
BNT162b2 or CoronaVac as the Third Dose against Omicron: Neutralizing Antibody Responses among Transplant Recipients Who Had Received Two Doses of CoronaVac

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
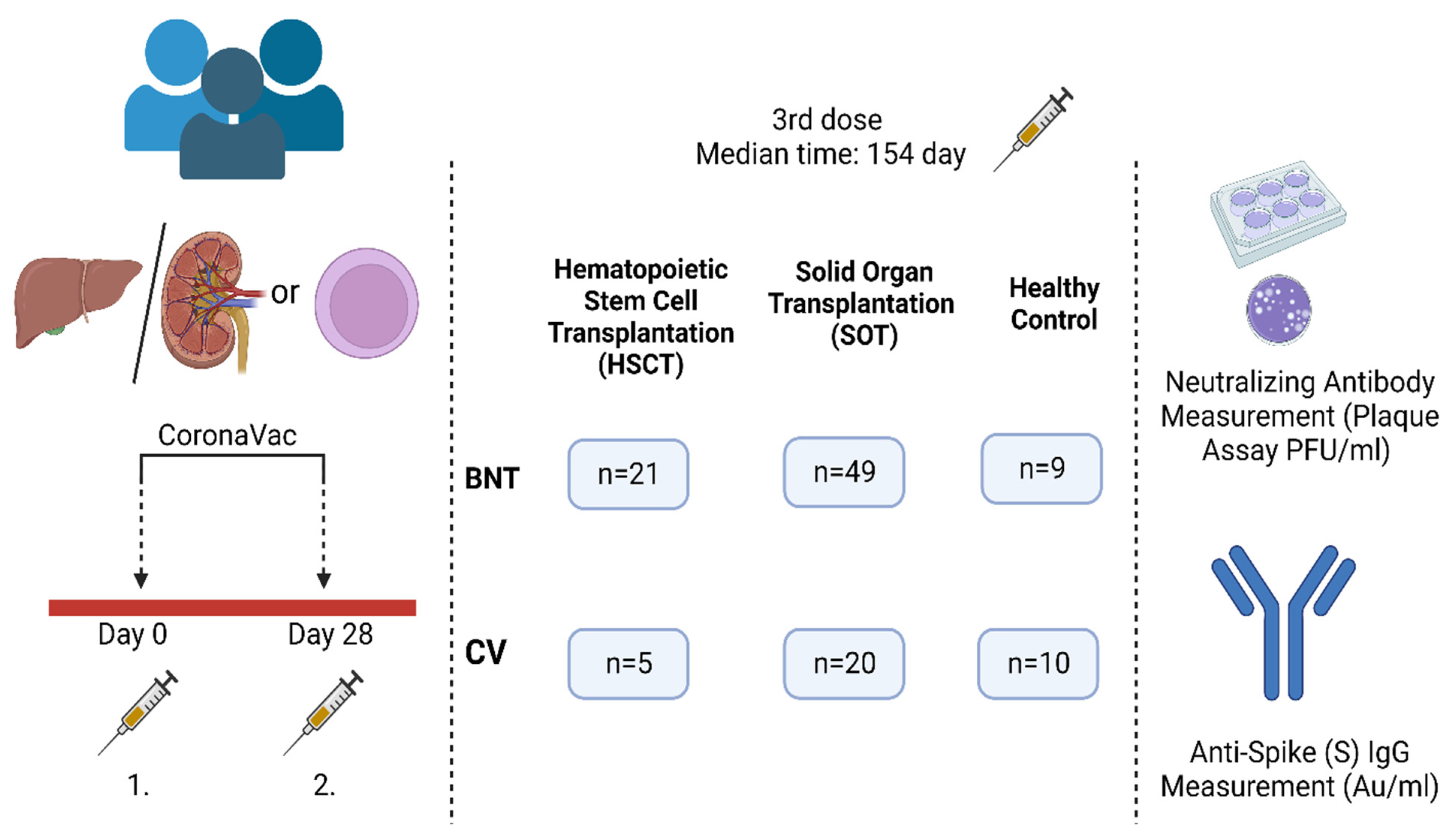
2.1. Study Design and Selection of Participants
2.2. Cell Culture and Plaque Assay
2.3. Anti-SARS-CoV-2 Spike (S) IgG Measurement
2.4. Statistical Analysis
3. Results
3.1. Study Design and Overall Results
3.2. The Demographic Characteristics of the Participants
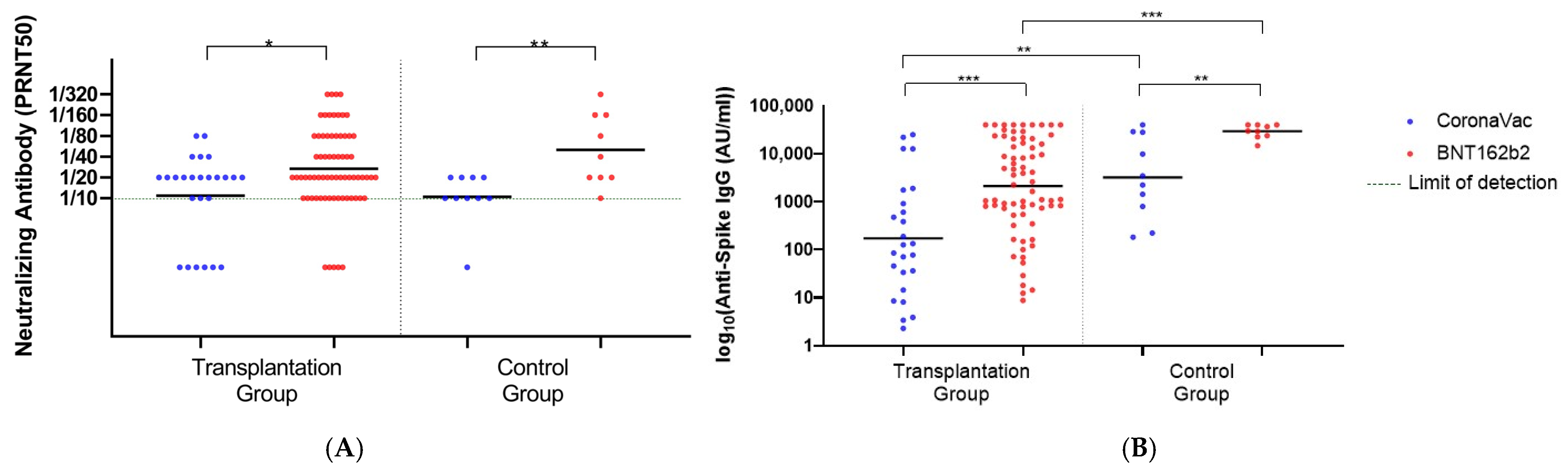
3.3. Overall Antibody Responses after the Third Dose in the Transplantation Group
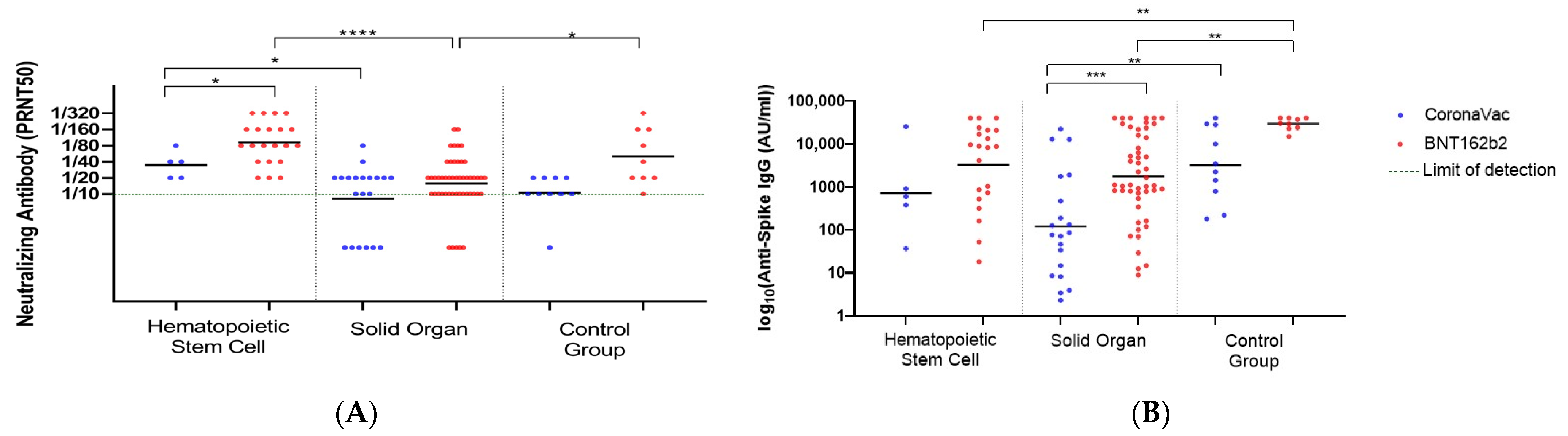
3.4. Antibody Responses after the Third Dose in the HSCT and the SOT Groups
3.5. Antibody Responses after the Third Dose in Each Transplantation Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://www.worldometers.info/coronavirus/ (accessed on 5 November 2022).
- Embi, P.J.; Levy, M.E.; Naleway, A.L.; Patel, P.; Gaglani, M.; Natarajan, K.; Dascomb, K.; Ong, T.C.; Klein, N.P.; Liao, I.C.; et al. Effectiveness of 2-Dose Vaccination with mRNA COVID-19 Vaccines Against COVID-19-Associated Hospitalizations Among Immunocompromised Adults—Nine States, January-September 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1553–1559. [Google Scholar] [CrossRef]
- Qin, C.X.; Moore, L.W.; Anjan, S.; Rahamimov, R.; Sifri, C.D.; Ali, N.M.; Morales, M.K.; Tsapepas, D.S.; Basic-Jukic, N.; Miller, R.A.; et al. Risk of Breakthrough SARS-CoV-2 Infections in Adult Transplant Recipients. Transplantation 2021, 105, e265–e266. [Google Scholar] [CrossRef]
- Galmiche, S.; Luong Nguyen, L.B.; Tartour, E.; de Lamballerie, X.; Wittkop, L.; Loubet, P.; Launay, O. Immunological and clinical efficacy of COVID-19 vaccines in immunocompromised populations: A systematic review. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2022, 28, 163–177. [Google Scholar] [CrossRef]
- Kumar, S.; Karuppanan, K.; Subramaniam, G. Omicron (BA.1) and sub-variants (BA.1.1, BA.2, and BA.3) of SARS-CoV-2 spike infectivity and pathogenicity: A comparative sequence and structural-based computational assessment. J. Med. Virol. 2022, 94, 4780–4791. [Google Scholar] [CrossRef]
- Rescigno, M.; Agrati, C.; Salvarani, C.; Giannarelli, D.; Costantini, M.; Mantovani, A.; Massafra, R.; Zinzani, P.L.; Morrone, A.; Notari, S.; et al. Neutralizing antibodies to Omicron after the fourth SARS-CoV-2 mRNA vaccine dose in immunocompromised patients highlight the need of additional boosters. Front. Immunol. 2023, 14, 1104124. [Google Scholar] [CrossRef]
- Kumar, D.; Hu, Q.; Samson, R.; Ferreira, V.H.; Hall, V.G.; Ierullo, M.; Majchrzak-Kita, B.; Hardy, W.; Gingras, A.C.; Humar, A. Neutralization against Omicron variant in transplant recipients after three doses of mRNA vaccine. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2022, 22, 2089–2093. [Google Scholar] [CrossRef] [PubMed]
- Medina-Pestana, J.; Almeida Viana, L.; Nakamura, M.R.; Lucena, E.F.; Granato, C.F.H.; Dreige, Y.C.; Amorim, L.V.P.; Chow, C.Y.Z.; Demarchi Foresto, R.; Roberto Requião-Moura, L.; et al. Immunogenicity After a Heterologous BNT262b2 Versus Homologous Booster in Kidney Transplant Recipients Receiving 2 Doses of CoronaVac Vaccine: A Prospective Cohort Study. Transplantation 2022, 106, 2076–2084. [Google Scholar] [CrossRef] [PubMed]
- Chiarucci, M.; Paolasini, S.; Isidori, A.; Guiducci, B.; Loscocco, F.; Capalbo, M.; Visani, G. Immunological Response Against SARS-CoV-2 After BNT162b2 Vaccine Administration Is Impaired in Allogeneic but Not in Autologous Stem Cell Transplant Recipients. Front. Oncol. 2021, 11, 737300. [Google Scholar] [CrossRef] [PubMed]
- Medina-Pestana, J.; Cristelli, M.P.; Viana, L.A.; Foresto, R.D.; Requião-Moura, L.R.; Tedesco-Silva, H.; Covas, D.T. Clinical Impact, Reactogenicity, and Immunogenicity After the First CoronaVac Dose in Kidney Transplant Recipients. Transplantation 2022, 106, e95–e97. [Google Scholar] [CrossRef]
- Rozen-Zvi, B.; Yahav, D.; Agur, T.; Zingerman, B.; Ben-Zvi, H.; Atamna, A.; Tau, N.; Mashraki, T.; Nesher, E.; Rahamimov, R. Antibody response to SARS-CoV-2 mRNA vaccine among kidney transplant recipients: A prospective cohort study. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2021, 27, 1173.e1171–1173.e1174. [Google Scholar] [CrossRef]
- Tanriover, M.D.; Doğanay, H.L.; Akova, M.; Güner, H.R.; Azap, A.; Akhan, S.; Köse, Ş.; Erdinç, F.; Akalın, E.H.; Tabak, Ö.F.; et al. Efficacy and safety of an inactivated whole-virion SARS-CoV-2 vaccine (CoronaVac): Interim results of a double-blind, randomised, placebo-controlled, phase 3 trial in Turkey. Lancet 2021, 398, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Yalçın, T.Y.; Topçu, D.I.; Doğan, Ö.; Aydın, S.; Sarı, N.; Erol, Ç.; Kuloğlu, Z.E.; Azap, Ö.K.; Can, F.; Arslan, H. Immunogenicity after two doses of inactivated virus vaccine in healthcare workers with and without previous COVID-19 infection: Prospective observational study. J. Med. Virol. 2021, 94, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18-59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet. Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Erol, Ç.; Yanık Yalçın, T.; Sarı, N.; Bayraktar, N.; Ayvazoğlu Soy, E.; Yavuz Çolak, M.; Azap, Ö.; Arslan, H.; Haberal, M. Differences in Antibody Responses Between an Inactivated SARS-CoV-2 Vaccine and the BNT162b2 mRNA Vaccine in Solid-Organ Transplant Recipients. Exp. Clin. Transplant. Off. J. Middle East Soc. Organ Transplant. 2021, 19, 1334–1340. [Google Scholar] [CrossRef]
- Kagina, B.M.; Dochez, C. COVID-19 vaccine-induced immunity: Head-to-head comparison of mRNA (BNT162b2) versus inactivated (CoronaVac) vaccines. Respirology 2022, 27, 260–261. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier, G.; Perrin, P.; Olagne, J.; Cognard, N.; Fafi-Kremer, S.; Caillard, S. Antibody Response After a Third Dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients With Minimal Serologic Response to 2 Doses. JAMA 2021, 236, 1063–1065. [Google Scholar] [CrossRef] [PubMed]
- CDC. COVID-19: Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Approved or Authorized in the United States; US Department of Health and Human Services, CDC: Atlanta, GA, USA, 2021. Available online: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html (accessed on 15 September 2022).
- Kwon, J.H.; Tenforde, M.W.; Gaglani, M.; Talbot, H.K.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Casey, J.D.; Mohr, N.M.; et al. mRNA Vaccine Effectiveness Against Coronavirus Disease 2019 Hospitalization Among Solid Organ Transplant Recipients. J. Infect. Dis. 2022, 226, 797–807. [Google Scholar] [CrossRef]
- Kuloğlu, Z.E.; El, R.; Guney-Esken, G.; Tok, Y.; Talay, Z.G.; Barlas, T.; Kuskucu, M.A.; Albayrak, Ö.; Doğan, Ö.; Yavuz, S.; et al. Effect of BTN162b2 and CoronaVac boosters on humoral and cellular immunity of individuals previously fully vaccinated with CoronaVac against SARS-CoV-2: A longitudinal study. Allergy 2022, 77, 2459–2467. [Google Scholar] [CrossRef]
- Pérez-Then, E.; Lucas, C.; Monteiro, V.S.; Miric, M.; Brache, V.; Cochon, L.; Vogels, C.B.F.; Malik, A.A.; De la Cruz, E.; Jorge, A.; et al. Neutralizing antibodies against the SARS-CoV-2 Delta and Omicron variants following heterologous CoronaVac plus BNT162b2 booster vaccination. Nat. Med. 2022, 28, 481–485. [Google Scholar] [CrossRef]
- Dib, M.; Le Corre, N.; Ortiz, C.; García, D.; Ferrés, M.; Martinez-Valdebenito, C.; Ruiz-Tagle, C.; Ojeda, M.J.; Espinoza, M.A.; Jara, A.; et al. SARS-CoV-2 vaccine booster in solid organ transplant recipients previously immunised with inactivated versus mRNA vaccines: A prospective cohort study. Lancet Reg. Health–Am. 2022, 16, 100371. [Google Scholar] [CrossRef]
- Rahav, G.; Lustig, Y.; Lavee, J.; Ohad, B.; Magen, H.; Hod, T.; Noga, S.-T.; Shmueli, E.S.; Drorit, M.; Ben-Ari, Z.; et al. BNT162b2 mRNA COVID-19 vaccination in immunocompromised patients: A prospective cohort study. EClinicalMedicine 2021, 41, 101158. [Google Scholar] [CrossRef] [PubMed]
- Abid, M.B.; Rubin, M.; Ledeboer, N.; Szabo, A.; Longo, W.; Mohan, M.; Shah, N.N.; Fenske, T.S.; Abedin, S.; Runaas, L.; et al. Efficacy of a third SARS-CoV-2 mRNA vaccine dose among hematopoietic cell transplantation, CAR T cell, and BiTE recipients. Cancer Cell 2022, 40, 340–342. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Wang, L.; Shen, L.; He, L.; Tang, K. Immune response to vaccination against SARS-CoV-2 in hematopoietic stem cell transplantation and CAR T-cell therapy recipients. J. Hematol. Oncol. 2022, 15, 81. [Google Scholar] [CrossRef]
- Canti, L.; Humblet-Baron, S.; Desombere, I.; Neumann, J.; Pannus, P.; Heyndrickx, L.; Henry, A.; Servais, S.; Willems, E.; Ehx, G.; et al. Predictors of neutralizing antibody response to BNT162b2 vaccination in allogeneic hematopoietic stem cell transplant recipients. J. Hematol. Oncol. 2021, 14, 174. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 95) | BNT162b2 Group (n = 70) | CoronaVac Group (n = 25) | |
|---|---|---|---|
| Median age (IQR *) Age group (n/%) 18–29 30–39 40–49 50–59 >60 | 56 (42–63) 9 (9.5) 12 (12.6) 18 (18.9) 24 (25.3) 32 (33.7) | 56.5 (43–65) 6 (8.6) 9 (12.9) 13 (18.6) 16 (22.9) 26 (37.1) | 52 (39.5–60) 3 (12.0) 3 (12.0) 5 (20.0) 8 (32.0) 6 (24.0) |
| Female gender (n/%) | 28 (29.5) | 24 (34.3) | 4 (16.0) |
| Type of transplantation (n/%) SOT ** Liver Kidney HSCT *** Autologous Allogeneic | 69 (72.6) 52 (54.7) 17 (17.9) 26 (27.4) 21 (22.1) 5 (5.3) | 49 (70.0) 38 (54.3) 11 (15.7) 21 (30.0) 16 (22.9) 5 (7.1) | 20 (80.0) 14 (56.0) 6 (24.0) 5 (20.0) 5 (20.0) 0 (0) |
| Median time after transplantation-years (IQR) | 4 (2–6) | 4 (2–6) | 4 (3–6) |
| Time after the booster dose (n/%) <6 months ≥6 months | 82 (86.3) 13 (13.7) | 60 (85.7) 10 (14.3) | 22 (88.0) 3 (12.0) |
| Antimetabolite usage for SOT (n/%) | 28 (40.6) | 23 (32.9) | 5 (20.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erol, Ç.; Kuloğlu, Z.E.; Kayaaslan, B.; Esken, G.; Altunsoy, A.; Barlas, T.; Çınar, G.; Hasanoğlu, İ.; Oruç, E.; İncir, S.; et al. BNT162b2 or CoronaVac as the Third Dose against Omicron: Neutralizing Antibody Responses among Transplant Recipients Who Had Received Two Doses of CoronaVac. Viruses 2023, 15, 1534. https://doi.org/10.3390/v15071534
Erol Ç, Kuloğlu ZE, Kayaaslan B, Esken G, Altunsoy A, Barlas T, Çınar G, Hasanoğlu İ, Oruç E, İncir S, et al. BNT162b2 or CoronaVac as the Third Dose against Omicron: Neutralizing Antibody Responses among Transplant Recipients Who Had Received Two Doses of CoronaVac. Viruses. 2023; 15(7):1534. https://doi.org/10.3390/v15071534
Chicago/Turabian StyleErol, Çiğdem, Zeynep Ece Kuloğlu, Bircan Kayaaslan, Gülen Esken, Adalet Altunsoy, Tayfun Barlas, Güle Çınar, İmran Hasanoğlu, Ebru Oruç, Said İncir, and et al. 2023. "BNT162b2 or CoronaVac as the Third Dose against Omicron: Neutralizing Antibody Responses among Transplant Recipients Who Had Received Two Doses of CoronaVac" Viruses 15, no. 7: 1534. https://doi.org/10.3390/v15071534
APA StyleErol, Ç., Kuloğlu, Z. E., Kayaaslan, B., Esken, G., Altunsoy, A., Barlas, T., Çınar, G., Hasanoğlu, İ., Oruç, E., İncir, S., Azap, A., Korkmaz, G., Turan Gökçe, D., Kırımker, O. E., Coşkun Yenigün, E., Ölçücüoğlu, E., Ayvazoğlu Soy, E., Çetinkünar, S., Kurt Azap, Ö., ... Haberal, M. (2023). BNT162b2 or CoronaVac as the Third Dose against Omicron: Neutralizing Antibody Responses among Transplant Recipients Who Had Received Two Doses of CoronaVac. Viruses, 15(7), 1534. https://doi.org/10.3390/v15071534