef]
- Qian Zm, K.Y. Huperzine A: Is it an Effective Disease-Modifying Drug for Alzheimer’s Disease? Front. Aging Neurosci. 2014, 6, 216. [Google Scholar] [CrossRef] [PubMed]
- Friedli, M.J.; Inestrosa, N.C. Huperzine A and Its Neuroprotective Molecular Signaling in Alzheimer’s Disease. Molecules 2021, 26, 6531. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Liu, C.; Zhai, W.; Zhuang, N.; Han, T.; Ding, Z. The Optimization Design of Lactoferrin Loaded HupA Nanoemulsion for Targeted Drug Transport Via Intranasal Route. Int. J. Nanomed. 2019, 14, 9217–9234. [Google Scholar] [CrossRef]
- Meng, Q.; Wang, A.; Hua, H.; Jiang, Y.; Wang, Y.; Mu, H.; Wu, Z.; Sun, K. Intranasal delivery of Huperzine A to the brain using lactoferrin-conjugated N-trimethylated chitosan surface-modified PLGA nanoparticles for treatment of Alzheimer’s disease. Int. J. Nanomed. 2018, 2018, 705–718. [Google Scholar] [CrossRef]
- Wang, C.Y.; Zheng, W.; Wang, T.; Xie, J.W.; Wang, S.L.; Zhao, B.L.; Teng, W.P.; Wang, Z.Y. Huperzine A activates Wnt/β-catenin signaling and enhances the nonamyloidogenic pathway in an Alzheimer transgenic mouse model. Neuropsychopharmacology 2011, 36, 1073–1089. [Google Scholar] [CrossRef]
- Ruan, S.; Li, J.; Ruan, H.; Xia, Q.; Hou, X.; Wang, Z.; Guo, T.; Zhu, C.; Feng, N.; Zhang, Y. Microneedle-mediated nose-to-brain drug delivery for improved Alzheimer’s disease treatment. J. Control. Release 2024, 366, 712–731. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Feng, X.; Chai, L.; Cao, S.; Qiu, F. The metabolism of berberine and its contribution to the pharmacological effects. Drug Metab. Rev. 2017, 49, 139–157. [Google Scholar] [CrossRef]
- Akbar, M.; Shabbir, A.; Rehman, K.; Akash, M.; Shah, M.A. Neuroprotective potential of berberine in modulating Alzheimer’s disease via multiple signaling pathways. J. Food Biochem. 2021, 45, e13936. [Google Scholar] [CrossRef]
- Murakami, T.; Bodor, E.; Bodor, N. Approaching strategy to increase the oral bioavailability of berberine, a quaternary ammonium isoquinoline alkaloid: Part 2. development of oral dosage formulations. Expert Opin. Drug Metab. Toxicol. 2023, 19, 139–148. [Google Scholar] [CrossRef]
- Xiong, R.G.; Huang, S.Y.; Wu, S.X.; Zhou, D.D.; Yang, Z.J.; Saimaiti, A.; Zhao, C.N.; Shang, A.; Zhang, Y.J.; Gan, R.Y.; et al. Anticancer Effects and Mechanisms of Berberine from Medicinal Herbs: An Update Review. Molecules 2022, 27, 4523. [Google Scholar] [CrossRef]
- Mishra, G.; Awasthi, R.; Singh, A.K.; Singh, S.; Mishra, S.K.; Singh, S.K.; Nandi, M.K. Intranasally Co-administered Berberine and Curcumin Loaded in Transfersomal Vesicles Improved Inhibition of Amyloid Formation and BACE-1. ACS Omega 2022, 7, 43290–43305. [Google Scholar] [CrossRef]
- Xi, Y.; Ye, Y.; Dou, G.; Chang, T.; Niu, Y.; Zhou, Z.; Chu, Z. Effects of paclitaxel on Müller cells in retina. Int. J. Ophthalmol.-Chi. 2023, 23, 1775–1780. [Google Scholar]
- Brunden, K.R.; Yao, Y.; Potuzak, J.S.; Ferrer, N.I.; Ballatore, C.; James, M.J.; Hogan, A.M.; Trojanowski, J.Q.; Smith, A.R.; Lee, V.M. The characterization of microtubule-stabilizing drugs as possible therapeutic agents for Alzheimer’s disease and related tauopathies. Pharmacol. Res. 2011, 63, 341–351. [Google Scholar] [CrossRef]
- Cross, D.J.; Huber, B.R.; Silverman, M.A.; Cline, M.M.; Gill, T.B.; Cross, C.G.; Cook, D.G.; Minoshima, S. Intranasal Paclitaxel Alters Alzheimer’s Disease Phenotypic Features in 3xTg-AD Mice. J. Alzheimers Dis. 2021, 83, 379–394. [Google Scholar] [CrossRef]
- Wang, C.; Cai, Z.; Wang, W.; Wei, M.; Kou, D.; Li, T.; Yang, Z.; Guo, H.; Le, W.; Li, S. Piperine attenuates cognitive impairment in an experimental mouse model of sporadic Alzheimer’s disease. J. Nutr. Biochem. 2019, 70, 147–155. [Google Scholar] [CrossRef]
- Nazifi, M.; Oryan, S.; Esfahani, D.E.; Ashrafpoor, M. The functional effects of piperine and piperine plus donepezil on hippocampal synaptic plasticity impairment in rat model of Alzheimer’s disease. Life Sci. 2021, 265, 118802. [Google Scholar] [CrossRef]
- Delgoda, R.; Westlake, A.C. Herbal interactions involving cytochrome p450 enzymes: A mini review. Toxicol. Rev. 2004, 23, 239–249. [Google Scholar] [CrossRef]
- Elnaggar, Y.; Etman, S.M.; Abdelmonsif, D.A.; Abdallah, O.Y. Intranasal Piperine-Loaded Chitosan Nanoparticles as Brain-Targeted Therapy in Alzheimer’s Disease: Optimization, Biological Efficacy, and Potential Toxicity. J. Pharm. Sci. 2015, 104, 3544–3556. [Google Scholar] [CrossRef]
- Sahoo, A.K.; Dandapat, J.; Dash, U.C.; Kanhar, S. Features and outcomes of drugs for combination therapy as multi-targets strategy to combat Alzheimer’s disease. J. Ethnopharmacol. 2018, 215, 42–73. [Google Scholar] [CrossRef] [PubMed]
- Raffaele, K.C.; Asthana, S.; Berardi, A.; Haxby, J.V.; Morris, P.P.; Schapiro, M.B.; Soncrant, T.T. Differential response to the cholinergic agonist arecoline among different cognitive modalities in Alzheimer’s disease. Neuropsychopharmacology 1996, 15, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Asthana, S.; Greig, N.H.; Holloway, H.W.; Raffaele, K.C.; Berardi, A.; Schapiro, M.B.; Rapoport, S.I.; Soncrant, T.T. Clinical pharmacokinetics of arecoline in subjects with Alzheimer’s disease. Clin. Pharmacol. Ther. 1996, 60, 276–282. [Google Scholar] [CrossRef]
- Hussain, M.A.; Mollica, J.A. Intranasal absorption of physostigmine and arecoline. J. Pharm. Sci. 1991, 80, 750–751. [Google Scholar] [CrossRef]
- Geetha, R.G.; Ramachandran, S. Recent Advances in the Anti-Inflammatory Activity of Plant-Derived Alkaloid Rhynchophylline in Neurological and Cardiovascular Diseases. Pharmaceutics 2021, 13, 1170. [Google Scholar] [CrossRef]
- Zhang, C.; Xue, Z.; Zhu, L.; Zhou, J.; Zhuo, L.; Zhang, J.; Zhang, X.; Liu, W.; Han, L.; Liao, W. Rhynchophylline alleviates neuroinflammation and regulates metabolic disorders in a mouse model of Parkinson’s disease. Food Funct. 2023, 14, 3208–3219. [Google Scholar] [CrossRef]
- Lin, H.; Xie, L.; Lv, L.; Chen, J.; Feng, F.; Liu, W.; Han, L.; Liu, F. Intranasally administered thermosensitive gel for brain-targeted delivery of rhynchophylline to treat Parkinson’s disease. Colloids Surf. B Biointerfaces 2023, 222, 113065. [Google Scholar] [CrossRef]
- Xu, Y.; Wei, H.; Gao, J. Natural Terpenoids as Neuroinflammatory Inhibitors in LPS-stimulated BV-2 Microglia. Mini Rev. Med. Chem. 2021, 21, 520–534. [Google Scholar] [CrossRef]
- Asl, M.N.; Hosseinzadeh, H. Review of pharmacological effects of Glycyrrhiza sp. and its bioactive compounds. Phytother. Res. 2008, 22, 709–724. [Google Scholar] [CrossRef]
- Kao, T.C.; Shyu, M.H.; Yen, G.C. Neuroprotective effects of glycyrrhizic acid and 18beta-glycyrrhetinic acid in PC12 cells via modulation of the PI3K/Akt pathway. J. Agric. Food Chem. 2009, 57, 754–761. [Google Scholar] [CrossRef]
- Gad, S.R.; El-Gogary, R.I.; George, M.Y.; Hathout, R.M. Nose-to-brain delivery of 18beta-Glycyrrhetinic acid using optimized lipid nanocapsules: A novel alternative treatment for Alzheimer’s disease. Int. J. Pharm. 2023, 645, 123387. [Google Scholar] [CrossRef]
- Huang, X.; Deng, H.; Shen, Q.K.; Quan, Z.S. Tanshinone IIA: Pharmacology, Total Synthesis, and Progress in Structure-modifications. Curr. Med. Chem. 2022, 29, 1959–1989. [Google Scholar] [CrossRef]
- Subedi, L.; Gaire, B.P. Tanshinone IIA: A phytochemical as a promising drug candidate for neurodegenerative diseases. Pharmacol. Res. 2021, 169, 105661. [Google Scholar] [CrossRef]
- Hassan, D.M.; El-Kamel, A.H.; Allam, E.A.; Bakr, B.A.; Ashour, A.A. Chitosan-coated nanostructured lipid carriers for effective brain delivery of Tanshinone IIA in Parkinson’s disease: Interplay between nuclear factor-kappa beta and cathepsin B. Drug Deliv. Transl. Res. 2024, 14, 400–417. [Google Scholar] [CrossRef]
- Lei, Y.; Fu, P.; Jun, X.; Cheng, P. Pharmacological Properties of Geraniol—A Review. Planta Med. 2019, 85, 48–55. [Google Scholar] [CrossRef]
- Pandur, E.; Major, B.; Rak, T.; Sipos, K.; Csutak, A.; Horvath, G. Linalool and Geraniol Defend Neurons from Oxidative Stress, Inflammation, and Iron Accumulation in In Vitro Parkinson’s Models. Antioxidants 2024, 13, 917. [Google Scholar] [CrossRef]
- de Oliveira, J.E.; Truzzi, E.; Ferraro, L.; Fogagnolo, M.; Pavan, B.; Beggiato, S.; Rustichelli, C.; Maretti, E.; Lima, E.M.; Leo, E.; et al. Nasal administration of nanoencapsulated geraniol/ursodeoxycholic acid conjugate: Towards a new approach for the management of Parkinson’s disease. J. Control. Release 2020, 321, 540–552. [Google Scholar] [CrossRef]
- Truzzi, E.; Rustichelli, C.; de Oliveira, J.E.; Ferraro, L.; Maretti, E.; Graziani, D.; Botti, G.; Beggiato, S.; Iannuccelli, V.; Lima, E.M.; et al. Nasal biocompatible powder of Geraniol oil complexed with cyclodextrins for neurodegenerative diseases: Physicochemical characterization and in vivo evidences of nose to brain delivery. J. Control. Release 2021, 335, 191–202. [Google Scholar] [CrossRef]
- Jarzab, A.; Grabarska, A.; Skalicka-Wozniak, K.; Stepulak, A. Pharmacological features of osthole. Postep. Hig. Med. Dosw. (Online) 2017, 71, 411–421. [Google Scholar] [CrossRef]
- Yao, Y.; Gao, Z.; Liang, W.; Kong, L.; Jiao, Y.; Li, S.; Tao, Z.; Yan, Y.; Yang, J. Osthole promotes neuronal differentiation and inhibits apoptosis via Wnt/β-catenin signaling in an Alzheimer’s disease model. Toxicol. Appl. Pharmacol. 2015, 289, 474–481. [Google Scholar] [CrossRef]
- Yao, L.; Liu, M.; Chen, S.; Qin, Y.; Wang, Z.; Zhao, W. Study on Anti-inflammatory Mechanism of Osthole on in vitro Cell Model of Alzheimer’s Disease through APOE-TREM2. Tradit. Chin. Drug Res. Clin. Pharmacol. 2021, 32, 1606–1614. [Google Scholar]
- Zhang, L.; Li, D.C.; Liu, L.F. Paeonol: Pharmacological effects and mechanisms of action. Int. Immunopharmacol. 2019, 72, 413–421. [Google Scholar] [CrossRef]
- Tayeb, H.H.; Sainsbury, F. Nanoemulsions in drug delivery: Formulation to medical application. Nanomedicine 2018, 13, 2507–2525. [Google Scholar] [CrossRef]
- Song, Y.; Wang, X.; Wang, X.; Wang, J.; Hao, Q.; Hao, J.; Hou, X. Osthole-Loaded Nanoemulsion Enhances Brain Target in the Treatment of Alzheimer’s Disease via Intranasal Administration. Oxid. Med. Cell. Longev. 2021, 2021, 8844455. [Google Scholar] [CrossRef]
- Wu, F.; Huang, M.; Zuo, X.; Xie, R.; Liu, J.; Ke, J.; Li, W.; Wang, Q.; Liang, Y. Osthole/borneol thermosensitive gel via intranasal administration enhances intracerebral bioavailability to improve cognitive impairment in APP/PS1 transgenic mice. Front. Pharmacol. 2023, 14, 1224856. [Google Scholar] [CrossRef]
- Li, N.; Wu, X.; Zhuang, W.; Xia, L.; Chen, Y.; Wang, Y.; Wu, C.; Rao, Z.; Du, L.; Zhao, R.; et al. Green leafy vegetable and lutein intake and multiple health outcomes. Food Chem. 2021, 360, 130145. [Google Scholar] [CrossRef]
- Su, W.; Xu, W.; Liu, E.; Su, W.; Polyakov, N.E. Improving the Treatment Effect of Carotenoids on Alzheimer’s Disease through Various Nano-Delivery Systems. Int. J. Mol. Sci. 2023, 24, 7652. [Google Scholar] [CrossRef]
- Dhas, N.; Mehta, T. Cationic biopolymer functionalized nanoparticles encapsulating lutein to attenuate oxidative stress in effective treatment of Alzheimer’s disease: A non-invasive approach. Int. J. Pharm. 2020, 586, 119553. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, R.; Yang, Z.; Wen, Q.; Cao, X.; Zhao, N.; Yan, J. Protective Effects of Polysaccharides in Neurodegenerative Diseases. Front. Aging Neurosci. 2022, 14, 917629. [Google Scholar] [CrossRef]
- Zhang, R.; Zeng, M.; Zhang, X.; Zheng, Y.; Lv, N.; Wang, L.; Gan, J.; Li, Y.; Jiang, X.; Yang, L. Therapeutic Candidates for Alzheimer’s Disease: Saponins. Int. J. Mol. Sci. 2023, 24, 10505. [Google Scholar] [CrossRef]
- She, L.; Sun, J.; Xiong, L.; Li, A.; Li, L.; Wu, H.; Ren, J.; Wang, W.; Liang, G.; Zhao, X. Ginsenoside RK1 improves cognitive impairments and pathological changes in Alzheimer’s disease via stimulation of the AMPK/Nrf2 signaling pathway. Phytomedicine 2024, 122, 155168. [Google Scholar] [CrossRef]
- Wang, S.S.; Peng, Y.; Fan, P.L.; Ye, J.R.; Ma, W.Y.; Wu, Q.L.; Wang, H.Y.; Tian, Y.J.; He, W.B.; Yan, X.; et al. Ginsenoside Rg1 ameliorates stress-exacerbated Parkinson’s disease in mice by eliminating RTP801 and alpha-synuclein autophagic degradation obstacle. Acta Pharmacol. Sin. 2025, 46, 308–325. [Google Scholar] [CrossRef]
- Calis, Z.; Mogulkoc, R.; Baltaci, A.K. The Roles of Flavonols/Flavonoids in Neurodegeneration and Neuroinflammation. Mini Rev. Med. Chem. 2020, 20, 1475–1488. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Li, X.; Wang, Z.; Cao, Y.; Han, S.; Li, N.; Cai, J.; Cheng, S.; Liu, Q. Protective effects of luteolin against amyloid beta-induced oxidative stress and mitochondrial impairments through peroxisome proliferator-activated receptor gamma-dependent mechanism in Alzheimer’s disease. Redox. Biol. 2023, 66, 102848. [Google Scholar] [CrossRef] [PubMed]
- Cui, L.; Cai, Y.; Cheng, W.; Liu, G.; Zhao, J.; Cao, H.; Tao, H.; Wang, Y.; Yin, M.; Liu, T.; et al. A Novel, Multi-Target Natural Drug Candidate, Matrine, Improves Cognitive Deficits in Alzheimer’s Disease Transgenic Mice by Inhibiting Abeta Aggregation and Blocking the RAGE/Abeta Axis. Mol. Neurobiol. 2017, 54, 1939–1952. [Google Scholar] [CrossRef] [PubMed]
- Pang, S.; Li, S.; Cheng, H.; Luo, Z.; Qi, X.; Guan, F.; Dong, W.; Gao, S.; Liu, N.; Gao, X.; et al. Discovery of an evodiamine derivative for PI3K/AKT/GSK3β pathway activation and AD pathology improvement in mouse models. Front. Mol. Neurosci. 2023, 15, 1025066. [Google Scholar] [CrossRef]
- Kong, Y.R.; Tay, K.C.; Su, Y.X.; Wong, C.K.; Tan, W.N.; Khaw, K.Y. Potential of Naturally Derived Alkaloids as Multi-Targeted Therapeutic Agents for Neurodegenerative Diseases. Molecules 2021, 26, 728. [Google Scholar] [CrossRef]
- Shaito, A.; Posadino, A.M.; Younes, N.; Hasan, H.; Halabi, S.; Alhababi, D.; Al-Mohannadi, A.; Abdel-Rahman, W.M.; Eid, A.H.; Nasrallah, G.K.; et al. Potential Adverse Effects of Resveratrol: A Literature Review. Int. J. Mol. Sci. 2020, 21, 2084. [Google Scholar] [CrossRef]
- Hamayal, M.; Shahid, W.; Akhtar, C.H.; Awwab, M.; Hussain, S.; Ahmad, N. Effect of eucalyptus oil on symptoms of allergic rhinitis: A systematic review. Indian J. Otolaryngol. Head Neck Surg. 2025, 77, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Pengfei, L.; Xiaozhou, J.; Yan, Q.; Shili, L.; Zhibin, S. Advances in Study on Phenolic Acids. Guangdong Chem. Ind. 2017, 44, 50–52. [Google Scholar]
- Szwajgier, D.; Baranowska-Wojcik, E.; Borowiec, K. Phenolic Acids Exert Anticholinesterase and Cognition-Improving Effects. Curr. Alzheimer Res. 2018, 15, 531–543. [Google Scholar] [CrossRef]
- Bialecka-Florjanczyk, E.; Fabiszewska, A.; Zieniuk, B. Phenolic Acids Derivatives—Biotechnological Methods of Synthesis and Bioactivity. Curr. Pharm. Biotechnol. 2018, 19, 1098–1113. [Google Scholar] [CrossRef]
- Zhou, Q.; Lan, W.; Xie, J. Phenolic acid-chitosan derivatives: An effective strategy to cope with food preservation problems. Int. J. Biol. Macromol. 2024, 254, 127917. [Google Scholar] [CrossRef] [PubMed]
- Kurano, T.; Kanazawa, T.; Ooba, A.; Masuyama, Y.; Maruhana, N.; Yamada, M.; Iioka, S.; Ibaraki, H.; Kosuge, Y.; Kondo, H.; et al. Nose-to-brain/spinal cord delivery kinetics of liposomes with different surface properties. J. Control. Release 2022, 344, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Hao, R.; Chen, J.; Li, S.; Huang, K.; Cao, H.; Farag, M.A.; Battino, M.; Daglia, M.; Capanoglu, E.; et al. Health benefits of saponins and its mechanisms: Perspectives from absorption, metabolism, and interaction with gut. Crit. Rev. Food Sci. Nutr. 2024, 64, 9311–9332. [Google Scholar] [CrossRef]
- Lin, C.F.; Leu, Y.L.; Al-Suwayeh, S.A.; Ku, M.C.; Hwang, T.L.; Fang, J.Y. Anti-inflammatory activity and percutaneous absorption of quercetin and its polymethoxylated compound and glycosides: The relationships to chemical structures. Eur. J. Pharm. Sci. 2012, 47, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Mirchandani, Y.; Patravale, V.B.; S, B. Solid lipid nanoparticles for hydrophilic drugs. J. Control. Release 2021, 335, 457–464. [Google Scholar] [CrossRef]
- Dai, W.G.; Dong, L.C.; Song, Y. Enhanced bioavailability of poorly absorbed hydrophilic compounds through drug complex/in situ gelling formulation. Int. J. Pharm. 2013, 457, 63–70. [Google Scholar] [CrossRef]
- Wang, H.; Cui, Y.; Fu, Q.; Deng, B.; Li, G.; Yang, J.; Wu, T.; Xie, Y. A phospholipid complex to improve the oral bioavailability of flavonoids. Drug Dev. Ind. Pharm. 2015, 41, 1693–1703. [Google Scholar] [CrossRef]
- Miao-Miao, Y.; Hai-Hua, S.; Yue, H.; Ming, T.; Yi-Liang, L.; Wen-Bin, H. Research progress in cocrystal improvement of druggable properties of flavonoids. Cent. South Pharm. 2024, 22, 715–723. [Google Scholar]
- Shan, Q.; Yu, W.; Xu, Q.; Liu, R.; Ying, S.; Dong, J.; Bao, Y.; Lyu, Q.; Shi, C.; Xia, J.; et al. Detoxification and underlying mechanisms towards toxic alkaloids by Traditional Chinese Medicine processing: A comprehensive review. Phytomedicine 2024, 129, 155623. [Google Scholar] [CrossRef]
- Guo, X.; Luo, W.; Wu, L.; Zhang, L.; Chen, Y.; Li, T.; Li, H.; Zhang, W.; Liu, Y.; Zheng, J.; et al. Natural Products from Herbal Medicine Self-Assemble into Advanced Bioactive Materials. Adv. Sci. (Weinh) 2024, 11, e2403388. [Google Scholar] [CrossRef]
- Trimarchi, M.; Bussi, M.; Sinico, R.A.; Meroni, P.; Specks, U. Cocaine-induced midline destructive lesions—An autoimmune disease? Autoimmun. Rev. 2013, 12, 496–500. [Google Scholar] [CrossRef] [PubMed]
- Lason, E. Topical Administration of Terpenes Encapsulated in Nanostructured Lipid-Based Systems. Molecules 2020, 25, 5758. [Google Scholar] [CrossRef]
- Nair, A.B.; Chaudhary, S.; Jacob, S.; Patel, D.; Shinu, P.; Shah, H.; Chaudhary, A.; Aldhubiab, B.; Almuqbil, R.M.; Alnaim, A.S.; et al. Intranasal Administration of Dolutegravir-Loaded Nanoemulsion-Based In Situ Gel for Enhanced Bioavailability and Direct Brain Targeting. Gels 2023, 9, 130. [Google Scholar] [CrossRef]
- Nuzzo, D.; Girgenti, A.; Palumbo, L.; Naselli, F.; Bavetta, M.; Marfia, G.; Picone, P. Vesicles: New Advances in the Treatment of Neurodegenerative Diseases. Int. J. Mol. Sci. 2024, 25, 12672. [Google Scholar] [CrossRef]
- Akel, H.; Csoka, I.; Ambrus, R.; Bocsik, A.; Grof, I.; Meszaros, M.; Szecsko, A.; Kozma, G.; Veszelka, S.; Deli, M.A.; et al. In Vitro Comparative Study of Solid Lipid and PLGA Nanoparticles Designed to Facilitate Nose-to-Brain Delivery of Insulin. Int. J. Mol. Sci. 2021, 22, 13258. [Google Scholar] [CrossRef]
- Alvarez-Erviti, L.; Seow, Y.; Yin, H.; Betts, C.; Lakhal, S.; Wood, M.J.A. Delivery of siRNA to the mouse brain by systemic injection of targeted exosomes. Nat. Biotechnol. 2011, 29, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.H.; Betrehem, U.M.; Ali, N.; Khan, A.; Ali, F.; Nawaz, S.; Sajid, M.; Yang, Y.; Chen, T.; Bilal, M. Design strategies, surface functionalization, and environmental remediation potentialities of polymer-functionalized nanocomposites. Chemosphere 2022, 306, 135656. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Chen, G.; Zhang, J. A Review of Liposomes as a Drug Delivery System: Current Status of Approved Products, Regulatory Environments, and Future Perspectives. Molecules 2022, 27, 1372. [Google Scholar] [CrossRef]
- Bonferoni, M.C.; Rossi, S.; Sandri, G.; Ferrari, F.; Gavini, E.; Rassu, G.; Giunchedi, P. Nanoemulsions for “Nose-to-Brain” Drug Delivery. Pharmaceutics 2019, 11, 84. [Google Scholar] [CrossRef]
- Nguyen, H.X.; Nguyen, C.N. Microneedle-Mediated Transdermal Delivery of Biopharmaceuticals. Pharmaceutics 2023, 15, 277. [Google Scholar] [CrossRef]
- Qiao, L.; Yang, H.; Gao, S.; Li, L.; Fu, X.; Wei, Q. Research progress on self-assembled nanodrug delivery systems. J. Mater. Chem. B 2022, 10, 1908–1922. [Google Scholar] [CrossRef] [PubMed]

| Disease | Etiology | Age of Onset | Characteristic Clinical Manifestations | Reference |
|---|---|---|---|---|
| Alzheimer’s disease | Genetic factors: APP, PSEN1, and PSEN2 gene mutations; the APOE ε4 allele increases the risk. Environmental factors: age, hypertension, diabetes, head trauma, etc. | Predominantly occurs after 65 years (late-onset), with rare presentations before 65 (early-onset). | Cognitive manifestations: memory impairment (especially recent memory), language dysfunction, and disorientation. Behavioral symptoms: depression, anxiety, apathy, and hallucinations. Functional decline: decreased ability to perform activities of daily living. | [4] |
| Parkinson’s disease | Genetic factors: LRRK2, PARK2, SNCA, and other gene mutations. Environmental factors: exposure to pesticides, heavy metals, etc. Neuropathology: loss of dopaminergic neurons in substantia nigra. | Predominantly occurs at 50–70 years, with rare presentations before 50 (early-onset). | Movement symptoms: resting tremor, rigidity, bradykinesia, and postural imbalance. Non-motor symptoms: hyposmia, constipation, depression, and sleep disturbances. | [5] |
| Huntington’s disease | Genetic factors: CAG trinucleotide repeat amplification (>40 times) in the HTT gene. | Predominantly occurs at 30–50 years, with rare presentations before 20 (early-onset) or after 50 (late-onset). | Motor symptoms: choreiform movements, dystonia, and gait abnormalities. Cognitive symptoms: executive dysfunction and memory loss. Psychiatric symptoms: depression, anxiety, irritability, and psychotic symptoms. | [6] |
| Amyotrophic lateral sclerosis | Genetic factors: SOD1, C9ORF72, TARDBP, and other gene mutations. Environmental factors: smoking, heavy metal exposure, strenuous exercise, etc. | Predominantly occurs at 40–70 years, with rare presentations before 40 (early-onset). | Motor symptoms: muscle weakness, neurogenic atrophy (typically from the extremities or medulla oblongata), and fasciculation. Function decline: dysphagia, dysarthria, and dyspnea. Cognitive symptoms: Co-occurring frontotemporal dementia in subset of patients | [7] |
| Spinal muscular atrophy | Hereditary factors: Deletion or mutation of the SMN1 gene, resulting in a deficiency of the motor neuron survival protein (SMN). | Infants (0–6 months), children (6 months–18 years), and adults (after 18 years). | Motor symptoms: progressive muscle weakness and muscle atrophy (proximal heavier than distal). Function decline: dyspnea and dysphagia (severe type). Others: Scoliosis and joint contracture. | [8] |
| Hereditary spastic paraplegia | Genetic factors: SPAST, ATL1, REEP1, and other gene mutations. Pathology: degeneration of corticospinal tract. | Predominantly occurs 10–40 years, with rare presentations before 10 or after 40. | Movement symptoms: spastic weakness of lower limbs and abnormal gait. Other symptoms: bladder dysfunction and mild cognitive impairment (complex hereditary spastic paraplegia). | [9] |
| Multiple sclerosis | Genetic factors: HLA-DRB1 gene polymorphism. Environmental factors: viral infection, vitamin D deficiency, smoking, etc. -Pathology: demyelination and inflammation of the central nervous system. | Predominantly occurs 20–40 years, with rare presentations before 20 or after 40. | Motor symptoms: limb weakness, ataxia, and spasticity. Sensory symptoms: numbness, tingling, and decreased vision (optic neuritis). Other symptoms: fatigue, cognitive impairment, and bladder dysfunction. | [10] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, Y.; Ma, X.; Liu, S.; Zong, S.; Cheng, Y.; Zhang, H.; Wang, C.; Li, Y. Application of Natural Products in Neurodegenerative Diseases by Intranasal Administration: A Review. Pharmaceutics 2025, 17, 675. https://doi.org/10.3390/pharmaceutics17050675
Jin Y, Ma X, Liu S, Zong S, Cheng Y, Zhang H, Wang C, Li Y. Application of Natural Products in Neurodegenerative Diseases by Intranasal Administration: A Review. Pharmaceutics. 2025; 17(5):675. https://doi.org/10.3390/pharmaceutics17050675
Chicago/Turabian StyleJin, Yu, Xinyu Ma, Shuo Liu, Shiyu Zong, Yunlong Cheng, Hong Zhang, Chunliu Wang, and Ye Li. 2025. "Application of Natural Products in Neurodegenerative Diseases by Intranasal Administration: A Review" Pharmaceutics 17, no. 5: 675. https://doi.org/10.3390/pharmaceutics17050675
APA StyleJin, Y., Ma, X., Liu, S., Zong, S., Cheng, Y., Zhang, H., Wang, C., & Li, Y. (2025). Application of Natural Products in Neurodegenerative Diseases by Intranasal Administration: A Review. Pharmaceutics, 17(5), 675. https://doi.org/10.3390/pharmaceutics17050675