


Laser-Assisted Drug Delivery: A Systematic Review of Safety and Adverse Events


Abstract
1. Introduction
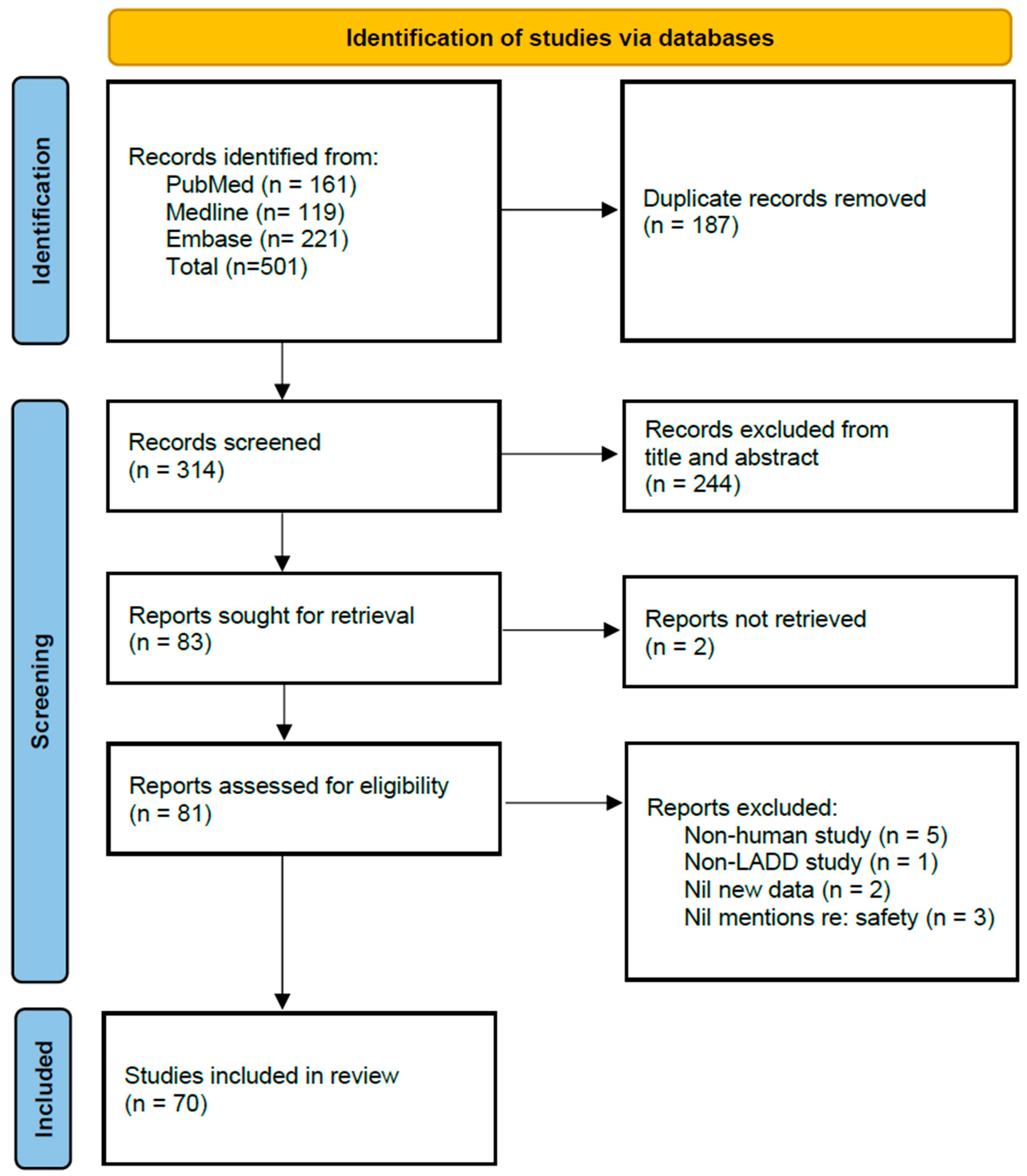
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A
Search Strategy
References
- Wenande, E.; Anderson, R.R.; Haedersdal, M. Fundamentals of fractional laser-assisted drug delivery: An in-depth guide to experimental methodology and data interpretation. Adv. Drug Deliv. Rev. 2020, 153, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Labadie, J.G.; Ibrahim, S.A.; Worley, B.; Kang, B.Y.; Rakita, U.; Rigali, S.; Arndt, K.A.; Bernstein, E.; Brauer, J.A.; Chandra, S.; et al. Evidence-Based Clinical Practice Guidelines for Laser-Assisted Drug Delivery. JAMA Dermatol. 2022, 158, 1193–1201. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Li, P.; Wang, B.; Deng, Y.; Li, J.; Mao, M.; Jian, D. Multi-Factors Associated With Efficacy and Adverse Events of Fractional Erbium:YAG Laser-Assisted Delivery of Topical Betamethasone for Stable Vitiligo: A Retrospective Analysis. Lasers Surg. Med. 2020, 52, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.W.; Levitt, A.E.; Erickson, B.P.; Ko, A.; Nikpoor, N.; Ezuddin, N.; Lee, W.W. Ablative Fractional Laser Resurfacing with Laser-Assisted Delivery of 5-Fluorouracil for the Treatment of Cicatricial Ectropion and Periocular Scarring. Ophthalmic Plast. Reconstr. Surg. 2018, 34, 274–279. [Google Scholar] [CrossRef]
- Jacques, S.L.; McAuliffe, D.J.; Blank, I.H.; Parrish, J.A. Controlled removal of human stratum corneum by pulsed laser. J. Investig. Dermatol. 1987, 88, 88–93. [Google Scholar] [CrossRef]
- Ruela, A.L.; Perissinato, A.G.; Lino, M.E.; Mudrik, P.S.; Pereira, G.R. Evaluation of skin absorption of drugs from topical and transdermal formulations. Braz. J. Pharm. Sci. 2016, 52, 527–544. [Google Scholar] [CrossRef]
- Rapalli, V.K.; Singhvi, G. Dermato-pharmacokinetic: Assessment tools for topically applied dosage forms. Expert Opin. Drug Deliv. 2021, 18, 423–426. [Google Scholar] [CrossRef]
- Gao, Y.; Du, L.; Li, Q.; Li, Q.; Zhu, L.; Yang, M.; Wang, X.; Zhao, B.; Ma, S. How physical techniques improve the transdermal permeation of therapeutics: A review. Medicine 2022, 101, e29314. [Google Scholar] [CrossRef]
- Alegre-Sánchez, A.; Jiménez-Gómez, N.; Boixeda, P. Laser-Assisted Drug Delivery. Vehiculización de fármacos asistida por láser. Actas Dermosifiliogr. 2018, 109, 858–867. [Google Scholar] [CrossRef]
- Haedersdal, M.; Sakamoto, F.H.; Farinelli, W.A.; Doukas, A.G.; Tam, J.; Anderson, R.R. Fractional CO(2) laser-assisted drug delivery. Lasers Surg. Med. 2010, 42, 113–122. [Google Scholar] [CrossRef]
- Bachhav, Y.G.; Heinrich, A.; Kalia, Y.N. Using laser microporation to improve transdermal delivery of diclofenac: Increasing bioavailability and the range of therapeutic applications. Eur. J. Pharm. Biopharm. 2011, 78, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Sklar, L.R.; Burnett, C.T.; Waibel, J.S.; Moy, R.L.; Ozog, D.M. Laser assisted drug delivery: A review of an evolving technology. Lasers Surg. Med. 2014, 46, 249–262. [Google Scholar] [CrossRef] [PubMed]
- Ali, F.R.; Al-Niaimi, F. Laser-assisted drug delivery in dermatology: From animal models to clinical practice. Lasers Med. Sci. 2016, 31, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Truong, K.; Prasidha, I.; Wain, T. A systematic review of randomised controlled trials investigating laser assisted drug delivery for the treatment of keloid and hypertrophic scars. Lasers Med. Sci. 2022, 37, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Steeb, T.; Schlager, J.G.; Kohl, C.; Ruzicka, T.; Heppt, M.V.; Berking, C. Laser-assisted photodynamic therapy for actinic keratosis: A systematic review and meta-analysis. J. Am. Acad. Dermatol. 2019, 80, 947–956. [Google Scholar] [CrossRef]
- Ng, W.H.S.; Smith, S.D. Laser-Assisted Drug Delivery: A Systematic Review of Safety and Adverse Events; OSF: Charlottesville, VA, USA, 2022. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Alster, T.S.; Tanzi, E.L. Photodynamic therapy with topical aminolevulinic acid and pulsed dye laser irradiation for sebaceous hyperplasia. J. Drugs Dermatol. 2003, 2, 501–504. [Google Scholar]
- Stevenson, M.L.; Karen, J.K.; Hale, E.K. Laser-Assisted Photodynamic Therapy: Two Novel Protocols for Enhanced Treatment Results. J. Drugs Dermatol. 2017, 16, 329–331. [Google Scholar]
- Lonsdorf, A.S.; Keller, A.; Hartmann, J.; Enk, A.H.; Gholam, P. Ablative Fractional Laser-assisted Low-irradiance Photodynamic Therapy for Treatment of Actinic Keratoses in Organ Transplant Recipients: A Prospective, Randomized, Intraindividual Controlled Trial. Acta Derm. Venereol. 2022, 102, adv00694. [Google Scholar] [CrossRef]
- Fredman, G.; Wenande, E.; Hendel, K.; Togsverd-Bo, K.; Haedersdal, M. Efficacy and safety of laser-assisted combination chemotherapy: A follow-up study of treatment with 5-fluorouracil and cisplatin for basal cell carcinoma. Lasers Surg. Med. 2022, 54, 113–120. [Google Scholar] [CrossRef]
- Paasch, U.; Said, T. Treating Field Cancerization by Ablative Fractional Laser and Indoor Daylight: Assessment of Efficacy and Tolerability. J. Drugs Dermatol. 2020, 19, 425–427. [Google Scholar] [CrossRef] [PubMed]
- Wenande, E.; Hendel, K.; Mogensen, M.; Bagger, C.; Mårtensson, N.L.; Persson, D.P.; Lerche, C.M.; Husted, S.; Janfelt, C.; Togsverd-Bo, K.; et al. Efficacy and Safety of Laser-Assisted Combination Chemotherapy: An Explorative Imaging-Guided Treatment With 5-Fluorouracil and Cisplatin for Basal Cell Carcinoma. Lasers Surg. Med. 2021, 53, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Pires, M.T.F.; Pereira, A.D.; Durães, S.M.B.; Issa, M.C.A.; Pires, M. Laser-assisted MAL-PDT associated with acoustic pressure wave ultrasound with short incubation time for field cancerization treatment: A left-right comparison. Photodiagnosis Photodyn. Ther. 2019, 28, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Dairi, M.; Dadban, A.; Arnault, J.P.; Lok, C.; Chaby, G. Localized mycosis fungoides treated with laser-assisted photodynamic therapy: A case series. Clin. Exp. Dermatol. 2019, 44, 930–932. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Song, K.H. Ablative fractional laser-assisted photodynamic therapy provides superior long-term efficacy compared with standard methyl aminolevulinate photodynamic therapy for lower extremity Bowen disease. J. Am. Acad. Dermatol. 2018, 79, 860–868. [Google Scholar] [CrossRef]
- Vrani, F.; Sotiriou, E.; Lazaridou, E.; Vakirlis, E.; Sideris, N.; Kirmanidou, E.; Apalla, Z.; Lallas, A.; Ioannides, D. Short incubation fractional CO2 laser-assisted photodynamic therapy vs. conventional photodynamic therapy in field-cancerized skin: 12-month follow-up results of a randomized intraindividual comparison study. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Hsu, S.H.; Gan, S.D.; Nguyen, B.T.; Konnikov, N.; Liang, C.A. Ablative Fractional Laser-Assisted Topical Fluorouracil for the Treatment of Superficial Basal Cell Carcinoma and Squamous Cell Carcinoma In Situ: A Follow-Up Study. Dermatol. Surg. 2016, 42, 1050–1053. [Google Scholar] [CrossRef]
- Nisticò, S.; Sannino, M.; Del Duca, E.; Tamburi, F.; Bottoni, U.; Cannarozzo, G. Ablative fractional laser improves treatment of actinic keratoses with Ingenol Mebutate. Eur. J. Inflamm. 2016, 14, 200–205. [Google Scholar] [CrossRef]
- Braun, S.A.; Hevezi, P.; Homey, B.; Gerber, P.A. Laser-assisted drug delivery: Enhanced response to ingenol mebutate after ablative fractional laser treatment. J. Am. Acad. Dermatol. 2015, 72, 364–365. [Google Scholar] [CrossRef]
- Choi, S.H.; Kim, K.H.; Song, K.H. Efficacy of ablative fractional laser-assisted photodynamic therapy for the treatment of actinic cheilitis: 12-month follow-up results of a prospective, randomized, comparative trial. Br. J. Dermatol. 2015, 173, 184–191. [Google Scholar] [CrossRef]
- Choi, S.H.; Kim, K.H.; Song, K.H. Efficacy of ablative fractional laser-assisted photodynamic therapy with short-incubation time for the treatment of facial and scalp actinic keratosis: 12-month follow-up results of a randomized, prospective, comparative trial. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1598–1605. [Google Scholar] [CrossRef] [PubMed]
- Helsing, P.; Togsverd-Bo, K.; Veierød, M.B.; Mørk, G.; Haedersdal, M. Intensified fractional CO2 laser-assisted photodynamic therapy vs. laser alone for organ transplant recipients with multiple actinic keratoses and wart-like lesions: A randomized half-side comparative trial on dorsal hands. Br. J. Dermatol. 2013, 169, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Ko, D.Y.; Jeon, S.Y.; Kim, K.H.; Song, K.H. Fractional erbium: YAG laser-assisted photodynamic therapy for facial actinic keratoses: A randomized, comparative, prospective study. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 1529–1539. [Google Scholar] [CrossRef] [PubMed]
- Machado, B.H.B.; Zhang, J.; Frame, J.; Najlah, M. Treatment of Scars with Laser-Assisted Delivery of Growth Factors and Vitamin C: A Comparative, Randomised, Double-blind, Early Clinical Trial. Aesthetic Plast. Surg. 2021, 45, 2363–2374. [Google Scholar] [CrossRef]
- Manuskiatti, W.; Kaewkes, A.; Yan, C.; Ng, J.N.; Glahn, J.Z.; Wanitphakdeedecha, R. Hypertrophic Scar Outcomes in Fractional Laser Monotherapy Versus Fractional Laser-Assisted Topical Corticosteroid Delivery: A Randomized Clinical Trial. Acta Derm. Venereol. 2021, 101, adv00416. [Google Scholar] [CrossRef]
- Abd El-Dayem, D.H.; Nada, H.A.; Hanafy, N.S.; Elsaie, M.L. Laser-assisted topical steroid application versus steroid injection for treating keloids: A split side study. J. Cosmet. Dermatol. 2021, 20, 138–142. [Google Scholar] [CrossRef]
- Neinaa, Y.M.E.; Al-Khayat, L.A.; Suliman, G.A.M.; Ameen, T.E. Fractional carbon dioxide laser-assisted delivery of lyophilized-growth factors is a promising treatment modality of post-acne scars. Dermatol. Ther. 2020, 33, e14488. [Google Scholar] [CrossRef]
- Sabry, H.H.; Ibrahim, E.A.; Hamed, A.M. Assessment of laser-assisted delivery vs intralesional injection of botulinum toxin A in treatment of hypertrophic scars and keloids. Dermatol. Ther. 2020, 33, e13980. [Google Scholar] [CrossRef]
- Wang, J.; Wu, J.; Xu, M.; Gao, Q.; Chen, B.; Wang, F.; Song, H. Combination therapy of refractory keloid with ultrapulse fractional carbon dioxide (CO2) laser and topical triamcinolone in Asians-long-term prevention of keloid recurrence. Dermatol. Ther. 2020, 33, e14359. [Google Scholar] [CrossRef]
- Waibel, J.S.; Wulkan, A.J.; Rudnick, A.; Daoud, A. Treatment of Hypertrophic Scars Using Laser-Assisted Corticosteroid Versus Laser-Assisted 5-Fluorouracil Delivery. Dermatol. Surg. 2019, 45, 423–430. [Google Scholar] [CrossRef]
- Kraeva, E.; Ho, D.; Jagdeo, J. Successful Treatment of Keloid with Fractionated Carbon Dioxide (CO2) Laser and Laser-Assisted Drug Delivery of Triamcinolone Acetonide Ointment in an African-American Man. J. Drugs Dermatol. 2017, 16, 925–927. [Google Scholar] [PubMed]
- Park, J.H.; Chun, J.Y.; Lee, J.H. Laser-assisted topical corticosteroid delivery for the treatment of keloids. Lasers Med. Sci. 2017, 32, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Cavalié, M.; Sillard, L.; Montaudié, H.; Bahadoran, P.; Lacour, J.P.; Passeron, T. Treatment of keloids with laser-assisted topical steroid delivery: A retrospective study of 23 cases. Dermatol. Ther. 2015, 28, 74–78. [Google Scholar] [CrossRef]
- Botsali, A.; Esme, P.; Erbil, H.; Caliskan, E. Comparison of fractional erbium:YAG laser-assisted tranexamic acid delivery alone and in combination with oral tranexamic acid in melasma. Lasers Med. Sci. 2022, 37, 2823–2830. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Yao, C.; Zhang, H.; Li, L.; Song, Y. Efficacy and safety of 755-nm picosecond alexandrite laser with topical tranexamic acid versus laser monotherapy for melasma and facial rejuvenation: A multicenter, randomized, double-blinded, split-face study in Chinese patients. Lasers Med. Sci. 2022, 37, 2879–2887. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Park, J.W.; Seo, S.J.; Park, K.Y. Evaluating the tolerance and efficacy of laser-assisted delivery of tranexamic acid, niacinamide, and kojic acid for melasma: A single center, prospective, split-face trial. Dermatol. Ther. 2022, 35, e15287. [Google Scholar] [CrossRef]
- Wang, J.V.; Christman, M.P.; Feng, H.; Ferzli, G.; Jeon, H.; Geronemus, R.G. Laser-assisted delivery of tranexamic acid for melasma: Pilot study using a novel 1927 nm fractional thulium fiber laser. J. Cosmet. Dermatol. 2021, 20, 105–109. [Google Scholar] [CrossRef]
- Wanitphakdeedecha, R.; Sy-Alvarado, F.; Patthamalai, P.; Techapichetvanich, T.; Eimpunth, S.; Manuskiatti, W. The efficacy in treatment of facial melasma with thulium 1927-nm fractional laser-assisted topical tranexamic acid delivery: A split-face, double-blind, randomized controlled pilot study. Lasers Med. Sci. 2020, 35, 2015–2021. [Google Scholar] [CrossRef]
- Doghaim, N.N.; El-Tatawy, R.A.; Ismail, M.A.; Ali, D.A.M.; El Attar, Y.A. Study the effect of erbium:YAG laser plus topical 5-flurouracil in stable vitiligo resistant to NB-UVB phototherapy. J. Cosmet. Dermatol. 2020, 19, 122–130. [Google Scholar] [CrossRef]
- Badawi, A.M.; Osman, M.A. Fractional erbium-doped yttrium aluminum garnet laser-assisted drug delivery of hydroquinone in the treatment of melasma. Clin. Cosmet. Investig. Dermatol. 2018, 11, 13–20. [Google Scholar] [CrossRef]
- Yan, R.; Yuan, J.; Chen, H.; Li, Y.-H.; Wu, Y.; Gao, X.-H.; Chen, H.-D. Fractional Er:YAG laser assisting topical betamethasone solution in combination with NB-UVB for resistant non-segmental vitiligo. Lasers Med. Sci. 2017, 32, 1571–1577. [Google Scholar] [CrossRef] [PubMed]
- Hanthavichai, S.; Archavarungson, N.; Wongsuk, T. A study to assess the efficacy of fractional carbon dioxide laser with topical platelet-rich plasma in the treatment of androgenetic alopecia. Lasers Med. Sci. 2022, 37, 2279–2286. [Google Scholar] [CrossRef] [PubMed]
- Soror, O.A.; Abdel-Bary, A.; Khalil, B.M. Fractional carbon dioxide laser-assisted topical steroid delivery versus intralesional steroid in the treatment of alopecia areata. J. Egypt. Women’s Dermatol. Soc. 2021, 18, 43. [Google Scholar] [CrossRef]
- Majid, I.; Jeelani, S.; Imran, S. Fractional Carbon Dioxide Laser in Combination with Topical Corticosteroid Application in Resistant Alopecia Areata: A Case Series. J. Cutan. Aesthet. Surg. 2018, 11, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Bertin, A.C.J.; Vilarinho, A.; Junqueira, A.L.A. Fractional non-ablative laser-assisted drug delivery leads to improvement in male and female pattern hair loss. J. Cosmet. Laser Ther. 2018, 20, 391–394. [Google Scholar] [CrossRef]
- Kim, T.I.; Ahn, H.J.; Kang, I.H.; Jeong, K.H.; Kim, N.I.; Shin, M.K. Nonablative fractional laser-assisted daylight photodynamic therapy with topical methyl aminolevulinate for moderate to severe facial acne vulgaris: Results of a randomized and comparative study. Photodermatol. Photoimmunol. Photomed. 2017, 33, 253–259. [Google Scholar] [CrossRef]
- Jung, J.Y.; Hong, J.S.; Ahn, C.H.; Yoon, J.Y.; Kwon, H.H.; Suh, D.H. Prospective randomized controlled clinical and histopathological study of acne vulgaris treated with dual mode of quasi-long pulse and Q-switched 1064-nm Nd:YAG laser assisted with a topically applied carbon suspension. J. Am. Acad. Dermatol. 2012, 66, 626–633. [Google Scholar] [CrossRef]
- Haedersdal, M.; Togsverd-Bo, K.; Wiegell, S.R.; Wulf, H.C. Long-pulsed dye laser versus long-pulsed dye laser-assisted photodynamic therapy for acne vulgaris: A randomized controlled trial. J. Am. Acad. Dermatol. 2008, 58, 387–394. [Google Scholar] [CrossRef]
- Singer, A.J.; Weeks, R.; Regev, R. Laser-assisted anesthesia reduces the pain of venous cannulation in children and adults: A randomized controlled trial. Acad. Emerg. Med. 2006, 13, 623–628. [Google Scholar] [CrossRef]
- Singer, A.J.; Regev, R.; Weeks, R.; Tlockowski, D.S. Laser-assisted anesthesia prior to intravenous cannulation in volunteers: A randomized, controlled trial. Acad. Emerg. Med. 2005, 12, 804–807. [Google Scholar] [CrossRef]
- Baron, E.D.; Harris, L.; Redpath, W.S.; Shapiro, H.; Hetzel, F.; Morley, G.; Bar-Or, D.; Stevens, S.R. Laser-assisted penetration of topical anesthetic in adults. Arch. Dermatol. 2003, 139, 1288–1290. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, M.; Abu-Ghali, M.M.; El-Sayed, M.T.; Soltan, M.Y. Fractional CO2-assisted photodynamic therapy improves the clinical outcome and patient’s satisfaction in toenail onychomycosis treatment: An intra-patient comparative single-center study. J. Dermatol. Treat. 2022, 33, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Koren, A.; Salameh, F.; Sprecher, E.; Artzi, O. Laser-assisted Photodynamic Therapy or Laser-assisted Amorolfine Lacquer Delivery for Treatment of Toenail Onychomycosis: An Open-label Comparative Study. Acta Derm. Venereol. 2018, 98, 467–468. [Google Scholar] [CrossRef]
- Bhatta, A.K.; Keyal, U.; Huang, X.; Zhao, J.J. Fractional carbon-dioxide (CO2) laser-assisted topical therapy for the treatment of onychomycosis. J. Am. Acad. Dermatol. 2016, 74, 916–923. [Google Scholar] [CrossRef] [PubMed]
- Rajbanshi, B.; Shen, L.; Jiang, M.; Gao, Q.; Huang, X.; Ma, J.; Wang, J.; Hu, Y.; Lv, H.; Wu, X.; et al. Comparative Study of Traditional Ablative CO2 Laser-Assisted Topical Antifungal with only Topical Antifungal for Treating Onychomycosis: A Multicenter Study. Clin. Drug Investig. 2020, 40, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Agamia, N.F.; Sobhy, N.; Abd-Elraouf, A.; Tawfik, A. Fractional CO2 Laser for Transcutaneous Drug Delivery of Onabotulinum Toxin in Palmar Hyperhidrosis. Dermatol. Surg. 2021, 47, 678–683. [Google Scholar] [CrossRef] [PubMed]
- Johnson, H.; Kazemi, T.; Farah, R.S. Safety profile of laser-assisted drug delivery of vitamin C, E, and ferulic acid serum following ablative fractional resurfacing: A retrospective chart review. J. Cosmet. Laser Ther. 2021, 23, 207–208. [Google Scholar] [CrossRef]
- Wang, J.V.; Ugonabo, N.; Geronemus, R.G. Fractional Ablative Laser-Assisted Delivery of Topical Poly-l-lactic Acid: A 2.5-Year Safety Review. Dermatol. Surg. 2022, 48, 258–259. [Google Scholar] [CrossRef]
- Bauer, M.; Lackner, E.; Matzneller, P.; Al Jalali, V.; Pajenda, S.; Ling, V.; Böhler, C.; Braun, W.; Braun, R.; Boesch, M.; et al. Phase I Study to Assess Safety of Laser-Assisted Topical Administration of an Anti-TNF Biologic in Patients with Chronic Plaque-Type Psoriasis. Front. Med. 2021, 8, 712511. [Google Scholar] [CrossRef]
- Essa Abd Elazim, N.; Mahmoud Abdelsalam, A.; Mohamed Awad, S. Efficacy of combined fractional carbon dioxide laser and topical tazarotene in nail psoriasis treatment: A randomized intrapatient left-to-right study. J. Cosmet. Dermatol. 2022, 21, 2808–2816. [Google Scholar] [CrossRef]
- Helmy, A.Y.; El Batreek, M.H.; Abdel Fadeel, D.A.; Tawfik, A.A.; Samy, N.A. Efficacy of the topical cyclosporine cream assisted by fractional carbon dioxide laser vs topical clobetasol cream for the treatment of plaque psoriasis: Randomized comparative study. J. Cosmet. Dermatol. 2022, 21, 3362–3370. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Wang, C.; Cao, Y.; Lv, X.; Tian, L.; Liu, D.; Li, L.; Zhao, W. Fractional 2940-nm Er:YAG laser-assisted drug delivery of timolol maleate for the treatment of deep infantile hemangioma. J. Dermatol. Treat. 2021, 32, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Junsuwan, N.; Manuskiatti, W.; Phothong, W.; Wanitphakdeedecha, R. Fractional CO2 laser-assisted Botulinum toxin type A delivery for the treatment of primary palmar hyperhidrosis. Lasers Med. Sci. 2021, 36, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Shehadeh, W.; Matz, H.; Ellenbogen, E.; Sprecher, E.; Artzi, O. Pulse-Dye Laser Followed by Betamethasone-Calcipotriol and Fractional Ablative CO2-Laser-Assisted Delivery for Nail Psoriasis. Dermatol. Surg. 2021, 47, e111–e116. [Google Scholar] [CrossRef] [PubMed]
- Sobhi, R.M.; Sharaoui, I.; El Nabarawy, E.A.; El Nemr Esmail, R.S.; Hegazy, R.A.; Aref, D.H.F. Comparative study of fractional CO2 laser and fractional CO2 laser-assisted drug delivery of topical steroid and topical vitamin C in macular amyloidosis. Lasers Med. Sci. 2018, 33, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Park, S.M.; Kim, G.W.; Mun, J.H.; Song, M.; Kim, H.-S.; Kim, B.-S.; Kim, M.-B.; Ko, H.-C. Fractional Laser-Assisted Topical Imiquimod 5% Cream Treatment for Recalcitrant Common Warts in Children: A Pilot Study. Dermatol. Surg. 2016, 42, 1340–1346. [Google Scholar] [CrossRef]
- Ma, G.; Wu, P.; Lin, X.; Chen, H.; Hu, X.; Jin, Y.; Qiu, Y. Fractional carbon dioxide laser-assisted drug delivery of topical timolol solution for the treatment of deep infantile hemangioma: A pilot study. Pediatr. Dermatol. 2014, 31, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Veremis-Ley, M.; Ramirez, H.; Baron, E.; Hanneman, K.; Lankerani, L.; Scull, H.; Cooper, K.D.; Nedorost, S. Laser-assisted penetration of allergens for patch testing. Dermatitis 2006, 17, 15–22. [Google Scholar] [CrossRef]
- Benzaquen, M.; Fongue, J.; Pauly, V.; Collet-Villette, A.M. Laser-Assisted Hyaluronic Acid Delivery by Fractional Carbon Dioxide Laser in Facial Skin Remodeling: A Prospective Randomized Split-Face Study in France. Lasers Surg. Med. 2021, 53, 1166–1172. [Google Scholar] [CrossRef]
- Machado, B.H.B.; Frame, J.; Zhang, J.; Najlah, M. Comparative Study on the Outcome of Periorbital Wrinkles Treated with Laser-Assisted Delivery of Vitamin C or Vitamin C Plus Growth Factors: A Randomized, Double-blind, Clinical Trial. Aesthetic Plast. Surg. 2021, 45, 1020–1032. [Google Scholar] [CrossRef]
- Widianingsih, N.P.; Setyaningrum, T.; Prakoeswa, C.R. The efficacy and safety of fractional erbium YAG laser combined with topical amniotic membrane stem cell (AMSC) metabolite product for facial rejuvenation: A controlled, Split-Face Study. Dermatol. Rep. 2019. [Google Scholar] [CrossRef]
- Elsaie, M.L.; Nouri, K.; Vejjabhinanta, V.; Rivas, M.P.; Villafradez-Diaz, L.M.; Martins, A.; Rosso, R. Topical imiquimod in conjunction with Nd:YAG laser for tattoo removal. Lasers Med. Sci. 2009, 24, 871–875. [Google Scholar] [CrossRef]
- Ricotti, C.A.; Colaco, S.M.; Shamma, H.N.; Trevino, J.; Palmer, G.; Heaphy, M.R., Jr. Laser-assisted tattoo removal with topical 5% imiquimod cream. Dermatol. Surg. 2007, 33, 1082–1091. [Google Scholar] [CrossRef] [PubMed]
- Banzhaf, C.A.; Thaysen-Petersen, D.; Bay, C.; Philipsen, P.A.; Mogensen, M.; Prow, T.; Haedersdal, M. Fractional laser-assisted drug uptake: Impact of time-related topical application to achieve enhanced delivery. Lasers Surg. Med. 2017, 49, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Oni, G.; Rasko, Y.; Kenkel, J. Topical lidocaine enhanced by laser pretreatment: A safe and effective method of analgesia for facial rejuvenation. Aesthet. Surg. J. 2013, 33, 854–861. [Google Scholar] [CrossRef]
- Prohaska, J.; Hohman, M.H. Laser Complications. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Alam, M.; Warycha, M. Complications of lasers and light treatments. Dermatol. Ther. 2011, 24, 571–580. [Google Scholar] [CrossRef]
- Alexiades-Armenakas, M. Laser-mediated photodynamic therapy. Clin. Dermatol. 2006, 24, 16–25. [Google Scholar] [CrossRef]
- Ibbotson, S.H.; Wong, T.H.; Morton, C.A.; Collier, N.; Haylett, A.; McKenna, K.; Mallipeddi, R.; Moseley, H.; Rhodes, L.; Seukeran, D.; et al. Adverse effects of topical photodynamic therapy: A consensus review and approach to management. Br. J. Dermatol. 2019, 180, 715–729. [Google Scholar] [CrossRef]
- Piaserico, S.; Mazzetto, R.; Sartor, E.; Bortoletti, C. Combination-Based Strategies for the Treatment of Actinic Keratoses with Photodynamic Therapy: An Evidence-Based Review. Pharmaceutics 2022, 14, 1726. [Google Scholar] [CrossRef]
- Landa, N.; Corrons, N.; Zabalza, I.; Azpiazu, J.L. Urticaria induced by laser epilation: A clinical and histopathological study with extended follow-up in 36 patients. Lasers Surg. Med. 2012, 44, 384–389. [Google Scholar] [CrossRef]
- England, R.W.; Vogel, P.; Hagan, L. Immediate cutaneous hypersensitivity after treatment of tattoo with nd:YAG laser: A case report and review of the literature. Ann. Allergy Asthma Immunol. 2002, 89, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Khunger, N.; Molpariya, A.; Khunger, A. Complications of Tattoos and Tattoo Removal: Stop and Think Before you ink. J. Cutan. Aesthet. Surg. 2015, 8, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Wilken, R.; Ho, D.; Petukhova, T.; Jagdeo, J. Intraoperative localized urticarial reaction during Q-switched Nd:YAG laser tattoo removal. J. Drugs Dermatol. 2015, 14, 303–304. [Google Scholar] [PubMed]
- Hibler, B.P.; Rossi, A.M. A case of delayed anaphylaxis after laser tattoo removal. JAAD Case Rep. 2015, 1, 80–81. [Google Scholar] [CrossRef]
- Lee, A.Y. Recent progress in melasma pathogenesis. Pigment. Cell Melanoma Res. 2015, 28, 648–660. [Google Scholar] [CrossRef]
- Seneschal, J.; Boniface, K.; D’Arino, A.; Picardo, M. An update on Vitiligo pathogenesis. Pigment. Cell Melanoma Res. 2021, 34, 236–243. [Google Scholar] [CrossRef]
- Tierney, E.P.; Hanke, C.W. Review of the literature: Treatment of dyspigmentation with fractionated resurfacing. Dermatol. Surg. 2010, 36, 1499–1508. [Google Scholar] [CrossRef]
- Preissig, J.; Hamilton, K.; Markus, R. Current Laser Resurfacing Technologies: A Review that Delves Beneath the Surface. Semin. Plast. Surg. 2012, 26, 109–116. [Google Scholar] [CrossRef]
- Love, W.E.; Bernhard, J.D.; Bordeaux, J.S. Topical imiquimod or fluorouracil therapy for basal and squamous cell carcinoma: A systematic review. Arch. Dermatol. 2009, 145, 1431–1438. [Google Scholar] [CrossRef]
- Ibbotson, S.H. Adverse effects of topical photodynamic therapy. Photodermatol. Photoimmunol. Photomed. 2011, 27, 116–130. [Google Scholar] [CrossRef]


{kind=link}
| Author | Patient Cohorts | Number of LADD Recipients | Condition | Intervention | Laser | Adverse Events | Relevant Negative Findings |
|---|---|---|---|---|---|---|---|
| Lonsdorf 2022 [20] | Intrapatient comparison | 18 | AKs in organ transplant recipients | LADD + MAL-PDT vs. PDT | AFXL Er:YAG | Pain necessitating early termination of PDT (n = 2) | No therapy-associated systemic side-effects on day of rx and in F/U period |
| Fredman 2022 [21] | Single arm (follow up from previous study) | 20 | BCC (superficial & low-risk nodular) | LADD + Cisplatin + 5-FU | AFXL CO2 | Persistent erythema (n = 5, <6 months; n = 2, @12 months), Hypopigmentation (n = 11 @12 months), Hyperpigmentation (n = 10 @3 months; n = 4 @6months) Scarring (n = 8 @6 months; n = 4 @12 months) Temporary crusting, inflammation | Nil severe adverse events |
| Paasch 2020 [22] | Prospective uncontrolled | 46 | Field cancerization (AK) | LADD + ALA-PDT (indoor light) | AFXL CO2 | Pain (severe) | - |
| Wenande 2020 [23] | Single arm, prospective | 19 | BCC | LADD + 5-FU and cisplatin | AFXL CO2 | Ooze (100%), Persistent erythema (83%), Hyperpigmentation (56%), Scarring (50%), Oedema, pruritus (32%), Mild hypopigmentation (17%) | Nil reported infection, systemic symptoms Nil cisplatin, 5-FU detected in blood 24h post-treatment (6 patients tested) |
| Pires 2019 [24] | Intrapatient comparison (split-arm) | 15 | AK | LADD + Acoustic pressure wave ultrasound + MAL-PDT vs. MAL-PDT | AFXL CO2 | Mild pain (all, <3 h), Erythema, edema, crusts (all, <15 days) | Nil scarring on follow-up |
| Dairi 2018 [25] | Case series | 4 | Mycosis fungoides | LADD+MAL-PDT | AFXL CO2 | Varying degrees of pain, local irritation, post-inflammatory hyperpigmentation lasting months (all) | Nil other adverse events noted |
| Kim 2018 [26] | Prospective uncontrolled | 30 | Lower extremity Bowen disease | LADD + MAL-PDT | AFXL Er:YAG | Erythema (n = 28 <7 days), Crusting (n = 24), Hyperpigmentation (n = 23), Burning sensation (n = 22), Pruritus (n = 21) Oedema (n = 9), Bullae (n = 3), Pain | - |
| Vrani 2018 [27] | Intrapatient comparison | 50 | AK | LADD + MAL-PDT vs. PDT | AFXL CO2 | Erythema, oedema (all) Pustular eruption and crusting formation (n = 15). | Nil pain with AFXL, nil post-procedure scarring/pigmentary changes |
| Hsu 2016 [28] | Prospective single arm | 28 | Primary SCCis and sBCC | LADD + 5-FU | AFXL CO2 | - | Nil treatment-related adverse events |
| Nisticò 2016 [29] | Intrapatient comparison | 13 | AK | LADD + Ingenol Mebutate vs. Ingenol Mebutate | AFXL CO2 | Erythema (n = 13), Vesicles (n = 8), Oozing & crusts (n = 4) | |
| Braun 2015 [30] | Case report | 1 | Multiple AK | LADD + Ingenol mebutate | AFXL Er:YAG | - | No systemic side effects or safety concerns |
| Choi 2015 [31] | Prospective, dual arm | 14 | Actinic chelitis | LADD + MAL-PDT vs. MAL-PDT | AFXL Er:YAG | Mild-moderate pain (all, <7 d) Erythema (n = 13), Burning sensation (n = 13), Swelling, (n = 5) Haemorrhagic crusting (n = 3), Blistering (n = 2) | Nil systemic adverse effects |
| Choi 2015 [32] | Prospective, three-arm | 64 | AK | LADD + 2h MAL-PDT vs. LADD + 3h MAL-PDT vs. MAL-PDT | AFXL Er:YAG | 2h vs. 3h Crust (86.8% vs. 82.8%), Erythema (78.1% vs. 80%), Hyperpigmentation (75.5% vs. 75.9%), Burning sensation (73.5%, vs. 75.9%), Pruritus (45.7%, vs. 52.4%) Oedema (7.9% vs. 6.9%), Bullae (4.6% vs. 6.2%) | Phototoxic adverse events were mild-moderate, short duration, did not require additional therapy |
| Helsing 2013 [33] | Intrapatient comparison | 10 | AK and wart-like lesions in organ transplant recipients | LADD + MAL-PDT vs. AFXL laser only | AFXL CO2 | Intense inflammation and purpura (n=3) Erythema, oedema, pain (n=3) | - |
| Ko 2013 [34] | Prospective, dual arm | 23 | Facial AK | LADD + MAL-PDT vs. MAL-PDT | AFXL Er:YAG | Erythema (100%), Hyperpigmentation (100%, <20weeks)) Crust (100%), Burning sensation (73.8%), Pruritus (53.3%), Bleeding (31.8%), Scale (31.8%), Oedema (8.4%), Bullae (6.5%) | - |
| Author | Patient Cohorts | Number of LADD Recipients | Condition | Intervention | Laser | Adverse Events | Relevant Negative Findings |
|---|---|---|---|---|---|---|---|
| Machado 2021 [35] | RCT–2 arms | 132 | Scars (misc) | LADD + Vitamin C vs. LADD + Vitamin C and Growth Factors | AFXL ErYag | Nil reported | Nil local or systemic adverse reaction |
| Manuskiatti 2021 [36] | Intrapatient comparison (split-scar) | 24 | Hypertrophic scars | LADD + Clobetasol Propionate vs. LADD + Petrolatum | AFXL Er:YAG | Nil reported | Nil telangiectasias, dyspigmentation, skin atrophy, acneiform eruption |
| Abd El-Dayem 2020 [37] | Intrapatient comparison | 30 | Keloid scars | LADD betamethasone vs. intralesional triamcinolone acetonide | AFXL Er:YAG | Hyperpigmentation (n = 2) | No serious side effects |
| Neinaa 2020 [38] | Intrapatient comparison | 45 | Post-acne scars | LADD lypophylized-growth factors vs. LADD PRP | AFXL CO2 | PRP vs. L-GFs Mild post-inflammatory hyperpigmentation (n = 8 vs. n = 13), Moderate post-inflammatory hyperpigmentation (n = 5 vs. n = 0) Acneiform eruption (n = 8) Downtime (2–5 days) Pain (<3 days) | No major side effects |
| Sabry 2020 [39] | Intrapatient comparison (split-scar) | 20 | Keloids/hypetrophic scars | LADD + BTX-A vs. Intralesional BTX-A | AFXL CO2 | Pain, pruritus | - |
| Wang 2020 [40] | Prospective uncontrolled | 41 | Refractory keloids | LADD + Triamcinolone | AFXL CO2 | Telengiectasia (n = 1), Hyperpigmentation (n = 4) | Nil allergic reaction, infection |
| Waibel 2019 [41] | Prospective–2 arms | 20 | Hypertrophic scars | LADD + Triamcinolone vs. LADD+5-FU | AFXL CO2 | With LADD + triamcinolone-dermal atrophy, telangiectasia, persistent erythema | - |
| Kraeva 2017 [42] | Case report | 1 | Keloid scar (Fitzpatrick type VI skin) | LADD+ Triamcinolone acetonide | AFXL CO2 | - | Nil complications or adverse events |
| Park 2015 [43] | Intrapatient comparison | 10 | Keloid scars (from BCG vaccination) | LADD + Desoxymethasone vs. AFXL+ Triamcinolone acetonide | AFXL Er:YAG | Micro-crust | No serious adverse reactions or events |
| Cavalié 2014 [44] | Retrospective cohort | 23 | Treatment resistant keloids | LADD betamethasone under occlusion | AFXL Er:YAG | Hypochromia in darker skin types, (n = 5 <1 month), Folliculitis (n = 3), Eczematous reaction to occlusive film (n = 3), Pain | - |
| Author | Patient Cohorts | Number of LADD Recipients | Condition | Intervention | Laser | Adverse Events | Relevant Negative Findings |
|---|---|---|---|---|---|---|---|
| Botsali 2022 [45] | Propsective trial | 54 | Melasma | LADD 5% Tranexamic Acid vs. LADD 5% Tranexamic + Oral Tranexamic Acid | AFXL Er:YAG | Increase in MASI (1.8–3.2 points) in skin types III, IV (n = 2) | No serious adverse effects |
| Li 2022 [46] | Intrapatient comparison | 37 | Melasma | LADD+ 10% Tranexamic acid vs. Laser + saline | 755 nm picosecond alexandrite | Irritation (n = 17), Erythema (n = 36), Dryness (n = 36), Post-inflammatory hyperpigmentation (n = 10), Scaling (n = 3) | Nil hypopigmentation, infection, and scarring |
| Park 2021 [47] | Intrapatient comparison | 25 | Melasma | LADD + 3%Tranexamic acid, 5% Niacinamide, 1% Kojic acid vs. Nd-YAG alone | Q-switched Nd:YAG | Facial erythema (self-limiting) | Treatment was well-tolerated |
| Wang 2020 [48] | Prospective study | 10 | Melasma | LADD Tranexamic Acid | 1927nm fractional thulium | Transient (skin) roughness, dryness, itching | All adverse effects were mild |
| Wanitphakdeedecha 2020 [49] | Intrapatient comparison | 46 | Facial melasma | LADD + 1.2% Tranexamic acid vs. Laser + Saline | FTL | Mild hyperpigmentation (n = 4) Mild pain | No scarring, hypopigmentation, or persistent erythema |
| Doghaim 2019 [50] | Intrapatient comparison | 40 | Stable vitiligo resistant to NBUVB | LADD + 5-FU + NBUVB vs. NBUVB | AFXL Er:YAG | Transient hyperpigmentation (all), Minimal scarring (n = 1), Tolerable pain (all) | Nil Koebnerization on follow-up |
| Huang 2019 [3] | Retrospective review; single arm | 684 | Stable vitiligo | LADD + Betamethasone | AFXL Er:YAG | Slight erythema, oedema (all) Hyperpigmentation (14.4%) Epidermal atrophy, telangiectasia, and hypertrichosis in lesions (0.14%) | Nil local infections, scarring, Koebner’s phenomenon, and aggravation of vitiligo |
| Badawi 2018 [51] | Intrapatient comparison (split-face) | 32 | Melasma | LADD + Hydroxychloroquine vs. hydroxychloroquine | AFXL Er:YAG | Erythema (all, <4 days), Superficial crusting, burning sensation (n = 7), Pruritus (n = 3), Superficial crusting | Nil worsening of melasma |
| Yan 2016 [52] | Intrapatient comparison | 22 | Non-segmental, resistant vitiligo | LADD + Betamethasone+ NBUVB vs. NBUVB | AFXL Er:YAG | Slight pain, burning sensation, edema, erythema (all), Micro-crust (~50%, <3 days) | Nil local infection, scarring, Koebner phenomenon, aggravation of vitiligo |
| Author | Patient Cohorts | Number of LADD Recipients | Condition | Intervention | Laser | Adverse Events | Relevant Negative Findings |
|---|---|---|---|---|---|---|---|
| Hanthavichai 2021 [53] | Prospective trial | 8 | Androgenetic alopecia | LADD + PRP | AFXL CO2 | Tolerable pain (n = 7, <several days) Mild pruritus (n = 2, <several days), Dandruff (n = 4, pts <2 weeks) | Analgesia not required before/after LADD Nil participants withdrew from study due to pain No serious adverse events such as infection, scarring, worsening of hair loss, and burn No scalp erythema and swelling were detected |
| Soror 2021 [54] | Intrapatient comparison | 30 | Alopecia areata | LADD + Triamcinolone vs. Intralesional Triamcinolone | AFXL CO2 | Mild telangiectasia (n = 1) | No significant adverse effects |
| Majid 2019 [55] | Case series | 10 | Alopecia areata | LADD + Triamcinolone | AFXL CO2 | - | No significant adverse effects, skin atrophy |
| Bertin 2018 [56] | Case series | 5 | Female/male pattern hair loss | LADD of topical finasteride, growth factors (vEGF, FGF, IGF, cooper peptide) | Non-ablative 1550 nm fractional Er:Glass | Mild pain, post-procedure transient erythema; (n = 2, <2 h) | “No significant side effects” |
| Author | Patient Cohorts | Number of LADD Recipients | Condition | Intervention | Laser | Adverse Events | Relevant Negative Findings |
|---|---|---|---|---|---|---|---|
| Kim 2017 [57] | Prospective trial | 14 | Severe acne vulgaris | LADD + MAL + DL-PDT vs. MAL + DL-PDT | Non-ablative Er:glass | Erythema (n = 2, <1 week), Hyperpigmentation (n = 1), Tanning (n = 1) Pain | Nil bullae, crust, post-inflammatory hyperpigmentation |
| Jung 2011 [58] | Intrapatient comparison | 22 | Acne vulgaris | LADD + carbon lotion vs. Laser only. Noted that laser was after lotion application | Quasi-long and Q-switched ND:YAG | Transient erythema (all, <3 h), Mild dryness, mild desquamation (n = 15) Mild pain | Nil severe adverse events |
| Hædersdal 2008 [59] | Intrapatient comparison (split-face) | 15 | Acne vulgaris | LADD + MAL vs. Laser only | Long-pulsed dye laser | Erythema, oedema (n = 15) Pustular eruptions (n = 12) Yellow crusting mx with topical abx (n = 1) Moderate-severe pain | Nil long-term adverse reactions such as pigment changes, scarring |
| Author | Patient Cohorts | Number of LADD Recipients | Condition | Intervention | Laser | Adverse Events | Relevant Negative Findings |
|---|---|---|---|---|---|---|---|
| Singer 2006 [60] | RCT | 30 | Pre- cannulation analgesia | LADD + Lidocaine vs. lidocaine | AFXL Er:YAG | Mild pain with laser | Nil persistent erythema, infections |
| Singer 2005 [61] | RCT (Intrapatient comparison) | 30 | Pre- cannulation analgesia | LADD + Lidocaine vs. lidocaine | Er:YAG | Mild pain | Nil persistent erythema, infection, or scarring |
| Baron 2003 [62] | 2x trials, Prospective dual arm | 320 | Needlestick (investigating analgesia efficacy) | LADD + Lidocaine vs. Laser + Placebo AND LADD + Lidocaine vs. Topical Lidocaine | Er:YAG | Mild pain, Erythema (n = 10) | - |
| Author | Patient Cohorts | Number of LADD Recipients | Condition | Intervention | Laser | Adverse Events | Relevant Negative Findings |
|---|---|---|---|---|---|---|---|
| Abdallah 2022 [63] | Intrapatient comparison (foot vs. foot) | 21 | Onychomycosis | LADD + PDT vs. PDT | AFXL CO2 | Significant pain (n = 21), Pinpoint bleeding (n = 3) | All side effects were tolerated and temporary. |
| Koren 2017 [64] | Intrapatient comparison | 60 | Toenail onychomycosis | LADD + ALA-PDT vs. LADD + Amorolfine | AFXL CO2 | Pain; scores 2.1–8.5/10 | - |
| Bhatta 2016 [65] | Prospective, nil comparison | 75 | Onychomycosis | LADD + 1% terbinafine | AFXL CO2 | Pain; mean 1.93/10 | Nil bleeding, oozing, bacterial infection, contact dermatitis |
| Rajbanshi 2020 [66] | Prospective, dual arm | 80 | Onychomycosis | LADD + Terbinafine vs. Terbinafine | AFXL CO2 | Pain (mean = 3.5/10) | Nil bleeding, infection Nil dermatitis, oozing. Nil observed medication cross-reaction |
| Author | Patient Cohorts | Number of LADD Recipients | Condition | Intervention | Laser | Adverse Events | Relevant Negative Findings |
|---|---|---|---|---|---|---|---|
| Agamia 2022 [67] | Intrapatient comparison | 30 | Palmar hyperhidrosis | LADD + BTX-A vs. Intradermal BTX-A | AFXL CO2 | Pain | - |
| Johnson 2022 [68] | Retrospective review | 33 | Misc medical & cosmetic | LADD + Serum (15% Vitamin C, 1% Vitamin E, and 0.5% Ferulic acid) | AFXL CO2 | Erythema (n = 6), Erythema+tenderness (n = 1), Erythema+mild bumpiness (n = 1), Skin peeling (n = 1), Pain+bleeding (n = 1) | All side effects resolved |
| Wang 2022 [69] | Retrospective review | 94 | Misc medical & cosmetic | LADD poly-l-lactic acid | AFXL CO2 | - | Nil documented adverse effects. Nil filler nodules, delayed wound healing, prolonged erythema, and abnormal scarring |
| Bauer 2021 [70] | Intrapatient comparison | 8 | Chronic plaque-type psoriasis | LADD + Etanercept vs. Etanercept vs. AFXL alone | AFXL Er:YAG | Itching, redness, pain, ulceration * | Nil clinically significant deviation in lab results (chemistry, haematology, lipid panels) |
| Elazim 2021 [71] | Intrapatient comparison | 32 | Nail psoriasis | LADD + 0.1% Tazarotene vs. 0.1% Tazarotene | AFXL CO2 | Mild-moderate pain (all, transient), Bleeding (n = 2) Periungual erythema (n = 2) | - |
| Helmy 2021 [72] | Prospective trial | 11 | Plaque psoriasis | LADD + Cyclosporine vs. Clobetasol | AFXL CO2 | Mild burning and stinging (n = 2, < 48 h) | - |
| Sun 2021 [73] | Single arm prospective | 30 | Infantile hemangioma | LADD + Timolol | AFXL Er Yag | Detectable timolol systemically, 1.580–14.718 pg/mL in 8/20 patients. Erythema, oedema, blisters | Nil bradycardia, hypotension, hypoglycaemia, liver and kidney dysfunction, dyspnoea, lethargy, sweating in all subjects. Nil pigmentation, hypopigmentation, scars |
| Junsuwan 2020 [74] | Intrapatient comparison (palm vs. palm) | 3 | Palmar hyperhidrosis | LADD + BTX-A vs. nil treatment | AFXL | Pain–scale: 4-6/10 | Nil pigmentation, textural changes. Nil change in hand dexterity, strength. |
| Shehadeh 2020 [75] | Intrapatient comparison | 22 | Nail Psoriasis | LADD + Betamethasone-Calcipotriol gel | Proximal and lateral nail folds–595nm PDL, Nail–AFXL CO2 | Pain, Participants withdrew due to pain (n = 3) Local irritation/pain (<hours) erythema, purpura (<days) | - |
| Sobhi 2018 [76] | Intrapatient comparison (split-lesion) | 10 | Macular amyloidosis | AFXL vs. LADD + Topical Corticosteroid vs. LADD + Topical Corticosteroid + Vitamin C | AFXL CO2 | Post-inflammatory hyperpigmentation (n = 1) | - |
| Lee 2017 [4] | Retrospective cohort | 6 | Cicatricial ectropion | LADD 5-FU | Various AFXL | - | No adverse effects other than AFXL-related |
| Park 2016 [77] | Prospective single arm | 11 | Common warts (paediatric patients) | LADD + Imiquimod | AFXL Er:YAG | Transient scabbing (n = 10), Erythema (n = 6), Pruritus (n = 4), (All adverse effects resolving in several days) | Nil serious adverse events necessitating additional treatment |
| Ma 2014 [78] | Prospective single arm | 9 | Infantile hemangiomas | LADD + Timolol | AFXL CO2 | Pinpoint bleeding, fluid exudation (<1 day), Erythema, oedema (2–3 days), Dot crusting (5–7 days) | Nil detectable plasma timolol post-procedure. Nil significant change in HR, BP, BSL |
| Veremis-Ley 2006 [79] | Intrapatient comparison | 14 | For patch-testing | LADD + Patch Tests vs. Laser only vs. Patch Tests only | AFXL Er:YAG | Pruritus to positive- reaction sites, Crust and transient skin darkening (skin types IV, V)/lightening in skin types II, III (<10 days), TEWL increase (<48 h) | Nil reported side effects by patients, pain at laser-treated sites |
| Author | Patient Cohorts | Number of LADD Recipients | Condition | Intervention | Laser | Adverse Events | Relevant Negative Findings |
|---|---|---|---|---|---|---|---|
| Benzaquen 2021 [80] | Intrapatient comparison | 20 | Heloderma stigmas | LADD + Hyaluronic acid vs. LADD Saline | AFXL | Erythema, oedema, crust | Nil granuloma formation at 8 months F/U |
| Machado 2020 [81] | RCT | 149 | Periorbital wrinkles | LADD + Vitamin C vs. LADD + Vitamin C+ Growth Factors | AFXL Er:YAG | Nil reported | Nil adverse reaction locally or systemically |
| Widianingsih 2019 [82] | Intrapatient comparison | 9 | Phoaging | LADD Amniotic Membrane Stem Cell vs. Laser + Saline | AFXL Er:YAG | Erythema (all, <2 weeks), Mild pain (n = 7), Acneiform eruption (n = 2), Crusting | Nil post-inflammatory hyperpigmentation |
| Elsaie 2009 [83] | Intrapatient comparison | 3 | Tattoo removal | LADD Imiquimod vs. Laser + Vehicle cream | Nd:YAG | Moderate pain Pruritus (n = 1) | Nil pruritus, pain, burning, scarring, ulceration, pigmentary alterations, or vascular changes |
| Ricotti 2007 [84] | Intrapatient comparison | 20 | Tattoo removal | LADD Imiquimod vs. Laser + Placebo Cream | Q-switched Nd:YAG, frequency-doubled Nd:YAG laser, Q-switched alexandrite | Pruritus (60%) Erythema (55%) Scale (40%) Burning (35%), Erosions (30%), Poor healing of biopsy site (20%) Urticaria (10%) 1 subject-recurrent and generalized urticarial reaction with facial angioedema | - |
| Author | Patient Cohorts | Number of LADD Recipients | Condition | Intervention | Laser | Adverse Events | Relevant Negative Findings |
|---|---|---|---|---|---|---|---|
| Banzhaf 2016 [85] | Intrapatient comparison | 11 | Healthy skin | AFXL + Fluorescein | AFXL CO2 | Transient oedema, erythema, micro-crusting | - |
| Oni 2013 [86] | Prospective, dual arm | 10 | To study LADD anaesthetic safety | LADD (Full ablative Er:YAG) vs. LADD (AFXL CO2) Delivery of 20% benzocaine, 6% lidocaine, and 4% tetracaine cream | Er:YAG and AFXL CO2 | Post-treatment hyperpigmentation (n = 1, <1 mo), rx w hydroxychloroquine cream) Pain | For all patients in all groups, serum lidocaine and MEGX did not reach toxic levels, maximum was 0.935 μg/mL. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, W.H.S.; Smith, S.D. Laser-Assisted Drug Delivery: A Systematic Review of Safety and Adverse Events. Pharmaceutics 2022, 14, 2738. https://doi.org/10.3390/pharmaceutics14122738
Ng WHS, Smith SD. Laser-Assisted Drug Delivery: A Systematic Review of Safety and Adverse Events. Pharmaceutics. 2022; 14(12):2738. https://doi.org/10.3390/pharmaceutics14122738
Chicago/Turabian StyleNg, William Hao Syuen, and Saxon D. Smith. 2022. "Laser-Assisted Drug Delivery: A Systematic Review of Safety and Adverse Events" Pharmaceutics 14, no. 12: 2738. https://doi.org/10.3390/pharmaceutics14122738
APA StyleNg, W. H. S., & Smith, S. D. (2022). Laser-Assisted Drug Delivery: A Systematic Review of Safety and Adverse Events. Pharmaceutics, 14(12), 2738. https://doi.org/10.3390/pharmaceutics14122738