Recent Advances and Impact of Chemotherapeutic and Antiangiogenic Nanoformulations for Combination Cancer Therapy




Abstract
1. Introduction
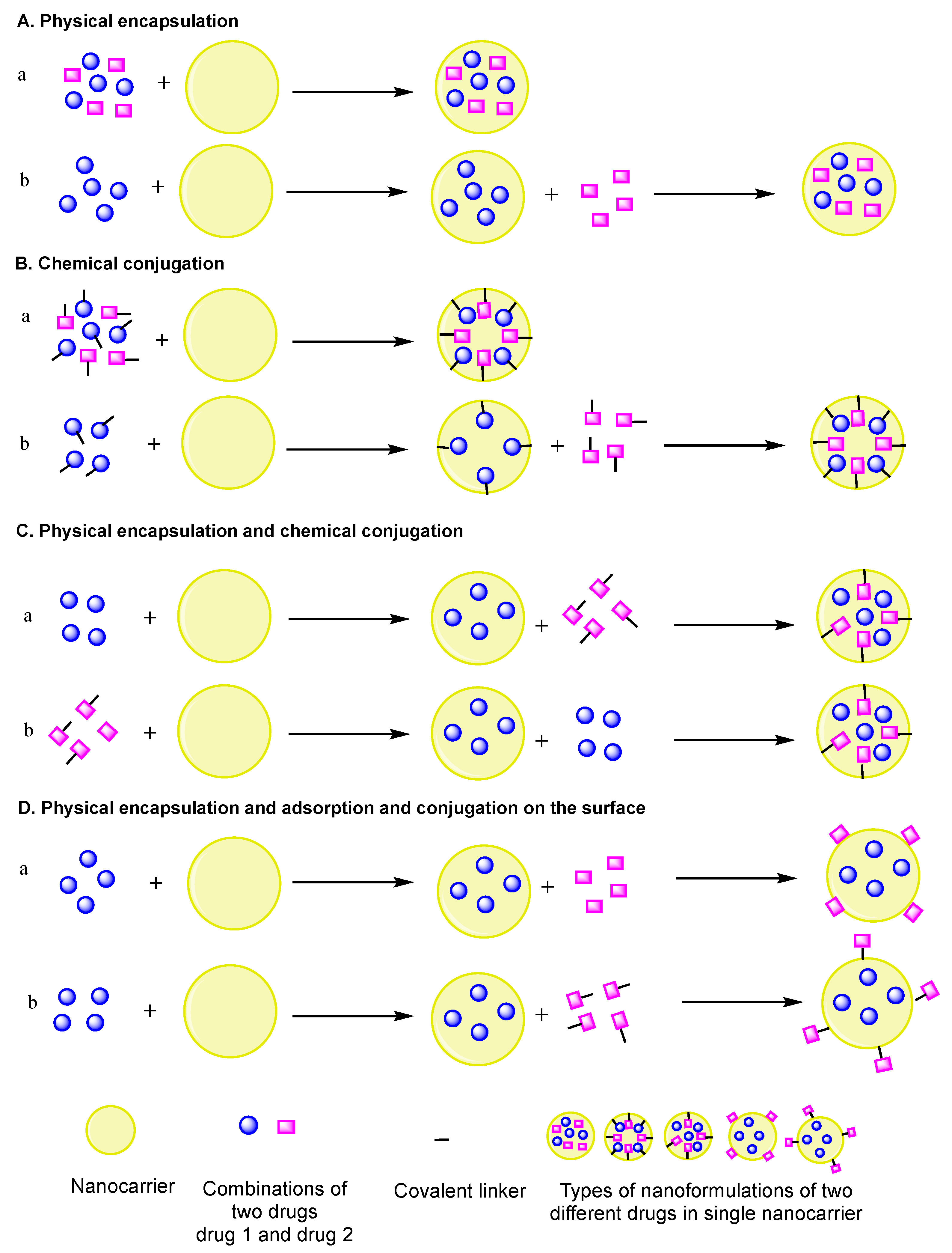
2. Nanoformulations of Anticancer and Antiangiogenesis Drugs for Combination Cancer Therapy
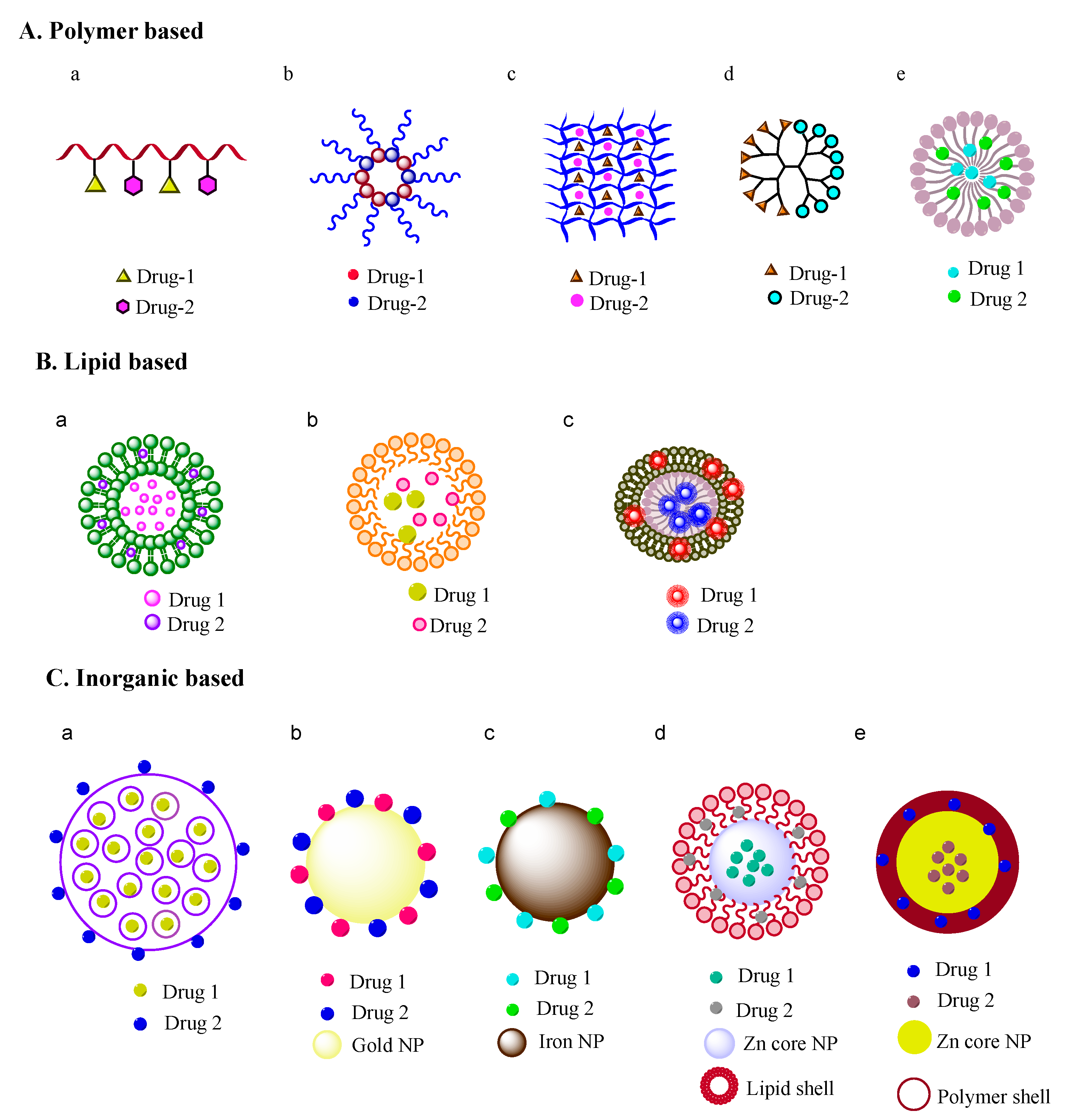
2.1. Polymeric-Based Nanoformulations
2.2. Lipid Based Nanoformulations
2.3. Inorganic Material-Based Nanoformulations
3. Future Perspectives, Outlook, and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO Factsheet. Available online: https://www.who.int/en/news-room/fact-sheets/detail/cancer (accessed on 29 March 2020).
- Devita, V.T.; Chu, E. A history of cancer chemotherapy. Cancer Res. 2008, 68, 8643–8653. [Google Scholar] [CrossRef] [PubMed]
- DePinho, R.A. The age of cancer. Nature 2000, 408, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Bertram, J.S. The molecular biology of cancer. Mol. Asp. Med. 2000, 21, 167–223. [Google Scholar] [CrossRef]
- Bizzarri, M.; Cucina, A. Tumour and the microenvironment: A chance to reframe the paradigm of carcinogenesis? BioMed Res. Int. 2014, 2014, 934038. [Google Scholar] [CrossRef]
- Sonugür, F.G.; Akbulut, H. The Role of tumour microenvironment in genomic instability of malignant tumours. Front. Genet. 2019, 10, 1063. [Google Scholar] [CrossRef]
- Chabner, B.A.; Roberts, T.G. Chemotherapy and the war on cancer. Nat. Rev. Cancer 2005, 5, 65–72. [Google Scholar] [CrossRef]
- Blagosklonny, M.V. Prospective strategies to enforce selectively cell death in cancer cells. Oncogene 2004, 23, 2967–2975. [Google Scholar] [CrossRef][Green Version]
- Haber, D.A.; Gray, N.S.; Baselga, J. The evolving war on cancer. Cell 2011, 145, 19–24. [Google Scholar] [CrossRef]
- Folkman, J. Angiogenesis inhibitors: A new class of drugs. Cancer Biol. Ther. 2003, 2, 127–133. [Google Scholar] [CrossRef]
- Quail, D.F.; Joyce, J.A. Microenvironmental Regulation of Tumor Progression and Metastasis. Nat. Med. 2013, 19, 1423–1437. [Google Scholar] [CrossRef]
- Miao, L.; Huang, L. Exploring the tumour microenvironment with nanoparticles. Cancer Treat. Res. 2015, 166, 193–226. [Google Scholar] [PubMed]
- Hurley, L.H. DNA and its associated processes as targets for cancer therapy. Nat. Rev. Cancer 2002, 2, 188–200. [Google Scholar] [CrossRef] [PubMed]
- Kasi, P.M.; Thanarajasingam, G.; Finnes, H.D.; Villasboas Bisneto, J.C.; Hubbard, J.M.; Grothey, A. Chemotherapy in the setting of severe liver dysfunction in patients with metastatic colorectal cancer. Case Rep. Oncol. Med. 2015, 2015, 420159. [Google Scholar] [CrossRef] [PubMed]
- Albini, A.; Tosetti, F.; Li, V.W.; Noonan, D.M.; Li, W.W. Cancer prevention by targeting angiogenesis. Nat. Rev. Clin. Oncol. 2012, 9, 498–509. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.K. Normalization of tumour vasculature: An emerging concept in antiangiogenic therapy. Science 2005, 307, 58–62. [Google Scholar] [CrossRef]
- Hanahan, D.; Folkman, J. Patterns and emerging mechanisms of the angiogenic switch during tumourigenesis. Cell 1996, 86, 353–364. [Google Scholar] [CrossRef]
- Carmeliet, P.; Jain, R.K. Molecular mechanisms and clinical application of angiogenesis. Nature 2011, 473, 298–307. [Google Scholar] [CrossRef]
- Folkman, J. Tumour angiogenesis: Therapeutic implications. N. Engl. J. Med. 1971, 285, 1182–1186. [Google Scholar]
- Folkman, J. Angiogenesis-dependent diseases. Semin. Oncol. 1995, 28, 536–542. [Google Scholar] [CrossRef]
- Folkman, J. Angiogenesis in cancer, vascular, rheumatoid and other disease. Nat. Med. 1995, 1, 27–31. [Google Scholar] [CrossRef]
- Senger, D.R.; Van de Water, L.; Brown, L.F.; Nagy, J.A.; Yeo, K.T.; Yeo, T.K.; Berse, B.; Jackman, R.W.; Dvorak, A.M.; Dvorak, H.F. Vascular permeability factor (VPF, VEGF) in tumour biology. Cancer Metastasis Rev. 1993, 12, 303–324. [Google Scholar] [CrossRef] [PubMed]
- Dejana, E.; Tournier-Lasserve, E.; Weinstein, B.M. The control of vascular integrity by endothelial cell junctions: Molecular basis and pathological implication. Cell 2009, 16, 209–221. [Google Scholar] [CrossRef] [PubMed]
- Folkman, J. Fundamental concepts of the angiogenic process. Curr. Mol. Med. 2003, 3, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Folkman, J. Angiogenesis: An organizing principle for drug delivery? Nat. Rev. 2007, 6, 273–286. [Google Scholar]
- Motzer, R.J.; Escudier, B.; Gannon, A.; Figlin, R.A. Sunitinib: Ten years of successful clinical use and study in advanced renal cell carcinoma. Oncologist 2017, 22, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Rixe, O.; Oudard, S.; Negrier, S.; Szczylik, C.; Kim, S.T.; et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N. Engl. J. Med. 2007, 356, 115–124. [Google Scholar] [CrossRef]
- Huang, D.; Ding, Y.; Li, Y.; Luo, W.M.; Zhang, Z.F.; Snider, J.; Vandenbeldt, K.; Qian, C.N.; The, B.T. Sunitinib acts primarily on tumour endothelium rather than tumour cells to inhibit the growth of renal cell carcinoma. Cancer Res. 2010, 70, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Escudier, B.; Michaelson, M.D.; Motzer, R.J.; Hutson, T.E.; Clark, J.I.; Lim, H.Y.; Porfiri, E.; Zalewski, P.; Kannourakis, G.; Staehler, M.; et al. Axitinib versus sorafenib in advanced renal cell carcinoma: Subanalyses by prior therapy from a randomised phase III trial. Br. J. Cancer 2014, 110, 2821–2828. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.; Haworth, L.; Sherry, R.M.; Hwu, P.; Schwartzentruber, D.J.; Topalian, S.L.; Steinberg, S.M.; Chen, H.X.; Rosenberg, S.A. A randomized trial of bevacizumab, an anti-vascular endothelial growth factor antibody, for metastatic renal cancer. N. Engl. J. Med. 2003, 349, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Kartz, F.; Senter, P.; Steinhagam, H. Drug Delivery in Oncology; Wiley-VCH-Verlag & Co. KGaABoschstr: Weinheim, Germany, 2012; pp. 875–876. [Google Scholar]
- Mukherjee, A.; Madamsetty, V.S.; Paul, M.K.; Mukherjee, S. Recent advancements of nanomedicine towards antiangiogenic therapy in cancer. Int. J. Mol. Sci. 2020, 21, 455. [Google Scholar] [CrossRef] [PubMed]
- Teleanu, R.I.; Chircov, C.; Grumezescu, A.; Teleanu, D.M. Tumour Angiogenesis and Anti-Angiogenic Strategies for Cancer Treatment. J. Clin. Med. 2020, 9, 84. [Google Scholar] [CrossRef] [PubMed]
- Tacar, O.; Sriamornsak, P.; Dass, C.R. Doxorubicin: An update on anticancer molecular action, toxicity and novel drug delivery systems. J. Pharm. Pharmacol. 2013, 65, 157–170. [Google Scholar] [CrossRef] [PubMed]
- Fauzee, N.J. Taxanes: Promising Anti-Cancer Drugs. Asian Pacific J. Cancer Prev. 2011, 12, 837–851. [Google Scholar]
- Bignold, L.P. Alkylating agents and DNA polymerases. Anticancer Res. 2006, 26, 1322–1336. [Google Scholar]
- Dragony, F.; Jennifer, A.C.; Leona, D. Balancing repair and tolerance of DNA damage caused by alkylating agents. Nat. Rev. Cancer 2012, 12, 104–120. [Google Scholar]
- Minotti, G.; Menna, P.; Salvatorelli, E.; Cairo, G.; Gianni, L. Anthracyclines: Molecular advances and pharmacologic developments in antitumour activity and cardiotoxicity. Pharmacol. Rev. 2004, 6, 185–229. [Google Scholar] [CrossRef] [PubMed]
- Rowinsky, E.K. The development and clinical utility of the taxane class of antimicrotubule chemotherapy agents. Annu. Rev. Med. 1997, 48, 353–374. [Google Scholar] [CrossRef]
- Grenon, N.N. Managing toxicities associated with antiangiogenic biologic agents in combination with chemotherapy for metastatic colorectal cancer. Clin. J. Oncol. Nurs. 2013, 17, 425–433. [Google Scholar] [CrossRef]
- Peer, D.; Karp, J.M.; Hong, S.; Farokhzad, O.C.; Margalit, R.; Langer, R. Nanocarriers as an emerging platform for cancer therapy. Nat. Nanotechnol. 2007, 2, 751–760. [Google Scholar] [CrossRef]
- Farokhzad, O.C.; Langer, R. Impact of nanotechnology on drug delivery. ACS Nano 2009, 3, 16–20. [Google Scholar] [CrossRef]
- Duncan, R. Polymer conjugates as anticancer nanomedicines. Nat. Rev. Cancer 2006, 6, 688–701. [Google Scholar] [CrossRef] [PubMed]
- Duncan, R. Polymer therapeutics as nanomedicine: New perspectives. Curr. Opin. Biotechnol. 2011, 22, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Hamidi, M.; Azadi, A.; Rafiei, P.; Ashrafi, H. A pharmacokinetic overview of nanotechnology-based drug delivery systems: An ADME-oriented approach. Crit. Rev. Ther. Drug Carr. Syst. 2013, 30, 435–467. [Google Scholar] [CrossRef] [PubMed]
- Zaro, J.L. Lipid-based drug carriers for prodrugs to enhance drug delivery. AAPS J. 2015, 17, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, Y.; Maeda, H. A new concept for macromolecular therapeutics in cancer chemotherapy: Mechanism of tumouritropic accumulation of proteins and the antitumour agent smancs. Cancer Res. 1986, 46, 6387–6392. [Google Scholar] [PubMed]
- Maeda, H. Toward a full understanding of the EPR effect in primary and metastatic tumours as well as issues related to its heterogeneity. Adv. Drug Deliv. Rev. 2015, 91, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Duncan, R.; Sat-Klopsch, Y.N.; Burger, A.M.; Bibby, M.C.; Fiebig, H.H.; Sausville, E.A. Validation of tumour models for use in anticancer nanomedicine evaluation: The EPR effect and cathepsin B-mediated drug release rate. Cancer Chemother. Pharmacol. 2013, 72, 417–427. [Google Scholar] [CrossRef]
- Duncan, R.; Gaspar, R. Nanomedicine(s) under the microscope. Mol. Pharm. 2011, 8, 2101–2141. [Google Scholar] [CrossRef]
- Tibbitt, M.W.; Dahlman, J.E.; Langer, R. Emerging frontiers in drug delivery. J. Am. Chem. Soc. 2016, 138, 704–717. [Google Scholar] [CrossRef]
- Min, Y.; Caster, J.M.; Eblan, M.J.; Wang, A.Z. Clinical translation of nanomedicine. Chem. Rev. 2015, 115, 11147–11190. [Google Scholar] [CrossRef]
- Barenholz, Y. Doxil®-the first FDA-approved nanodrug: Lessons learned. J. Control. Release 2012, 160, 117–134. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration ABRAXANE® (Paclitaxel Protein-Bound Particles) for Injection Suspension. Available online: https://search.usa.gov/search?utf8=✓&affiliate=fda1&sort_by=&query=Abraxane® (accessed on 4 April 2020).
- Food and Drug Administration DaunoXome® (Daunorubicin Citrate Liposome Injection). Available online: https://search.usa.gov/search?utf8=✓&affiliate=fda1&sort_by=&query=DaunoXome®%29+ (accessed on 4 April 2020).
- Ma, P.; Mumper, R.J. Paclitaxel nanodelivery systems: A comprehensive review. J. Nanomed. Nanotechnol. 2013, 4, 1000164. [Google Scholar] [CrossRef] [PubMed]
- Albain, K.S.; Belani, C.P.; Bonomi, P.; O’Byrne, K.J.; Schiller, J.H.; Socinski, M. PIONEER: A phase III randomized trial of paclitaxel poliglumex versus paclitaxel in chemotherapy-naive women with advanced-stage non-small-cell lung cancer and performance status of 2. Clin. Lung Cancer 2006, 7, 417–419. [Google Scholar] [CrossRef] [PubMed]
- Langer, C.J.; O’Byrne, K.J.; Socinski, M.A.; Mikhailov, S.M.; Leśniewski-Kmak, K.; Smakal, M.; Ciuleanu, T.E.; Orlov, S.V.; Dediu, M.; Heigener, D.; et al. Phase III trial comparing paclitaxel poliglumex (CT-2103, PPX) in combination with carboplatin versus standard paclitaxel and carboplatin in the treatment of PS 2 patients with chemotherapy-naïve advanced non-small cell lung cancer. J. Thorac. Oncol. 2008, 3, 623–630. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.E.; Socinski, M.A.; Popovich, A.Y.; Bondarenko, I.N.; Tomova, A.; Bilynsky, B.T.; Hotko, Y.S.; Ganul, V.L.; Kostinsky, I.Y.; Eisenfeld, A.J.; et al. Randomized phase III trial comparing single-agent paclitaxel poliglumex (CT-2103, PPX) with single-agent gemcitabine or vinorelbine for the treatment of PS 2 patients with chemotherapy-naive advanced non-small cell lung cancer. J. Thorac. Oncol. 2008, 3, 728–734. [Google Scholar] [CrossRef]
- Jabr-Milane, L.S.; van Vlerken, L.E.; Yadav, S.; Amiji, M.M. Multi-functional nanocarriers to overcome tumour drug resistance. Cancer Treat. Rev. 2008, 34, 592–602. [Google Scholar] [CrossRef]
- Pacardo, D.B.; Ligler, F.S.; Gu, Z. Programmable nanomedicine: Synergistic and sequential drug delivery systems. Nanoscale 2015, 7, 3381–3391. [Google Scholar] [CrossRef]
- Mayer, L.D.; Janoff, A.S. Optimizing combination chemotherapy by controlling drug ratios. Mol. Interv. 2007, 7, 216. [Google Scholar] [CrossRef]
- Jia, J.; Zhu, F.; Ma, X.; Cao, Z.W.; Li, Y.X.; Chen, Y.Z. Mechanisms of drug combinations: Interaction and network perspectives. Nat. Rev. Drug Discov. 2009, 8, 111–128. [Google Scholar] [CrossRef]
- Xu, X.; Ho, W.; Zhang, X.; Bertrand, N.; Farokhzad, O. Cancer nanomedicine: From targeted delivery to combination therapy. Trends Mol. Med. 2015, 21, 223–232. [Google Scholar] [CrossRef]
- Greco, F.; Vicent, M.J. Combination therapy: Opportunities and challenges for polymer–drug conjugates as anticancer nanomedicines. Adv. Drug Deliv. Rev. 2009, 61, 1203–1213. [Google Scholar] [CrossRef] [PubMed]
- Miao, L.; Guo, S.; Lin, C.M.; Liu, Q.; Huang, L. Nanoformulations for combination or cascade anticancer therapy. Adv. Drug Deliv. Rev. 2017, 115, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Shim, G.; Kim, M.G.; Kim, D.; Park, J.Y.; Oh, Y.K. Nanoformulation-based sequential combination cancer therapy. Adv. Drug Deliv. Rev. 2017, 115, 57–81. [Google Scholar] [CrossRef]
- Hu, Q.; Sun, W.; Wang, C.; Gu, Z. Recent advances of cocktail chemotherapy by combination drug delivery systems. Adv. Drug Deliv. Rev. 2016, 98, 19–34. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.X.; Wong, H.L.; Xue, H.Y.; Eoh, J.Y.; Wu, X.Y. Nanomedicine of synergistic drug combinations for cancer therapy-strategies and perspectives. J. Control. Release 2016, 240, 489–503. [Google Scholar] [CrossRef] [PubMed]
- Feldman, E.J.; Lancet, J.E.; Kolitz, J.E.; Ritchie, E.K.; Roboz, G.J.; List, A.F.; Allen, S.L.; Asatiani, E.; Mayer, L.D.; Swenson, C.; et al. First-in-man study of CPX-351: A liposomal carrier containing cytarabine and daunorubicin in a fixed 5:1 molar ratio for the treatment of relapsed and refractory acute myeloid leukemia. J. Clin. Oncol. 2011, 29, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Aryal, S.; Hu, C.-M.J.; Zhang, L. Polymeric nanoparticles with precise ratiometric control over drug loading for combination therapy. Mol. Pharm. 2011, 8, 1401–1407. [Google Scholar] [CrossRef]
- Bell, A. Antimalarial drug synergism and antagonism: Mechanistic and clinical significance. FEMS Microbiol. Lett. 2005, 253, 171–184. [Google Scholar] [CrossRef]
- Chou, T.C. Theoretical basis, experimental design, and computerized simulation of synergism and antagonism in drug combination studies. Pharmacol. Rev. 2006, 58, 621–681. [Google Scholar] [CrossRef]
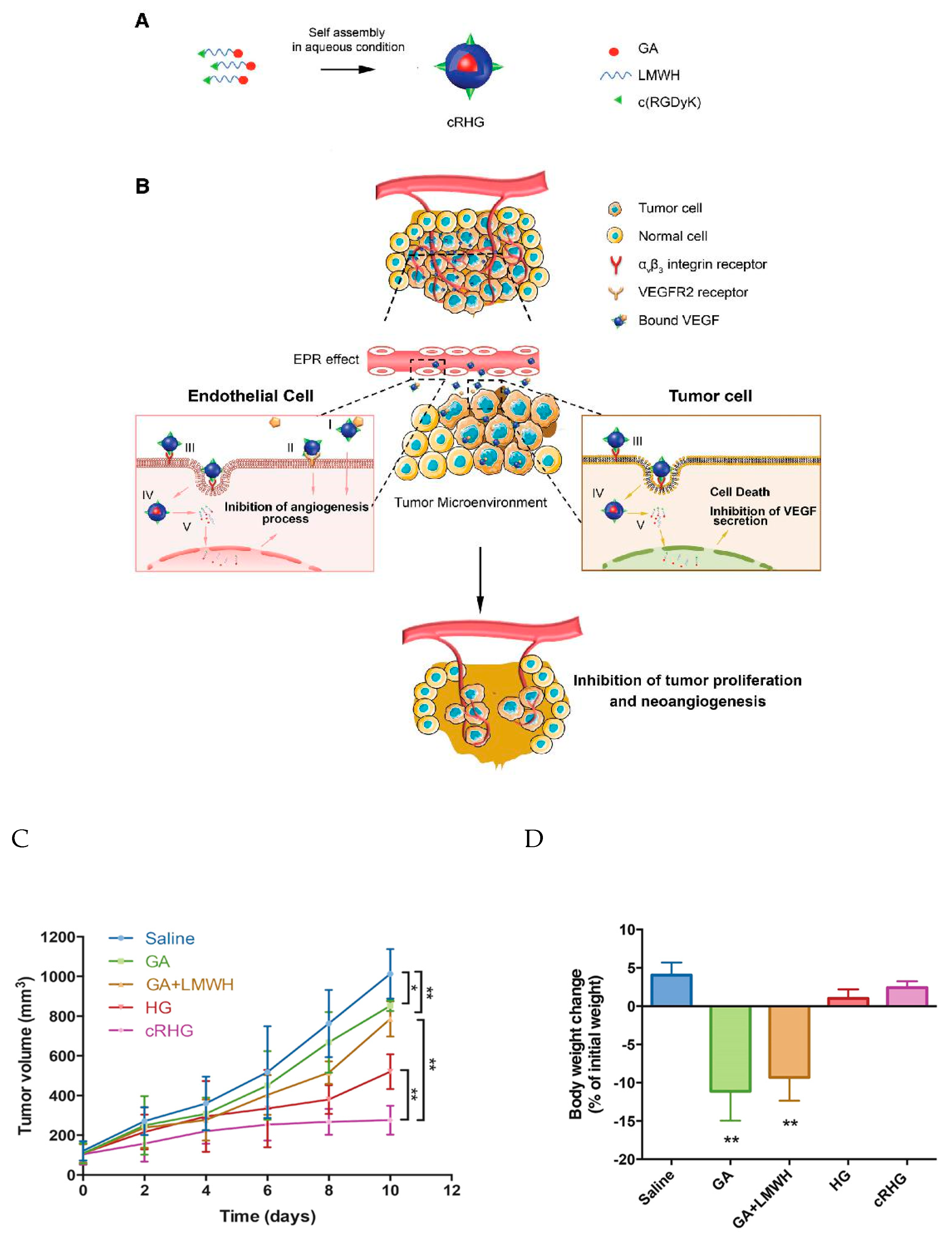
- Chou, T.C. Drug combination studies and their synergy quantification using the Chou-Talalay method. Cancer Res. 2010, 70, 440–446. [Google Scholar] [CrossRef]
- Pinto, A.C.; Oreira, N.J.; Simoes, S. Combination Chemotherapy in Cancer: Principles, Evaluation and Drug Delivery Strategies. In Current Cancer Treatment, Current Cancer Treatment; InTechopen: London, UK, 2011; pp. 693–711. [Google Scholar]
- Food and Drug AdministrationCPX-351 (Cytrabine; Daunorubicin) Liposome Injection. Available online: https://search.usa.gov/search?utf8=✓&affiliate=fda1&sort_by=&query=CPX-351%2C+or+Vyxeos (accessed on 4 April 2020).
- Mayer, L.D.; Tardi, P.; Louie, A.C. CPX-351: A nanoscale liposomal co-formulation of daunorubicin and cytarabine with unique biodistribution and tumour cell uptake properties. Int. J. Nanomed. 2019, 14, 3819–3830. [Google Scholar] [CrossRef] [PubMed]
- Lancet, J.E.; Uy, G.L.; Cortes, J.E.; Newell, L.F.; Lin, T.L.; Ritchie, E.K.; Stuart, R.K.; Strickland, S.A.; Hogge, D.; Solomon, S.R.; et al. CPX-351 (cytarabine and daunorubicin) Liposome for Injection Versus Conventional Cytarabine Plus Daunorubicin in Older Patients With Newly Diagnosed Secondary Acute Myeloid Leukemia. J. Clin. Oncol. 2018, 36, 2684–2692. [Google Scholar] [CrossRef] [PubMed]
- Batist, G.; Sawyer, M.; Gabrail, N.; Christiansen, N.; Marshall, J.L.; Spigel, D.R.; Louie, A. Multicenter, phase II study of CPX-1 liposome injection in patients (pts) with advanced colorectal cancer (CRC). J. Clin. Oncol. 2015, 26, 4108. [Google Scholar] [CrossRef]
- Zhang, J.; Li, J.; Shi, Z.; Yang, Y.; Xie, X.; Lee, S.M.; Wang, Y.; Leong, K.W.; Chen, M. pH-sensitive polymeric nanoparticles for co-delivery of doxorubicin and curcumin to treat cancer via enhanced pro-apoptotic and anti- angiogenic activities. Acta Biomater. 2017, 58, 349–364. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.; Wang, Y.; He, X.; Zhang, Z.; Yin, Q.; Chen, Y.; Yu, H.; Huang, Y.; Chen, L.; Xu, M.; et al. Codelivery of sorafenib and curcumin by directed self-assembled nanoparticles enhances therapeutic effect on hepatocellular carcinoma. Mol. Pharm. 2015, 12, 922–931. [Google Scholar] [CrossRef] [PubMed]
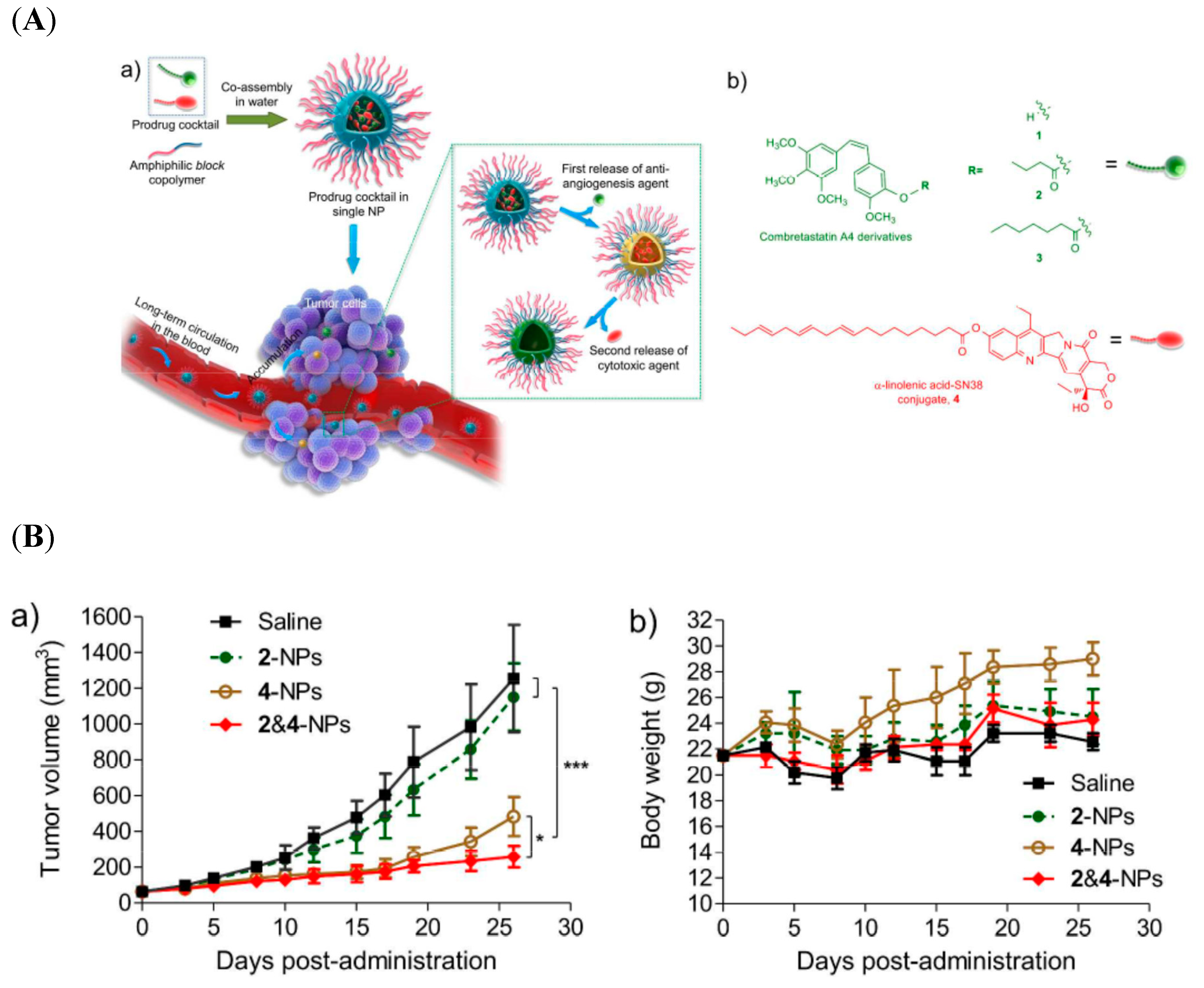
- Wang, H.; Wu, J.; Xie, K.; Fang, T.; Chen, C.; Xie, H.; Zhou, L.; Zheng, S. Precise engineering of prodrug cocktails into single polymeric nanoparticles for combinationcancer therapy: Extended and sequentially controllable drug release. ACS Appl. Mater. Interfaces 2017, 9, 10567–10576. [Google Scholar] [CrossRef]
- Yang, W.J.; Zhou, P.; Liang, L.; Cao, Y.; Qiao, J.; Li, X.; Teng, Z.; Wang, L. Nanogel-incorporated injectable hydrogel for synergistic therapy based on sequential local delivery of combretastatin-A4 phosphate (CA4P) and doxorubicin (DOX). ACS Appl. Mater. Interfaces 2018, 10, 18560–18573. [Google Scholar] [CrossRef]
- Aboubakr, E.M.; Taye, A.; Aly, O.M.; Gamal-Eldeen, A.M.; El-Moselhy, M.A. Combretastatin A4-camptothecin micelles as combination therapy for effective anticancer activity. Biomed. Pharmacother. 2017, 89, 36–46. [Google Scholar] [CrossRef]
- Dahmani, F.Z.; Xiao, Y.; Zhang, J.; Yu, Y.; Zhou, J.; Yao, J. Multifunctional polymeric nanosystems for dual-targeted combinatorial chemo/antiangiogenesis therapy of tumours. Adv. Healthc. Mater. 2016, 5, 1447–1461. [Google Scholar] [CrossRef]
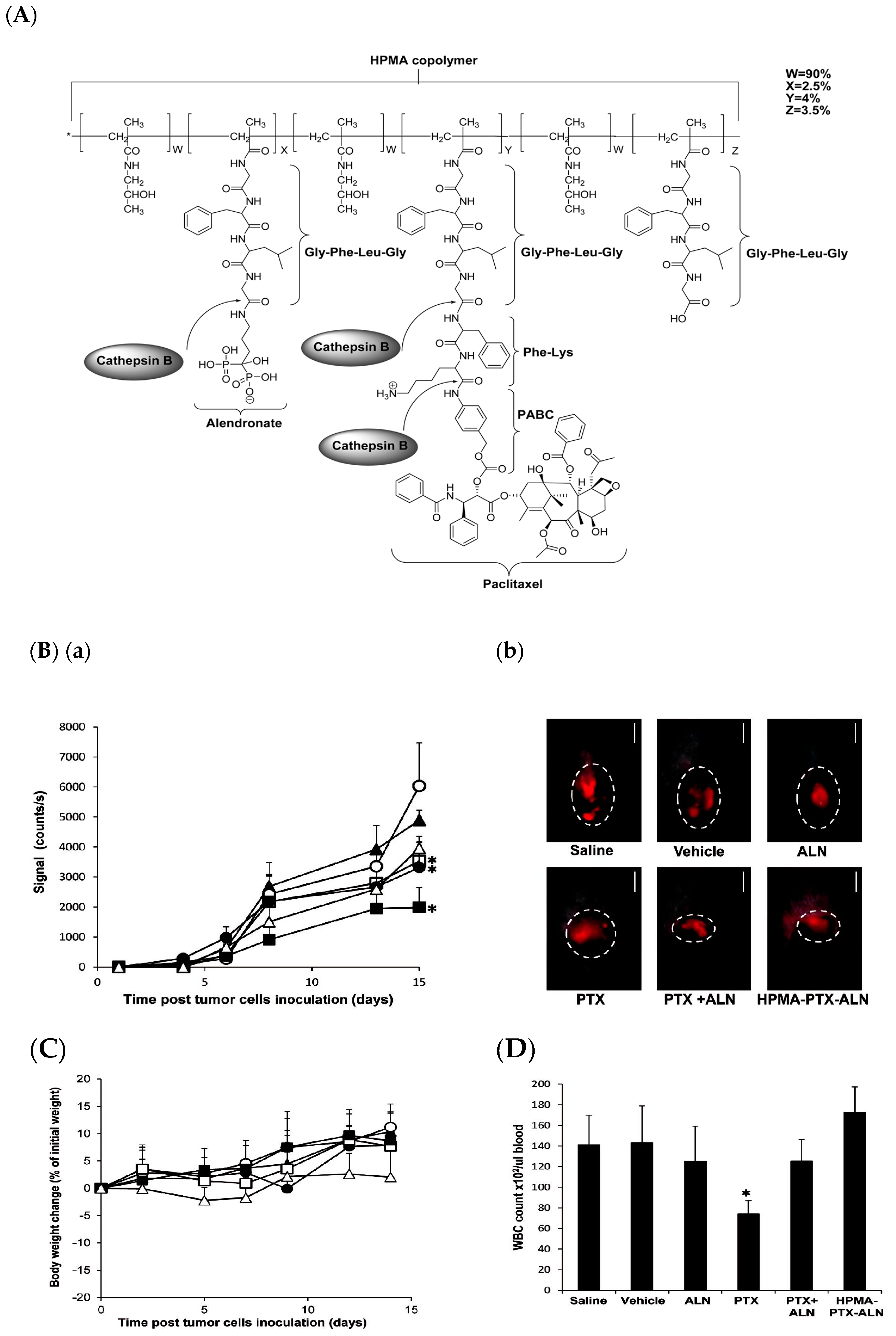
- Miller, K.; Eldar-Boock, A.; Polyak, D.; Segal, E.; Benayoun, L.; Shaked, Y.; Satchi-Fainaro, R. Antiangiogenic antitumour activity of HPMA copolymer-paclitaxel alendronate conjugate on breastcancer bone metastasis mouse model. Mol. Pharm. 2011, 8, 1052–1062. [Google Scholar] [CrossRef]
- Rao, D.A.; Mishra, G.; Doddapaneni, B.S.; Kyryachenko, S.; Wierzbicki, I.H.; Nguyen, D.X.; Shah, V.; Fatease Adel, M.A.; Alany, R.; Adam, W.G. Alani combinatorial polymeric conjugated micelles with dual cytotoxic and antiangiogenic effects for the treatment of ovarian cancer. Chem. Mater. 2016, 28, 6068–6079. [Google Scholar] [CrossRef]
- Wang, Y.; Yang, T.; Wang, X.; Dai, W.; Wang, J.; Zhang, X.; Li, Z.; Zhang, Q. Materializing sequential killing of tumour vasculature and tumour cells via targeted polymeric micelle system. J. Control. Release 2011, 149, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, S.; Eavarone, D.; Capila, I.; Zhao, G.; Watson, N.; Kiziltepe, T.; Sasisekharan, R. Temporal targeting of tumour cells and neovasculature with a nanoscale delivery system. Nature 2005, 436, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.; Jin, W.; Zhang, J.; Wang, X.; Wang, J.; Zhang, X.; Wan, Y.; Zhang, Q. Spatiotemporally controlled co-delivery of anti-vasculature agent and cytotoxic drug by octreotide-modified stealth liposomes. Pharm. Res. 2012, 29, 2902–2911. [Google Scholar] [CrossRef]
- Zhang, Y.F.; Wang, J.C.; Bian, D.Y.; Zhang, X.; Zhang, Q. Targeted delivery of RGD-modified liposomes encapsulating both combretastatin A-4 and doxorubicin for tumour therapy: In vitro and in vivo studies. Eur. J. Pharm. Biopharm. 2010, 74, 467–473. [Google Scholar] [CrossRef]
- Chen, S.; Liang, Q.; Liu, E.; Yu, Z.; Sun, L.; Ye, J.; Shin, M.C.; Wang, J.; He, H. Curcumin/sunitinib co-loaded BSA-stabilized SPIOs for synergistic combination therapy for breast cancer. J. Mater. Chem. B 2017, 5, 4060–4072. [Google Scholar] [CrossRef]
- Li, X.; Wu, M.; Pan, L.; Shi, J. Tumour vascular-targeted co-delivery of anti-angiogenesis and chemotherapeutic agents by mesoporous silica nanoparticlebased drug delivery system for synergetic therapy of tumour. Int. J. Nanomed. 2015, 11, 93–105. [Google Scholar] [CrossRef]
- You, Y.H.; Lin, Y.F.; Nirosha, B.; Chang, H.T.; Huang, Y.F. Polydopamine-coated gold nanostar for combined antitumour and antiangiogenic therapy in multidrug-resistant breast cancer. Nanotheranostics 2019, 3, 266–283. [Google Scholar] [CrossRef]
- Zagorodko, O.; Arroyo-Crespo, J.J.; Nebot, V.J.; Vicent, M.J. Polypeptide-Based Conjugates as Therapeutics: Opportunities and Challenges. Macromol. Biosci. 2017, 17, 1600316. [Google Scholar] [CrossRef]
- Ekladious, I.; Colson, Y.L.; Grinstaff, M.W. Polymer-drug Conjugate Therapeutics: Advances, Insights and Prospects. Nat. Rev. Drug Discov. 2019, 18, 273–294. [Google Scholar] [CrossRef]
- Markovsky, E.; Baabur-Cohen, H.; Eldar-Boock, A.; Omer, L.; Tiram, G.; Ferber, S.; Ofek, P.; Polyak, D.; Scomparin, A.; Satchi-Fainaro, R. Administration, distribution, metabolism and elimination of polymer therapeutics. J. Control. Release 2012, 16, 446–460. [Google Scholar] [CrossRef] [PubMed]
- Bauer, W.; Briner, U.; Doepfner, W.; Haller, R.; Huguenin, R.; Marbach, P.; Petcher, T.J.; Pless, J. SMS 201-995: A very potent and selective octapeptide analogue of somatostatin with prolonged action. Life Sci. 1982, 31, 1133–1140. [Google Scholar] [CrossRef]
- Reubi, J.C.; Kvols, L.; Krenning, E.; Lamberts, S.W. Distribution of somatotatin receptors in normal and tumour tissue. Metabolism 1990, 39, 78–81. [Google Scholar] [CrossRef]
- Volante, M.; Rosas, R.; Allia, E.; Granata, R.; Baragli, A.; Muccioli, G.; Papotti, M. Somatostatin, cortistatin and their receptors in tumours. Mol. Cell Endocrinol. 2008, 286, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Ehmann, F.; Sakai-Kato, K.; Duncan, R.; Hernán Pérez de la Ossa, D.; Pita, R.; Vidal, J.M.; Kohli, A.; Tothfalusi, L.; Sanh, A.; Tinton, S.; et al. Next-generation Nanomedicines and Nanosimilars: EU Regulators’ Initiatives Relating to the Development and Evaluation of Nanomedicines. Nanomedicine (Lond.) 2013, 8, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Attia, M.F.; Anton, N.; Wallyn, J.; Omran, Z.; Vandamme, T.F. An Overview of Active and Passive Targeting Strategies to Improve the Nanocarriers Efficiency to Tumour Sites. J. Pharm. Pharmacol. 2019, 71, 1185–1198. [Google Scholar] [CrossRef] [PubMed]
- Farjadian, F.; Ghasemi, A.; Gohari, O.; Roointan, A.; Karimi, M.; Hamblin, M.R. Nanopharmaceuticals and Nanomedicines Currently on the Market: Challenges and Opportunities. Nanomedicine (Lond.) 2019, 4, 93–126. [Google Scholar] [CrossRef] [PubMed]
- Duncan, R.; Vicent, M.J. Polymer Therapeutics-Prospects for 21st Century: The End of the Beginning. Adv. Drug Deliv. Rev. 2013, 65, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Duncan, R. Polymer Therapeutics at a Crossroads? Finding the Path for Improved Translation in the Twenty-First Century. J. Drug Target. 2017, 25, 759–780. [Google Scholar] [CrossRef]
- Ono, M. Molecular links between tumor angiogenesis and inflammation: Inflammatory stimuli of macrophages and cancer cells as targets for therapeutic strategy. Cancer Sci. 2008, 99, 1501–1506. [Google Scholar] [CrossRef]
- Zappavigna, S.; Cossu, A.M.; Grimaldi, A.; Bocchetti, M.; Ferraro, G.A.; Nicoletti, G.F.; Filosa, R.; Caraglia, M. Anti-Inflammatory Drugs as Anticancer Agents. Int. J. Mol. Sci. 2020, 21, 2605. [Google Scholar] [CrossRef] [PubMed]
- Pa, L.S.; Medatwal, N.; Kumar, S.; Kar, A.; Komalla, V.; Yavvari, P.S.; Mishra, D.; Rizvi, Z.A.; Nandan, S.; Malakar, D.; et al. A Localized Chimeric Hydrogel Therapy Combats Tumor Progression through Alteration of Sphingolipid Metabolism. ACS Cent. Sci. 2019, 5, 1648–1662. [Google Scholar]
- Ogbomo, S.M.; Shi, W.; Wagh, N.K.; Zhou, Z.; Brusnahan, S.K.; Garrison, J.C. 177Lu-labeled HPMA copolymers utilizing cathepsin B and S cleavable linkers: Synthesis, characterization and preliminary in vivo investigation in a pancreatic cancer model. Nucl. Med. Biol. 2013, 40, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J. Review of Therapeutic Applications of Radiolabeled Functional Nanomaterials. Int. J. Mol. Sci. 2019, 20, 2323. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Vugts, D.J.; Visser, G.W.; Stigtervan, W.M.; Bolijn, M.; Spiga, M.; Lazzari, P.; Shankar, S.; Sani, M.; Zanda, M.; et al. Development of Novel ADCs: Conjugation of Tubulysin Analogues to Trastuzumab Monitored by Dual Radiolabeling. Cancer Res. 2014, 74, 5700–5710. [Google Scholar] [CrossRef]
- Ni, D.; Jiang, D.; Ehlerding, E.B.; Huang, P.; Cai, W. Radiolabeling Silica-Based Nanoparticles via Coordination Chemistry: Basic Principles, Strategies, and Applications. Acc. Chem. Res. 2018, 51, 778–788. [Google Scholar] [CrossRef] [PubMed]
- Amreddy, N.; Babu, A.; Muralidharan, R.; Panneerselvam, J.; Srivastava, A.; Ahmed, R.; Mehta, M.; Munshi, A.; Ramesh, R. Recent Advances in Nanoparticle-Based Cancer Drug and Gene Delivery. Adv. Cancer Res. 2018, 137, 115–170. [Google Scholar]
- Zhang, L.; Zhang, R.; Yang, J.; Wang, J.; Kopeček, J. Indium-based and iodine-based labeling of HPMA copolymer–epirubicin conjugates: Impact of structure on the in vivo fate. J. Control. Release 2016, 235, 306–318. [Google Scholar] [CrossRef]
- Park, J.; Park, J.; Ju, E.J.; Park, S.S.; Choi, J.; Lee, J.H.; Lee, K.J.; Shin, S.H.; Ko, E.J.; Park, I.; et al. Multifunctional hollow gold nanoparticles designed for triple combination therapy and CT imaging. J. Control. Release 2015, 207, 77–85. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Nanoformulations | Nanocarrier Materials | Combination Drugs | Encapsulation Method | Cancer Types (In Vivo) | Outcome | Ref |
|---|---|---|---|---|---|---|
| Polymer based | ||||||
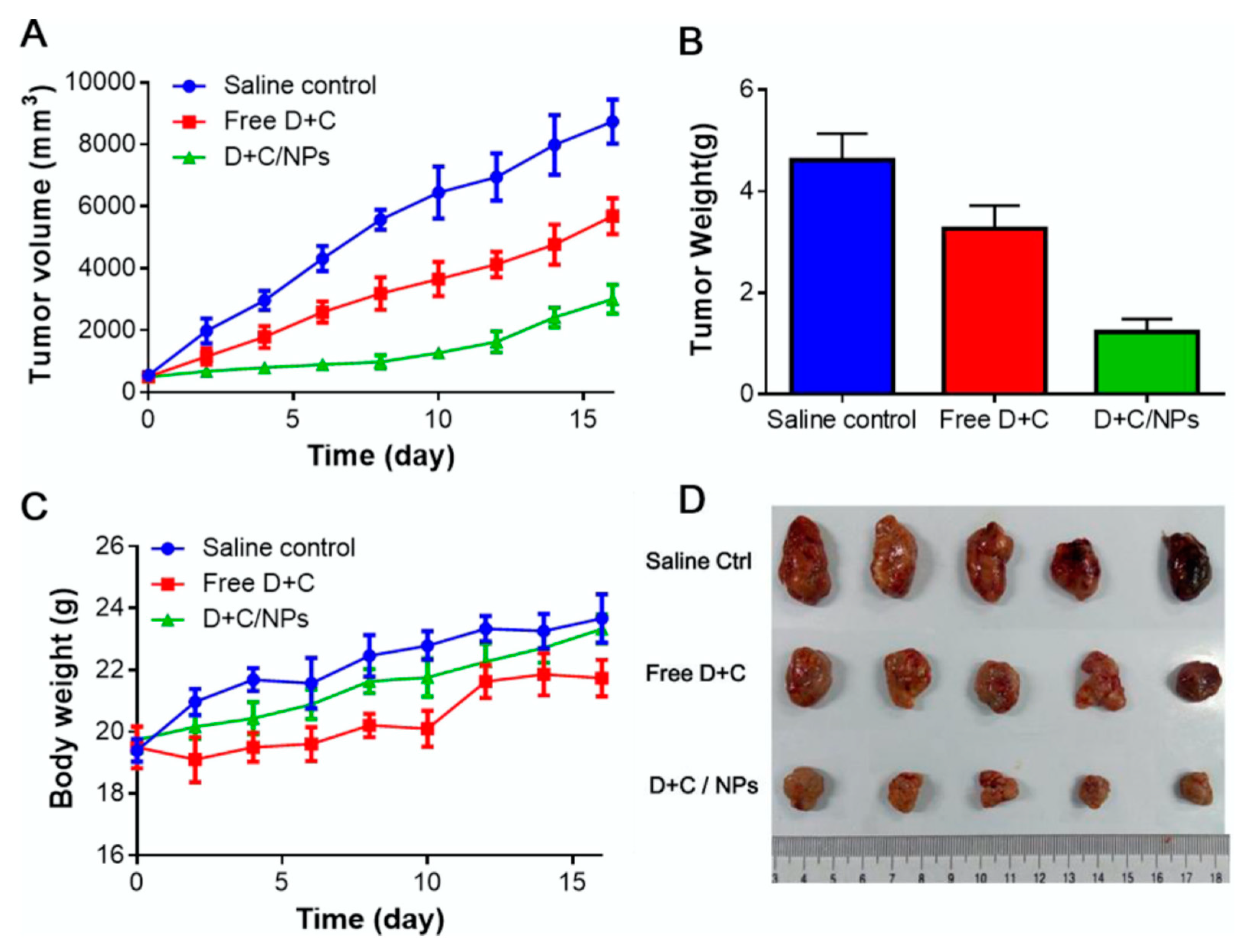
| Polymeric nanoparticles | D-a-tocopheryl poly-ethylene glycol 1000-block-poly(b-amino ester) polymers | Doxorubicin and Curcumin | Physical encapsulation + Physical encapsulation | Hepatocellular carcinoma (human tumour xenograft model) | pH-sensitive nano-carrier enhanced the synergistic effect of simultaneous delivery of Dox and Cur | [80] |
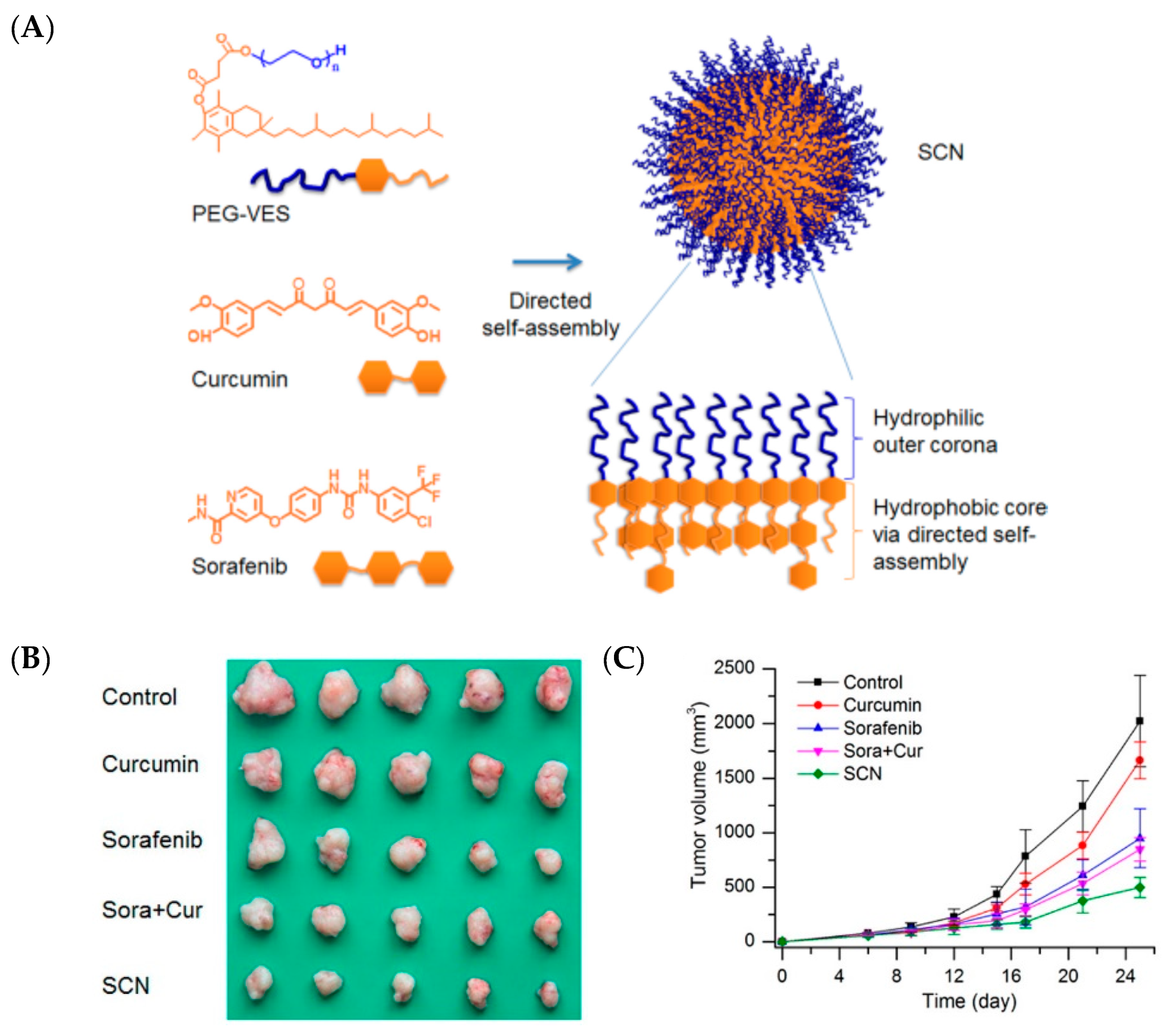
| Polymer-self-assembled nanoparticles | Polyethylene glycol-vitamin E succinate | Curcumin and Sorafenib | Intermolecular hydrophobic interactions | Hepatocellular carcinoma (human tumour xenograft model) | Co-assembled nanoparticles provided higher therapeutic efficacy against tumor progression compared with free drug monotherapy or their free combination | [81] |
| Polymeric nanoparticles | Methoxypoly (ethylene glycol)-block-poly(d,l-lactide) copolymer and poly(acrylic acid-co-4-vubylphenylbornonic acid | 7-ethyl-10-hydroxycamptothecin (SN38) and Combretastatin-A4 | Chemical conjugation + Chemical conjugation | Colon cancer (human tumour tumors model) | Synergistic antiproliferative and antiangiogenic effects observed | [82] |
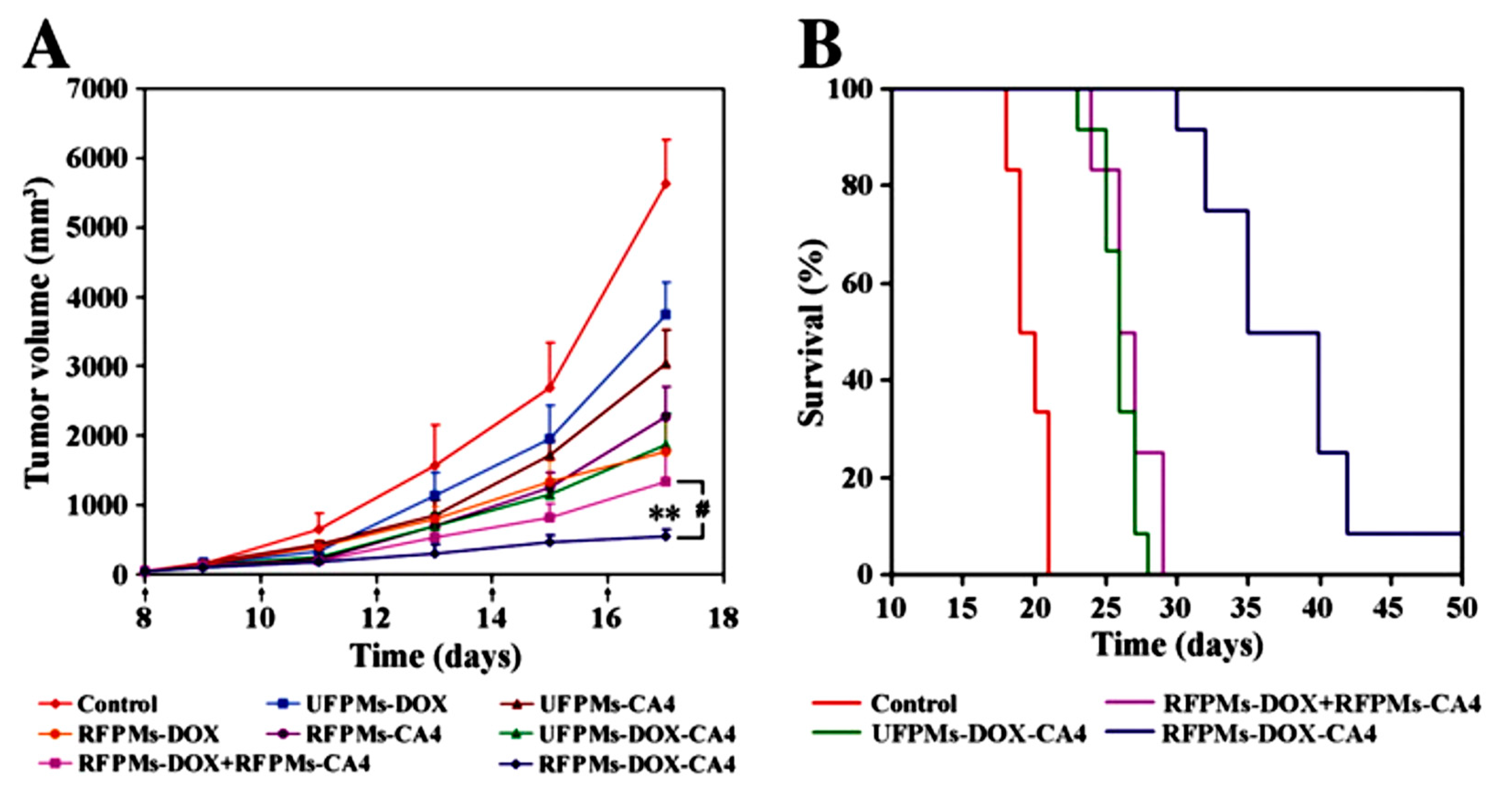
| Hydrogel | Poly(N-(3,4- dihydroxyphenethyl) methacrylamide-co-polyethylene glycol methyl ether methacrylate | Doxorubicin and Combretastatin-A4 Phosphate | Electrostatic + Physical encapsulation | Hepatocellular carcinoma (HepG2 xenograft model) | Sequential local delivery with superior in vivo efficacy observed | [83] |
| Micelle | Polyethylene glycol | Camptothecin and Combretastatin A4 | Chemical conjugation + Chemical conjugation | - | Enhanced anticancer activity with a strong synergistic effect | [84] |
| Polymeric-self- assemble nanoparticles | Cyclo Arg-Gly-Asp-d-Tyr-Lys and low molecular weight heparin | Gambogic acid and cyclo (Arg-Gly-Asp-D-Tyr-Lys) peptide | Chemical conjugation | Glioblastoma (tumour xenograft model) | Efficiently inhibited the tumor growth in xenograft model with a reduced side-toxicity | [85] |
| Polymer-drug conjugate | N-(2-hydroxypropyl)meth acrylamide copolymer | Paclitaxel and Alendronate | Chemical conjugation + Chemical conjugation | Breast Cancer Bone Metastasis (4T-mCherry adenocarcinoma model) | Improved antitumor and antiangiogenic activity observed | [86] |
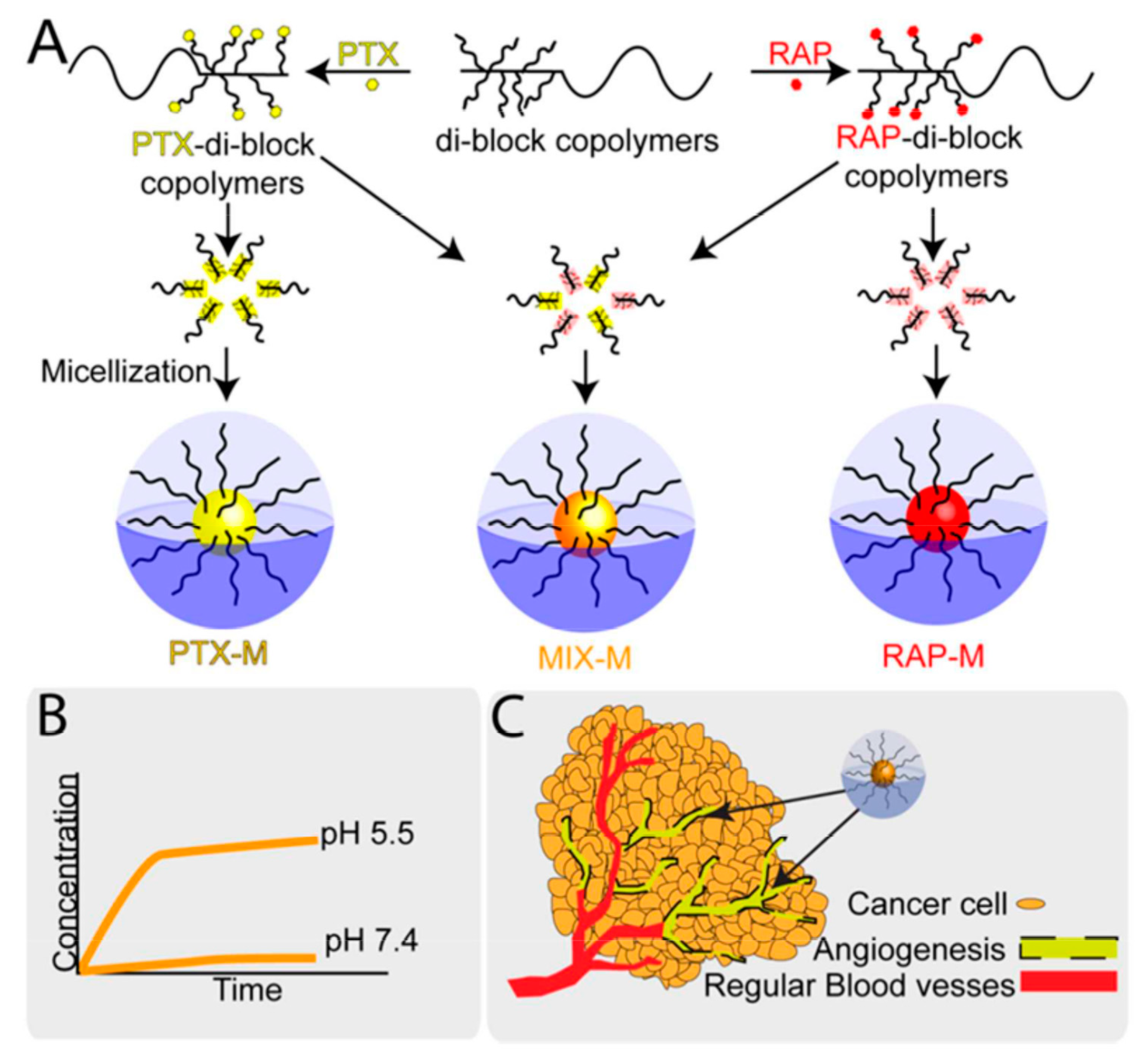
| Micelle | α-Aminopropyl-ω-methoxy-poly(ethylene glycol) and β-benzyl-l-aspartate N-carboxyanhydride | Paclitaxel and Rapamycin | Chemical conjugation + Chemical conjugation | Ovarian Cancer (ES2 murine xenograft model) | Synergistic apoptotic and antiangiogenic effects observed | [87] |
| Micelle | Poly(ethylene glycol)-b-poly(d,l-lactide) | Doxorubicin and Combretastatin-A4 | Physical encapsulation + Physical encapsulation | Skin and lung cancer (B16-F10 tumor-bearing mice) | Exhibited stronger tumor growth inhibition and greater survival rate compared with the other treatment groups | [88] |
| Lipid based | ||||||
| Nanocell | Poly(lactic-co-glycolic acid)copolymer | Doxorubicin and Combretastatin-A4 | Chemical conjugation + Physical encapsulation | Skin and lung cancer (B16/F10 melanoma and Lewis lung carcinoma | Improved therapeutic index with reduced toxicity | [89] |
| Liposome | Egg phosphatidylcholine + 1,2-distearoyl-sn-glycero-3-phosphoethanolamine-N-[ amino(polyethylene glycol) +Cholesterol | Doxorubicin and Combretastatin-A4 | Physical encapsulation + Physical encapsulation | Breast cancer (tumor bearing xenografts model) | Programmed in vitro drug release observed with sequential in vivo Cytotoxic effects of these two drugs | [90] |
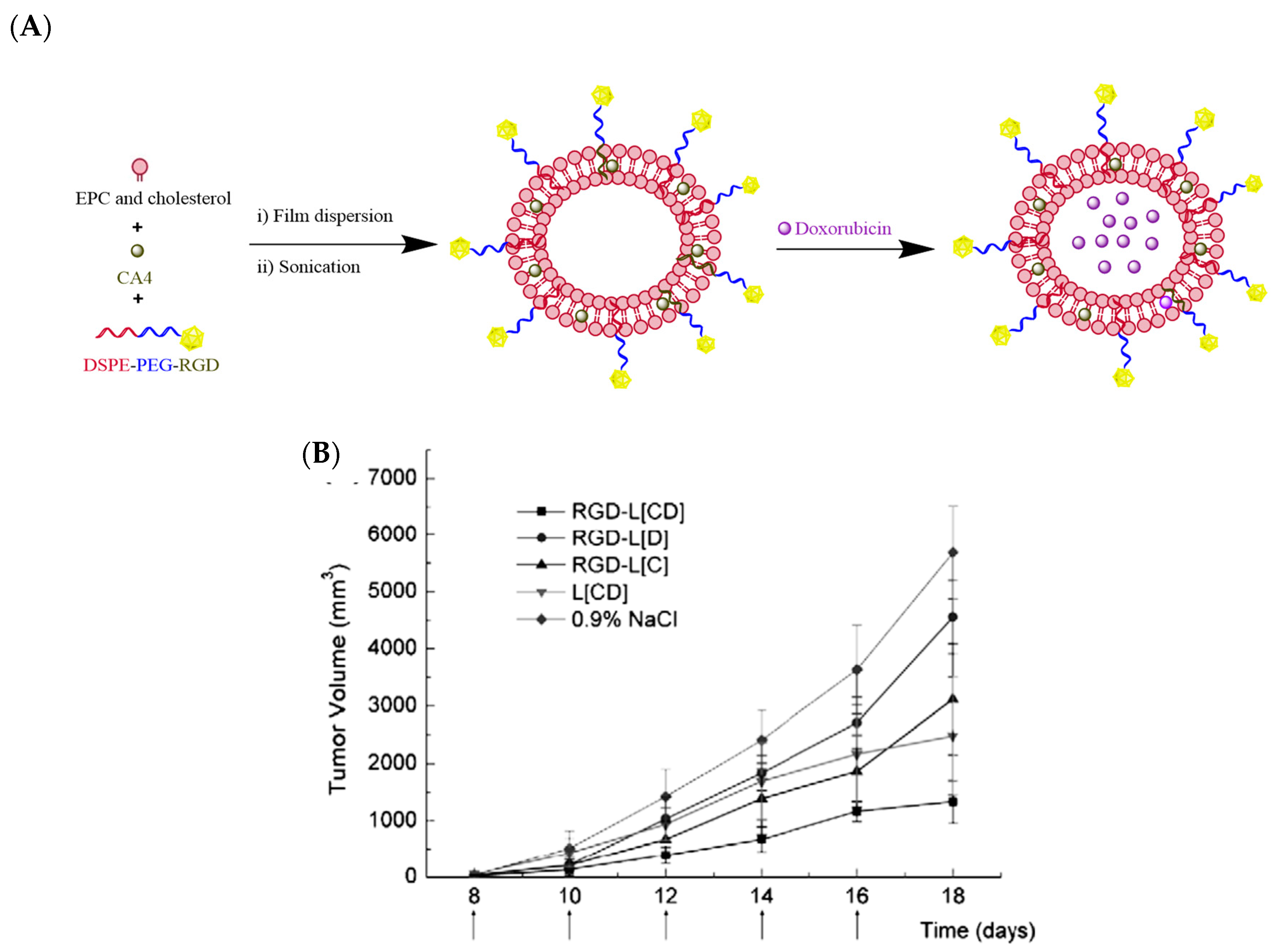
| Liposome | Egg phosphatidylcholine + 1,2-distearoyl-sn-glycero-3-phosphoethanolamine N-[ amino(polyethylene glycol)] + Cholesterol + arginine-glycine-aspartic acid | Doxorubicin and Combretastatin-A4 | Physical encapsulation + Physical encapsulation | B16F10 melanoma (C57BL/6 xenografts model) | Synergistic effect of the combined therapeutics with the increased anti-tumor response observed | [91] |
| Inorganic based | ||||||
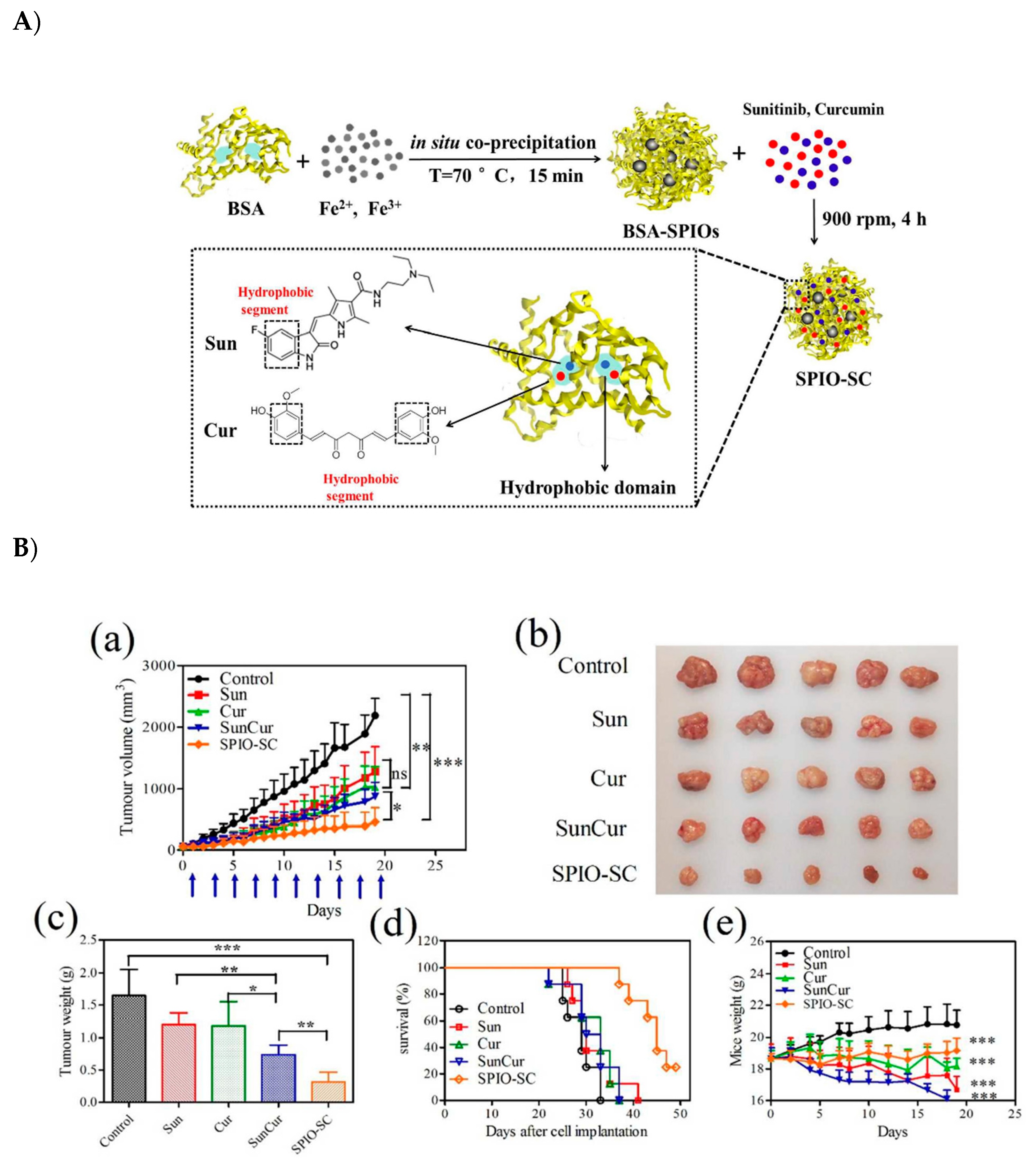
| Super magnetic iron oxide nanoparticles | Super magnetic iron oxide and albumin/bovine serum albumin | Curcumin and Sunitinib | Physical encapsulation + Physical encapsulation | Breast cancer (MCF-7 xenograft mouse model) | Observed significant tumor inhibition with a reduced systemic toxicity | [92] |
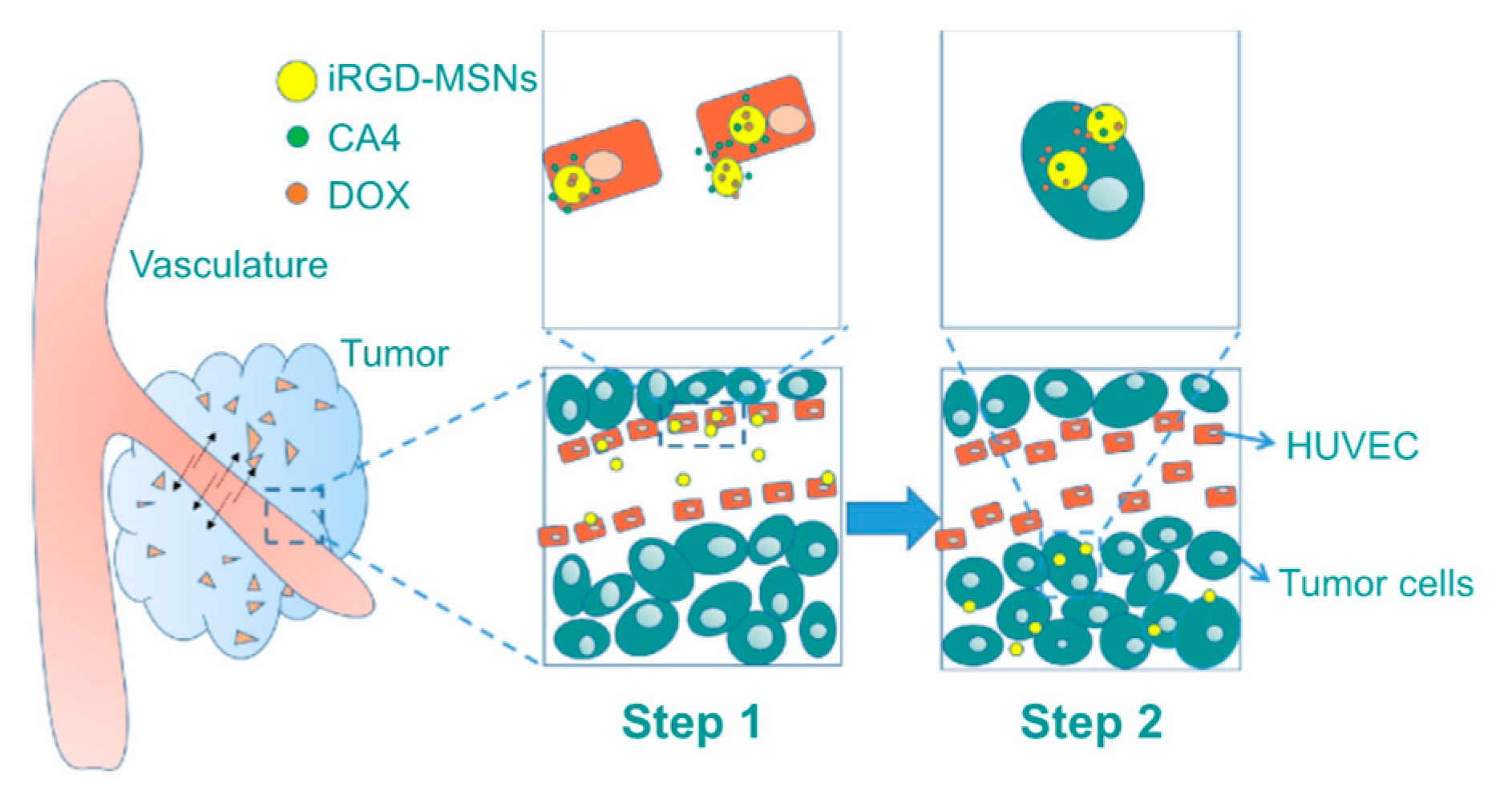
| Mesoporous silica nanoparticle | Cetyltrimethylammonium chloride tetraethyl orthosilicate +arginine-glycine-aspartic acid | Doxorubicin and Combretastatin-A4 | Physical encapsulation + Physical conjugation | Human cervical adenocarcinoma (HeLa xenograft model) | Observed synergistic anticancer and antiangiogenic effected | [93] |
| Gold nanoparticles | Thiol polyethylene glycol/folic acid-tethered thiol polyethylene glycol and polydopamine-coated gold | Doxorubicin and dopamine | Electrostatic interactions | Breast cancer (MCF-7/Adriamycin resistance cells) tumor xenograft model | Superior tumor inhibitory effects against multidrug resistance cancer | [94] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajora, A.K.; Ravishankar, D.; Zhang, H.; Rosenholm, J.M. Recent Advances and Impact of Chemotherapeutic and Antiangiogenic Nanoformulations for Combination Cancer Therapy. Pharmaceutics 2020, 12, 592. https://doi.org/10.3390/pharmaceutics12060592
Rajora AK, Ravishankar D, Zhang H, Rosenholm JM. Recent Advances and Impact of Chemotherapeutic and Antiangiogenic Nanoformulations for Combination Cancer Therapy. Pharmaceutics. 2020; 12(6):592. https://doi.org/10.3390/pharmaceutics12060592
Chicago/Turabian StyleRajora, Amit Kumar, Divyashree Ravishankar, Hongbo Zhang, and Jessica M. Rosenholm. 2020. "Recent Advances and Impact of Chemotherapeutic and Antiangiogenic Nanoformulations for Combination Cancer Therapy" Pharmaceutics 12, no. 6: 592. https://doi.org/10.3390/pharmaceutics12060592
APA StyleRajora, A. K., Ravishankar, D., Zhang, H., & Rosenholm, J. M. (2020). Recent Advances and Impact of Chemotherapeutic and Antiangiogenic Nanoformulations for Combination Cancer Therapy. Pharmaceutics, 12(6), 592. https://doi.org/10.3390/pharmaceutics12060592