

The Impact of Inflammation on the In Vivo Activity of the Renal Transporters OAT1/3 in Pregnant Women Diagnosed with Acute Pyelonephritis

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
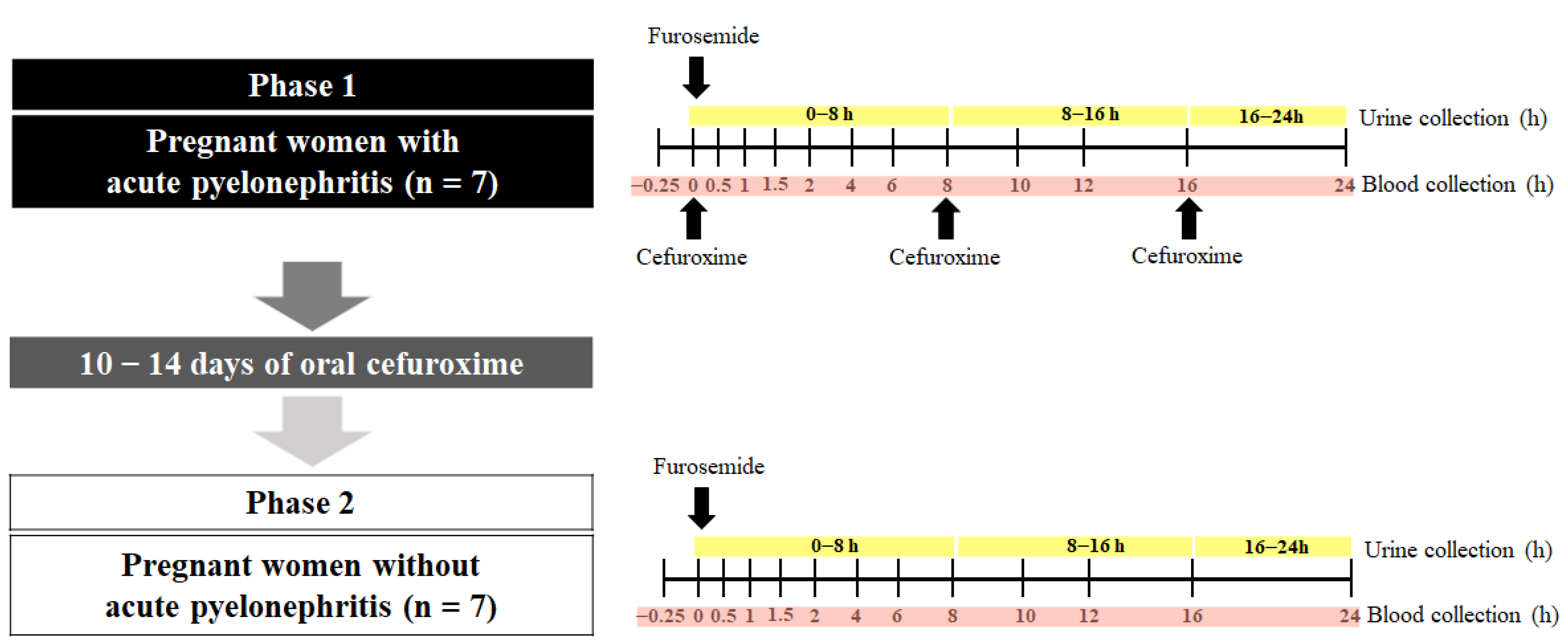
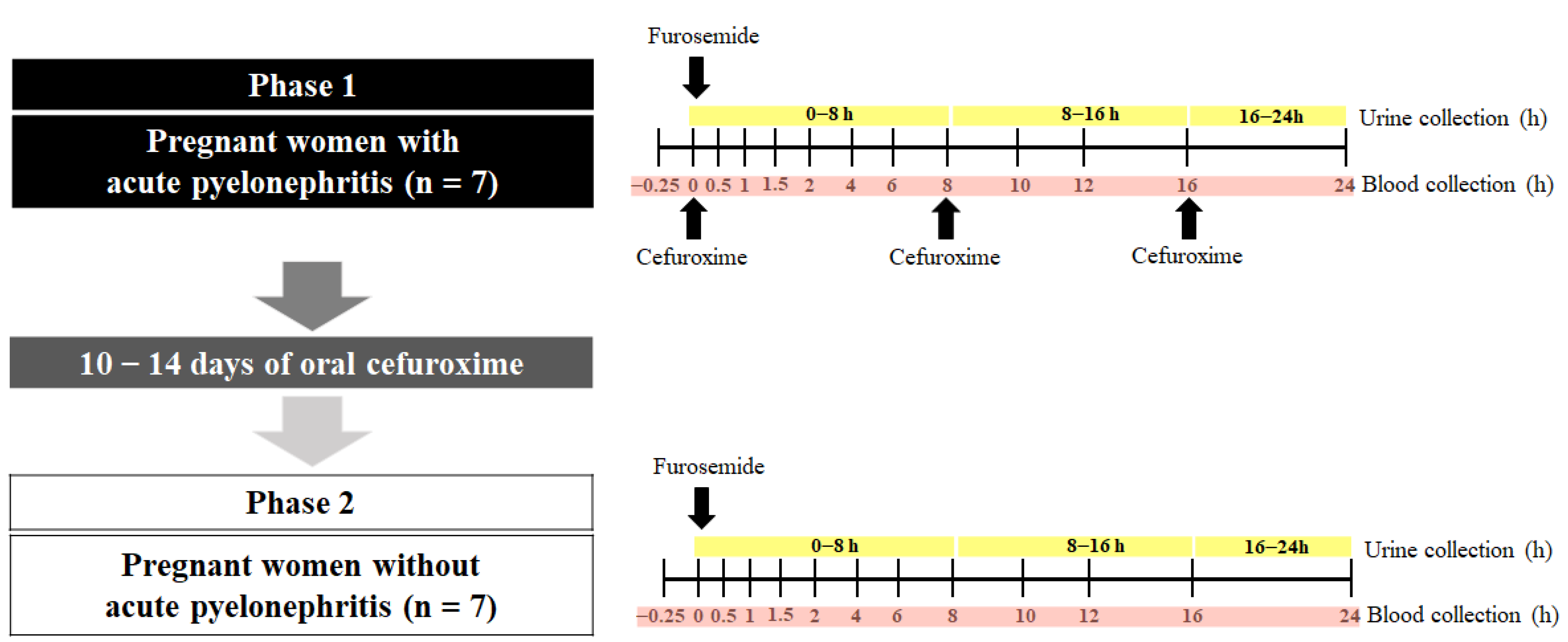
2.1. Clinical Study
2.2. Power Analysis
2.3. Analyses of Furosemide and Furosemide-Glucuronidein Plasma, Urine, and Plasma Ultrafiltrate
2.4. Quantification of Plasma Cytokine Concentrations
2.5. Pharmacokinetic Analyses
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morgan, E.T. Impact of Infectious and Inflammatory Disease on Cytochrome P450-Mediated Drug Metabolism and Pharmacokinetics. Clin. Pharmacol. Ther. 2009, 85, 434–438. [Google Scholar] [CrossRef]
- Fardel, O.; Le Vée, M. Regulation of Human Hepatic Drug Transporter Expression by Pro-Inflammatory Cytokines. Expert. Opin. Drug Metab. Toxicol. 2009, 5, 1469–1481. [Google Scholar] [CrossRef]
- Klöditz, K.; Tewolde, E.; Nordling, Å.; Ingelman-Sundberg, M. Mechanistic, Functional and Clinical Aspects of pro-Inflammatory Cytokine Mediated Regulation of ADME Gene Expression in 3D Human Liver Spheroids. Clin. Pharmacol. Ther. 2023, 114, 673–685. [Google Scholar] [CrossRef]
- Lanchote, V.L.; Almeida, R.; Barral, A.; Barral-Netto, M.; Marques, M.P.; Moraes, N.V.; Da Silva, A.M.; Souza, T.M.V.; Suarez-Kurtz, G. Impact of Visceral Leishmaniasis and Curative Chemotherapy on Cytochrome P450 Activity in Brazilian Patients. Br. J. Clin. Pharmacol. 2015, 80, 1160–1168. [Google Scholar] [CrossRef]
- Pippa, L.F.; Vieira, C.P.; Caris, J.A.; Rocha, A.; Garcia, C.P.; Rezende, R.E.F.; Lanchote, V.L. Clinical Treatment for Hepatitis C Reverses CYP2C19 Inhibition. Br. J. Clin. Pharmacol. 2021, 87, 4013–4019. [Google Scholar] [CrossRef]
- Caris, J.A.; de Lima Benzi, J.R.; de Souza, F.F.L.; de Oliveira, R.D.R.; Donadi, E.A.; Lanchote, V.L. Rheumatoid Arthritis Downregulates the Drug Transporter OATP1B1: Fluvastatin as a Probe. Eur. J. Pharm. Sci. 2020, 146, 105264. [Google Scholar] [CrossRef]
- Pippa, L.F.; Vieira, C.P.; Caris, J.A.; Rocha, A.; Marques, M.P.; Garcia, C.P.; Rezende, R.E.F.; Lanchote, V.L. Effect of Chronic Hepatitis C on the Activity of the Membrane Transporters P-gp and OATP1B1/BCRP on Patients with Different Stages of Hepatic Fibrosis. Clin. Pharmacol. Ther. 2023, 114, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Cestari, R.N.; de Oliveira, R.D.R.; de Souza, F.F.L.; Pippa, L.F.; Nardotto, G.H.B.; Rocha, A.; Donadi, E.A.; Lanchote, V.L. Systemic Lupus Erythematosus Activity Affects the Sinusoidal Uptake Transporter OATP1B1 Evaluated by the Pharmacokinetics of Atorvastatin. Clin. Transl. Sci. 2020, 13, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
- Quinney, S.K.; Bonate, P.L. A Pharmacometrician’s Role in Enhancing Medication Use in Pregnancy and Lactation. J. Pharmacokinet. Pharmacodyn. 2020, 47, 267–269. [Google Scholar] [CrossRef]
- Kazma, J.M.; van den Anker, J.; Allegaert, K.; Dallmann, A.; Ahmadzia, H.K. Anatomical and Physiological Alterations of Pregnancy. J. Pharmacokinet. Pharmacodyn. 2020, 47, 271–285. [Google Scholar] [CrossRef] [PubMed]
- Eke, A.C.; Olagunju, A.; Momper, J.; Penazzato, M.; Abrams, E.J.; Best, B.M.; Capparelli, E.V.; Bekker, A.; Belew, Y.; Kiser, J.J.; et al. Optimizing Pharmacology Studies in Pregnant and Lactating Women Using Lessons From HIV: A Consensus Statement. Clin. Pharmacol. Ther. 2021, 110, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Abduljalil, K.; Ning, J.; Pansari, A.; Pan, X.; Jamei, M. Prediction of Maternal and Fetoplacental Concentrations of Cefazolin, Cefuroxime, and Amoxicillin during Pregnancy Using Bottom-Up Physiologically Based Pharmacokinetic Models. Drug Metab. Dispos. 2022, 50, 386–400. [Google Scholar] [CrossRef]
- Saleh, P.; Noshad, H.; Mallah, F.; Ramouz, A. Acute Pyelonephritis in Pregnancy and the Outcomes in Pregnant Patients. Arch. Clin. Infect. Dis. 2015, 10, e28886. [Google Scholar] [CrossRef]
- Jim, B.; Garovic, V.D. Acute Kidney Injury in Pregnancy. Semin. Nephrol. 2017, 37, 378–385. [Google Scholar] [CrossRef]
- Hedges, S.; Stenqvist, K.; Lidin-Janson, G.; Martinell, J.; Sandberg, T.; Svanborg, C. Comparison of Urine and Serum Concentrations of Interleukin-6 in Women with Acute Pyelonephritis or Asymtomatic Bacteriuria. J. Infect. Dis. 1992, 166, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, S.H.; Hylander, B.; Wretlind, B.; Brauner, A. Interleukin-6 and Interleukin-8 in Serum and Urine in Patients with Acute Pyelonephritis in Relation to Bacterial-Virulence-Associated Traits and Renal Function. Nephron 1994, 67, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Horcajada, J.P.; Velasco, M.; Filella, X.; Alvarez, L.; De Làzzari, E.; Marín, J.L.; Collvinent, B.; Smithson, A.; Martínez, J.A.; Noguero, M.; et al. Evaluation of Inflammatory and Renal-Injury Markers in Women Treated with Antibiotics for Acute Pyelonephritis Caused by Escherichia Coli. Clin. Diagn. Lab. Immunol. 2004, 11, 142–146. [Google Scholar] [CrossRef]
- Vree, T.B.; Van Den Biggelaar-Martea, M.; Verwey-van Wissen, C.P. Probenecid Inhibits the Renal Clearance of Frusemide and Its Acyl Glucuronide. Br. J. Clin. Pharmacol. 1995, 39, 692–695. [Google Scholar] [PubMed]
- Ebner, T.; Ishiguro, N.; Taub, M.E. The Use of Transporter Probe Drug Cocktails for the Assessment of Transporter-Based Drug-Drug Interactions in a Clinical Setting—Proposal of a Four Component Transporter Cocktail. J. Pharm. Sci. 2015, 104, 3220–3228. [Google Scholar] [CrossRef]
- Stopfer, P.; Giessmann, T.; Hohl, K.; Sharma, A.; Ishiguro, N.; Taub, M.E.; Zimdahl-Gelling, H.; Gansser, D.; Wein, M.; Ebner, T.; et al. Pharmacokinetic Evaluation of a Drug Transporter Cocktail Consisting of Digoxin, Furosemide, Metformin, and Rosuvastatin. Clin. Pharmacol. Ther. 2016, 100, 259–267. [Google Scholar] [CrossRef]
- Evers, R.; Piquette-Miller, M.; Polli, J.W.; Russel, F.G.M.; Sprowl, J.A.; Tohyama, K.; Ware, J.A.; de Wildt, S.N.; Xie, W.; Brouwer, K.L.R. Disease-Associated Changes in Drug Transporters May Impact the Pharmacokinetics and/or Toxicity of Drugs: A White Paper from the International Transporter Consortium. Clin. Pharmacol. Ther. 2018, 104, 900–915. [Google Scholar] [CrossRef] [PubMed]
- Hammarlund-Udenaes, M.; Benet, L.Z. Furosemide Pharmacokinetics and Pharmacodynamics in Health and Disease-An Update. J. Pharmacokinet. Biopharm. 1989, 17, 1–46. [Google Scholar] [CrossRef] [PubMed]
- Kerdpin, O.; Knights, K.M.; Elliot, D.J.; Miners, J.O. In Vitro Characterisation of Human Renal and Hepatic Frusemide Glucuronidation and Identification of the UDP-Glucuronosyltransferase Enzymes Involved in This Pathway. Biochem. Pharmacol. 2008, 76, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, P.V.B.; de Lima Moreira, F.; de Lima Benzi, J.R.; Duarte, G.; Lanchote, V.L. A Pilot Study of the Maternal-Fetal Pharmacokinetics of Furosemide in Plasma, Urine, and Amniotic Fluid of Hypertensive Parturient Women Under Cesarean Section. J. Clin. Pharmacol. 2020, 60, 1655–1661. [Google Scholar] [CrossRef]
- Mizuma, T.; McDonagh, A.F.; Lin, E.T.; Benet, L.Z. Photoinduced Covalent Binding of Frusemide and Frusemide Glucuronide to Human Serum Albumin. Br. J. Clin. Pharmacol. 1999, 48, 79–87. [Google Scholar] [CrossRef]
- Shen, H.; Holenarsipur, V.K.; Mariappan, T.T.; Drexler, D.M.; Cantone, J.L.; Rajanna, P.; Gautam, S.S.; Zhang, Y.; Gan, J.; Shipkova, P.A.; et al. Evidence for the Validity of Pyridoxic Acid (PDA) as a Plasma-Based Endogenous Probe for OAT1 and OAT3 Function in Healthy Subjects. J. Pharmacol. Exp. Ther. 2019, 368, 136–145. [Google Scholar] [CrossRef]
- De Lima Benzi, J.R.; Rocha, A.; Colombari, J.C.; Pego, A.M.G.; dos Santos Melli, P.P.; Duarte, G.; Lanchote, V.L. Determination of Furosemide and Its Glucuronide Metabolite in Plasma, Plasma Ultrafiltrate and Urine by HPLC-MS/MS with Application to Secretion and Metabolite Formation Clearances in Non-Pregnant and Pregnant Women. J. Pharm. Biomed. Anal. 2023, 235, 115635. [Google Scholar] [CrossRef]
- Klinkmann, G.; Klammt, S.; Jäschke, M.; Henschel, J.; Gloger, M.; Reuter, D.A.; Mitzner, S. Impact of Albumin Binding Function on Pharmacokinetics and Pharmacodynamics of Furosemide. Medicina 2022, 58, 1780. [Google Scholar] [CrossRef]
- Zaghloul, D.E.; Ryu, R.; Kestenbaum, B.; Smith, C.; Fay, E.; Hebert, M.F. Renal Function Estimating Equations Performance during Pregnancy and Postpartum. Pharmacotherapy 2023, 43, 359–372. [Google Scholar] [CrossRef]
- Statistical Guide for Clinical Pharmacology Therapeutics. Clin. Pharmacol. Ther. 2010, 88, 150–152. [CrossRef]
- Abbassi-Ghanavati, M.; Greer, L.G.; Cunningham, F.G. Pregnancy and Laboratory Studies A Reference Table for Clinicians. Obstet. Gynecol. 2009, 114, 1326–1357. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.O.; Kim, H.S.; Youn, J.C.; Shin, E.C.; Park, S. Serum Cytokine Profiles in Healthy Young and Elderly Population Assessed Using Multiplexed Bead-Based Immunoassays. J. Transl. Med. 2011, 9, 113. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, M.; Kusuhara, H.; Adachi, M.; Schuetz, J.D.; Takeuchi, K.; Sugiyama, Y. Multidrug Resistance-Associated Protein 4 Is Involved in the Urinary Excretion of Hydrochlorothiazide and Furosemide. J. Am. Soc. Nephrol. 2007, 18, 37–45. [Google Scholar] [CrossRef]
- Chapa, R.; Li, C.Y.; Basit, A.; Thakur, A.; Ladumor, M.K.; Sharma, S.; Singh, S.; Selen, A.; Prasad, B. Contribution of Uptake and Efflux Transporters to Oral Pharmacokinetics of Furosemide. ACS Omega 2020, 5, 32939–32950. [Google Scholar] [CrossRef]
- Prandota, J.; Witkowska, M.; Man, I. Pharmacokinetics and Metabolism of Furosemide in Man. Eur. J. Drug Metab. Pharmacokinet. 1976, 4, 177–181. [Google Scholar] [CrossRef]
- Mathialagan, S.; Feng, B.; Rodrigues, A.D.; Varma, M.V.S. Drug-Drug Interactions Involving Renal OCT2/MATE Transporters: Clinical Risk Assessment May Require Endogenous Biomarker-Informed Approach. Clin. Pharmacol. Ther. 2021, 110, 855–859. [Google Scholar] [CrossRef]
- Hasannejad, H.; Takeda, M.; Taki, K.; Shin, H.J.; Babu, E.; Jutabha, P.; Khamdang, S.; Aleboyeh, M.; Onozato, M.L.; Tojo, A.; et al. Interactions of Human Organic Anion Transporters with Diuretics. J. Pharmacol. Exp. Ther. 2004, 308, 1021–1029. [Google Scholar] [CrossRef]
- Lepist, E.I.; Zhang, X.; Hao, J.; Huang, J.; Kosaka, A.; Birkus, G.; Murray, B.P.; Bannister, R.; Cihlar, T.; Huang, Y.; et al. Contribution of the Organic Anion Transporter OAT2 to the Renal Active Tubular Secretion of Creatinine and Mechanism for Serum Creatinine Elevations Caused by Cobicistat. Kidney Int. 2014, 86, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Lenoir, C.; Rollason, V.; Desmeules, J.A.; Samer, C.F. Influence of Inflammation on Cytochromes P450 Activity in Adults: A Systematic Review of the Literature. Front. Pharmacol. 2021, 12, 733935. [Google Scholar] [CrossRef]
- Stanke-Labesque, F.; Gautier-Veyret, E.; Chhun, S.; Guilhaumou, R. Inflammation Is a Major Regulator of Drug Metabolizing Enzymes and Transporters: Consequences for the Personalization of Drug Treatment. Pharmacol. Ther. 2020, 215, 107627. [Google Scholar] [CrossRef] [PubMed]
- Cressman, A.M.; Petrovic, V.; Piquette-Miller, M. Inflammation-Mediated Changes in Drug Transporter Expression/Activity: Implications for Therapeutic Drug Response. Expert. Rev. Clin. Pharmacol. 2012, 5, 69–89. [Google Scholar] [CrossRef] [PubMed]
- Shibayama, T.; Sugiyama, D.; Kamiyama, E.; Tokui, T.; Hirota, T.; Ikeda, T. Characterization of CS-023 (RO4908463), a Novel Parenteral Carbapenem Antibiotic, and Meropenem as Substrates of Human Renal Transporters. Drug Metab. Pharmacokinet. 2007, 22, 41–47. [Google Scholar] [CrossRef]
- Akanuma, S.I.; Uchida, Y.; Ohtsuki, S.; Kamiie, J.I.; Tachikawa, M.; Terasaki, T.; Hosoya, K.I. Molecular-Weight-Dependent, Anionic-Substrate-Preferential Transport of β-Lactam Antibiotics via Multidrug Resistance-Associated Protein 4. Drug Metab. Pharmacokinet. 2011, 26, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, M.; Wakabayashi, Y.; Higuchi, A.; Kadotani, Y.; Ogino, S.; Ushigome, H.; Akioka, K.; Kaihara, S.; Yoshimura, N. Therapeutic Drug Monitoring of Mycophenolic Acid in Renal Transplant Recipients. Transplant. Proc. 2005, 37, 859–860. [Google Scholar] [CrossRef] [PubMed]
- Sommerer, C.; Müller-Krebs, S.; Schaier, M.; Glander, P.; Budde, K.; Schwenger, V.; Mikus, G.; Zeier, M. Pharmacokinetic and Pharmacodynamic Analysis of Enteric-Coated Mycophenolate Sodium: Limited Sampling Strategies and Clinical Outcome in Renal Transplant Patients. Br. J. Clin. Pharmacol. 2010, 69, 346–357. [Google Scholar] [CrossRef] [PubMed]
- García-Torre, A.; Bueno-García, E.; López-Martínez, R.; Rioseras, B.; Díaz-Molina, B.; Lambert, J.L.; Quirós, C.; Alonso-Álvarez, S.; Alonso-Arias, R.; Moro-García, M.A. CMV Infection Is Directly Related to the Inflammatory Status in Chronic Heart Failure Patients. Front. Immunol. 2021, 12, 687582. [Google Scholar] [CrossRef]
- Pour, N.K.; McColl, E.R.; Piquette-Miller, M. Impact of Viral Inflammation on the Expression of Renal Drug Transporters in Pregnant Rats. Pharmaceutics 2019, 11, 624. [Google Scholar] [CrossRef]
- Höcherl, K.; Schmidt, C.; Bucher, M. COX-2 Inhibition Attenuates Endotoxin-Induced Downregulation of Organic Anion Transporters in the Rat Renal Cortex. Kidney Int. 2009, 75, 373–380. [Google Scholar] [CrossRef]
- Deshmane, S.L.; Kremlev, S.; Amini, S.; Sawaya, B.E. Monocyte Chemoattractant Protein-1 (MCP-1): An Overview. J. Interferon Cytokine Res. 2009, 29, 313–325. [Google Scholar] [CrossRef]
- Lenoir, C.; Terrier, J.; Gloor, Y.; Curtin, F.; Rollason, V.; Desmeules, J.A.; Daali, Y.; Reny, J.L.; Samer, C.F. Impact of SARS-CoV-2 Infection (COVID-19) on Cytochromes P450 Activity Assessed by the Geneva Cocktail. Clin. Pharmacol. Ther. 2021, 110, 1358–1367. [Google Scholar] [CrossRef]
- Le Vee, M.; Lecureur, V.; Stieger, B.; Fardel, O. Regulation of Drug Transporter Expression in Human Hepatocytes Exposed to the Proinflammatory Cytokines Tumor Necrosis Factor-α or Interleukin-6. Drug Metab. Dispos. 2009, 37, 685–693. [Google Scholar] [CrossRef]
- Le Vee, M.; Jouan, E.; Stieger, B.; Lecureur, V.; Fardel, O. Regulation of Drug Transporter Expression by Oncostatin M in Human Hepatocytes. Biochem. Pharmacol. 2011, 82, 304–311. [Google Scholar] [CrossRef]
- Coppola, P.; Kerwash, E.; Cole, S. The Use of Pregnancy Physiologically Based Pharmacokinetic Modeling for Renally Cleared Drugs. J. Clin. Pharmacol. 2022, 62, S129–S139. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Olaleye, O.E.; Yu, X.; Jia, W.; Yang, J.; Lu, C.; Liu, S.; Yu, J.; Duan, X.; Wang, Y.; et al. Supporting Information for High Degree of Pharmacokinetic Compatibility Exists between the Five-Herb Medicine XueBiJing and Antibiotics Comedicated in Sepsis Care. Acta Pharm. Sin. B 2019, 9, 1035–1049. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, C.A.; Mattie, H.; Van Strijen, E. The Renal Clearance of Cefuroxime and Ceftazidime and the Effect of Probenecid on Their Tubular Excretion. Br. J. Clin. Pharmac. 1994, 37, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Kågedal, M.; Nilsson, D.; Huledal, G.; Reinholdsson, I.; Cheng, Y.F.; Åsenblad, N.; Pekar, D.; Borgå, O. A Study of Organic Acid Transporter-Mediated Pharmacokinetic Interaction between NXY-059 and Cefuroxime. J. Clin. Pharmacol. 2007, 47, 1043–1048. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Reference Range # | Phase 1 (n = 7) | Phase 2 (n = 7) | |
|---|---|---|---|
| Age (years) | - | 24.3 (16.1) | 24.3 (17.4) |
| Gestational age (weeks) | - | 26.7 (19.2) | 29.6 (17.3) |
| Body mass index (kg/m2) | - | 28.7 (17.0) | 29.3 (17.2) |
| Serum creatinine (mg/dL) | 0.6–1.1 | 0.63 (25.1) | 0.5 (23.0) |
| Estimated creatinine clearance * (mL/min) | >90.0 | 161.1 (21.3) | 189.2 (14.1) |
| AST (U/L) | 3.0–32.0 | 22.0 (42.1) | 22.7 (162.0) |
| ALT (U/L) | 3.0–33.0 | 16.0 (66.1) | 24.0 (187.4) |
| GGT (U/L) | 7.0–32.0 | 17.5 (66.5) | 27.9 (42.8) |
| Total plasma proteins (g/dL) | 6.1–7.90 | 5.9 (6.72) | 6.2 (4.70) |
| Albumin (g/dL) | 3.4–4.8 | 3.5 (9.31) | 3.6 (8.10) |
| α1-Acid glycoprotein | 50.0–120.0 | 86.9 (35.1) | 65.0 (23.4) |
| Alkaline phosphatase (U/L) | 65.0–300.0 | 157.1 (23.6) | 169.5 (22.7) |
| Fasting glycemia (mg/dL) | 70.0–100.0 | 79.8 (12.1) | 76.7 (11.2) |
| Medications in use | cefuroxime; oseltamivir; ferrous sulfate; metamizole; tramadol; folic acid; scopolamine; tinidazole (topical); terbutaline; betamethasone; levothyroxine; ondansetron; progesterone; heparin; sulfamethoxazole; and trimethoprim | ferrous sulfate; metamizole; folic acid; miconazole (topic); levothyroxine; and heparin |
| Cytokines (pg/mL) and CRP (mg/dL) | Phase 1 (n = 7) | Phase 2 (n = 7) | p-Value |
|---|---|---|---|
| IFN-γ | 5.80 (5.50–9.41) | 0.92 (0.73–1.91) | 0.0313 |
| IL-10 | 32.30 (19.79–113.80) | 3.12 (1.53–49.7) | 0.3125 |
| IL-12p40 | 3.28 (1.17–35.32) | 1.34 (1.07–17.4) | >0.999 |
| IL-12p70 | 1.85 (1.04–2.37) | 1.04 (1.04–1.32) | 0.1563 |
| IL-1β | 1.00 (0.59–4.18) | 1.10 (0.60–2.40) | >0.999 |
| IL-2 | 0.76 (0.62–1.21) | 0.68 (0.61–1.16) | 0.6875 |
| IL-6 | 34.04 (1.97–126.60) | 0.21 (0.11–23.7) | 0.0469 |
| IL-8 | 4.70 (0.22–100.83) | 0.28 (0.15–31.4) | 0.8438 |
| MCP-1 | 807.34 (418.20–1232.50) | 373.32 (277.00–403.45) | 0.0313 |
| TNF-α | 41.63 (17.28–54.15) | 17.01 (13.30–21.42) | 0.0313 |
| CRP | 21.54 (13.46–58.84) | 2.34 (1.10–3.54) | 0.0313 |
| Geometric Mean (CV%) | Geometric Mean Ratios (90% CI) | p-Value | ||
|---|---|---|---|---|
| Phase 1 (n = 7) | Phase 2 (n = 7) | Phase 2/Phase 1 | ||
| AUC0–24 (ng·h/mL) | 1303.0 (38.3) | 1065.0 (7.1) | 0.67 (0.45–1.01) | 0.2386 |
| AUC0–∞ (ng·h/mL) | 1373.0 (38.3) | 1196.0 (14.1) | 0.72 (0.48–1.08) | 0.4465 |
| CL/F (L/h) | 29.1 (38.8) | 37.6 (7.20) | 1.61 (1.10–2.35) | 0.2300 |
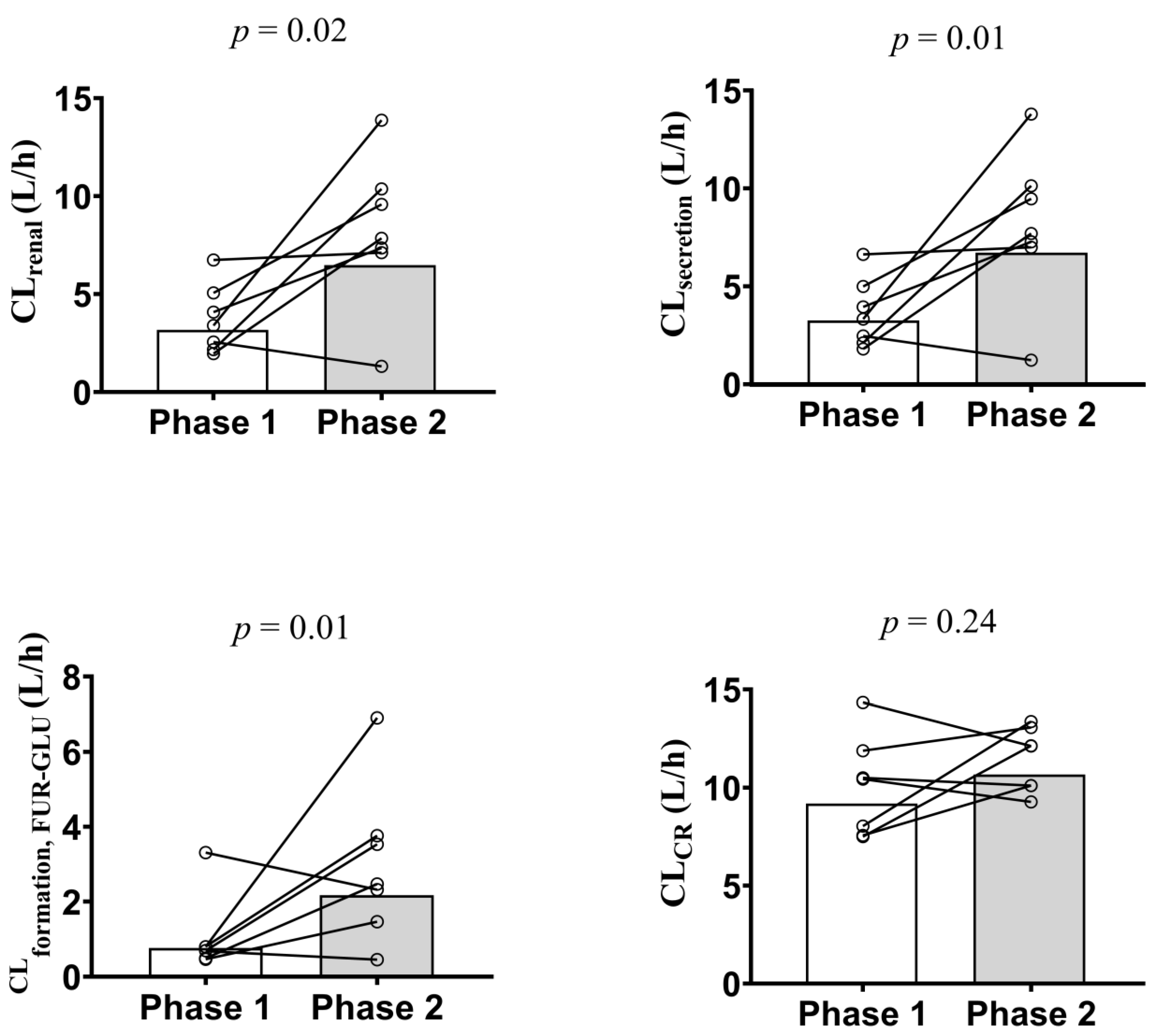
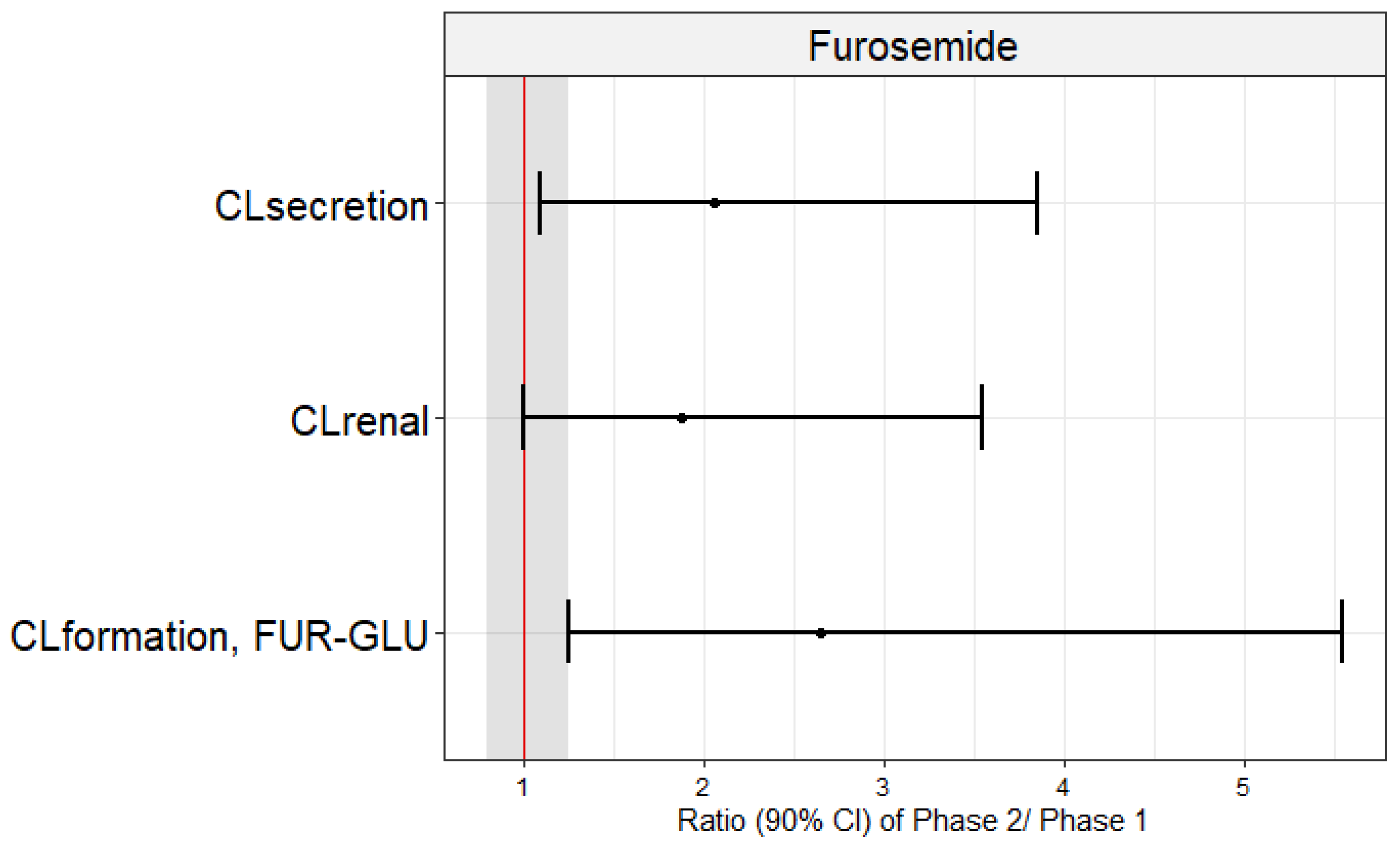
| CLrenal (L/h) | 4.2 (45.5) | 6.9 (43.3) | 1.89 (1.01–3.54) | 0.0262 |
| CLsecretion (L/h) | 3.9 (43.4) | 6.7 (43.8) | 2.06 (1.12–3.80) | 0.0126 |
| CLformation, FUR-GLU (L/h) | 1.1 (85.9) | 2.3 (64.1) | 2.65 (1.28–5.49) | 0.0161 |
| Ae (mg) | 5.5 (20.8) | 7.3 (46.3) | 1.29 (0.73–2.28) | 0.3006 |
| CL/Fnon-renal (L/h) | 21.5 (62.4) | 29.1 (14.6) | 1.65 (0.92–2.96) | 0.6999 |
| Cmax (ng/mL) | 337.2 (48.5) | 377.4 (39.8) | 0.95 (0.51–1.77) | 0.3525 |
| Tmax (h) | 1.5 (1.0–4.0) * | 1.0 (1.0–2.0) * | 0.7 (0.5–1.0) | 0.0938 |
| fu | 0.010 (32.0) | 0.011 (40.3) | 1.04 (0.77–1.42) | 0.6499 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benzi, J.R.d.L.; Melli, P.P.d.S.; Duarte, G.; Unadkat, J.D.; Lanchote, V.L. The Impact of Inflammation on the In Vivo Activity of the Renal Transporters OAT1/3 in Pregnant Women Diagnosed with Acute Pyelonephritis. Pharmaceutics 2023, 15, 2427. https://doi.org/10.3390/pharmaceutics15102427
Benzi JRdL, Melli PPdS, Duarte G, Unadkat JD, Lanchote VL. The Impact of Inflammation on the In Vivo Activity of the Renal Transporters OAT1/3 in Pregnant Women Diagnosed with Acute Pyelonephritis. Pharmaceutics. 2023; 15(10):2427. https://doi.org/10.3390/pharmaceutics15102427
Chicago/Turabian StyleBenzi, Jhohann Richard de Lima, Patrícia Pereira dos Santos Melli, Geraldo Duarte, Jashvant D. Unadkat, and Vera Lucia Lanchote. 2023. "The Impact of Inflammation on the In Vivo Activity of the Renal Transporters OAT1/3 in Pregnant Women Diagnosed with Acute Pyelonephritis" Pharmaceutics 15, no. 10: 2427. https://doi.org/10.3390/pharmaceutics15102427
APA StyleBenzi, J. R. d. L., Melli, P. P. d. S., Duarte, G., Unadkat, J. D., & Lanchote, V. L. (2023). The Impact of Inflammation on the In Vivo Activity of the Renal Transporters OAT1/3 in Pregnant Women Diagnosed with Acute Pyelonephritis. Pharmaceutics, 15(10), 2427. https://doi.org/10.3390/pharmaceutics15102427