
Matrix-Mediated Delivery of Silver Nanoparticles for Prevention of Staphylococcus aureus and Pseudomonas aeruginosa Biofilm Formation in Chronic Rhinosinusitis


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Material
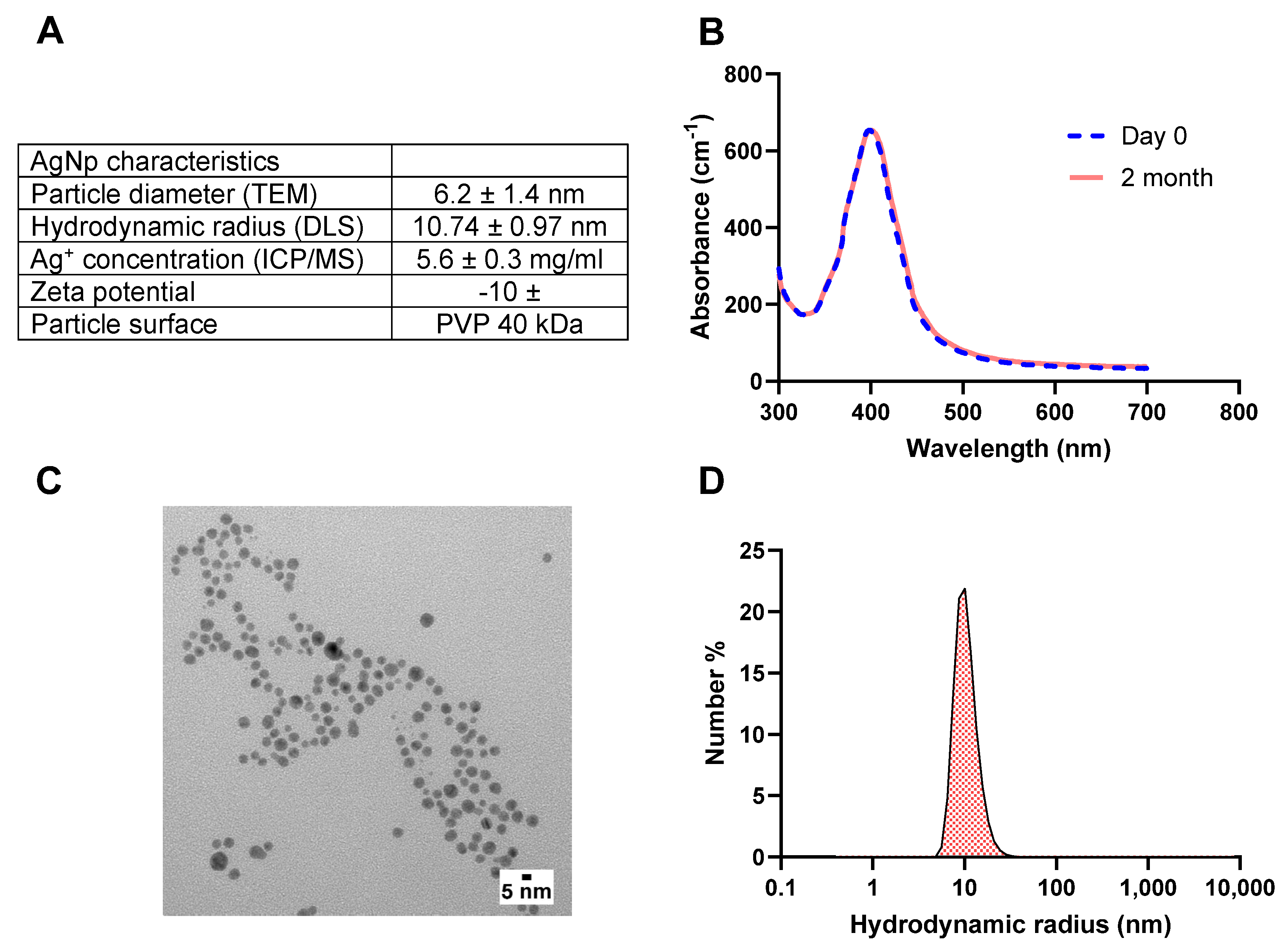
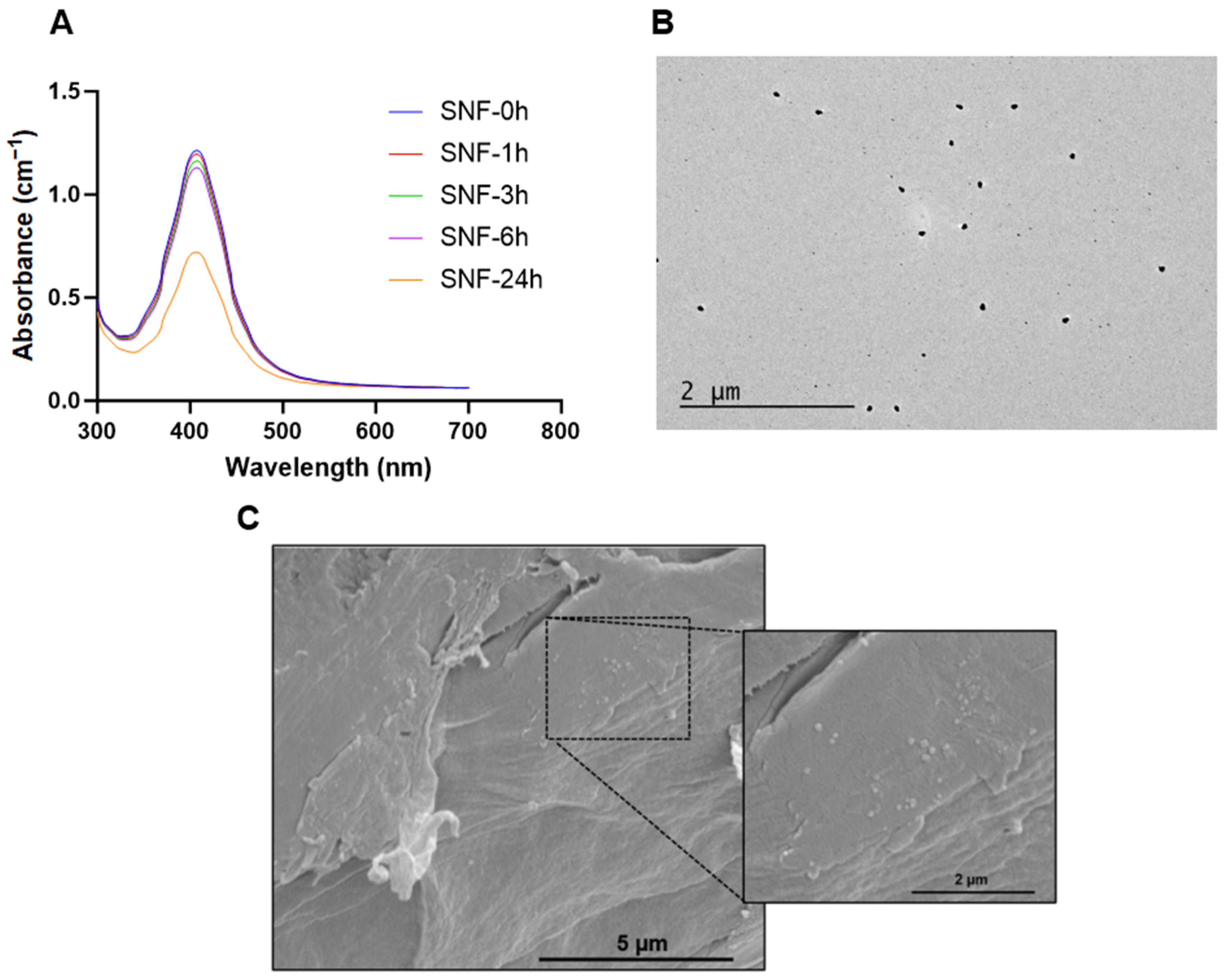
2.2. Characterization of AgNps
2.3. Minimum Inhibitory Concentration (MIC) and Minimum Bactericidal Concentration (MBC) Assays
2.4. HA Concentration Optimization
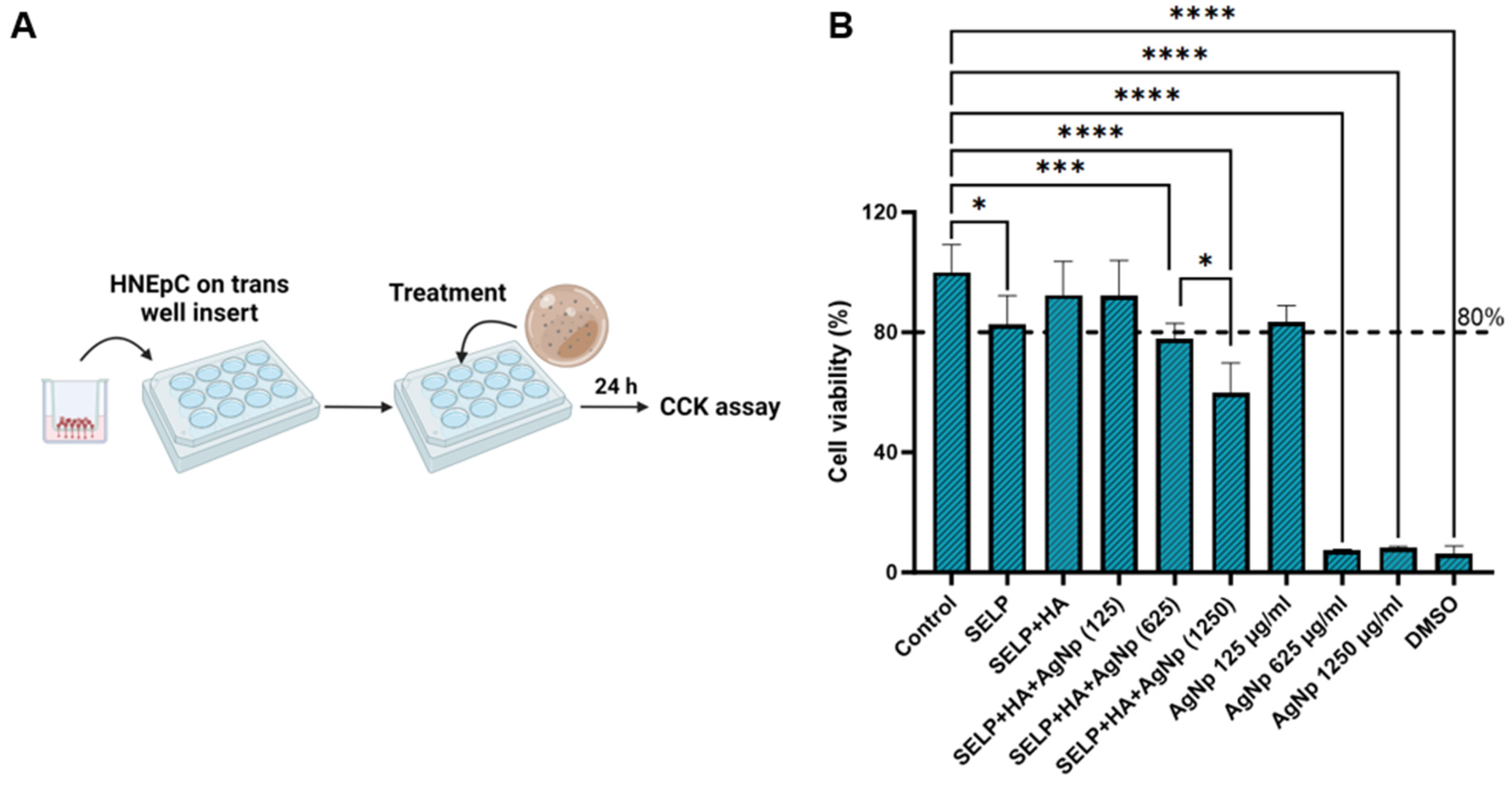
2.5. Cytocompatibility Assessment—Cell Counting Kit-8 (CCK) Assay
2.6. Antibacterial Effect Assessment—Viable Count Assay
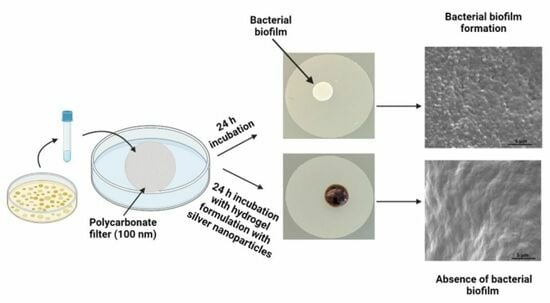
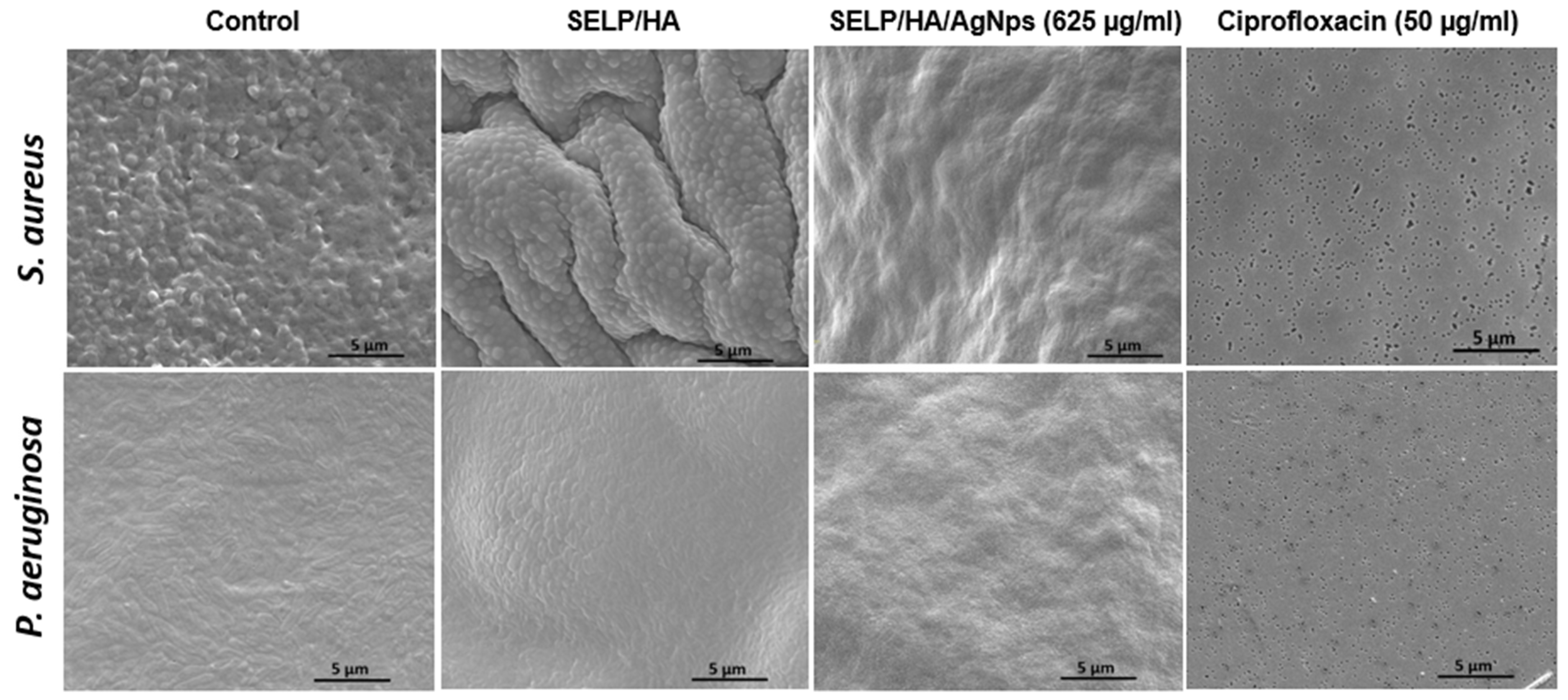
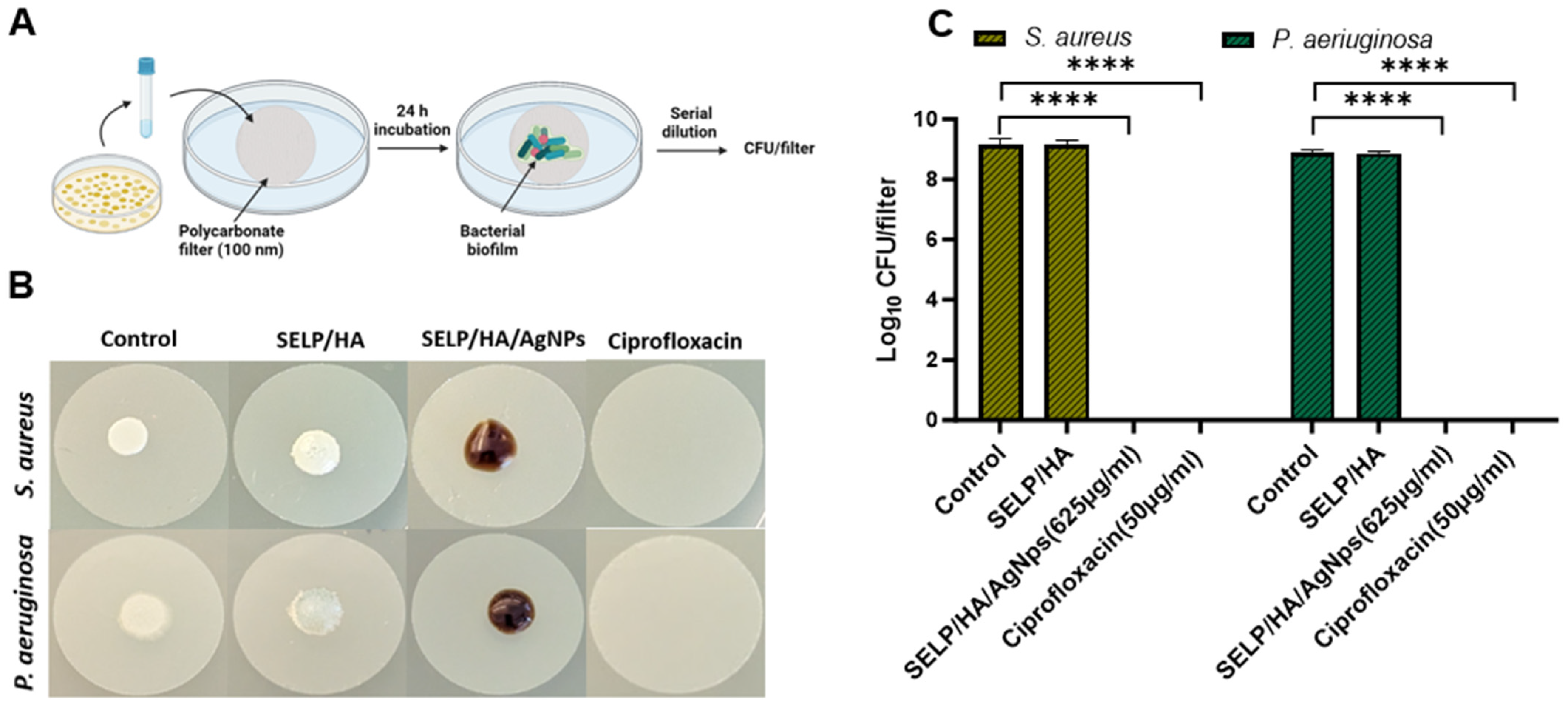
2.7. Biofilm Prevention Assay—Colony Biofilm Assay
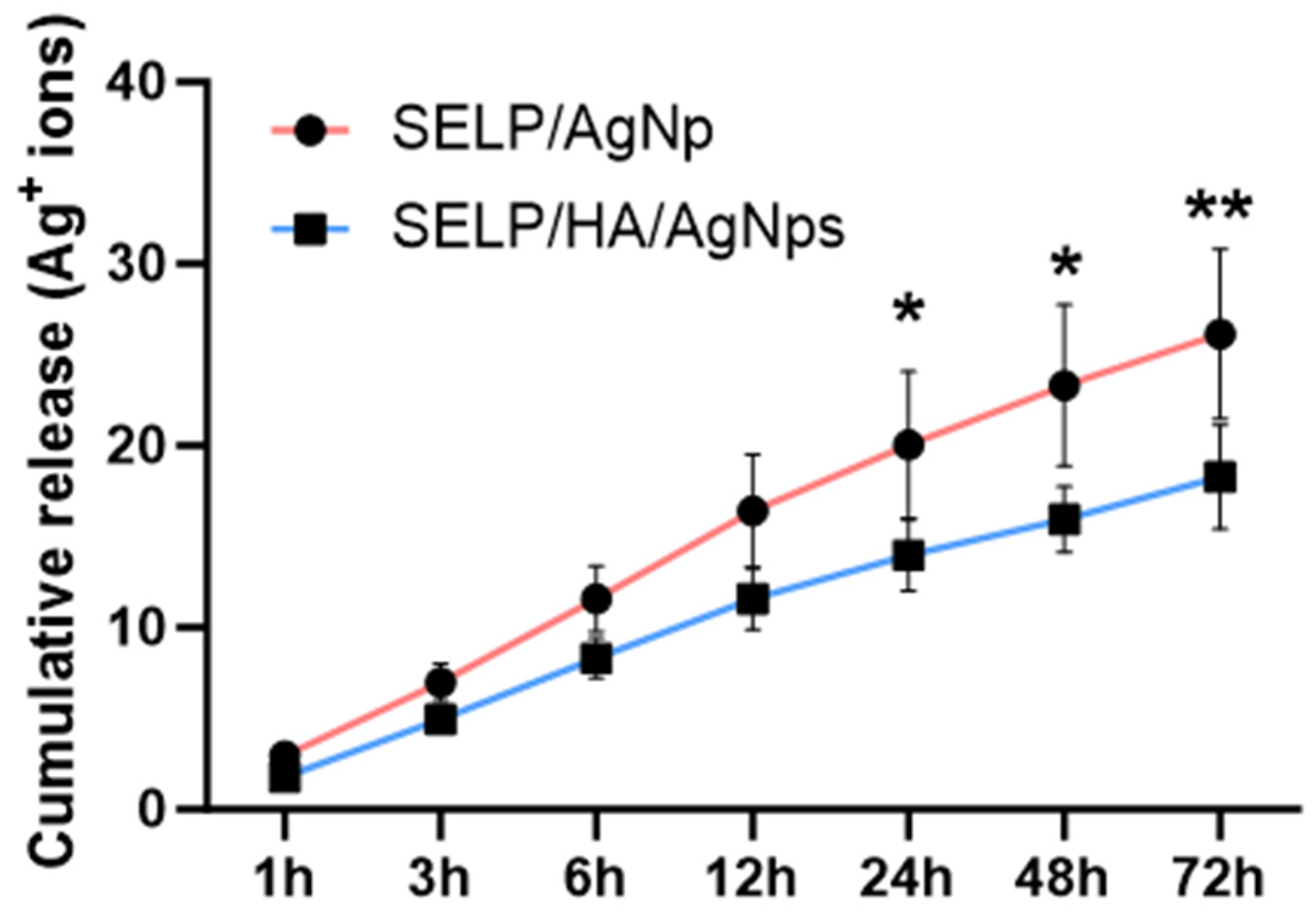
2.8. In Vitro Release Study
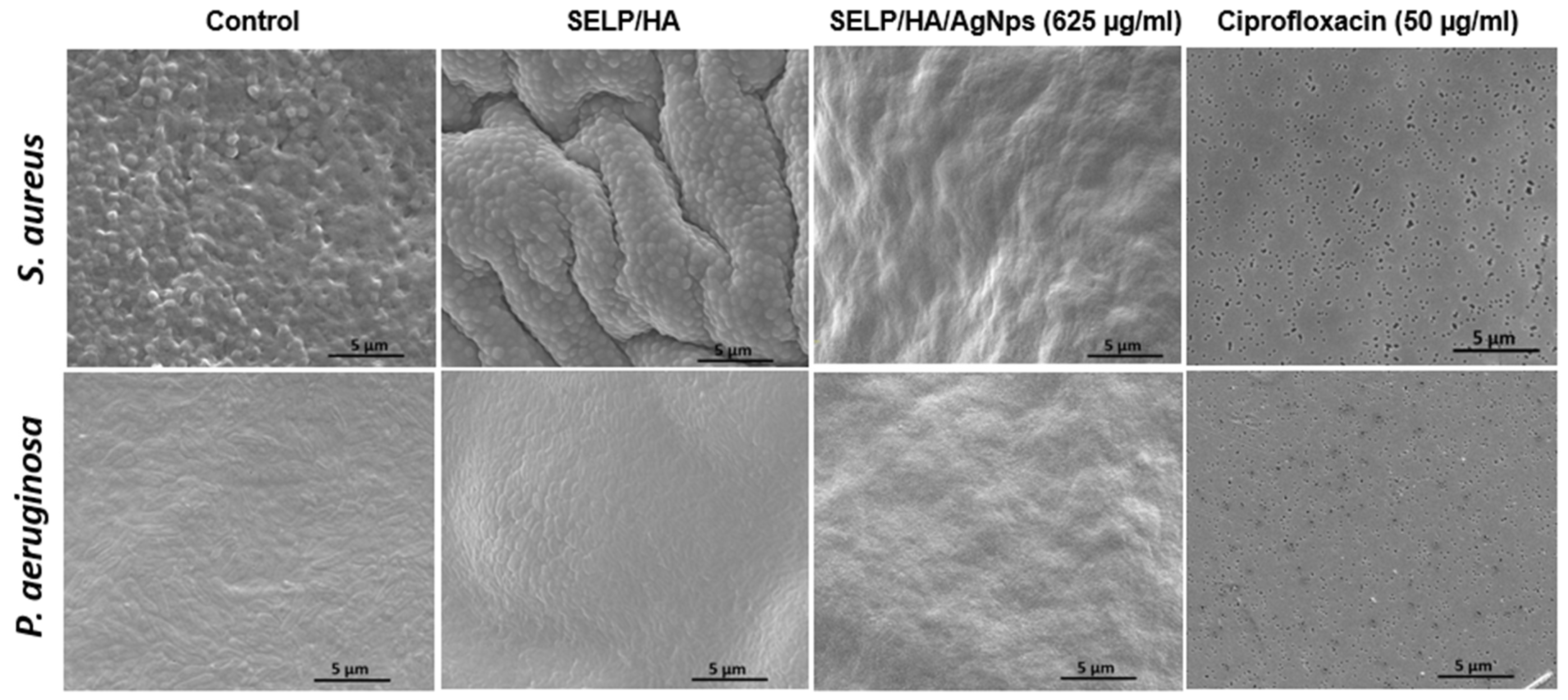
2.9. Scanning Electron Microscopy (SEM)
2.10. Rheological Properties
2.11. Statistical Analysis
3. Results
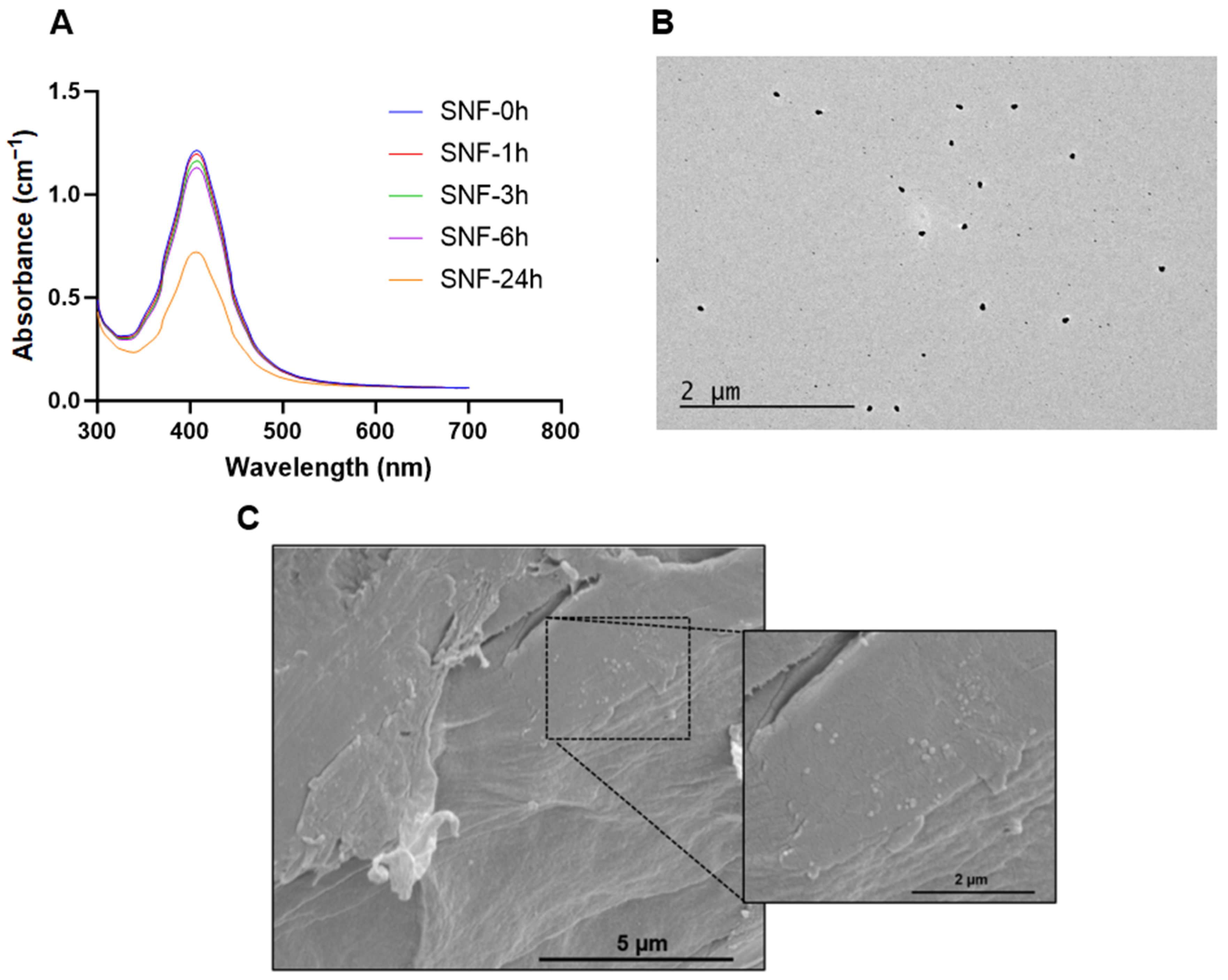
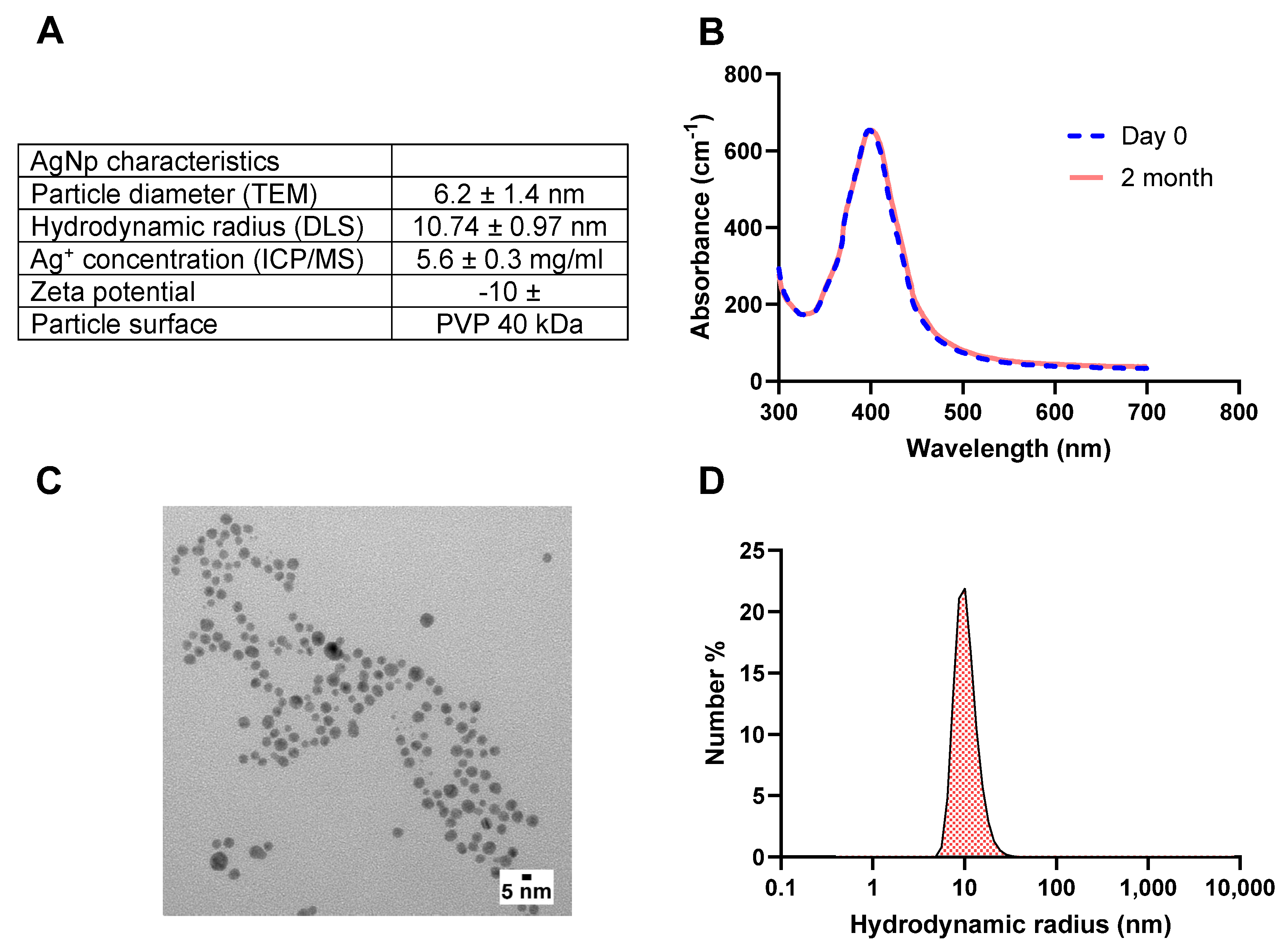
3.1. AgNps Characterization
3.2. Identification of MIC and MBC of AgNps against S. aureus and P. aeruginosa
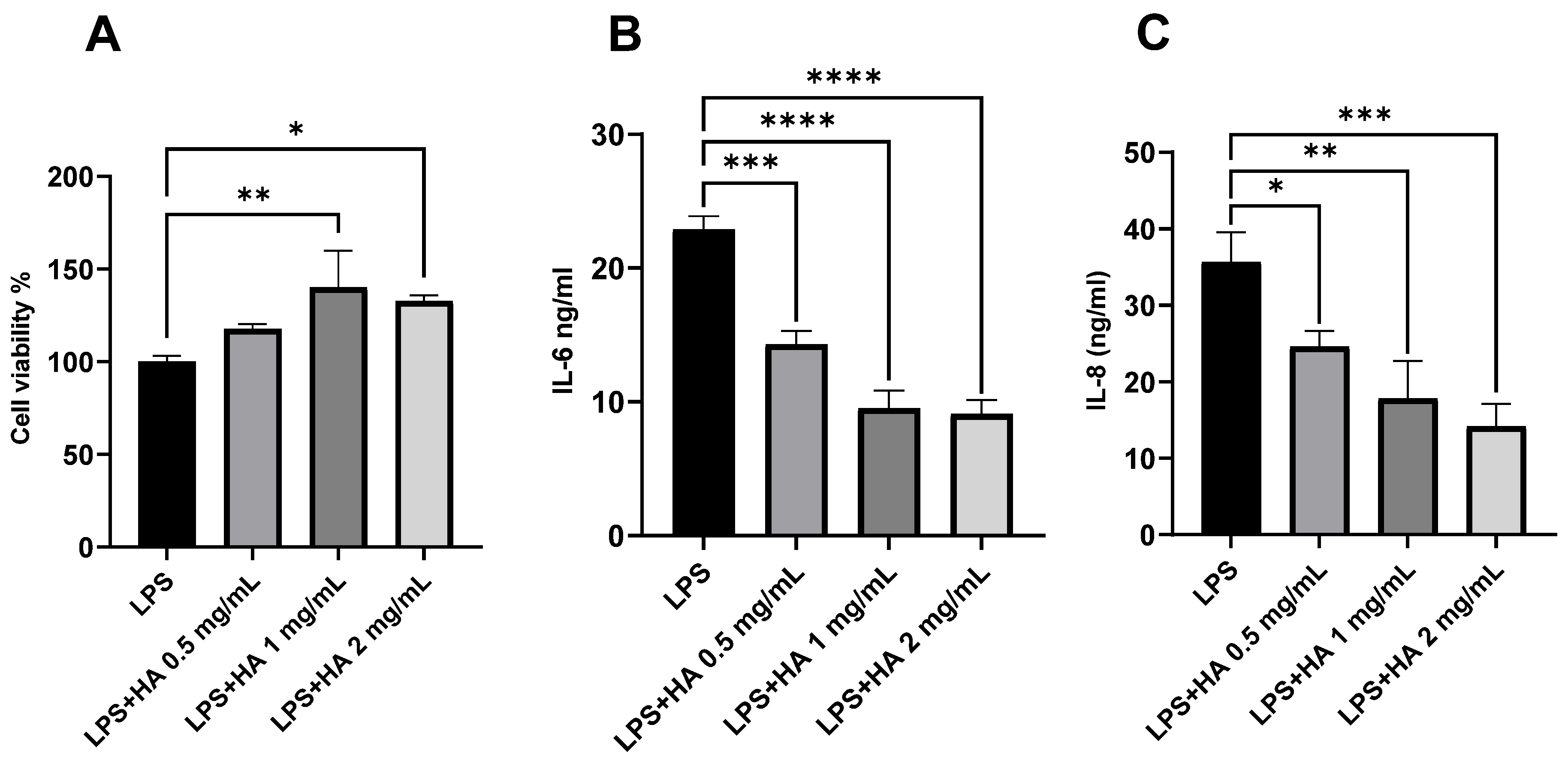
3.3. Optimization of HA Concentration for Anti-Inflammatory Effect
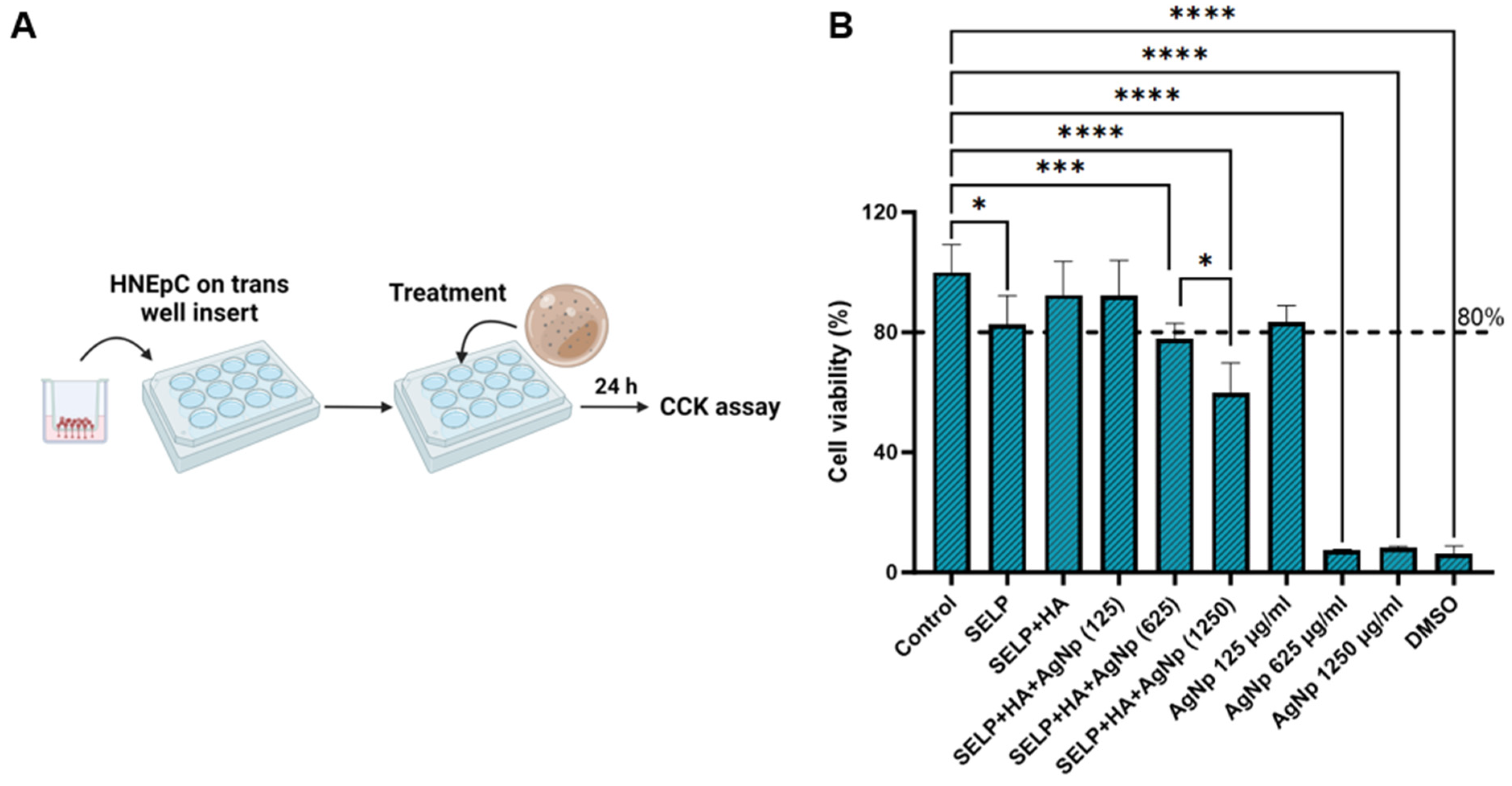
3.4. Cytocompatibility of Free AgNps and Hydrogel Formulations
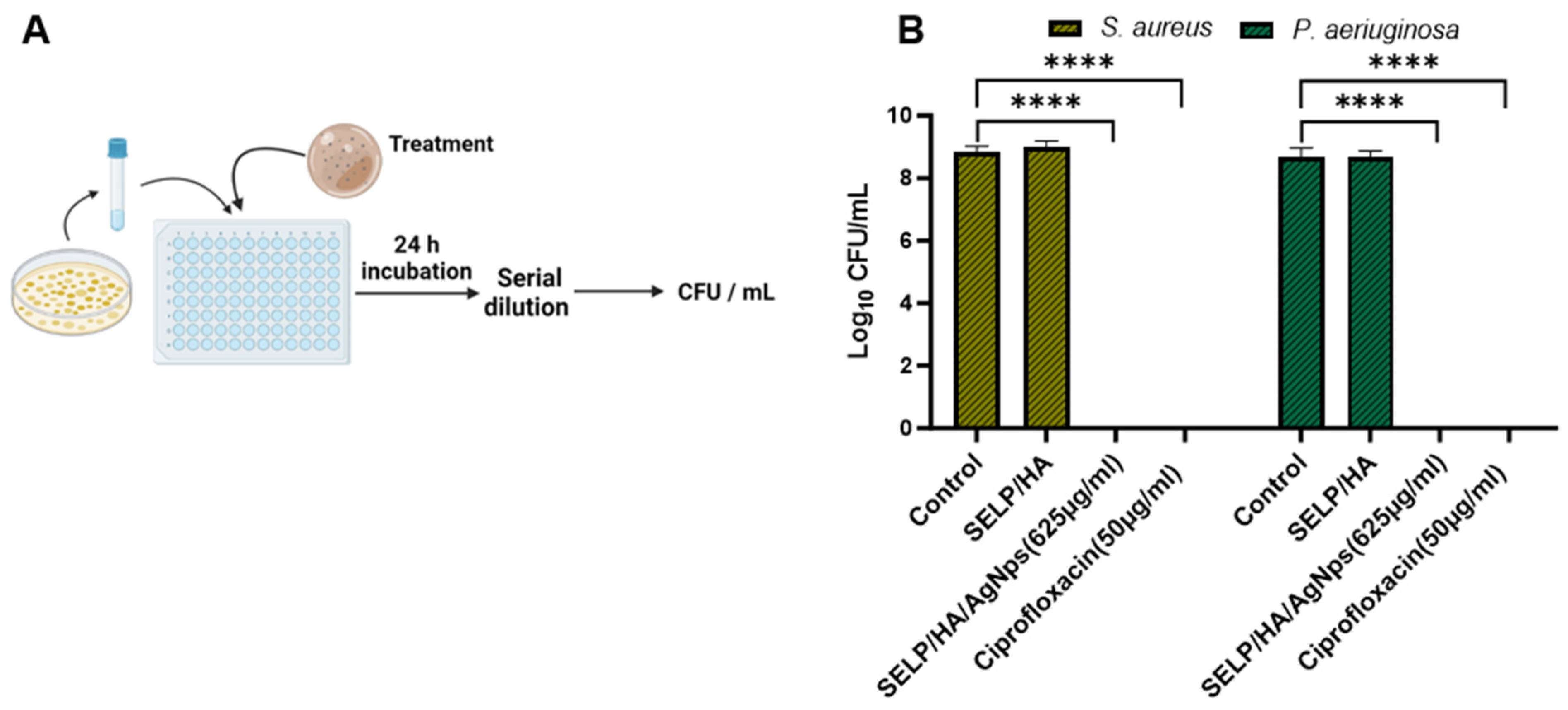
3.5. Antibacterial Effect of Hydrogel Formulations Measured by Viable Count Assay
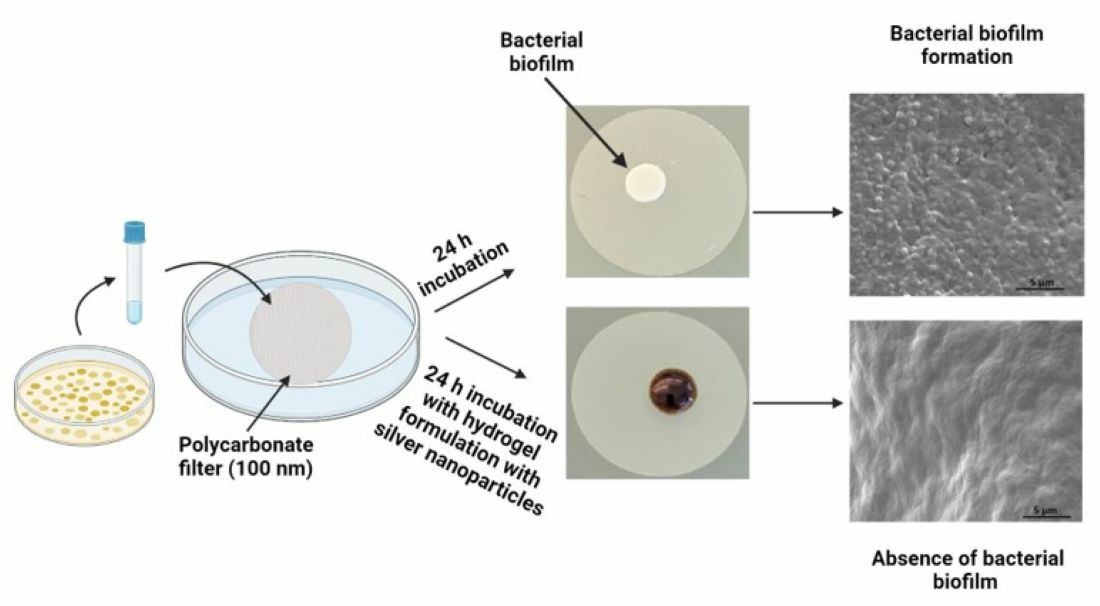
3.6. Biofilm Prevention Assessment with Matrix-Mediated Delivery of AgNps
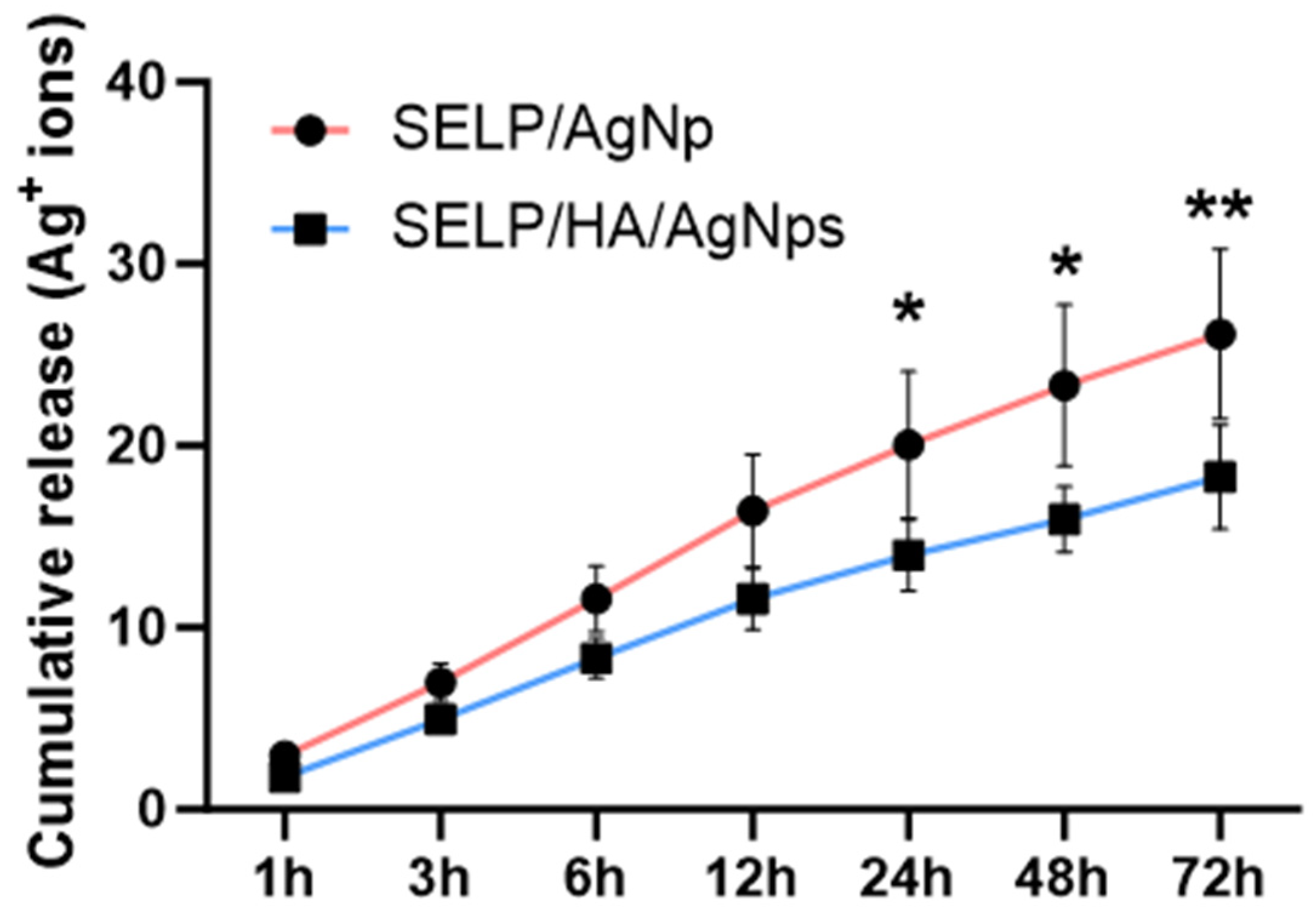
3.7. Assessment of AgNps Release from Hydrogels
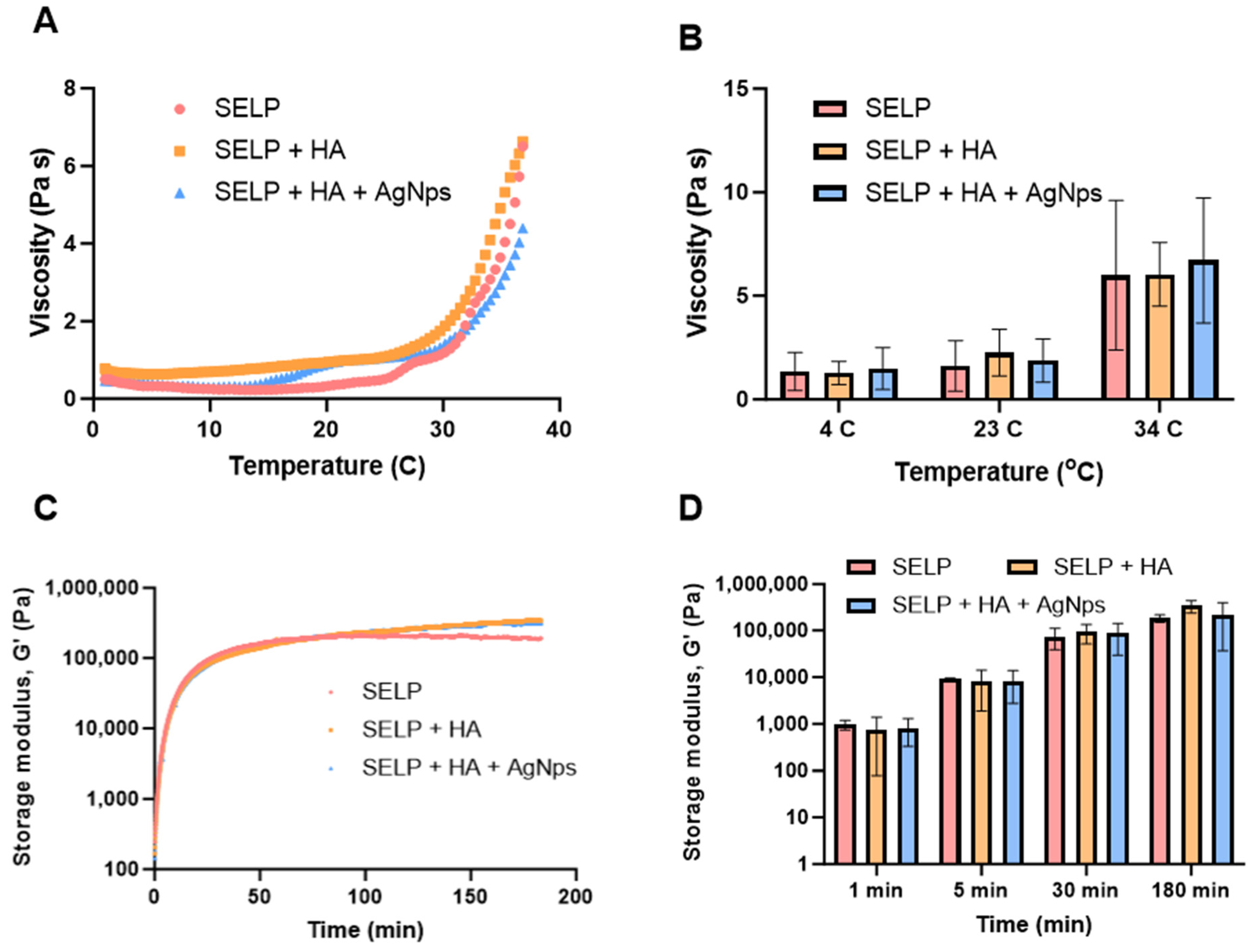
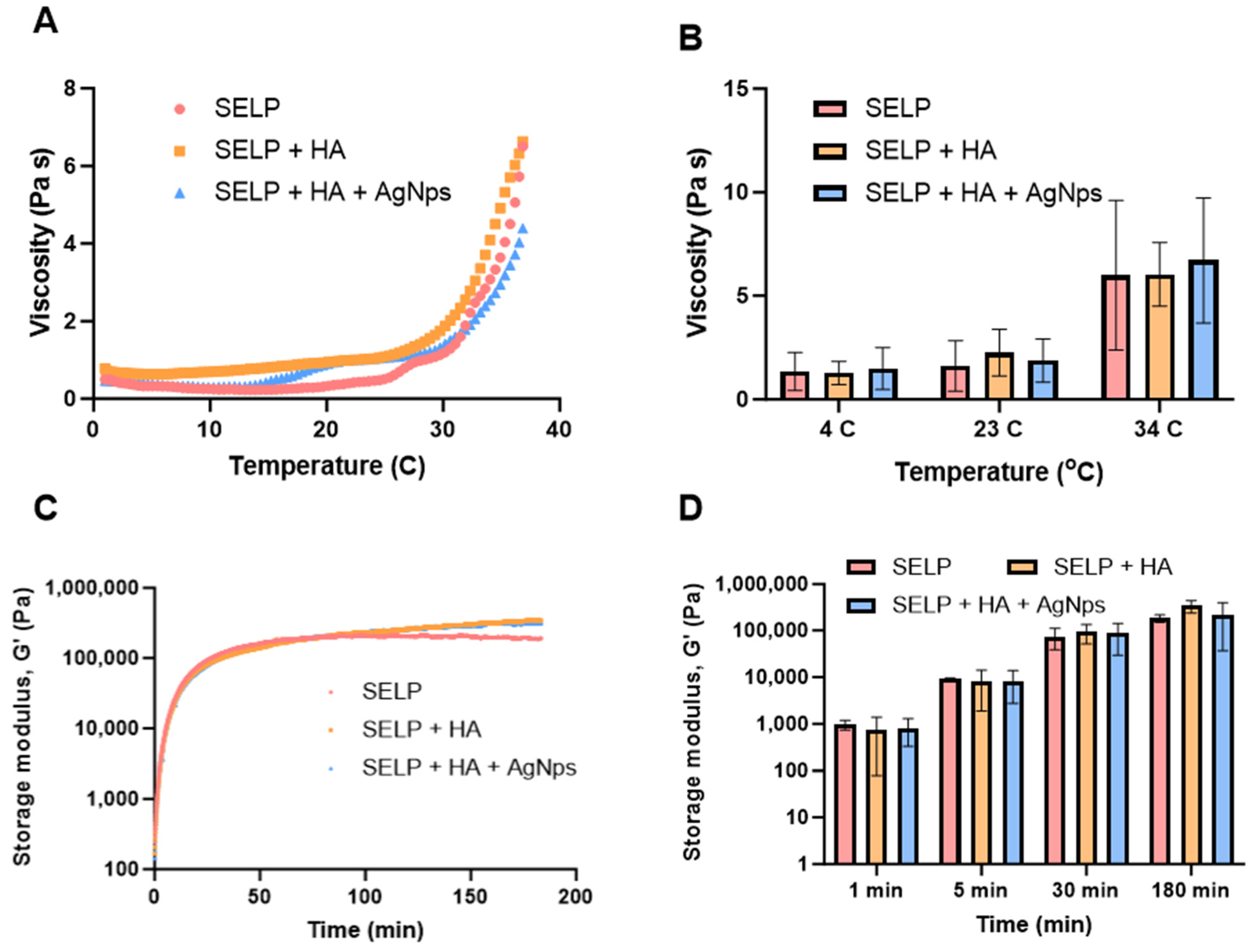
3.8. Rheological Characterization of the Final Antibacterial Dressing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Palmer, J.N.; Messina, J.C.; Biletch, R.; Grosel, K.; Mahmoud, R.A. A cross-sectional, population-based survey of U.S. adults with symptoms of chronic rhinosinusitis. Allergy Asthma Proc. 2019, 40, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, R.R.; Kingdom, T.T.; Smith, T.L.; Bleier, B.; DeConde, A.; Luong, A.U.; Poetker, D.M.; Soler, Z.; Welch, K.C.; Wise, S.K.; et al. International consensus statement on allergy and rhinology: Rhinosinusitis 2021. Int. Forum Allergy Rhinol. 2021, 11, 213–739. [Google Scholar] [CrossRef] [PubMed]
- Kaper, N.M.; Aarts, M.C.J.; Stokroos, R.J.; van der Heijden, G.J.M.G. Healthcare utilisation, follow-up of guidelines and practice variation on rhinosinusitis in adults: A healthcare reimbursement claims study in The Netherlands. Clin. Otolaryngol. 2020, 45, 159–166. [Google Scholar] [CrossRef]
- Brandsted, R.; Sindwani, R. Impact of depression on disease-specific symptoms and quality of life in patients with chronic rhinosinusitis. Am. J. Rhinol. 2007, 21, 50–54. [Google Scholar] [CrossRef]
- Alt, J.A.; Mace, J.C.; Smith, T.L.; Soler, Z.M. Endoscopic sinus surgery improves cognitive dysfunction in patients with chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2016, 6, 1264–1272. [Google Scholar] [CrossRef]
- Alt, J.A.; Smith, T.L.; Mace, J.C.; Soler, Z.M. Sleep quality and disease severity in patients with chronic rhinosinusitis. Laryngoscope 2013, 123, 2364–2370. [Google Scholar] [CrossRef]
- Laidlaw, T.M.; Mullol, J.; Woessner, K.M.; Amin, N.; Mannent, L.P. Chronic Rhinosinusitis with Nasal Polyps and Asthma. J. Allergy Clin. Immunol. Pract. 2021, 9, 1133–1141. [Google Scholar] [CrossRef]
- Bachert, C.; Han, J.K.; Desrosiers, M.; Hellings, P.W.; Amin, N.; Lee, S.E.; Mullol, J.; Greos, L.S.; Bosso, J.V.; Laidlaw, T.M.; et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): Results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet 2019, 394, 1638–1650. [Google Scholar] [CrossRef]
- Kohanski, M.A.; Toskala, E.; Kennedy, D.W. Evolution in the surgical management of chronic rhinosinusitis: Current indications and pitfalls. J. Allergy Clin. Immunol. 2018, 141, 1561–1569. [Google Scholar] [CrossRef]
- Lourijsen, E.S.; Reitsma, S.; Vleming, M.; Hannink, G.; Adriaensen, G.F.J.P.; Cornet, M.E.; Hoven, D.R.; Videler, W.J.M.; Bretschneider, J.H.; Reinartz, S.M.; et al. Endoscopic sinus surgery with medical therapy versus medical therapy for chronic rhinosinusitis with nasal polyps: A multicentre, randomised, controlled trial. Lancet Respir. Med. 2022, 10, 337–346. [Google Scholar] [CrossRef]
- Zhang, Z.; Adappa, N.D.; Chiu, A.G.; Doghramji, L.J.; Cohen, N.A.; Palmer, J.N. Biofilm-forming bacteria and quality of life improvement after sinus surgery. Int. Forum Allergy Rhinol. 2015, 5, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Maina, I.W.; Patel, N.N.; Cohen, N.A. Understanding the Role of Biofilms and Superantigens in Chronic Rhinosinusitis. Curr. Otorhinolaryngol. Rep. 2018, 6, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Fastenberg, J.H.; Hsueh, W.D.; Mustafa, A.; Akbar, N.A.; Abuzeid, W.M. Biofilms in chronic rhinosinusitis: Pathophysiology and therapeutic strategies. World J. Otorhinolaryngol. Head Neck Surg. 2016, 2, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Dlugaszewska, J.; Leszczynska, M.; Lenkowski, M.; Tatarska, A.; Pastusiak, T.; Szyfter, W. The pathophysiological role of bacterial biofilms in chronic sinusitis. Eur. Arch. Otorhinolaryngol. 2016, 273, 1989–1994. [Google Scholar] [CrossRef]
- Vestby, L.K.; Grønseth, T.; Simm, R.; Nesse, L.L. Bacterial Biofilm and its Role in the Pathogenesis of Disease. Antibiotics 2020, 9, 59. [Google Scholar] [CrossRef]
- Foreman, A.; Psaltis, A.J.; Tan, L.W.; Wormald, P.J. Characterization of bacterial and fungal biofilms in chronic rhinosinusitis. Am. J. Rhinol. Allergy 2009, 23, 556–561. [Google Scholar] [CrossRef]
- Bendouah, Z.; Barbeau, J.; Hamad, W.A.; Desrosiers, M. Biofilm formation by Staphylococcus aureus and Pseudomonas aeruginosa is associated with an unfavorable evolution after surgery for chronic sinusitis and nasal polyposis. Otolaryngol. Head Neck Surg. 2006, 134, 991–996. [Google Scholar] [CrossRef]
- Foreman, A.; Boase, S.; Psaltis, A.; Wormald, P.J. Role of bacterial and fungal biofilms in chronic rhinosinusitis. Curr. Allergy Asthma Rep. 2012, 12, 127–135. [Google Scholar] [CrossRef]
- Lux, C.A.; Wagner Mackenzie, B.; Johnston, J.; Zoing, M.; Biswas, K.; Taylor, M.W.; Douglas, R.G. Antibiotic Treatment for Chronic Rhinosinusitis: Prescription Patterns and Associations with Patient Outcome and the Sinus Microbiota. Front. Microbiol. 2020, 11, 595555. [Google Scholar] [CrossRef]
- Zernotti, M.E.; Angel Villegas, N.; Roques Revol, M.; Baena-Cagnani, C.E.; Arce Miranda, J.E.; Paredes, M.E.; Albesa, I.; Paraje, M.G. Evidence of bacterial biofilms in nasal polyposis. J. Investig. Allergol. Clin. Immunol. 2010, 20, 380–385. [Google Scholar]
- Singhal, D.; Psaltis, A.J.; Foreman, A.; Wormald, P.J. The impact of biofilms on outcomes after endoscopic sinus surgery. Am. J. Rhinol. Allergy 2010, 24, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Hai, P.V.; Lidstone, C.; Wallwork, B. The effect of endoscopic sinus surgery on bacterial biofilms in chronic rhinosinusitis. Otolaryngol. Head Neck Surg. 2010, 142, S27–S32. [Google Scholar] [CrossRef]
- Smith, S.S.; Kim, R.; Douglas, R. Is there a role for antibiotics in the treatment of chronic rhinosinusitis? J. Allergy Clin. Immunol. 2022, 149, 1504–1512. [Google Scholar] [CrossRef]
- Pynnonen, M.A.; Venkatraman, G.; Davis, G.E. Macrolide therapy for chronic rhinosinusitis: A meta-analysis. Otolaryngol. Head Neck Surg. 2013, 148, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Buchinsky, F.J.; Post, J.C. Eradicating chronic ear, nose, and throat infections: A systematically conducted literature review of advances in biofilm treatment. Otolaryngol. Head Neck Surg. 2011, 144, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Calus, L.; Van Bruaene, N.; Bosteels, C.; Dejonckheere, S.; Van Zele, T.; Holtappels, G.; Bachert, C.; Gevaert, P. Twelve-year follow-up study after endoscopic sinus surgery in patients with chronic rhinosinusitis with nasal polyposis. Clin. Transl. Allergy 2019, 9, 30. [Google Scholar] [CrossRef] [PubMed]
- Slavin, Y.N.; Asnis, J.; Häfeli, U.O.; Bach, H. Metal nanoparticles: Understanding the mechanisms behind antibacterial activity. J. Nanobiotechnology 2017, 15, 65. [Google Scholar] [CrossRef]
- Liao, C.; Li, Y.; Tjong, S.C. Bactericidal and Cytotoxic Properties of Silver Nanoparticles. Int. J. Mol. Sci. 2019, 20, 449. [Google Scholar] [CrossRef]
- de Lacerda Coriolano, D.; de Souza, J.B.; Bueno, E.V.; Medeiros, S.M.F.R.; Cavalcanti, I.D.L.; Cavalcanti, I.M.F. Antibacterial and antibiofilm potential of silver nanoparticles against antibiotic-sensitive and multidrug-resistant Pseudomonas aeruginosa strains. Braz. J. Microbiol. 2021, 52, 267–278. [Google Scholar] [CrossRef]
- Sim, W.; Barnard, R.T.; Blaskovich, M.A.T.; Ziora, Z.M. Antimicrobial Silver in Medicinal and Consumer Applications: A Patent Review of the Past Decade (2007–2017). Antibiotics 2018, 7, 93. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Hu, C.; Shao, L. The antimicrobial activity of nanoparticles: Present situation and prospects for the future. Int. J. Nanomed. 2017, 12, 1227–1249. [Google Scholar] [CrossRef] [PubMed]
- Rajiv, S.; Drilling, A.; Bassiouni, A.; James, C.; Vreugde, S.; Wormald, P.J. Topical colloidal silver as an anti-biofilm agent in a Staphylococcus aureus chronic rhinosinusitis sheep model. Int. Forum Allergy Rhinol. 2015, 5, 283–288. [Google Scholar] [CrossRef]
- Jia, M.; Chen, Z.; Guo, Y.; Chen, X.; Zhao, X. Efficacy of silk fibroin-nano silver against Staphylococcus aureus biofilms in a rabbit model of sinusitis. Int. J. Nanomed. 2017, 12, 2933–2939. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.R.; Krishnan, R.; Rotenberg, B.W.; Sowerby, L.J. The effectiveness of topical colloidal silver in recalcitrant chronic rhinosinusitis: A randomized crossover control trial. J. Otolaryngol. Head Neck Surg. 2017, 46, 64. [Google Scholar] [CrossRef] [PubMed]
- Ooi, M.L.; Richter, K.; Bennett, C.; Macias-Valle, L.; Vreugde, S.; Psaltis, A.J.; Wormald, P.J. Topical Colloidal Silver for the Treatment of Recalcitrant Chronic Rhinosinusitis. Front. Microbiol. 2018, 9, 720. [Google Scholar] [CrossRef] [PubMed]
- Tian, D.M.; Wan, H.H.; Chen, J.R.; Ye, Y.B.; He, Y.; Liu, Y.; Tang, L.Y.; He, Z.Y.; Liu, K.Z.; Gao, C.J.; et al. In-situ formed elastin-based hydrogels enhance wound healing via promoting innate immune cells recruitment and angiogenesis. Mater. Today Bio 2022, 15, 100300. [Google Scholar] [CrossRef]
- Dimatteo, R.; Darling, N.J.; Segura, T. In situ forming injectable hydrogels for drug delivery and wound repair. Adv. Drug Deliv. Rev. 2018, 127, 167–184. [Google Scholar] [CrossRef]
- Schilling, A.L.; Cannon, E.; Lee, S.E.; Wang, E.W.; Little, S.R. Advances in controlled drug delivery to the sinonasal mucosa. Biomaterials 2022, 282, 121430. [Google Scholar] [CrossRef]
- Schilling, A.L.; Kulahci, Y.; Moore, J.; Wang, E.W.; Lee, S.E.; Little, S.R. A thermoresponsive hydrogel system for long-acting corticosteroid delivery into the paranasal sinuses. J. Control Release 2021, 330, 889–897. [Google Scholar] [CrossRef]
- Dandu, R.; Von Cresce, A.; Briber, R.; Dowell, P.; Cappello, J.; Hamidreza, G. Silk–elastinlike protein polymer hydrogels: Influence of monomer sequence on physicochemical properties. Polymer 2009, 50, 366–374. [Google Scholar] [CrossRef]
- Cappello, J.; Crissman, J.; Dorman, M.; Mikolajczak, M.; Textor, G.; Marquet, M.; Ferrari, F. Genetic engineering of structural protein polymers. Biotechnol. Prog. 1990, 6, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.M.; Jia, W.; Isaacson, K.J.; Schults, A.; Cappello, J.; Prestwich, G.D.; Oottamasathien, S.; Ghandehari, H. Silk-elastinlike protein polymers enhance the efficacy of a therapeutic glycosaminoglycan for prophylactic treatment of radiation-induced proctitis. J. Control Release 2017, 263, 46–56. [Google Scholar] [CrossRef]
- Jensen, M.M.; Jia, W.; Schults, A.J.; Isaacson, K.J.; Steinhauff, D.; Green, B.; Zachary, B.; Cappello, J.; Ghandehari, H.; Oottamasathien, S. Temperature-responsive silk-elastinlike protein polymer enhancement of intravesical drug delivery of a therapeutic glycosaminoglycan for treatment of interstitial cystitis/painful bladder syndrome. Biomaterials 2019, 217, 119293. [Google Scholar] [CrossRef] [PubMed]
- Steinhauff, D.; Jensen, M.; Talbot, M.; Jia, W.; Isaacson, K.; Jedrzkiewicz, J.; Cappello, J.; Oottamasathien, S.; Ghandehari, H. Silk-elastinlike copolymers enhance bioaccumulation of semisynthetic glycosaminoglycan ethers for prevention of radiation induced proctitis. J. Control Release 2021, 332, 503–515. [Google Scholar] [CrossRef] [PubMed]
- Poursaid, A.; Jensen, M.M.; Nourbakhsh, I.; Weisenberger, M.; Hellgeth, J.W.; Sampath, S.; Cappello, J.; Ghandehari, H. Silk-Elastinlike Protein Polymer Liquid Chemoembolic for Localized Release of Doxorubicin and Sorafenib. Mol. Pharm. 2016, 13, 2736–2748. [Google Scholar] [CrossRef] [PubMed]
- Griswold, E.; Cappello, J.; Ghandehari, H. Silk-elastinlike protein-based hydrogels for drug delivery and embolization. Adv. Drug Deliv. Rev. 2022, 191, 114579. [Google Scholar] [CrossRef]
- Poursaid, A.; Price, R.; Tiede, A.; Olson, E.; Huo, E.; McGill, L.; Ghandehari, H.; Cappello, J. In situ gelling silk-elastinlike protein polymer for transarterial chemoembolization. Biomaterials 2015, 57, 142–152. [Google Scholar] [CrossRef]
- Fong, E.; Garcia, M.; Woods, C.M.; Ooi, E. Hyaluronic acid for post sinus surgery care: Systematic review and meta-analysis. J. Laryngol. Otol. 2017, 131, S2–S11. [Google Scholar] [CrossRef]
- Cassandro, E.; Chiarella, G.; Cavaliere, M.; Sequino, G.; Cassandro, C.; Prasad, S.C.; Scarpa, A.; Iemma, M. Hyaluronan in the Treatment of Chronic Rhinosinusitis with Nasal Polyposis. Indian J. Otolaryngol. Head Neck Surg. 2015, 67, 299–307. [Google Scholar] [CrossRef]
- Price, R.; Poursaid, A.; Cappello, J.; Ghandehari, H. Effect of shear on physicochemical properties of matrix metalloproteinase responsive silk-elastinlike hydrogels. J. Control Release 2014, 195, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Wiegand, I.; Hilpert, K.; Hancock, R.E. Agar and broth dilution methods to determine the minimal inhibitory concentration (MIC) of antimicrobial substances. Nat. Protoc. 2008, 3, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Daly, S.M.; Sturge, C.R.; Greenberg, D.E. Inhibition of Bacterial Growth by Peptide-Conjugated Morpholino Oligomers. Methods Mol. Biol. 2017, 1565, 115–122. [Google Scholar] [CrossRef]
- Merritt, J.H.; Kadouri, D.E.; O’Toole, G.A. Growing and analyzing static biofilms. Curr. Protoc. Microbiol. 2005, 1, Unit 1B.1. [Google Scholar] [CrossRef]
- Yao, Y.; Wang, Z.C.; Liu, J.X.; Ma, J.; Chen, C.L.; Deng, Y.K.; Liao, B.; Wang, N.; Wang, H.; Ning, Q.; et al. Increased expression of TIPE2 in alternatively activated macrophages is associated with eosinophilic inflammation and disease severity in chronic rhinosinusitis with nasal polyps. Int. Forum Allergy Rhinol. 2017, 7, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Holtappels, G. Pathophysiology of chronic rhinosinusitis, pharmaceutical therapy options. GMS Curr. Top. Otorhinolaryngol. Head Neck Surg. 2015, 14, Doc09. [Google Scholar] [CrossRef]
- ISO 10993-5:2009; Biological Evaluation of Medical Devices—Part 5: Test for Invitro Cytotoxicity. International Organization for Standardization: Geneva, Switzerland, 2009. Available online: https://www.iso.org/standard/36406.html (accessed on 8 August 2023).
- Relucenti, M.; Familiari, G.; Donfrancesco, O.; Taurino, M.; Li, X.; Chen, R.; Artini, M.; Papa, R.; Selan, L. Microscopy Methods for Biofilm Imaging: Focus on SEM and VP-SEM Pros and Cons. Biology 2021, 10, 51. [Google Scholar] [CrossRef]
- Woodworth, B.A.; Chandra, R.K.; LeBenger, J.D.; Ilie, B.; Schlosser, R.J. A gelatin-thrombin matrix for hemostasis after endoscopic sinus surgery. Am. J. Otolaryngol. 2009, 30, 49–53. [Google Scholar] [CrossRef]
- Surgiflo® Hemostatic Matrix Essential Product Information. Ethicon, Inc. Available online: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.jnjmedtech.com/system/files/pdf/SURGIFLO-and-Go-Sales-Brochure-135173-200320.pdf (accessed on 8 August 2023).
- Siu, J.; Klingler, L.; Wang, Y.; Hung, C.T.; Jeong, S.H.; Smith, S.; Tingle, M.D.; Wagner Mackenzie, B.; Biswas, K.; Douglas, R.G. Oral antibiotics used in the treatment of chronic rhinosinusitis have limited penetration into the sinonasal mucosa: A randomized trial. Xenobiotica 2020, 50, 1443–1450. [Google Scholar] [CrossRef]
- Hale, S.J.M.; Wagner Mackenzie, B.; Lux, C.A.; Biswas, K.; Kim, R.; Douglas, R.G. Topical Antibiofilm Agents With Potential Utility in the Treatment of Chronic Rhinosinusitis: A Narrative Review. Front. Pharmacol. 2022, 13, 840323. [Google Scholar] [CrossRef]
- Jensen, M.M.; Hatlevik, Ø.; Steinhauff, D.D.; Griswold, E.D.; Wei, X.; Isaacson, K.J.; Barber, Z.B.; Huo, E.; Taussky, P.; Jedrzkiewicz, J.; et al. Protein-based polymer liquid embolics for cerebral aneurysms. Acta Biomater. 2022, 151, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Fröhlich, E.E.; Fröhlich, E. Cytotoxicity of Nanoparticles Contained in Food on Intestinal Cells and the Gut Microbiota. Int. J. Mol. Sci. 2016, 17, 509. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Luo, Y. Bacterial Quorum-Sensing Systems and Their Role in Intestinal Bacteria-Host Crosstalk. Front. Microbiol. 2021, 12, 611413. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.R.; Singh, B.N.; Singh, A.; Khan, W.; Naqvi, A.H.; Singh, H.B. Mycofabricated biosilver nanoparticles interrupt Pseudomonas aeruginosa quorum sensing systems. Sci. Rep. 2015, 5, 13719. [Google Scholar] [CrossRef]
- Haidari, H.; Kopecki, Z.; Bright, R.; Cowin, A.J.; Garg, S.; Goswami, N.; Vasilev, K. Ultrasmall AgNP-Impregnated Biocompatible Hydrogel with Highly Effective Biofilm Elimination Properties. ACS Appl. Mater. Interfaces 2020, 12, 41011–41025. [Google Scholar] [CrossRef]
- Liu, T.; Aman, A.; Ainiwaer, M.; Ding, L.; Zhang, F.; Hu, Q.; Song, Y.; Ni, Y.; Tang, X. Evaluation of the anti-biofilm effect of poloxamer-based thermoreversible gel of silver nanoparticles as a potential medication for root canal therapy. Sci. Rep. 2021, 11, 12577. [Google Scholar] [CrossRef]
- Loo, C.Y.; Young, P.M.; Lee, W.H.; Cavaliere, R.; Whitchurch, C.B.; Rohanizadeh, R. Non-cytotoxic silver nanoparticle-polyvinyl alcohol hydrogels with anti-biofilm activity: Designed as coatings for endotracheal tube materials. Biofouling 2014, 30, 773–788. [Google Scholar] [CrossRef]
- Gurina, D.; Surov, O.; Voronova, M.; Zakharov, A.; Kiselev, M. Water Effects on Molecular Adsorption of Poly(N-vinyl-2-pyrrolidone) on Cellulose Nanocrystals Surfaces: Molecular Dynamics Simulations. Materials 2019, 12, 2155. [Google Scholar] [CrossRef]
- Maslova, E.; Eisaiankhongi, L.; Sjöberg, F.; McCarthy, R.R. Burns and biofilms: Priority pathogens and in vivo models. NPJ Biofilms Microbiomes 2021, 7, 73. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MIC (µg/mL) | MBC (µg/mL) | |
|---|---|---|
| S. aureus (gram +ve) | 7.8 | 125 |
| P. aeruginosa (gram −ve) | 7.8 | 7.8 |
| S. aureus | P. aeruginosa | |||
|---|---|---|---|---|
| MBC (Streak Plate Method) | MBC (CFU/mL) | MBC (Streak Plate Method) | MBC (CFU/mL) | |
| Presence of Growth | Growth Reduction (%) | Presence of Growth | Growth Reduction (%) | |
| Control | + | <99.9 | + | <99.9 |
| Polymyxin B (50 µg/mL) | + | <99.9 | - | >99.9 |
| Ampicillin (50 µg/mL) | - | >99.9 | + | <99.9 |
| AgNps (250 µg/mL) | - | >99.9 | - | >99.9 |
| AgNps (125 µg/mL) | - | >99.9 | - | >99.9 |
| AgNps (62.5 µg/mL) | + | <99.9 | - | >99.9 |
| AgNps (31.3 µg/mL) | + | <99.9 | - | >99.9 |
| AgNps (15.6 µg/mL) | + | <99.9 | - | >99.9 |
| AgNps (7.8 µg/mL) | + | <99.9 | - | >99.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yathavan, B.; Chhibber, T.; Steinhauff, D.; Pulsipher, A.; Alt, J.A.; Ghandehari, H.; Jafari, P. Matrix-Mediated Delivery of Silver Nanoparticles for Prevention of Staphylococcus aureus and Pseudomonas aeruginosa Biofilm Formation in Chronic Rhinosinusitis. Pharmaceutics 2023, 15, 2426. https://doi.org/10.3390/pharmaceutics15102426
Yathavan B, Chhibber T, Steinhauff D, Pulsipher A, Alt JA, Ghandehari H, Jafari P. Matrix-Mediated Delivery of Silver Nanoparticles for Prevention of Staphylococcus aureus and Pseudomonas aeruginosa Biofilm Formation in Chronic Rhinosinusitis. Pharmaceutics. 2023; 15(10):2426. https://doi.org/10.3390/pharmaceutics15102426
Chicago/Turabian StyleYathavan, Bhuvanesh, Tanya Chhibber, Douglas Steinhauff, Abigail Pulsipher, Jeremiah A. Alt, Hamidreza Ghandehari, and Paris Jafari. 2023. "Matrix-Mediated Delivery of Silver Nanoparticles for Prevention of Staphylococcus aureus and Pseudomonas aeruginosa Biofilm Formation in Chronic Rhinosinusitis" Pharmaceutics 15, no. 10: 2426. https://doi.org/10.3390/pharmaceutics15102426
APA StyleYathavan, B., Chhibber, T., Steinhauff, D., Pulsipher, A., Alt, J. A., Ghandehari, H., & Jafari, P. (2023). Matrix-Mediated Delivery of Silver Nanoparticles for Prevention of Staphylococcus aureus and Pseudomonas aeruginosa Biofilm Formation in Chronic Rhinosinusitis. Pharmaceutics, 15(10), 2426. https://doi.org/10.3390/pharmaceutics15102426