
Does Intra-Uterine Exposure to the Zika Virus Increase Risks of Cognitive Delay at Preschool Ages? Findings from a Zika-Exposed Cohort from Grenada, West Indies
 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
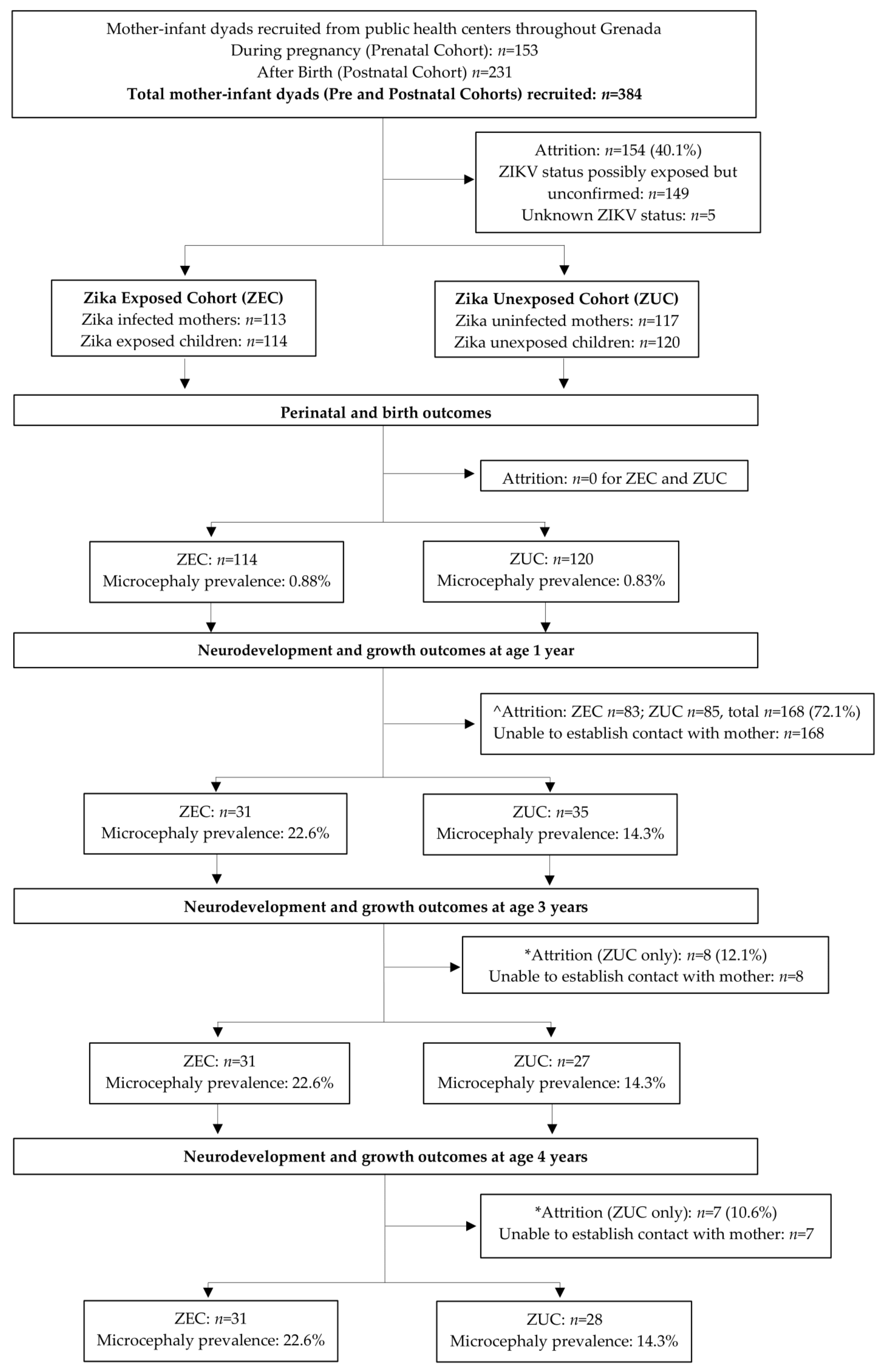
2.1. Study Population and Procedures
2.2. Laboratory Testing
2.3. Inclusion Criteria
2.4. Neurodevelopmental and Vision Assessments
2.4.1. The Oxford Neurodevelopmental Assessment (OX-NDA)
2.4.2. The Developmental Neuropsychological Assessment, Second Edition (NEPSY-II)
2.4.3. The Cardiff Tests of Vision
2.5. Anthropometric Measures and Head Circumference Classification
2.6. Health and Socio-Environmental Outcomes
2.7. Statistical Analysis
2.8. Ethical Approval
3. Results
3.1. Participant Characteristics
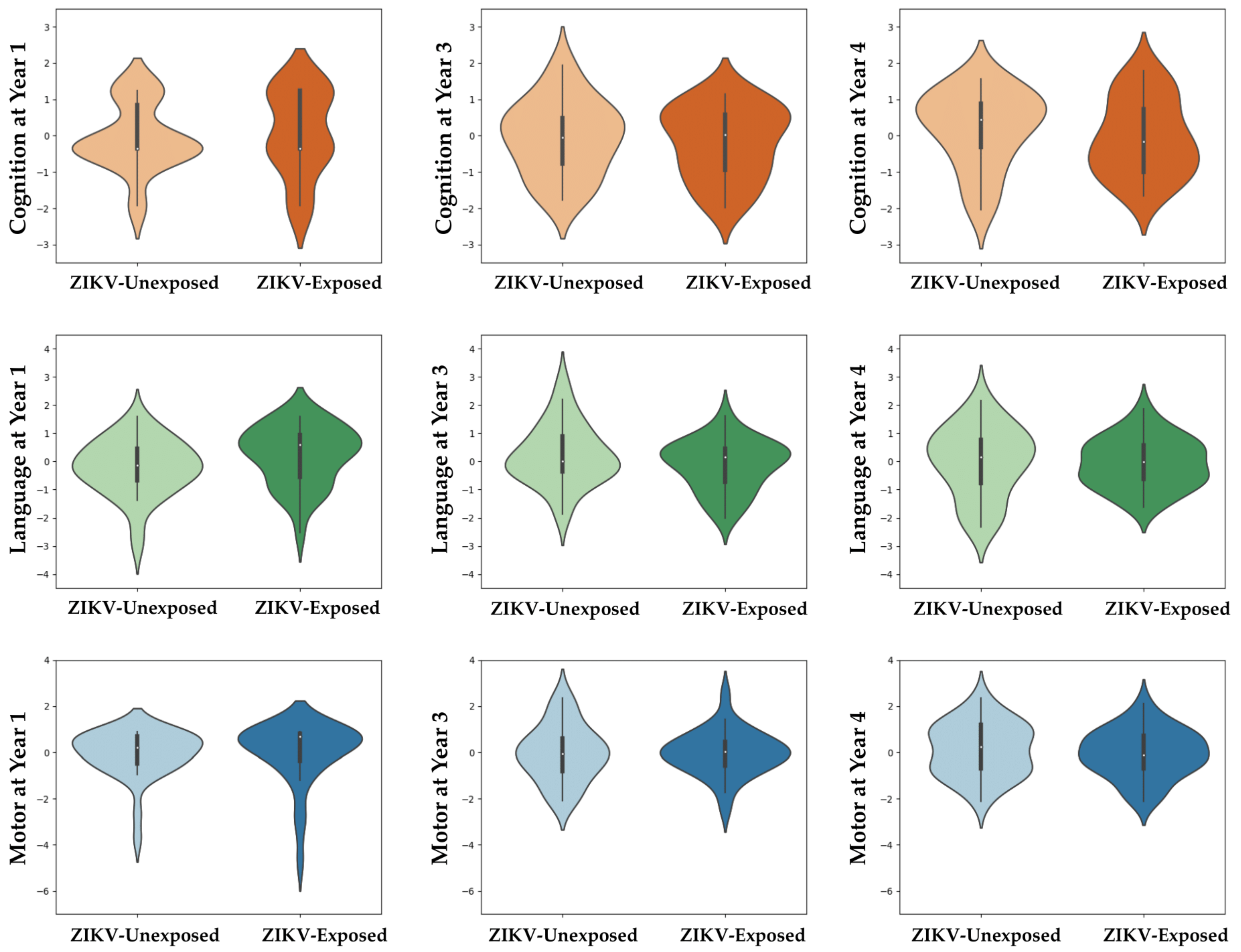
3.2. Comparisons between ZIKV-Exposed and Unexposed Children at 1, 3 and 4 Years
3.2.1. Neurodevelopmental Scores and Prevalence of Neurodevelopmental Delay
3.2.2. Visual Acuity and Contrast Sensitivity
3.2.3. Microcephaly and Growth Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Black, M.M.; Walker, S.P.; Fernald, L.C.H.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early childhood development coming of age: Science through the life course. Lancet 2016, 389, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Bethlehem, R.A.; Seidlitz, J.; White, S.R.; Vogel, J.W.; Anderson, K.M.; Adamson, C.; Adler, S.; Alexopoulos, G.S.; Anagnostou, E.; Areces-Gonzalez, A. Brain charts for the human lifespan. Nature 2022, 604, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Blackmon, K.; Evans, R.; Fernandes, M.; Landon, B.; Noel, T.; Macpherson, C.; Cudjoe, N.; Burgen, K.S.; Punch, B.; Krystosik, A. Neurodevelopment in normocephalic children with and without prenatal Zika virus exposure. Arch. Dis. Child. 2021, 107, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Sobral da Silva, P.F.; Eickmann, S.H.; Ximenes, R.A.d.A.; Martelli, C.M.T.; Brickley, E.B.; Lima, M.C.; Montarroyos, U.R.; Carvalho, M.D.C.G.d.; Rodrigues, L.C.; Araújo, T.V.B.d. Neurodevelopment in Children Exposed to Zika Virus: What Are the Consequences for Children Who Do Not Present with Microcephaly at Birth? Viruses 2021, 13, 1427. [Google Scholar] [CrossRef] [PubMed]
- Walker, C.L.; Little, M.-T.E.; Roby, J.A.; Armistead, B.; Gale, M., Jr.; Rajagopal, L.; Nelson, B.R.; Ehinger, N.; Mason, B.; Nayeri, U. Zika virus and the nonmicrocephalic fetus: Why we should still worry. Am. J. Obstet. Gynecol. 2019, 220, 45–56. [Google Scholar] [CrossRef]
- Musso, D.; Ko, A.I.; Baud, D. Zika virus infection—After the pandemic. N. Engl. J. Med. 2019, 381, 1444–1457. [Google Scholar] [CrossRef]
- da Silva, P.F.S.; Eickmann, S.H.; de Alencar Ximenes, R.A.; Montarroyos, U.R.; de Carvalho Lima, M.; Martelli, C.M.T.; de Araújo, T.V.B.; Brickley, E.B.; Rodrigues, L.C.; da Silva Pastich, F.C.L. Pediatric neurodevelopment by prenatal Zika virus exposure: A cross-sectional study of the Microcephaly Epidemic Research Group Cohort. BMC Pediatr. 2020, 20, 472. [Google Scholar]
- Blackmon, K.; Evans, R.; Fernandes, M.; Landon, B.; Noël, T.; Macpherson, C.; Cudjoe, N.; Burgen, K.S.; Punch, B.; Krystosik, A.R. Visual Acuity Deficits in Otherwise Normally Developing Zika Virus Exposed Children. Available online: https://ssrn.com/abstract=3576849 (accessed on 8 October 2022).
- Rice, M.E.; Galang, R.R.; Roth, N.M.; Ellington, S.R.; Moore, C.A.; Valencia-Prado, M.; Ellis, E.M.; Tufa, A.J.; Taulung, L.A.; Alfred, J.M. Vital signs: Zika-associated birth defects and neurodevelopmental abnormalities possibly associated with congenital Zika virus infection—US territories and freely associated states, 2018. Morb. Mortal. Wkly. Rep. 2018, 67, 858. [Google Scholar]
- Aragao, M.; Holanda, A.; Brainer-Lima, A.; Petribu, N.; Castillo, M.; Van Der Linden, V.; Serpa, S.; Tenório, A.; Travassos, P.; Cordeiro, M. Nonmicrocephalic infants with congenital Zika syndrome suspected only after neuroimaging evaluation compared with those with microcephaly at birth and postnatally: How large is the Zika virus “iceberg”? Am. J. Neuroradiol. 2017, 38, 1427–1434. [Google Scholar] [CrossRef]
- Shao, Q.; Herrlinger, S.; Yang, S.-L.; Lai, F.; Moore, J.M.; Brindley, M.A.; Chen, J.-F. Zika virus infection disrupts neurovascular development and results in postnatal microcephaly with brain damage. Development 2016, 143, 4127–4136. [Google Scholar] [CrossRef]
- Cardoso, T.F.; Dos Santos, R.S.; Corrêa, R.M.; Campos, J.V.; de Bastos Silva, R.; Tobias, C.C.; Prata-Barbosa, A.; da Cunha, A.J.L.A.; Ferreira, H.C. Congenital Zika infection: Neurology can occur without microcephaly. Arch. Dis. Child. 2019, 104, 199–200. [Google Scholar] [CrossRef] [PubMed]
- Brenciaglia, M.; Noël, T.P.; Fields, P.J.; Bidaisee, S.; Myers, T.E.; Nelson, W.M.; Venkateswaran, N.; Venkateswaran, K.; Parameswaran, N.; Bahadoor, A. Clinical, serological, and molecular observations from a case series study during the Asian lineage Zika virus outbreak in Grenada during 2016. Can. J. Infect. Dis. Med. Microbiol. 2018, 2018, 4635647. [Google Scholar] [CrossRef] [PubMed]
- Grossi-Soyster, E.N.; Cook, E.A.; de Glanville, W.A.; Thomas, L.F.; Krystosik, A.R.; Lee, J.; Wamae, C.N.; Kariuki, S.; Fevre, E.M.; LaBeaud, A.D. Serological and spatial analysis of alphavirus and flavivirus prevalence and risk factors in a rural community in western Kenya. PLoS Negl. Trop. Dis. 2017, 11, e0005998. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Pinsky, B.A.; Ananta, J.S.; Zhao, S.; Arulkumar, S.; Wan, H.; Sahoo, M.K.; Abeynayake, J.; Waggoner, J.J.; Hopes, C. Diagnosis of Zika virus infection on a nanotechnology platform. Nat. Med. 2017, 23, 548–550. [Google Scholar] [CrossRef]
- Fernandes, M.; Bassani, D.; Albernaz, E.; Bertoldi, A.; Silveira, M.F.; Matijsevich, A.; Anselmi, L.; Cruz, S.; Halal, C.S.; Tovo-Rodrigues, L. Pre-print: Construction and Validation of the Oxford Neurodevelopment Assessment (OX-NDA) in 1-year-old Brazilian Children. BMC Pediatr. 2022, 22, 733. [Google Scholar] [CrossRef]
- Santos, I.S.; Bassani, D.G.; Matijasevich, A.; Halal, C.S.; Del-Ponte, B.; da Cruz, S.H.; Anselmi, L.; Albernaz, E.; Fernandes, M.; Tovo-Rodrigues, L. Infant sleep hygiene counseling (sleep trial): Protocol of a randomized controlled trial. BMC Psychiatry 2016, 16, 307. [Google Scholar] [CrossRef]
- Harkness, J.; Pennell, B.; Villar, A.; Gebler, N.; Aguilar-Gaxiola, S.; Bilgen, I. Translation procedures and translation assessment in the World Mental Health Survey Initiative. In The WHO World Mental Health Surveys: Global Perspectives on the Epidemiology of Mental Disorders; World Health Organization: Geneva, Switzerland, 2008; pp. 91–113. [Google Scholar]
- Brooks, B.L.; Sherman, E.M.; Strauss, E. NEPSY-II: A developmental neuropsychological assessment. Child Neuropsychol. 2009, 16, 80–101. [Google Scholar] [CrossRef]
- Korkman, M.; Kemp, S.; Kirk, U. NEPSY: A Developmental Neuropsychological Assessment Manual; PsychCorp: San Antonio, TX, USA, 1998. [Google Scholar]
- Fogarty Associates; The Cardiff Contrast Test. Available online: http://www.cardiffacuity.co.uk/contrast.htm (accessed on 18 November 2022).
- Adoh, T.O.; Woodhouse, J.M. The Cardiff acuity test used for measuring visual acuity development in toddlers. Vis. Res. 1994, 34, 555–560. [Google Scholar] [CrossRef]
- Adoh, T.O.; Woodhouse, J.M.; Oduwaiye, K.A. The Cardiff Test: A New Visual Acuity Test for Toddlers and Children with Intellectual Impairment. A Preliminary Report. Optom. Vis. Sci. 1992, 69, 427–432. [Google Scholar] [CrossRef]
- De Onis, M.; Garza, C.; Victora, C.G.; Onyango, A.W.; Frongillo, E.A.; Martines, J. The WHO Multicentre Growth Reference Study: Planning, study design, and methodology. Food Nutr. Bull. 2004, 25 (Suppl. S1), S15–S26. [Google Scholar] [CrossRef]
- WHO Multicentre Growth Reference Study Group; de Onis, M. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. 2006, 95, 76–85. [Google Scholar] [CrossRef]
- World Health Organization. WHO Child Growth Standards: Head Circumference-for-Age, Arm Circumference-for-Age, Triceps Skinfold-for-Age and Subscapular Skinfold-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Abbasi, N.; Ghoochani, O.; Ghanian, M.; Kitterlin, M. Assessment of Households’ Food Insecurity through use of a USDA Questionnaire. Adv. Plants Agric. Res. 2016, 4, 00155. [Google Scholar]
- Gureje, O.; Obikoya, B. The GHQ-12 as a screening tool in a primary care setting. Soc. Psychiatry Psychiatr. Epidemiol. 1990, 25, 276–280. [Google Scholar] [CrossRef]
- Malda, M. There Is No Place like Home: On the Relation between Culture and Children’s Cognition; Ridderprint: Alblasserdam, The Netherlands, 2009. [Google Scholar]
- Sines, J.; Clarke, W.; Lauer, R. Home environment questionnaire. J. Abnorm. Child Psychol. 1984, 12, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Patridge, E.F.; Bardyn, T.P. Research electronic data capture (REDCap). J. Med. Libr. Assoc.: JMLA 2018, 106, 142. [Google Scholar] [CrossRef]
- Grant, R.; Fléchelles, O.; Tressières, B.; Dialo, M.; Elenga, N.; Mediamolle, N.; Mallard, A.; Hebert, J.C.; Lachaume, N.; Couchy, E.; et al. In utero Zika virus exposure and neurodevelopment at 24 months in toddlers normocephalic at birth: A cohort study. BMC Med. 2021, 19, 12. [Google Scholar] [CrossRef]
- Subissi, L.; Dub, T.; Besnard, M.; Mariteragi-Helle, T.; Nhan, T.; Lutringer-Magnin, D.; Barboza, P.; Gurry, C.; Brindel, P.; Nilles, E.J. Zika virus infection during pregnancy and effects on early childhood development, French Polynesia, 2013–2016. Emerg. Infect. Dis. 2018, 24, 1850. [Google Scholar] [CrossRef] [PubMed]
- Neelam, V.; Woodworth, K.R.; Chang, D.J.; Roth, N.M.; Reynolds, M.R.; Akosa, A.; Carr, C.P.; Anderson, K.N.; Mulkey, S.B.; DeBiasi, R.L. Outcomes up to Age 36 Months after Congenital Zika Virus Infection–US States. 2023. Available online: https://assets.researchsquare.com/files/rs-2475564/v1/df073c0d-0941-4593-96f5-3adad02dd9cc.pdf?c=1673907757 (accessed on 12 February 2023).
- Cranston, J.S.; Tiene, S.F.; Nielsen-Saines, K.; Vasconcelos, Z.; Pone, M.V.; Pone, S.; Zin, A.; Salles, T.S.; Pereira, J.P.; Orofino, D. Association between antenatal exposure to Zika virus and anatomical and neurodevelopmental abnormalities in children. JAMA Netw. Open 2020, 3, e209303. [Google Scholar] [CrossRef] [PubMed]
- Lopes Moreira, M.E.; Nielsen-Saines, K.; Brasil, P.; Kerin, T.; Damasceno, L.; Pone, M.; Carvalho, L.M.; Pone, S.M.; Vasconcelos, Z.; Ribeiro, I.P. Neurodevelopment in infants exposed to Zika virus in utero. N. Engl. J. Med. 2018, 379, 2377–2379. [Google Scholar] [CrossRef]
- Faiçal, A.V.; de Oliveira, J.C.; Oliveira, J.V.V.; de Almeida, B.L.; Agra, I.A.; Alcantara, L.C.J.; Acosta, A.X.; de Siqueira, I.C. Neurodevelopmental delay in normocephalic children with in utero exposure to Zika virus. BMJ Paediatr. Open 2019, 3, e000486. [Google Scholar] [CrossRef] [PubMed]
- Tiene, S.F.; Cranston, J.S.; Nielsen-Saines, K.; Kerin, T.; Fuller, T.; Vasconcelos, Z.; Marschik, P.B.; Zhang, D.; Pone, M.; Pone, S. Early Predictors of Poor Neurologic Outcomes in a Prospective Cohort of Infants with Antenatal Exposure to Zika Virus. Pediatr. Infect. Dis. J. 2021, 41, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, O.; Newton, S.M.; Daza, M.; Cates, J.E.; Reales, J.A.; Burkel, V.K.; Mercado, M.; Godfred-Cato, S.; Gonzalez, M.; Anderson, K.N.; et al. Neurodevelopmental findings in children 20-30 months of age with postnatal Zika infection at 1-12 months of age, Colombia, September-November 2017. Paediatr. Perinat. Epidemiol. 2021, 35, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Marbán-Castro, E.; Vazquez Guillamet, L.J.; Pantoja, P.E.; Casellas, A.; Maxwell, L.; Mulkey, S.B.; Menéndez, C.; Bardají, A. Neurodevelopment in normocephalic children exposed to Zika virus in utero with No observable defects at birth: A systematic review with meta-analysis. Int. J. Environ. Res. Public Health 2022, 19, 7319. [Google Scholar] [CrossRef]
- Bayer, A.; Lennemann, N.J.; Ouyang, Y.; Bramley, J.C.; Morosky, S.; Marques, E.T.D.A., Jr.; Cherry, S.; Sadovsky, Y.; Coyne, C.B. Type III interferons produced by human placental trophoblasts confer protection against Zika virus infection. Cell Host Microbe 2016, 19, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, M.A.; Yunusov, D.; Balaraman, V.; Alexenko, A.P.; Yabe, S.; Verjovski-Almeida, S.; Schust, D.J.; Franz, A.W.; Sadovsky, Y.; Ezashi, T. Vulnerability of primitive human placental trophoblast to Zika virus. Proc. Natl. Acad. Sci. USA 2017, 114, E1587–E1596. [Google Scholar] [CrossRef]
- Mulkey, S.B.; Arroyave-Wessel, M.; Peyton, C.; Bulas, D.I.; Fourzali, Y.; Jiang, J.; Russo, S.; McCarter, R.; Msall, M.E.; Du Plessis, A.J. Neurodevelopmental abnormalities in children with in utero Zika virus exposure without congenital Zika syndrome. JAMA Pediatr. 2020, 174, 269–276. [Google Scholar] [CrossRef]
- Viens, L.J.; Fleck-Derderian, S.; Baez-Santiago, M.A.; Oduyebo, T.; Broussard, C.S.; Khan, S.; Jones, A.M.; Meaney-Delman, D. Role of Prenatal Ultrasonography and Amniocentesis in the Diagnosis of Congenital Zika Syndrome: A Systematic Review. Obstet. Gynecol. 2020, 135, 1185–1197. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Participant Characteristics | Pooled Sample: Birth and 1 Year | ZIKV-Exposed (Birth and 1 Year) | Unexposed (Birth and 1 Year) | Test Statistic, p | Pooled Sample: 3 Years Follow-Up (N or Mean (SD) | Pooled Sample: 4 Years Follow-Up (N or Mean (SD) |
|---|---|---|---|---|---|---|
| N (%) or Mean (SD) | N (%) or Mean (SD) | N (%) or Mean (SD) | Test Statistic g, p | Test Statistic h, p | ||
| Sex Male Female | 66 (0.50) | 16 (40.0) 15 (57.7) | 24 (60.0) 11 (42.3) | X2 = 1.98 p = 0.21 | 29 | 28 |
| X2 = 0.80 p = 0.37 | X2 = 0.48 p = 0.49 | |||||
| Age at 1 year assessment | 15.00 (2.29) | 15.52 (1.99) | 14.54 (2.47) | t = 1.75 p = 0.08 | 41.24 (3.56) | 50.36 (1.16) |
| t = 1.15 p = 0.26 | t = 0.08 p = 0.94 | |||||
| Birth Outcomes | ||||||
| Prematurity Premature Full-term | 52 (0.35) | 3 (42.9) 21 (46.7) | 4 (57.1) 24 (53.3) | ^^ p = 1.00 | 24 | 27 |
| X2 = 0.06 p = 0.80 | X2 = 0.63 p = 0.43 | |||||
| Delivery type Caesarean Vaginal | 66 (0.42) | 6 (40.0) 25 (49.0) | 9 (60.0) 26 (51.0) | X2= 0.38 p = 0.57 | 29 | 28 |
| X2 = 0.56 p = 0.76 | X2 = 1.06 p = 0.59 | |||||
| Delivery complications a Yes No | 65 (0.31) | 3 (42.9) 28 (48.3) | 4 (57.1) 30 (51.7) | ^^ X2= 0.07 p = 1.00 | 29 | 28 |
| X2 = 0.01 p = 0.94 | X2 = 0.90 p = 0.34 | |||||
| Neonatal resuscitation b Yes No | 66 (0.05) | 2 (66.7) 29 (46.0) | 1 (33.3) 34 (54.0) | ^^ p = 0.59 | 29 | 28 |
| X2 = 0.07 p = 0.79 | X2 = 0.12 p = 0.73 | |||||
| Neonatal complications c Yes No | 63 (0.37) | 5 (50.0) 25 (47.2) | 5 (50.0) 28 (52.8) | X2= 0.03 p = 1.00 | 28 | 28 |
| X2 = 0.01 p = 0.92 | X2 = 0.02 p = 0.90 | |||||
| Congenital abnormalities d Yes No | 66 (0.12) | 1 (100.0) 30 (46.2) | 0 (0.0) 35 (53.8) | ^ | 29 | 28 |
| X2 = 1.64 p = 0.20 | X2 = 0.12 p = 0.73 | |||||
| Chromosomal abnormalities Yes No | 48 (0.14) | 0 (0.0) 23 (48.9) | 1 (100.0) 24 (51.1) | ^ | 11 | 5 |
| ^ | ^ | |||||
| APGAR at 1 min | 7.92 (1.42) | 7.74 (1.86) | 8.09 (0.85) | t = −0.94 p = 0.35 | 8.28 (0.92) | 7.89 (1.19) |
| t = −1.05 p = 0.30 | t = 0.57 p = 0.57 | |||||
| Maternal age at delivery | 29.30 (6.74) | 28.68 (6.98) | 29.88 (6.56) | t = 0.71 p = 0.48 | 27.85 (5.93) | 28.56 (6.69) |
| t = 0.98 p = 0.33 | t = 0.67 p = 0.50 | |||||
| Gestational age at birth | 39.05 (2.17) | 39.17 (1.90) | 38.43 (2.95) | t =-1.05 p = 0.30 | 38.71 (2.71) | 39.48 (1.52) |
| t = 0.46 p = 0.65 | t = −1.10 p = 0.28 | |||||
| Total duration of exclusive breastfeeding period length (months) | 15.80 (7.53) | 14.67 (7.37) | 17.50 (8.54) | t = −0.56 p = 0.59 | 21.00 (8.19) | 15.60 (7.25) |
| t = −1.67 p = 0.12 | t = −0.50 p = 0.62 | |||||
| Age at weaning | 12.33 (7.06) | 13.30 (6.83) | 11.56 (7.30) | t = 0.91 p = 0.37 | 13.11 (8.60) | 13.04 (6.94) |
| t = −0.00 p = 0.99 | t = −0.02 p = 0.98 | |||||
| Growth Outcomes at Birth | ||||||
| Weight (kg) | 3.07 (0.55) | 3.11 (0.49) | 3.04 (0.61) | t = 0.41 p = 0.69 | 3.19 (0.56) | 3.26 (0.66) |
| t = 0.08 p = 0.93 | t = −0.55 p = 0.58 | |||||
| Weight WHO classification Wasted Normal | 33 (0.24) | 0 (0.0) 14 (45.2) | 2 (100.0) 17 (54.8) | ^^ p = 0.49 | 18 | 21 |
| X2 = 4.99 p = 0.03 | X2 = 1.41 p = 0.24 | |||||
| Length (cm) | 47.96 (3.89) | 47.97 (2.63) | 47.95 (4.73) | t = 0.01 p = 0.99 | 46.03 (7.00) | 49.27 (2.95) |
| t = 1.13 p = 0.27 | t = −1.60 p = 0.12 | |||||
| Length WHO classification Stunted Normal | 34 (0.41) | 4 (57.1) 11 (40.7) | 3 (42.9) 16 (59.3) | ^^ p = 0.67 | 18 | 22 |
| X2 = 0.17 p = 0.68 | X2 = 2.63 p = 0.11 | |||||
| Head circumference (cm) | 33.18 (1.75) | 33.29 (1.65) | 33.09 (1.85) | t = 0.37 p = 0.71 | 33.04 (1.92) | 33.61 (1.63) |
| t = 0.95 p = 0.35 | t = −0.55 p = 0.59 | |||||
| Head circumference classification at birth Normocephalic Borderline microcephalic e Microcephalic f Macrocephalic | 48 (0.47) | 19 (45.2) 1 (25.0) 1 (50.0) 0 (0.0) | 23 (54.8) 3 (75.0) 1 (50.0) 0 (0.0) | ^^ X2= 0.64 p = 0.81 | 23 | 22 |
| X2 = 2.28 p = 0.32 | X2 = 2.35 p = 0.50 | |||||
| Growth Outcomes at Age 1 Year | ||||||
| Weight (kg) | 6.70 (2.56) | 6.63 (1.97) | 6.76 (3.00) | t = −0.21 p = 0.83 | 7.25 (2.47) | 7.13 (1.84) |
| t = 0.87 p = 0.39 | t = 1.19 p = 0.24 | |||||
| Weight WHO classification Wasted Normal | 65 (0.44) | 3 (60.0) 27 (45.8) | 2 (40.0) 32 (54.2) | ^^ p = 0.66 | 9 | 7 |
| X2 = 0.67 p = 0.41 | X2 = 0.40 p = 0.53 | |||||
| Length (cm) | 63.93 (8.42) | 63.90 (7.99) | 62.71 (8.70) | t =-0.58 p =0.57 | 63.87 (9.14) | 64.11 (6.39) |
| t = 1.207 p = 0.23 | t = 1.36 p = 0.18 | |||||
| Length WHO classification Stunted Normal | 66 (0.29) | 2 (33.3) 29 (48.3) | 4 (51.7) 31 (66.7) | ^^ p = 0.67 | 11 | 7 |
| X2 = 0.70 p = 0.40 | X2 = 1.51 p = 0.22 | |||||
| Head circumference (cm) | 40.21 (3.83) | 40.59 (4.41) | 39.87 (3.27) | t = 0.75 p = 0.46 | 41.38 (4.40) | 41.13 (2.94) |
| t = 0.65 p = 0.52 | t = 1.07 p = 0.29 | |||||
| Head circumference classification at 1 Normocephalic Borderline microcephalic e Microcephalic f Macrocephalic | 66 (0.89) | 23 (47.9) 0 (0.0) 7 (58.3) 1 (100.0) | 25 (52.1) 5 (100.0) 5 (41.7) 0 (0.0) | ^^ X2 = 6.19 p = 0.07 | 11 | 7 |
| X2 = 3.72 p = 0.16 | X2 = 2.55 p = 0.28 | |||||
| Sociodemographic Characteristics | ||||||
| Maternal marital status Single Married | 64 (0.49) | 9 (33.3) 22 (56.4) | 18 (66.7) 17 (43.6) | X2 = 3.41 p = 0.08 | 29 | 28 |
| X2 = 3.20 p = 0.07 | X2 = 0.29 p = 0.59 | |||||
| Maternal education level Primary Secondary Tertiary | 49 (0.59) | 3 (42.9) 17 (47.2) 10 (58.8) | 4 (57.1) 19 (52.8) 7 (41.2) | ^^ X2 = 0.78 p = 0.75 | 29 | 25 |
| X2 = 0.26 p = 0.88 | X2 = 0.02 p = 0.99 | |||||
| Partner education level Primary Secondary Tertiary | 33 (0.46) | 3 (42.9) 22 (66.7) 3 (27.3) | 4 (57.1) 11 (33.3) 8 (72.7) | ^^ X2= 5.65 p = 0.06 | 27 | 24 |
| X2 = 2.81 p = 0.25 | X2 = 2.17 p = 0.34 | |||||
| Household monthly income (XCD) Under 1000 1001–2000 2001–3000 Over 3000 | 41 (0.99) | 7 (70.0) 7 (43.8) 7 (41.2) 5 (41.7) | 3 (30.0) 9 (56.3) 10 (58.8) 7 (58.3) | X2 = 2.56 p = 0.49 | 26 | 20 |
| X2 = 4.63 p = 0.20 | X2 = 7.24 p = 0.07 | |||||
| Infection Status | ||||||
| Child’s DENV infection status DENV-positive DENV-negative | 60 (0.30) | 3 (50.0) 27 (50.0) | 3 (50.0) 27 (50.0) | ^^ p = 1.00 | 24 | 22 |
| X2 = 0.67 p = 0.41 | X2 = 0.09 p = 0.76 | |||||
| Child’s ZIKV infection status ZIKV-positive ZIKV-negative | 60 (0.18) | 2 (100.0) 28 (48.3) | 0 (0.0) 30 (51.7) | ^^ X2 = 2.01 p = 0.49 | 23 | 22 |
| X2 = 1.13 p = 0.29 | X2 = 1.03 p = 0.31 | |||||
| Age at Assessment (Neurodevelopment Test) | ZIKV Exposure Group | Cognition | Motor | Language | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean (SD) | Test Statistic; p | N | Mean (SD) | Test Statistic; p | N | Mean (SD) | Test Statistic; p | ||
| 1 year (OX-NDA) | ZIKV-exposed | 30 | 56.96 (20.76) | t = –0.56 p = 0.58 | 30 | 95.83 (21.87) | t = 1.56 p = 0.12 | 29 | 71.43 (45.24) | t = 1.91 p = 0.06 |
| ZIKV-unexposed | 34 | 54.18 (19.16) | 34 | 87.5 (20.83) | 32 | 52.38 (32.14) | ||||
| 3 years (NEPSY-II) | ZIKV-exposed | 31 | 8.06 (2.48) | t = –0.20 p = 0.83 | 31 | 7.71 (2.66) | t = 0.42 p = 0.67 | 30 | 7.33 (1.99) | t = –1.34 p = 0.19 |
| ZIKV-unexposed | 27 | 8.20 (2.58) | 26 | 7.38 (3.18) | 26 | 8.13 (2.47) | ||||
| 4 years (NEPSY-II) | ZIKV-exposed | 31 | 7.95 (2.31) | t = –0.77 p = 0.44 | 31 | 8.52 (2.27) | t = -0.15 p = 0.88 | 31 | 7.95 (1.89) | t = 0.08 p = 0.93 |
| ZIKV-unexposed | 28 | 8.42 (2.35) | 28 | 8.61 (2.34) | 28 | 7.90 (2.66) | ||||
| Age at Assessment (Neurodevelopment Test) | ZIKV Exposure Group | Positive Behaviour | Negative Behaviour | Personal–Social | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean (SD) | Test Statistic; p | N | Mean (SD) | Test Statistic; p | N | Mean (SD) | Test Statistic; p | ||
| 1 year (OX-NDA) | ZIKV-exposed | 30 | 70.00 (80.00) | t = –0.02 p = 0.98 | 30 | 75.00 (25.00) | t = –0.00 p = 1.00 | – | – | - |
| ZIKV-unexposed | 30 | 70.38 (40.00) | 30 | 75.00 (50.00) | – | – | ||||
| 3 years (NEPSY-II) | ZIKV-exposed | – | – | – | – | – | – | 28 | 8.86 (3.59) | t = –0.30 p = 0.76 |
| ZIKV-unexposed | – | – | – | 21 | 9.14 (2.74) | |||||
| 4 years (NEPSY-II) | ZIKV-exposed | – | – | – | – | – | – | 30 | 8.00 (2.78) | t = –1.06 p = 0.29 |
| ZIKV-unexposed | – | – | – | 26 | 8.77 (2.61) | |||||
| Age at Assessment (Neuro-Development Test) | ZIKV Exposure Group | Cognition | Motor | Language | Personal–Social | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Delay | No Delay | Test Statistic; p | OR (95% CI) | Delay | No Delay | Test Statistic; p | OR (95% CI) | Delay | No Delay | Test Statistic; p | OR (95% CI) | Delay | No Delay | Test Statistic; p | OR (95% CI) | ||
| N (%), Mean (SD) or Median (IQR) | N (%), Mean (SD) or Median (IQR) | N (%), Mean (SD) or Median (IQR) | N (%), Mean (SD) or Median (IQR) | N (%), Mean (SD) or Median (IQR) | N (%), Mean (SD) or Median (IQR) | N (%), Mean (SD) or Median (IQR) | N (%), Mean (SD) or Median (IQR) | ||||||||||
| 1 year (OX-NDA) | ZIKV- exposed | 12 (40.0) | 18 (60.0) | X2 = 3.91 p = 0.048 | 0.36 (0.13 – 1.00) | 4 (13.3) | 26 (86.7) | ^^ p = 0.74 | 0.72 (0.18–2.83) | 11 (37.9) | 18 (62.1) | X2 = 3.67 p = 0.06 | 0.37 (0.13–1.03) | - | - | - | - |
| ZIKV- unexposed | 22 (64.7) | 12 (35.3) | 6 (17.6) | 28 (82.4) | 20 (62.5) | 12 (37.5) | - | - | - | - | |||||||
| 3 years (NEPSY-II) | ZIKV- exposed | 11 (37.9) | 18 (62.1) | X2 = 0.00 p = 0.97 | 1.02 (0.33 – 3.11) | 13 (44.8) | 16 (55.2) | X2 = 0.28 p = 0.60 | 0.75 (0.25–2.32) | 11 (40.7) | 16 (59.3) | X2 = 0.44 p = 0.51 | 0.69 (0.23–2.08) | 12 (42.9) | 16 (57.1) | X2 = 1.92 p = 0.17 | 2.40 (0.69–8.39) |
| ZIKV- unexposed | 9 (37.5) | 15 (62.5) | 12 (52.2) | 11 (47.8) | 12 (50.0) | 12 (50.0) | 5 (23.8) | 16 (76.2) | |||||||||
| 4 years (NEPSY-II) | ZIKV- exposed | 14 (48.3) | 15 (51.7) | X2 = 2.65 p = 0.10 | 2.53 (0.82 – 7.86) | 9 (31.0) | 20 (69.0) | X2 = 0.33 p = 0.56 | 0.72 (0.24–2.20) | 13 (44.8) | 16 (55.2) | X2 = 0.23 p = 0.63 | 1.30 (0.44–3.82) | 16 (53.3) | 14 (46.7) | X2 = 2.90 (p = 0.09) | 2.57 (0.86–7.72) |
| ZIKV- unexposed | 7 (26.9) | 19 (73.1) | 10 (38.5) | 16 (61.5) | 10 (38.5) | 16 (61.5) | 8 (30.8) | 18 (69.2) | |||||||||
| Age at Assessment | ZIKV Exposure Group | Visual Acuity (VA; LogMAR) 1 | Contrast Sensitivity (CS; %) 2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | VA Score | Group Comparison for VA Score | Low VA | Group Comparison for VA Score | OR (95% CI) | N | CS Score | Group Comparison for CS Score | Low CS | Group Comparison for CS Score | OR (95% CI) | ||
| Mean (SD) | Test Statistic; p | N (%) | Test Statistic; p | Mean (SD) | Test Statistic; p | N (%) | Test Statistic; p | ||||||
| 3 years | ZIKV-exposed | 22 | 0.26 (0.13) | t = 1.19 p = 0.24 | 4 (18.2%) | ^^ p = 0.69 | 1.55 (0.31–7.89) | 29 | 59.66 (23.76) | t = –0.97 p = 0.33 | 2 (6.9%) | ^^ p = 0.50 | – |
| ZIKV-unexposed | 24 | 0.22 (0.11) | 3 (12.5%) | 25 | 65.33 (18.58) | 0 (0.0%) | |||||||
| 4 years | ZIKV-exposed | 29 | 0.17 (0.08) | t = -2.02 p = 0.051 | – | – | – | 29 | 76.88 (20.94) | t = 1.13 p = 0.26 | 0 (0.0%) | ^^ p = 0.22 | – |
| ZIKV-unexposed | 26 | 0.24 (0.16) | – | 26 | 70.19 (22.87) | 2 (7.7%) | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandes, M.; Evans, R.; Cheng, M.; Landon, B.; Noël, T.; Macpherson, C.; Cudjoe, N.; Burgen, K.S.; Waechter, R.; LaBeaud, A.D.; et al. Does Intra-Uterine Exposure to the Zika Virus Increase Risks of Cognitive Delay at Preschool Ages? Findings from a Zika-Exposed Cohort from Grenada, West Indies. Viruses 2023, 15, 1290. https://doi.org/10.3390/v15061290
Fernandes M, Evans R, Cheng M, Landon B, Noël T, Macpherson C, Cudjoe N, Burgen KS, Waechter R, LaBeaud AD, et al. Does Intra-Uterine Exposure to the Zika Virus Increase Risks of Cognitive Delay at Preschool Ages? Findings from a Zika-Exposed Cohort from Grenada, West Indies. Viruses. 2023; 15(6):1290. https://doi.org/10.3390/v15061290
Chicago/Turabian StyleFernandes, Michelle, Roberta Evans, Mira Cheng, Barbara Landon, Trevor Noël, Calum Macpherson, Nikita Cudjoe, Kemi S. Burgen, Randall Waechter, A. Desiree LaBeaud, and et al. 2023. "Does Intra-Uterine Exposure to the Zika Virus Increase Risks of Cognitive Delay at Preschool Ages? Findings from a Zika-Exposed Cohort from Grenada, West Indies" Viruses 15, no. 6: 1290. https://doi.org/10.3390/v15061290
APA StyleFernandes, M., Evans, R., Cheng, M., Landon, B., Noël, T., Macpherson, C., Cudjoe, N., Burgen, K. S., Waechter, R., LaBeaud, A. D., & Blackmon, K. (2023). Does Intra-Uterine Exposure to the Zika Virus Increase Risks of Cognitive Delay at Preschool Ages? Findings from a Zika-Exposed Cohort from Grenada, West Indies. Viruses, 15(6), 1290. https://doi.org/10.3390/v15061290