

3D Printing Direct Powder Extrusion in the Production of Drug Delivery Systems: State of the Art and Future Perspectives



Abstract
1. Introduction
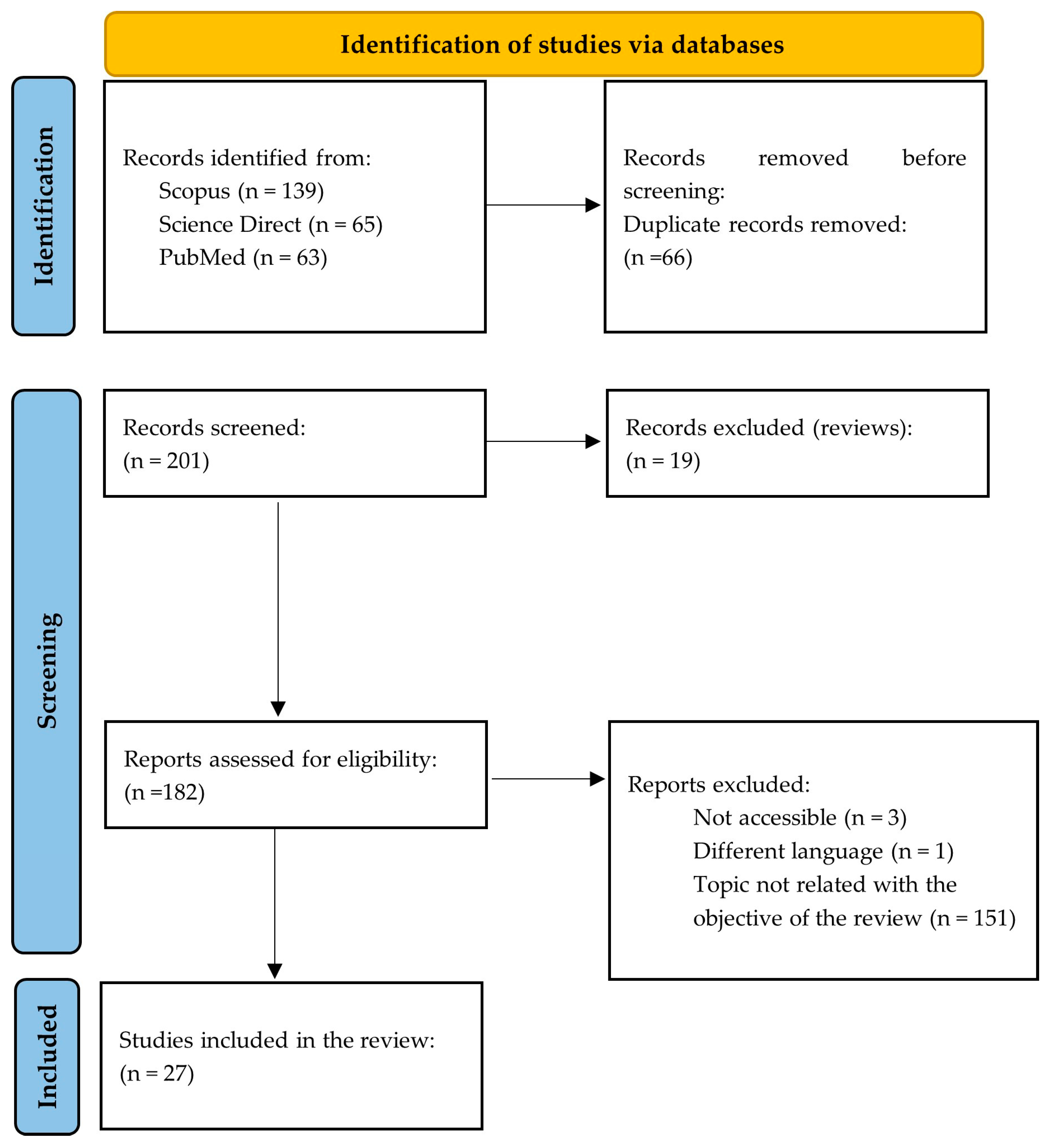
2. Methodology
3. Results
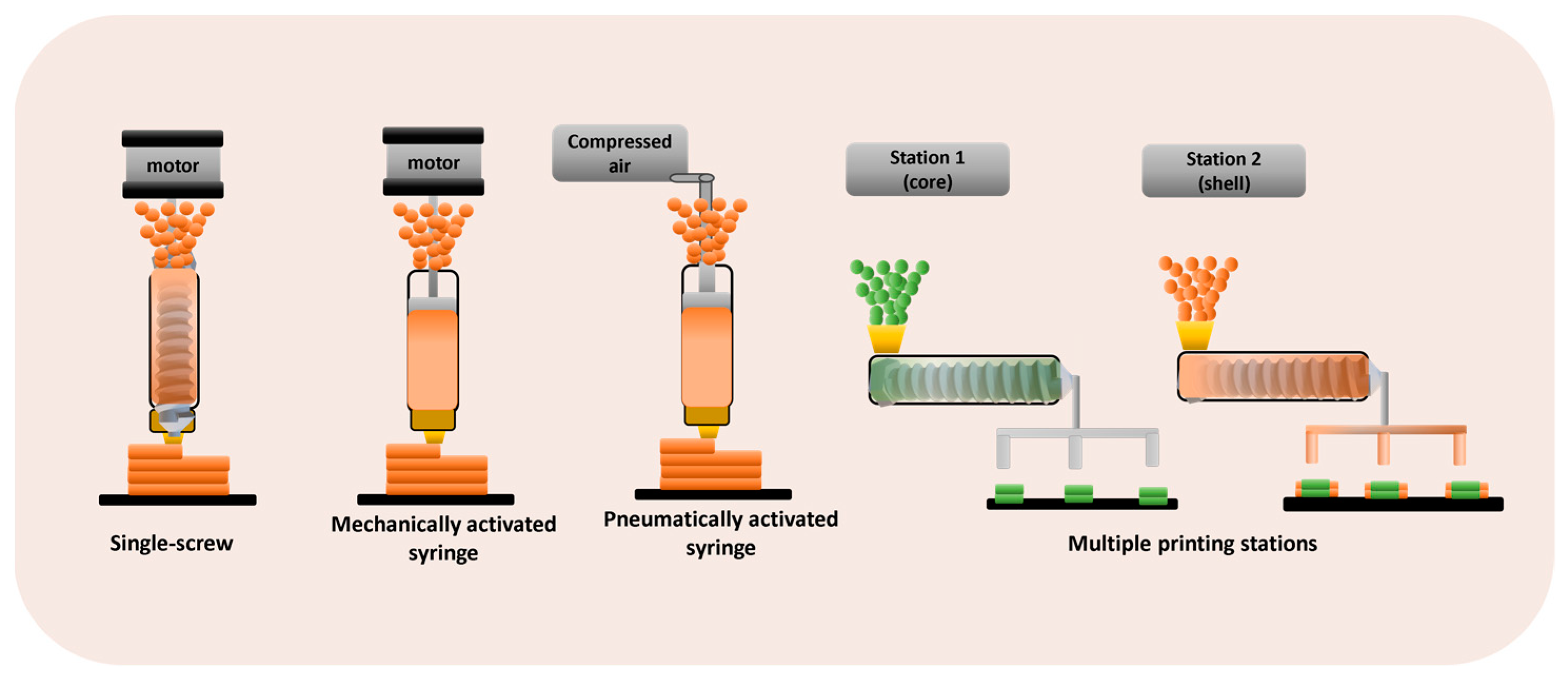
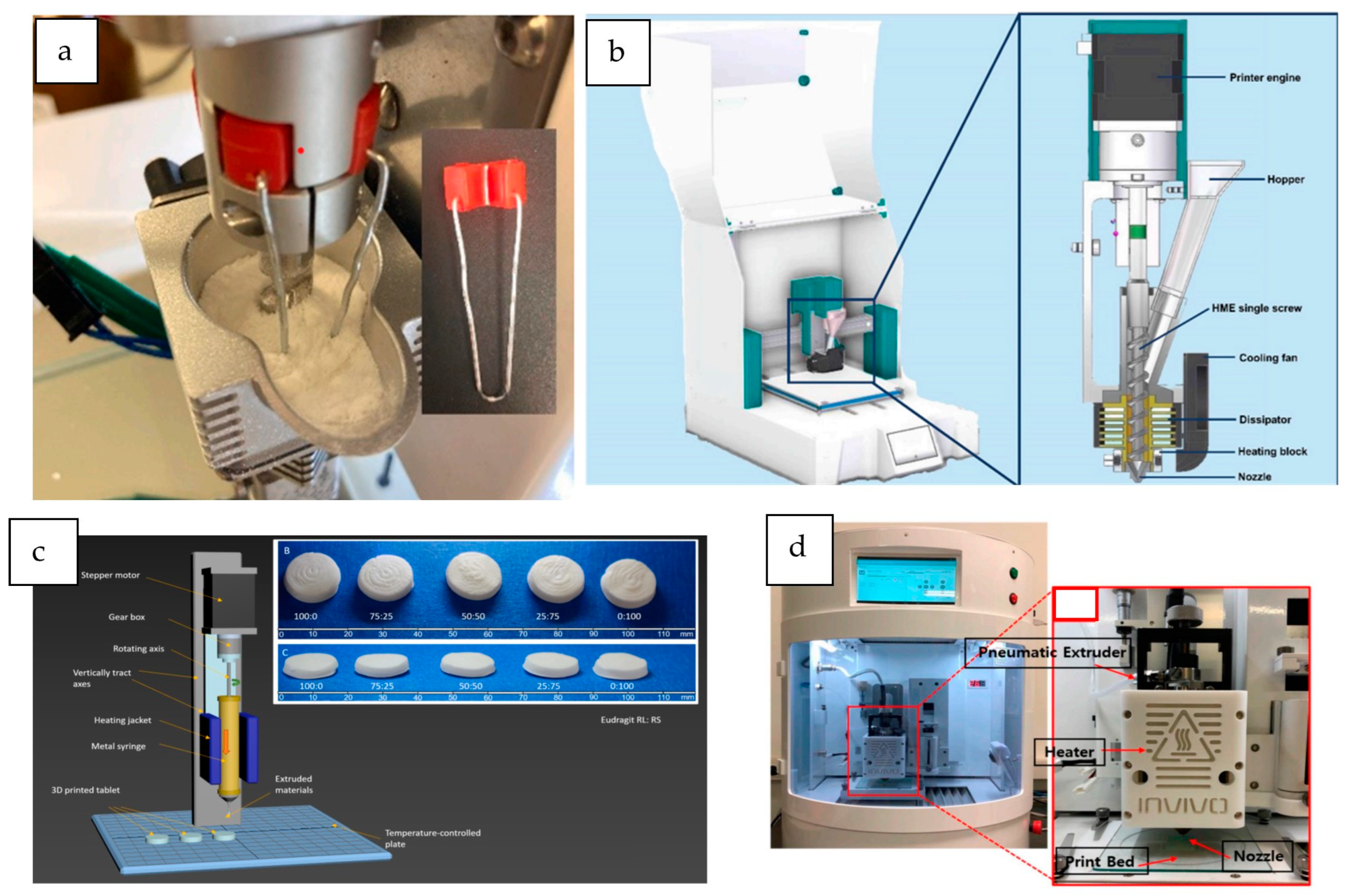
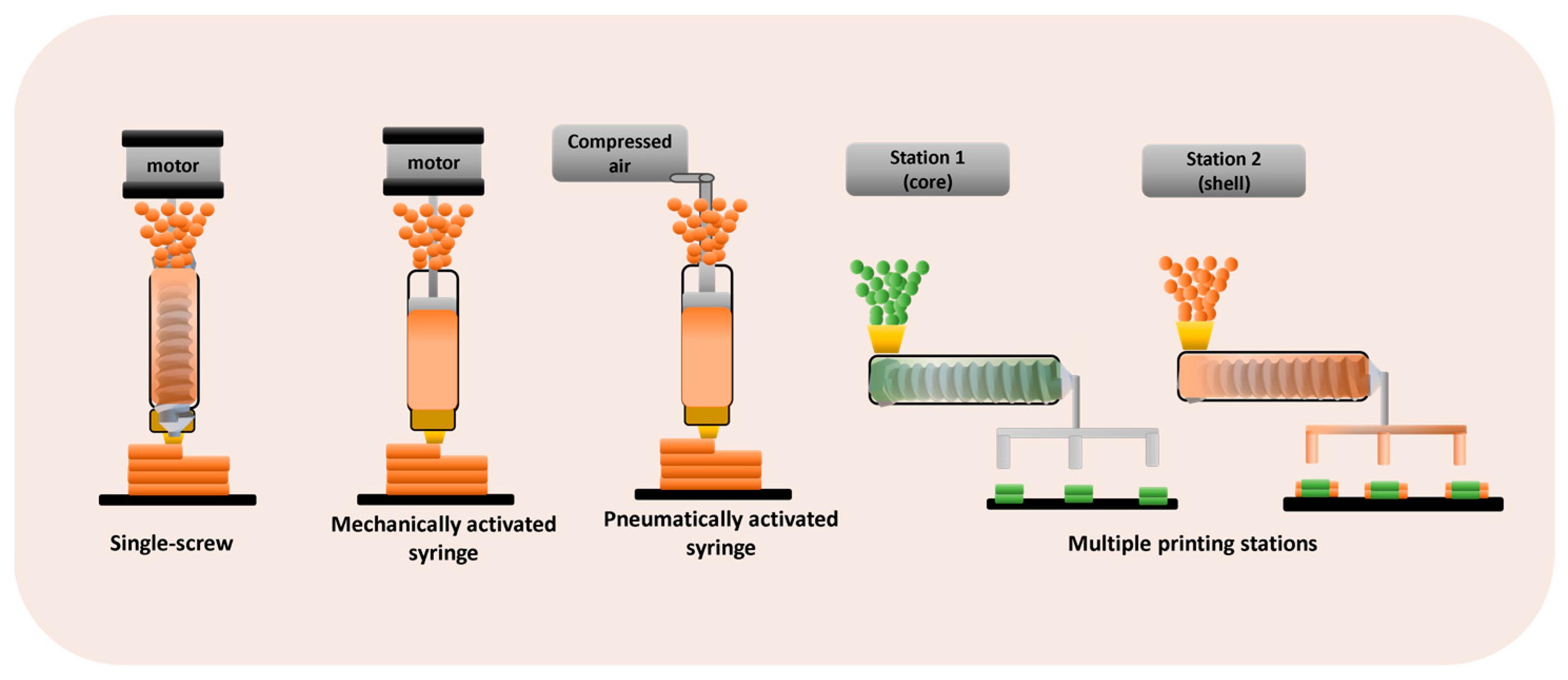
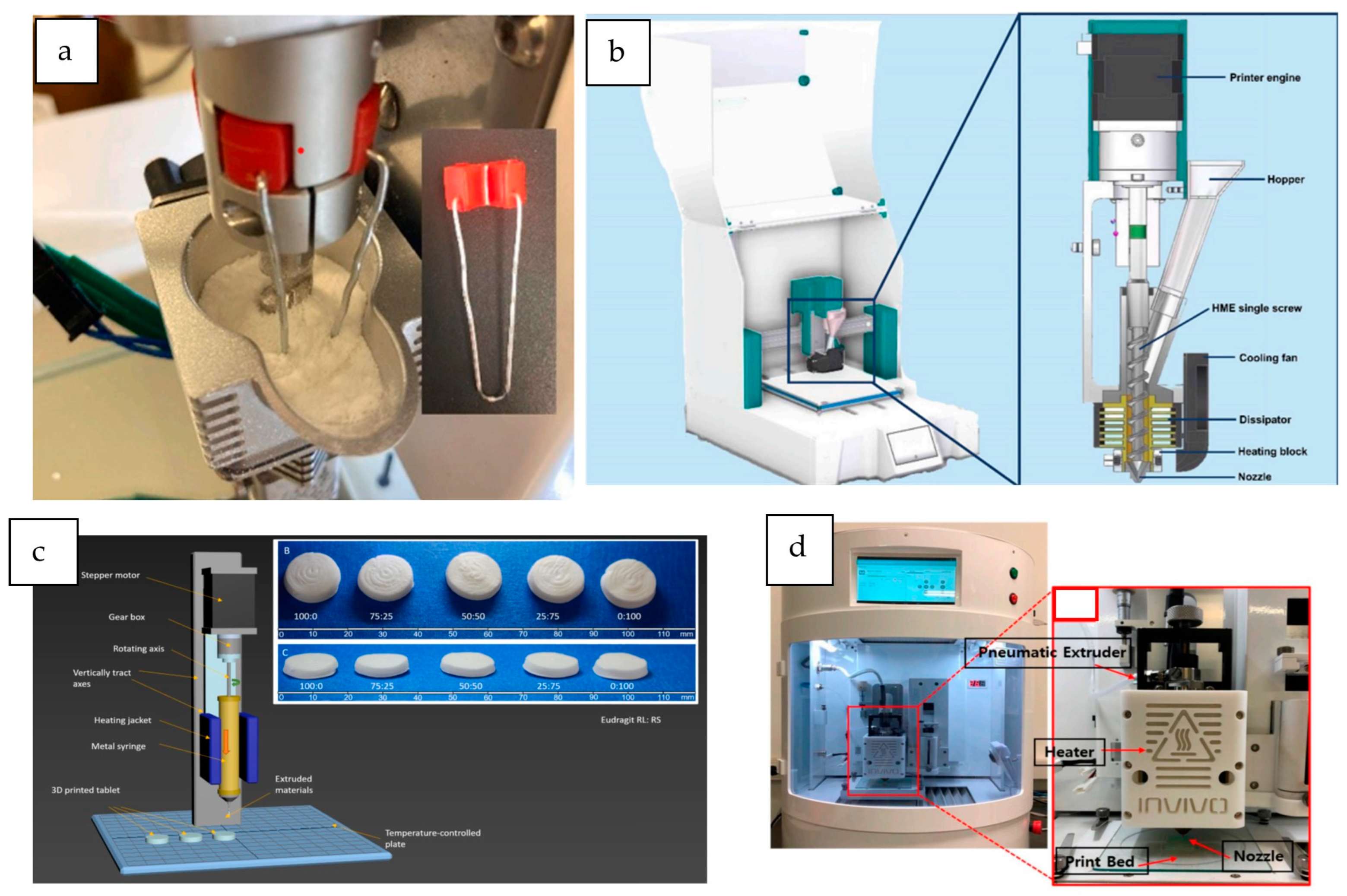
3.1. DPE 3D Printers
3.1.1. Single-Screw DPE 3D Printers
3.1.2. 3D Printers Based on a Mechanical Syringe System
3.1.3. 3D Printers Based on a Pneumatic Syringe System
3.2. Critical Formulation and Printing Parameters
3.2.1. Amount of Feeding Material
3.2.2. Rheological Parameters
3.2.3. Flowability
3.2.4. Printing and Platform Temperatures
3.2.5. Other Printing Parameters
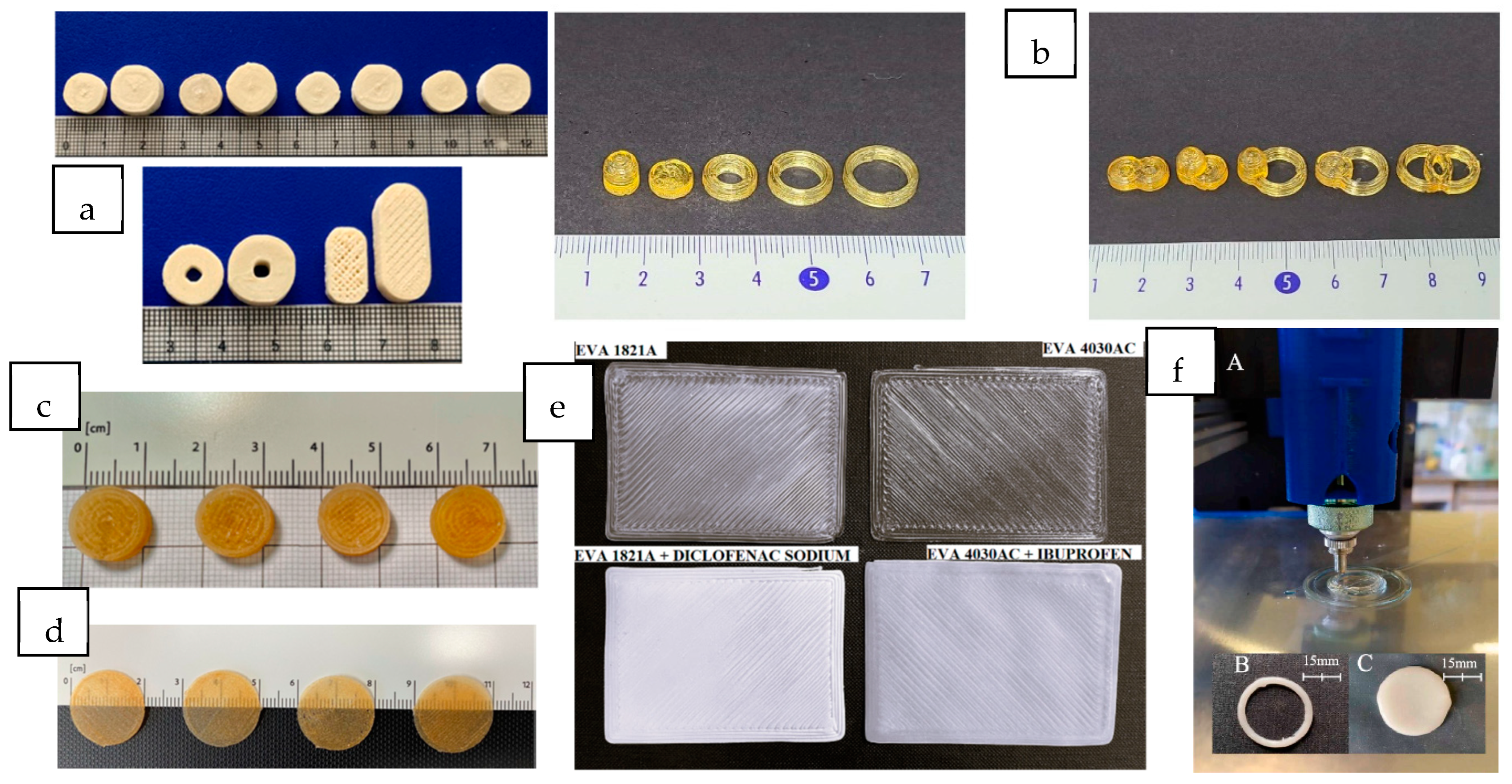
3.3. Drug Delivery Systems Based in DPE
3.3.1. Oral Administration
- 3D-printed tablets
- Core–shell 3D-printed tablets
- 3D-printed minitablets
- Multicomponent tablets
3.3.2. Buccal Administration
- Orodispersible Films (ODFs)
3.3.3. Transdermal Route
- Patches
3.3.4. Parenteral
- Implants
4. Discussion
5. Conclusions
6. Future Directions
- Economic and Environmental Impact: 3D printing techniques have great potential in the development of sustainable drug delivery systems. Although 3D printing is not a waste-free manufacturing technique, it generates less waste than traditional manufacturing processes, decreasing its environmental footprint. Sustainability of DPE 3D printing could be achieved through optimized material usage and recycling. The use of biodegradable, biocompatible, and eco-friendly polymers could help minimize environmental impact. Besides its sustainability, single-step DPE appears to be an innovative 3D printing technique for small-scale manufacturing of personalized dosage forms compared with rigid and multi-step conventional manufacturing processes. However, to improve its cost-efficiency, it would be essential to develop 3D printers with higher printing speeds. With regards to productivity and time efficiency, DPE also has clear advantages compared with other 3D printing material-extrusion techniques, such as FDM. Since there is no need for filament feedstock preparation, formulation development will be accelerated, and the cost of production of drug delivery systems will be reduced. Moreover, the small amount of powder blend required (only a few grams) also contributes to the cost-efficiency of this manufacturing process. This fact is particularly advantageous when processing high-cost drugs, such as orphan drugs. Moreover, in contrast with other 3D printing techniques such as SSE, which usually need a post-processing drying step, drug delivery systems prepared by DPE have no post-printing requirements, shortening the time needed to prepare the medical prescription [16,17,23,24,33,63,64,65].
- Regulatory Challenges: The future of DPE will probably be the application in clinical settings such as hospitals and compounding pharmacies, rather than the mass production of medicines. In this context, regulatory challenges need to be addressed. Due to the flexible and on-demand production process, standard regulations could not be applied, so new regulatory guidelines should be implemented. Another key aspect is the standardization of DPE 3D printers to meet Good Manufacturing Practice (GMP) requirements, which is critical to guaranteeing the production of high-quality and safe medicines. In fact, some GMP-compliant DPE printers have been recently introduced. Moreover, the limited number of preclinical and clinical studies performed currently is another hurdle for the regulatory approval of 3D-printed pharmaceuticals [10,17,61,64,65].
- Long-Term Stability Issues: Since 3D-printed medicines are expected to be produced on-demand and dispensed extemporaneously, the long-term stability of the product should not be a significant problem. Nevertheless, several studies have carried out stability analyses, most of them conducted over a period of 3 months at 25 °C and 60% RH. The results of these studies highlight the absence of recrystallization and/or degradation of the drug [14,15,28,31].
- Challenges with Personalized Medicines: DPE offers unique benefits in the tailoring of the dosage forms. Pediatric and geriatric patients present physiological particularities that require dose adjustment. Furthermore, children have swallowing problems and are especially sensitive to the taste of the formulation. DPE has demonstrated its ability to solve these issues. Hospital pharmacy services have the necessary infrastructure to accommodate this technology. Due to their compact and user-friendly nature, DPE printers are particularly suitable to produce small batches of customized formulations in community and hospital pharmacy settings. The decentralized manufacture of pharmaceuticals could be beneficial from a logistical perspective, as transport costs and storage time could be reduced. However, it would be of outmost importance to protect patient privacy and guarantee data security in the implementation of DPE technology in decentralized healthcare locations [18,28,65,66,67,68].
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crișan, A.G.; Iurian, S.; Porfire, A.; Rus, L.M.; Bogdan, C.; Casian, T.; Lucacel, R.C.; Turza, A.; Porav, S.; Tomuță, I. QbD Guided Development of Immediate Release FDM-3D Printed Tablets with Customizable API Doses. Int. J. Pharm. 2022, 613, 121411. [Google Scholar] [CrossRef]
- Shi, K.; Slavage, J.P.; Maniruzzaman, M.; Nokhodchi, A. Role of Release Modifiers to Modulate Drug Release from Fused Deposition Modelling (FDM) 3D Printed Tablets. Int. J. Pharm. 2021, 597, 120315. [Google Scholar] [CrossRef]
- Goyanes, A.; Robles Martinez, P.; Buanz, A.; Basit, A.W.; Gaisford, S. Effect of Geometry on Drug Release from 3D Printed Tablets. Int. J. Pharm. 2015, 494, 657–663. [Google Scholar] [CrossRef]
- Shojaie, F.; Ferrero, C.; Caraballo, I. Development of 3D-Printed Bicompartmental Devices by Dual-Nozzle Fused Deposition Modeling (FDM) for Colon-Specific Drug Delivery. Pharmaceutics 2023, 15, 2362. [Google Scholar] [CrossRef]
- Anaya, B.J.; Cerda, J.R.; D’Atri, R.M.; Yuste, I.; Luciano, F.C.; Kara, A.; Ruiz, H.K.; Ballesteros, M.P.; Serrano, D.R. Engineering of 3D Printed Personalized Polypills for the Treatment of the Metabolic Syndrome. Int. J. Pharm. 2023, 642, 123194. [Google Scholar] [CrossRef]
- Pereira, B.C.; Isreb, A.; Forbes, R.T.; Dores, F.; Habashy, R.; Petit, J.B.; Alhnan, M.A.; Oga, E.F. ‘Temporary Plasticiser’: A Novel Solution to Fabricate 3D Printed Patient-Centred Cardiovascular ‘Polypill’ Architectures. Eur. J. Pharm. Biopharm. 2019, 135, 94–103. [Google Scholar] [CrossRef]
- Khalid, G.M.; Billa, N. Solid Dispersion Formulations by FDM 3D Printing—A Review. Pharmaceutics 2022, 14, 690. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Vemula, S.K.; Bandari, S.; Repka, M.A. Preparation of Core-Shell Controlled Release Tablets Using Direct Powder Extrusion 3D Printing Techniques. J. Drug Deliv. Sci. Technol. 2023, 88, 104896. [Google Scholar] [CrossRef]
- Díaz-Torres, E.; Rodríguez-Pombo, L.; Ong, J.J.; Basit, A.W.; Santoveña-Estévez, A.; Fariña, J.B.; Alvarez-Lorenzo, C.; Goyanes, A. Integrating Pressure Sensor Control into Semi-Solid Extrusion 3D Printing to Optimize Medicine Manufacturing. Int. J. Pharm. X 2022, 4, 100133. [Google Scholar] [CrossRef] [PubMed]
- Seoane-Viaño, I.; Januskaite, P.; Alvarez-Lorenzo, C.; Basit, A.W.; Goyanes, A. Semi-Solid Extrusion 3D Printing in Drug Delivery and Biomedicine: Personalised Solutions for Healthcare Challenges. J. Control. Release 2021, 332, 367–389. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Chi, B.; Jiao, Z.; Tan, J.; Liu, F.; Yang, W. A Large-Scale Double-Stage-Screw 3D Printer for Fused Deposition of Plastic Pellets. J. Appl. Polym. Sci. 2017, 134, 45147. [Google Scholar] [CrossRef]
- Feuerbach, T.; Thommes, M. Design and Characterization of a Screw Extrusion Hot-End for Fused Deposition Modeling. Molecules 2021, 26, 590. [Google Scholar] [CrossRef] [PubMed]
- Borandeh, S.; van Bochove, B.; Teotia, A.; Seppälä, J. Polymeric Drug Delivery Systems by Additive Manufacturing. Adv. Drug Deliv. Rev. 2021, 173, 349–373. [Google Scholar] [CrossRef]
- Pistone, M.; Racaniello, G.F.; Arduino, I.; Laquintana, V.; Lopalco, A.; Cutrignelli, A.; Rizzi, R.; Franco, M.; Lopedota, A.; Denora, N. Direct Cyclodextrin-Based Powder Extrusion 3D Printing for One-Step Production of the BCS Class II Model Drug Niclosamide. Drug Deliv. Transl. Res. 2022, 12, 1895–1910. [Google Scholar] [CrossRef]
- Pistone, M.; Racaniello, G.F.; Rizzi, R.; Iacobazzi, R.M.; Arduino, I.; Lopalco, A.; Lopedota, A.A.; Denora, N. Direct Cyclodextrin Based Powder Extrusion 3D Printing of Budesonide Loaded Mini-Tablets for the Treatment of Eosinophilic Colitis in Paediatric Patients. Int. J. Pharm. 2023, 632, 122592. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Guirales, S.A.; Jurado, N.; Kara, A.; Lalatsa, A.; Serrano, D.R. Understanding Direct Powder Extrusion for Fabrication of 3D Printed Personalised Medicines: A Case Study for Nifedipine Minitablets. Pharmaceutics 2021, 13, 1583. [Google Scholar] [CrossRef]
- Annaji, M.; Ramesh, S.; Poudel, I.; Govindarajulu, M.; Arnold, R.D.; Dhanasekaran, M.; Babu, R.J. Application of Extrusion-Based 3D Printed Dosage Forms in the Treatment of Chronic Diseases. J. Pharm. Sci. 2020, 109, 3551–3568. [Google Scholar] [CrossRef] [PubMed]
- Malebari, A.M.; Kara, A.; Khayyat, A.N.; Mohammad, K.A.; Serrano, D.R. Development of Advanced 3D-Printed Solid Dosage Pediatric Formulations for HIV Treatment. Pharmaceuticals 2022, 15, 435. [Google Scholar] [CrossRef]
- Muhindo, D.; Ashour, E.A.; Almutairi, M.; Repka, M.A. Development of Subdermal Implants Using Direct Powder Extrusion 3D Printing and Hot-Melt Extrusion Technologies. AAPS PharmSciTech 2023, 24, 215. [Google Scholar] [CrossRef]
- Goyanes, A.; Allahham, N.; Trenfield, S.J.; Stoyanov, E.; Gaisford, S.; Basit, A.W. Direct Powder Extrusion 3D Printing: Fabrication of Drug Products Using a Novel Single-Step Process. Int. J. Pharm. 2019, 567, 118471. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Zheng, Y.; Deng, F.; Wang, B.; Wu, Y.; Luo, Q.; Zuo, X.; Liu, X.; Cao, L.; Li, M.; Lu, H.; et al. Melt Extrusion Deposition (MEDTM) 3D Printing Technology—A Paradigm Shift in Design and Development of Modified Release Drug Products. Int. J. Pharm. 2021, 602, 120639. [Google Scholar] [CrossRef]
- Rosch, M.; Gutowski, T.; Baehr, M.; Eggert, J.; Gottfried, K.; Gundler, C.; Nürnberg, S.; Langebrake, C.; Dadkhah, A. Development of an Immediate Release Excipient Composition for 3D Printing via Direct Powder Extrusion in a Hospital. Int. J. Pharm. 2023, 643, 123218. [Google Scholar] [CrossRef] [PubMed]
- Kuźmińska, M.; Pereira, B.C.; Habashy, R.; Peak, M.; Isreb, M.; Gough, T.D.; Isreb, A.; Alhnan, M.A. Solvent-Free Temperature-Facilitated Direct Extrusion 3D Printing for Pharmaceuticals. Int. J. Pharm. 2021, 598, 120305. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.-W.; Baek, S.-H.; Lee, B.-J.; Jin, H.-E. Orodispersible Polymer Films with the Poorly Water-Soluble Drug, Olanzapine: Hot-Melt Pneumatic Extrusion for Single-Process 3D Printing. Pharmaceutics 2020, 12, 692. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.J.; Awad, A.; Martorana, A.; Gaisford, S.; Stoyanov, E.; Basit, A.W.; Goyanes, A. 3D Printed Opioid Medicines with Alcohol-Resistant and Abuse-Deterrent Properties. Int. J. Pharm. 2020, 579, 119169. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-de-Leyva, Á.; Linares, V.; Domínguez-Robles, J.; Casas, M.; Caraballo, I. Extrusion-Based Technologies for 3D Printing: A Comparative Study of the Processability of Thermoplastic Polyurethane-Based Formulations. Pharm. Dev. Technol. 2023, 28, 939–947. [Google Scholar] [CrossRef]
- Boniatti, J.; Januskaite, P.; Fonseca, L.B.d.; Viçosa, A.L.; Amendoeira, F.C.; Tuleu, C.; Basit, A.W.; Goyanes, A.; Ré, M.-I. Direct Powder Extrusion 3D Printing of Praziquantel to Overcome Neglected Disease Formulation Challenges in Paediatric Populations. Pharmaceutics 2021, 13, 1114. [Google Scholar] [CrossRef] [PubMed]
- Seoane-Viaño, I.; Xu, X.; Ong, J.J.; Teyeb, A.; Gaisford, S.; Campos-Álvarez, A.; Stulz, A.; Marcuta, C.; Kraschew, L.; Mohr, W.; et al. A Case Study on Decentralized Manufacturing of 3D Printed Medicines. Int. J. Pharm. X 2023, 5, 100184. [Google Scholar] [CrossRef]
- Pflieger, T.; Venkatesh, R.; Dachtler, M.; Eggenreich, K.; Laufer, S.; Lunter, D. Novel Approach to Pharmaceutical 3D-Printing Omitting the Need for Filament—Investigation of Materials, Process, and Product Characteristics. Pharmaceutics 2022, 14, 2488. [Google Scholar] [CrossRef]
- Racaniello, G.F.; Pistone, M.; Meazzini, C.; Lopedota, A.; Arduino, I.; Rizzi, R.; Lopalco, A.; Musazzi, U.M.; Cilurzo, F.; Denora, N. 3D Printed Mucoadhesive Orodispersible Films Manufactured by Direct Powder Extrusion for Personalized Clobetasol Propionate Based Paediatric Therapies. Int. J. Pharm. 2023, 643, 123214. [Google Scholar] [CrossRef] [PubMed]
- Maurizii, G.; Moroni, S.; Khorshid, S.; Aluigi, A.; Tiboni, M.; Casettari, L. 3D-Printed EVA-Based Patches Manufactured by Direct Powder Extrusion for Personalized Transdermal Therapies. Int. J. Pharm. 2023, 635, 122720. [Google Scholar] [CrossRef] [PubMed]
- Moroni, S.; Khorshid, S.; Aluigi, A.; Tiboni, M.; Casettari, L. Poly(3-Hydroxybutyrate): A Potential Biodegradable Excipient for Direct 3D Printing of Pharmaceuticals. Int. J. Pharm. 2022, 623, 121960. [Google Scholar] [CrossRef] [PubMed]
- Samaro, A.; Shaqour, B.; Goudarzi, N.M.; Ghijs, M.; Cardon, L.; Boone, M.N.; Verleije, B.; Beyers, K.; Vanhoorne, V.; Cos, P.; et al. Can Filaments, Pellets and Powder Be Used as Feedstock to Produce Highly Drug-Loaded Ethylene-Vinyl Acetate 3D Printed Tablets Using Extrusion-Based Additive Manufacturing? Int. J. Pharm. 2021, 607, 120922. [Google Scholar] [CrossRef]
- Jennotte, O.; Koch, N.; Lechanteur, A.; Rosoux, F.; Emmerechts, C.; Beeckman, E.; Evrard, B. Feasibility Study of the Use of a Homemade Direct Powder Extrusion Printer to Manufacture Printed Tablets with an Immediate Release of a BCS II Molecule. Int. J. Pharm. 2023, 646, 123506. [Google Scholar] [CrossRef]
- Feuerbach, T.; Kock, S.; Thommes, M. Characterisation of Fused Deposition Modeling 3D Printers for Pharmaceutical and Medical Applications. Pharm. Dev. Technol. 2018, 23, 1136–1145. [Google Scholar] [CrossRef]
- Manini, G.; Deldime, M.; Benali, S.; Raquez, J.M.; Goole, J. Long-Acting Implantable Dosage Forms Containing Paliperidone Palmitate Obtained by 3D Printing. Int. J. Pharm. 2021, 603, 120702. [Google Scholar] [CrossRef]
- Liu, B.; Han, X.; Wang, Z.; Zhang, H.; Liu, N.; Gao, X.; Gao, J.; Zheng, A. Three-Dimensional Printing Personalized Acetaminophen Sustained-Release Tablets Using Hot Melt Extrusion. J. Drug Deliv. Sci. Technol. 2021, 66, 102855. [Google Scholar] [CrossRef]
- Fanous, M.; Gold, S.; Muller, S.; Hirsch, S.; Ogorka, J.; Imanidis, G. Simplification of Fused Deposition Modeling 3D-Printing Paradigm: Feasibility of 1-Step Direct Powder Printing for Immediate Release Dosage Form Production. Int. J. Pharm. 2020, 578, 119124. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Lee, J.C.; Ko, J.Y.; Lee, S.H.; Kim, N.A.; Jeong, S.H. 3D-Printed Tablets Using a Single-Step Hot-Melt Pneumatic Process for Poorly Soluble Drugs. Int. J. Pharm. 2021, 595, 120257. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Song, C.; Noh, I.; Song, S.; Rhee, Y.-S. Hot-Melt 3D Extrusion for the Fabrication of Customizable Modified-Release Solid Dosage Forms. Pharmaceutics 2020, 12, 738. [Google Scholar] [CrossRef]
- Ćwikła, G.; Grabowik, C.; Kalinowski, K.; Paprocka, I.; Ociepka, P. The Influence of Printing Parameters on Selected Mechanical Properties of FDM/FFF 3D-Printed Parts. IOP Conf. Ser. Mater. Sci. Eng. 2017, 227, 012033. [Google Scholar] [CrossRef]
- Cailleaux, S.; Sanchez-Ballester, N.M.; Gueche, Y.A.; Bataille, B.; Soulairol, I. Fused Deposition Modeling (FDM), the New Asset for the Production of Tailored Medicines. J. Control. Release 2021, 330, 821–841. [Google Scholar] [CrossRef]
- Algahtani, M.S.; Mohammed, A.A.; Ahmad, J.; Abdullah, M.M.; Saleh, E. 3D Printing of Dapagliflozin Containing Self-Nanoemulsifying Tablets: Formulation Design and In Vitro Characterization. Pharmaceutics 2021, 13, 993. [Google Scholar] [CrossRef]
- Zidan, A.; Alayoubi, A.; Asfari, S.; Coburn, J.; Ghammraoui, B.; Cruz, C.N.; Ashraf, M. Development of Mechanistic Models to Identify Critical Formulation and Process Variables of Pastes for 3D Printing of Modified Release Tablets. Int. J. Pharm. 2019, 555, 109–123. [Google Scholar] [CrossRef]
- Almeida, A.; Possemiers, S.; Boone, M.N.; De Beer, T.; Quinten, T.; Van Hoorebeke, L.; Remon, J.P.; Vervaet, C. Ethylene Vinyl Acetate as Matrix for Oral Sustained Release Dosage Forms Produced via Hot-Melt Extrusion. Eur. J. Pharm. Biopharm. 2011, 77, 297–305. [Google Scholar] [CrossRef]
- Chung, S.; Zhang, P.; Repka, M.A. Fabrication of Timed-Release Indomethacin Core–Shell Tablets for Chronotherapeutic Drug Delivery Using Dual Nozzle Fused Deposition Modeling (FDM) 3D Printing. Eur. J. Pharm. Biopharm. 2023, 188, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Pan, Y.; Chen, D.; Xu, X.; Yan, G.; Fan, T. Design, Preparation and In Vitro Evaluation of Core–Shell Fused Deposition Modelling 3D-Printed Verapamil Hydrochloride Pulsatile Tablets. Pharmaceutics 2022, 14, 437. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Feng, S.; Almotairy, A.; Bandari, S.; Repka, M.A. Development of Multifunctional Drug Delivery System via Hot-Melt Extrusion Paired with Fused Deposition Modeling 3D Printing Techniques. Eur. J. Pharm. Biopharm. 2023, 183, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Reddy Dumpa, N.; Bandari, S.; Repka, M.A. Novel Gastroretentive Floating Pulsatile Drug Delivery System Produced via Hot-Melt Extrusion and Fused Deposition Modeling 3D Printing. Pharmaceutics 2020, 12, 52. [Google Scholar] [CrossRef]
- Frankiewicz, M.; Sznitowska, M. Design of Experiments as a Tool to Optimize the Process of Coating Minitablets with Commercial Gastro-Resistant Coating Mixtures. Pharmaceutics 2022, 14, 1816. [Google Scholar] [CrossRef]
- Jacob, S.; Nair, A.B.; Boddu, S.H.S.; Gorain, B.; Sreeharsha, N.; Shah, J. An Updated Overview of the Emerging Role of Patch and Film-Based Buccal Delivery Systems. Pharmaceutics 2021, 13, 1206. [Google Scholar] [CrossRef]
- Magill, E.; Demartis, S.; Gavini, E.; Permana, A.D.; Thakur, R.R.S.; Adrianto, M.F.; Waite, D.; Glover, K.; Picco, C.J.; Korelidou, A.; et al. Solid Implantable Devices for Sustained Drug Delivery. Adv. Drug Deliv. Rev. 2023, 199, 114950. [Google Scholar] [CrossRef]
- Stewart, S.; Domínguez-Robles, J.; Donnelly, R.; Larrañeta, E. Implantable Polymeric Drug Delivery Devices: Classification, Manufacture, Materials, and Clinical Applications. Polymers 2018, 10, 1379. [Google Scholar] [CrossRef]
- Sun, H.; Mei, L.; Song, C.; Cui, X.; Wang, P. The in Vivo Degradation, Absorption and Excretion of PCL-Based Implant. Biomaterials 2006, 27, 1735–1740. [Google Scholar] [CrossRef] [PubMed]
- Fuenmayor, E.; Forde, M.; Healy, A.; Devine, D.; Lyons, J.; McConville, C.; Major, I. Material Considerations for Fused-Filament Fabrication of Solid Dosage Forms. Pharmaceutics 2018, 10, 44. [Google Scholar] [CrossRef] [PubMed]
- Linares, V.; Aguilar-de-Leyva, Á.; Casas, M.; Caraballo, I. 3D Printed Fractal-like Structures with High Percentage of Drug for Zero-Order Colonic Release. Pharmaceutics 2022, 14, 2298. [Google Scholar] [CrossRef]
- Parulski, C.; Jennotte, O.; Lechanteur, A.; Evrard, B. Challenges of Fused Deposition Modeling 3D Printing in Pharmaceutical Applications: Where Are We Now? Adv. Drug Deliv. Rev. 2021, 175, 113810. [Google Scholar] [CrossRef]
- Aho, J.; Bøtker, J.P.; Genina, N.; Edinger, M.; Arnfast, L.; Rantanen, J. Roadmap to 3D-Printed Oral Pharmaceutical Dosage Forms: Feedstock Filament Properties and Characterization for Fused Deposition Modeling. J. Pharm. Sci. 2019, 108, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Nasereddin, J.M.; Wellner, N.; Alhijjaj, M.; Belton, P.; Qi, S. Development of a Simple Mechanical Screening Method for Predicting the Feedability of a Pharmaceutical FDM 3D Printing Filament. Pharm. Res. 2018, 35, 151. [Google Scholar] [CrossRef] [PubMed]
- Awad, A.; Trenfield, S.J.; Gaisford, S.; Basit, A.W. 3D Printed Medicines: A New Branch of Digital Healthcare. Int. J. Pharm. 2018, 548, 586–596. [Google Scholar] [CrossRef] [PubMed]
- Mora-Castaño, G.; Millán-Jiménez, M.; Linares, V.; Caraballo, I. Assessment of the Extrusion Process and Printability of Suspension-Type Drug-Loaded Affinisol TM Filaments for 3D Printing. Pharmaceutics 2022, 14, 871. [Google Scholar] [CrossRef] [PubMed]
- Putra, N.E.; Zhou, J.; Zadpoor, A.A. Sustainable Sources of Raw Materials for Additive Manufacturing of Bone-Substituting Biomaterials. Adv. Healthc. Mater. 2024, 13, 2301837. [Google Scholar] [CrossRef] [PubMed]
- Seoane-Viaño, I.; Trenfield, S.J.; Basit, A.W.; Goyanes, A. Translating 3D Printed Pharmaceuticals: From Hype to Real-World Clinical Applications. Adv. Drug Deliv. Rev. 2021, 174, 553–575. [Google Scholar] [CrossRef]
- Awad, A.; Trenfield, S.J.; Goyanes, A.; Gaisford, S.; Basit, A.W. Reshaping Drug Development Using 3D Printing. Drug Discov. Today 2018, 23, 1547–1555. [Google Scholar] [CrossRef]
- Basit, A.W.; Trendfield, S.J. 3D Printing of Pharmaceuticals and the Role of Pharmacy. Pharm. J. 2022, 308, 7959. [Google Scholar] [CrossRef]
- Andreadis, I.I.; Gioumouxouzis, C.I.; Eleftheriadis, G.K.; Fatouros, D.G. The Advent of a New Era in Digital Healthcare: A Role for 3D Printing Technologies in Drug Manufacturing? Pharmaceutics 2022, 14, 609. [Google Scholar] [CrossRef]
- Awad, A.; Trenfield, S.J.; Pollard, T.D.; Ong, J.J.; Elbadawi, M.; McCoubrey, L.E.; Goyanes, A.; Gaisford, S.; Basit, A.W. Connected Healthcare: Improving Patient Care Using Digital Health Technologies. Adv. Drug Deliv. Rev. 2021, 178, 113958. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DPE 3D Printer | Extrusion Mechanism | Feeding Materials | References |
|---|---|---|---|
| M3DIMAKER (FabRx, London, UK) | Single-screw | Powder | [20,23,26,27] |
| HME pellets | [28] | ||
| Powder from milled pellets | |||
| Granules obtained by dry granulation process | [29] | ||
| FlexdoseTM printer (DiHeSys, Schwäbisch Gmünd, Germany) | Single-screw | HME granules | [30] |
| 3DForMe (Farmalabor, Canosa, Italy) | Single-screw | Powder | [14,15,31] |
| Single-screw powder extruder (3D Cultures, Philadelphia, PA, USA) | Single-screw | Powder | [32,33] |
| Modified da Vinci 1.0 FFF 3D printer (XYZPrinting, Ridderkerk, The Netherlands) | Single-screw | Powder/pellets obtained by HME | [34] |
| Modified Prusa i3 MK2S 3D printer (Prusa Research, Prague, Czech Republic) | Single-screw | Powder | [35] |
| In-house developed FDM 3D printer | Single-screw | Powder | [12,36] |
| MEDTM 3D printer (Triastek, Nanjing, China) | Twin-screw | Powder | [22] |
| Hyrel 3D printer (Norcross, GA, USA) SR model coupled with a TAM 15 extruder | Mechanically activated syringe | Powder | [16,18] |
| 30 M model coupled with a VOL-25 printhead | [24,37] | ||
| MAM—II printer (Fuqifan Technology C., Ltd., Shangai, China) | Mechanically activated syringe | Powder | [38] |
| 3D bio-printer (BIO X and BIO X2) (Cellink, Gothenburg, Sweden) | Pneumatically activated syringe | Powder | [8,19] |
| RegenHU Bioprinter (RegenHU, Villaz-St-Pierre, Switzerland) | Pneumatically activated syringe | Powder | [39] |
| ROKIT INVIVO (ROKIT Healthcare, Seoul, Republic of Korea) | Pneumatically activated syringe | Powder | [25,40,41] |
| Printing Technology | Geometrical Shape | Drug (% w/w) | Polymers (% w/w) | Auxiliar Excipients | Printing/Platform Temperatures | Reference |
|---|---|---|---|---|---|---|
| Immediate drug release 3D-printed tablets | Cylinder | Efavirenz (5–35%) | Kollidon® VA64 (40%) | Mannitol 100 (20–55%) | 180–190 | [29] |
| Magnesium stearate (5%) | ||||||
| Cylinder | Levodopa (28%), Carbidopa (7.56%) | Kollidon® VA64 (20–30%) | Mannitol (10%)/ | 180 | [23] | |
| Torus | Kollicoat® IR (24.44–34.44%) | Compressol® SM (10%) | ||||
| Oblong | ||||||
| Cylinder | Praziquantel (35–50%) | Kollidon® VA64 (50–60%) | Kolliphor® SLS fine (5%)/ | 130–140 | [28] | |
| SpanTM 20 (5%) | ||||||
| Oval | Caffeine (10%) | HPC SSL (45–90%) | PEG 4000 (13.5%) | 155–180 | [39] | |
| Kollidon® VA64 (31.5%) | ||||||
| Cylinder | Metoprolol succinate (25%) | Kollidon® VA64 (65%) | PEG 1500 (5%) | 140/50 | [30] | |
| Eudragit® EPO (75%) | 140/50 | |||||
| Cylinder | Cannabidiol (10%) | Eudragit® E100 (18–40%) | PEO (49.5–72%) | 155/25 | [35] | |
| Soluplus® (18–40%) | ||||||
| Cube | Dutasteride (1%) | Soluplus® (89%) | Lutrol® F68 (10%) | 160/40 | [40] | |
| Pyramid | Kollidon® VA 64 (89%) | 170/40 | ||||
| Hemisphere | Eudragit® EPO (89%) | 180/40 | ||||
| Tube | HPC (89%) | 190/40 | ||||
| Sustained drug release 3D-printed tablets | Cylinder | Itraconazole (35%) | HPC | [20] | ||
| UL (65%) | 170 | |||||
| SSL (65%) | 170 | |||||
| SL (65%) | 170 | |||||
| L (65%) | 170 | |||||
| Cylinder | Tramadol hydrochloride (5%) | HPC | [26] | |||
| SL (50%) | Mannitol (40%) | 170 | ||||
| L (50%) | Magnesium stearate (5%) | 170 | ||||
| HPC | ||||||
| SL (60%) | Mannitol (10%), PEO (20%), Magnesium stearate (5%) | 170 | ||||
| L (60%) | 170 | |||||
| Cylinder | Niclosamide (10%) | HPMC HME 15 LV (Affinisol®) (40.73–90%) | PEG 6000 (2.14–4.50%) | 180/70 | [14] | |
| HP- β-CD (47.13%) | ||||||
| Cylinder | Ibuprofen (20%) | PVP Kollidon® 12 PF (75%) | PEG 1500 (5%) | 155/25 | [41] | |
| Ring | ||||||
| Floating device | ||||||
| Cylinder | Acetaminophen (35%) | Copovidone (56%) | Poloxamer® 407 (9%) | 140 | [38] | |
| Cylinder | Metoprolol tartrate (50%) | EVA (18% VA content) (50%) | 130 | [34] | ||
| Cylinder | Theophylline (40%) | Eudragit® RL (0–40%) | Triethyl citrate (TEC) (12%) | 80–110/40–45 | [24] | |
| Eudragit® RS (0–40%) | Glyceryl monostearate (8%) | |||||
| Square | Acetaminophen (10–30%) | Poly (3-hydroxybutyrate) (PHB) (70–90%) | 175–180 | [33] | ||
| Core–shell tablets | Cylinder | Acetaminophen (40%) | Kollidon® VA64 (core) (60%) | 140 (core) | [8] | |
| Eudragit® E PO (Shell) (100%) | 150 | |||||
| HPMCAS LG (Shell) (30%) | PEG 4500 (Shell) (10–20%) | 160 | ||||
| Eudragit® RS PO (Shell) (50–100%) | 110–140 | |||||
| Mini-tablets | Sphere | Ritonavir/Lopinavir (25%) | HPMCAS LG (51.75%) | PEG 4000 (22.5%) | 80/80 | [18] |
| Magnesium stearate (0.75%) | ||||||
| Cylinder | Budesonide (0.59%) | HPMC HME 15 LV (Affinisol®) (41.84–75.44%) | PEG 6000 (2.99–3.97%) | 180/60 | [15] | |
| H-β-CD (46.41%) | ||||||
| Adjuvant blend (citric acid, | ||||||
| tartaric acid, | ||||||
| sodium bicarbonate) (8.17–20%) | ||||||
| Cylinder | Nifedipine (25%) | HPC LF (40%) | PEG 4000 (15%) | 165/70 | [16] | |
| HPMCAS LG (19%) | Magnesium stearate (1%) | |||||
| Multi-component tablets | Cylinder Oval | Shell | Eudragit® RSPO (60–90%) | Stearic acid (10–20%) | 110–135 | [22] |
| Ethyl cellulose (15–20%) | ||||||
| Delay layer | HPC EF (90%) | PEG 400 (10%) | 116 | |||
| Delay layer | HPC EF (85%) | Glycerol (15%) | 85 | |||
| pH-responsive layer | HPMCAS LG/HG (75%) | Deionized water (12.5%) | 85 | |||
| Triacetin (12.5%) | ||||||
| Tofacinib (30%) | HPC EF (60%) | PEG 400 (10%) | 114 | |||
| Topiramate (28%) | HPC EF (52%) | PEG 400 (20%) | 70 | |||
| Metoprolol(40%) | HPC JF (40%) | PEG 400 (20%) | 105 | |||
| Levodopa/Carbidopa (32/8%) | HPC JF (35%) | PEG 400 (25%) | 100 | |||
| Clonidine (0.25%) | HPC JF (79.95%) | TEC (19.95%) | 115 | |||
| Metoprolol (25%) | Kollidon® VA64 (60%) | PEG 400 (15%) | 90 | |||
| Tofacinib (40%) | Kollidon® VA64 (35%) | PEG 1500 (25%) | 90 | |||
| Levodopa/carbidopa (48/12%) | PEG 8000 (36%) | Croscarmellose sodium (4%) | 70 | |||
| Topiramate (60%) | PEG 8000 (35%) | Croscarmellose sodium (5%) | 75 | |||
| Orodispersible films (ODFs) | Cylinder | Clobetasol (0.2%) | PEO N10 (71.45–81.45%) | HP-β-CD (3%) | 170/40 | [31] |
| Chitosan (15–25%) | ||||||
| HPMC HME 15 LV (Affinisol®)(0.35%) | ||||||
| Square | Olanzapine (5%) | PEO N-10 (70–75%) | Poloxamer® 407/poloxamer® 188 (5%) | 160/35 | [25] | |
| Kollidon® VA64 (20%) | ||||||
| Transdermal patches | Square | Ibuprofen (30%) | EVA 4030AC (70%) | 80/45 | [32] | |
| Diclofenac sodium (30%) | EVA 1821A (70%) | 180/45 | ||||
| Long-term implants | Ring | Paliperidone (5–10%) | PCL (90–95%) | 100–110/40 | [37] | |
| Disc | ||||||
| Cuboid | Raloxifene (10%) | PCL (45%) | 90/25 | [19] | ||
| Cylinder | PEO-N80 (45%) | |||||
| Tube |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aguilar-de-Leyva, Á.; Casas, M.; Ferrero, C.; Linares, V.; Caraballo, I. 3D Printing Direct Powder Extrusion in the Production of Drug Delivery Systems: State of the Art and Future Perspectives. Pharmaceutics 2024, 16, 437. https://doi.org/10.3390/pharmaceutics16040437
Aguilar-de-Leyva Á, Casas M, Ferrero C, Linares V, Caraballo I. 3D Printing Direct Powder Extrusion in the Production of Drug Delivery Systems: State of the Art and Future Perspectives. Pharmaceutics. 2024; 16(4):437. https://doi.org/10.3390/pharmaceutics16040437
Chicago/Turabian StyleAguilar-de-Leyva, Ángela, Marta Casas, Carmen Ferrero, Vicente Linares, and Isidoro Caraballo. 2024. "3D Printing Direct Powder Extrusion in the Production of Drug Delivery Systems: State of the Art and Future Perspectives" Pharmaceutics 16, no. 4: 437. https://doi.org/10.3390/pharmaceutics16040437
APA StyleAguilar-de-Leyva, Á., Casas, M., Ferrero, C., Linares, V., & Caraballo, I. (2024). 3D Printing Direct Powder Extrusion in the Production of Drug Delivery Systems: State of the Art and Future Perspectives. Pharmaceutics, 16(4), 437. https://doi.org/10.3390/pharmaceutics16040437