
Clinical Differentiation of Severe Fever with Thrombocytopenia Syndrome from Japanese Spotted Fever

 , , , , , , , , ,
, , , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Clinical Data
2.2. Definitions
2.3. Evaluation of the Chest Radiograph and Computed Tomography (CT)
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Study Population
3.2. Patients’ Baseline Characteristics
3.3. Patients’ Clinical Symptoms
3.4. Labortory Findings
3.5. Radiologic Findings
3.6. Outcomes and Treatments
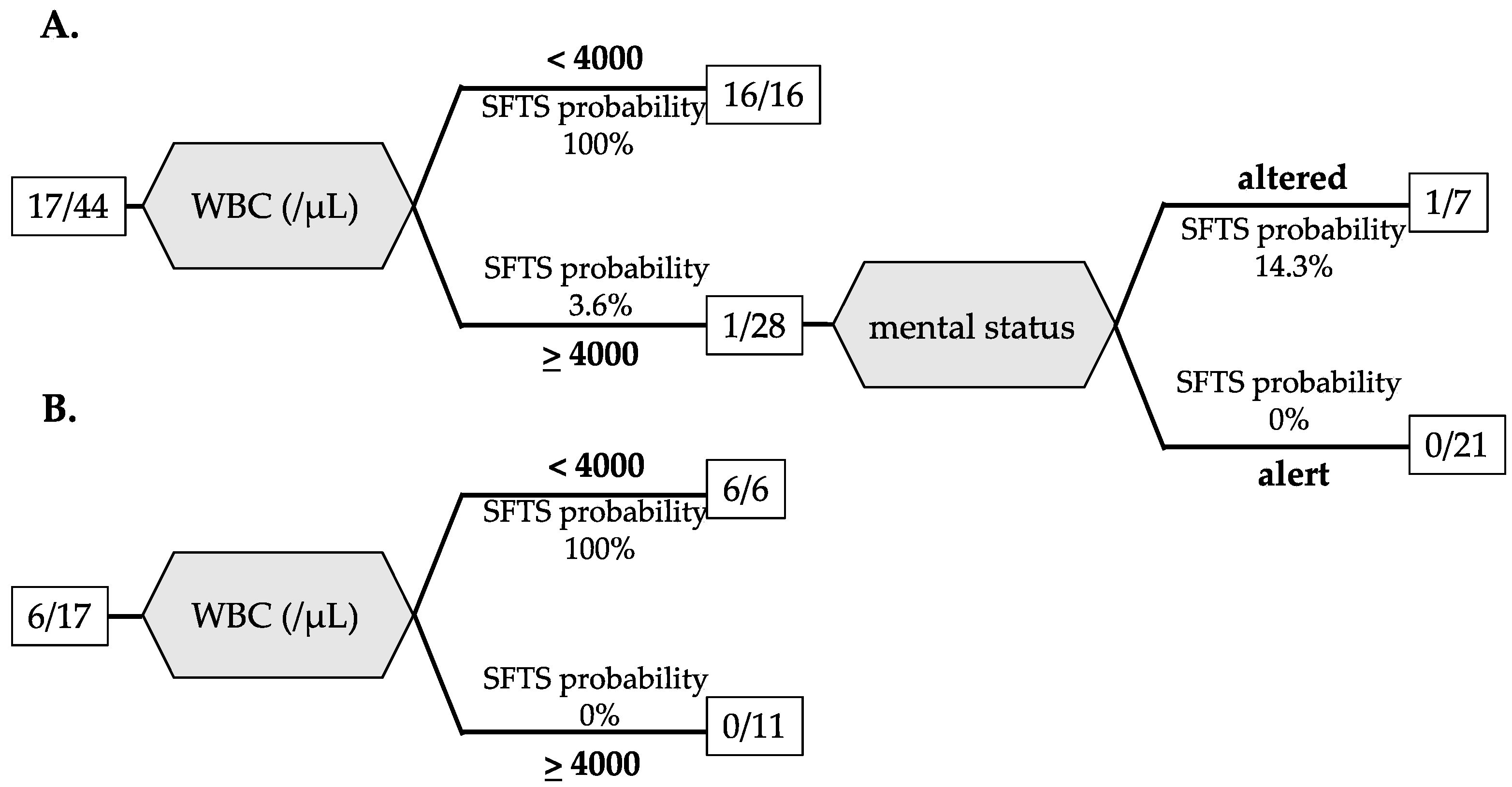
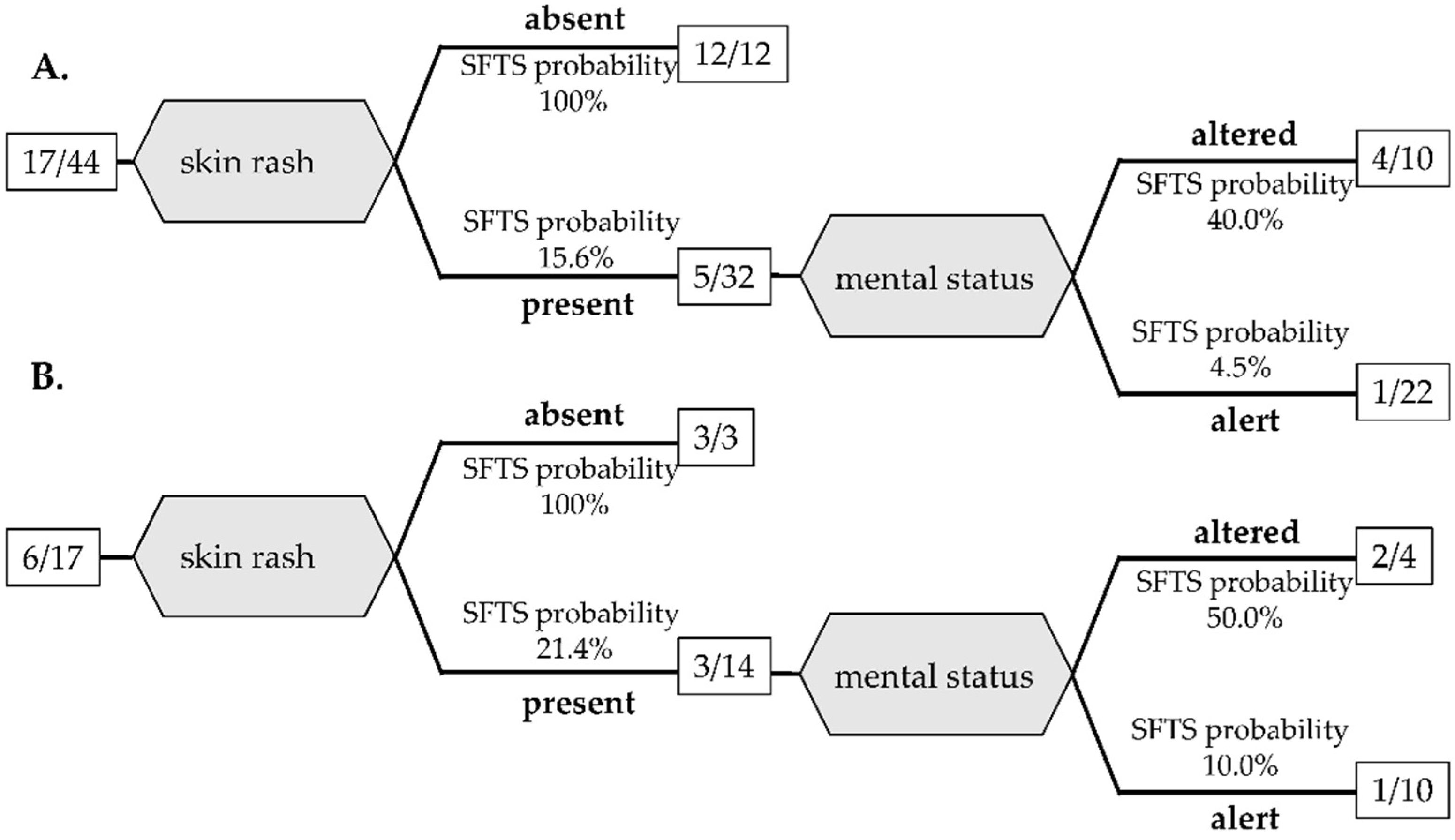
3.7. Decision Tree Analysis for Differentiation between JSF and SFTS
4. Discussion

{kind=link}
{kind=link}
| Studies | Study Patients | Differentiation Model | Results |
|---|---|---|---|
| Kim MC et al., 2018. [47] | SFTS (n = 21) scrub typhus (n = 98) | Scoring system (score > 1: SFTS) using 4 factors altered mental status leukopenia (WBC < 4000 /μL) prolonged APTT (>35 s) normal CRP (≤1.0 mg/dL) | score > 1 100% sensitivity 97% specificity AUC 0.995 |
| Sul H et al., 2022. [48] | SFTS (n = 183) scrub typhus (n = 173) | Scoring system (score > 1: SFTS) using 4 factors leukopenia (WBC < 4000 /μL) prolonged APTT (>40 s), normal CRP (≤3.0 mg/dL) elevated CK level (>1000 IU/L) | score > 1 97% sensitivity 98% specificity AUC 0.992 |
| Kawaguchi T et al., 2020. [8] | SFTS (n = 41) JSF (n = 40) | CRP ≤ 1.0 mg/dL | 95% sensitivity 97% specificity AUC 0.96 |
| Heo DH et al., 2020. [49] | SFTS (n = 35) other endemic zoonoses (n = 49) | Scoring system (score ≥ 2: SFTS) using 4 factors neurologic symptom diarrhea leukopenia (WBC < 4000 /μL) normal CRP (<0.5 mg/dL) | score ≥ 2 82.9% sensitivity 95.9% specificity AUC 0.950 |
| Our study | SFTS (n = 23) JSF (n = 38) | Decision tree analysis Pattern A: leukopenia (WBC < 4000 /μL) altered mental status | 100% sensitivity 100% specificity AUC 1.000 |
| Pattern B: absent of skin rash altered mental status | 71.4% sensitivity 90.0% specificity AUC 0.871 |
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yu, X.J.; Liang, M.F.; Zhang, S.Y.; Liu, Y.; Li, J.D.; Sun, Y.L.; Zhang, L.; Zhang, Q.F.; Popov, V.L.; Li, C.; et al. Fever with thrombocytopenia associated with a novel bunyavirus in China. N. Engl. J. Med. 2011, 364, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, J.H.; Adkins, S.; Alioto, D.; Alkhovsky, S.V.; Amarasinghe, G.K.; Anthony, S.J.; Avsic-Zupanc, T.; Ayllon, M.A.; Bahl, J.; Balkema-Buschmann, A.; et al. 2020 taxonomic update for phylum Negarnaviricota (Riboviria: Orthornavirae), including the large orders Bunyavirales and Mononegavirales. Arch. Virol. 2020, 165, 3023–3072. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; He, B.; Huang, S.-Y.; Wei, F.; Zhu, X.-Q. Severe fever with thrombocytopenia syndrome, an emerging tick-borne zoonosis. Lancet Infect. Dis. 2014, 14, 763–772. [Google Scholar] [CrossRef]
- Saijo, M. Pathophysiology of severe fever with thrombocytopenia syndrome and development of specific antiviral therapy. J. Infect. Chemother. 2018, 24, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Zhan, J.; Wang, Q.; Cheng, J.; Hu, B.; Li, J.; Zhan, F.; Song, Y.; Guo, D. Current status of severe fever with thrombocytopenia syndrome in China. Virol. Sin. 2017, 32, 51–62. [Google Scholar] [CrossRef]
- Choi, S.J.; Park, S.W.; Bae, I.G.; Kim, S.H.; Ryu, S.Y.; Kim, H.A.; Jang, H.C.; Hur, J.; Jun, J.B.; Jung, Y.; et al. Severe Fever with Thrombocytopenia Syndrome in South Korea, 2013–2015. PLoS Negl. Trop. Dis. 2016, 10, e0005264. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Kato, H.; Yamagishi, T.; Shimada, T.; Matsui, T.; Yoshikawa, T.; Kurosu, T.; Shimojima, M.; Morikawa, S.; Hasegawa, H.; et al. Severe Fever with Thrombocytopenia Syndrome, Japan, 2013–2017. Emerg. Infect. Dis. 2020, 26, 692–699. [Google Scholar] [CrossRef]
- Kawaguchi, T.; Umekita, K.; Yamanaka, A.; Hara, S.; Yamaguchi, T.; Inoue, E.; Okayama, A. Impact of C-Reactive Protein Levels on Differentiating of Severe Fever With Thrombocytopenia Syndrome From Japanese Spotted Fever. Open Forum Infect. Dis. 2020, 7, ofaa473. [Google Scholar] [CrossRef]
- National Institute of Infectious Diseases (NIID). Severe Fever With Thrombocytopenia Syndrome(SFTS). Available online: https://www.niid.go.jp/niid/ja/sfts/3143-sfts.html (accessed on 29 June 2022). (In Japanese)
- Parola, P.; Paddock, C.D.; Raoult, D. Tick-borne rickettsioses around the world: Emerging diseases challenging old concepts. Clin. Microbiol. Rev. 2005, 18, 719–756. [Google Scholar] [CrossRef]
- Mahara, F. Japanese spotted fever: Report of 31 cases and review of the literature. Emerg. Infect. Dis. 1997, 3, 105–111. [Google Scholar] [CrossRef]
- Chung, M.H.; Lee, S.H.; Kim, M.J.; Lee, J.H.; Kim, E.S.; Lee, J.S.; Kim, M.K.; Park, M.Y.; Kang, J.S. Japanese spotted fever, South Korea. Emerg. Infect. Dis. 2006, 12, 1122–1124. [Google Scholar] [CrossRef]
- Li, J.; Hu, W.; Wu, T.; Li, H.B.; Hu, W.; Sun, Y.; Chen, Z.; Shi, Y.; Zong, J.; Latif, A.; et al. Japanese Spotted Fever in Eastern China, 2013. Emerg. Infect. Dis. 2018, 24, 2107–2109. [Google Scholar] [CrossRef]
- Takada, N.; Fujita, H.; Kawabata, H.; Ando, S.; Sakata, A.; Takano, A.; Chaithong, U. Spotted fever group Rickettsia sp. closely related to Rickettsia japonica, Thailand. Emerg. Infect. Dis. 2009, 15, 610–611. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.R.; Han, H.J.; Han, F.J.; Zhao, F.M.; Zhang, Z.T.; Xue, Z.F.; Ma, D.Q.; Qi, R.; Zhao, M.; Wang, L.J.; et al. Rickettsia Japonica and Novel Rickettsia Species in Ticks, China. Emerg. Infect. Dis. 2019, 25, 992–995. [Google Scholar] [CrossRef] [PubMed]
- Yamaji, K.; Aonuma, H.; Kanuka, H. Distribution of tick-borne diseases in Japan: Past patterns and implications for the future. J. Infect. Chemother. 2018, 24, 499–504. [Google Scholar] [CrossRef]
- National Institute of Infectious Diseases (NIID), Japanese spotted fever 1999–2019. Infect. Agent Surveill. Rep. 2020, 41, 133–135.
- Sakabe, S.; Tanaka, H.; Nakanishi, Y.; Toyoshima, H. The clinical course of 239 cases of Japanese spotted fever in Ise Red Cross Hospital, 2006–2019. J. Infect. Chemother. 2022, 28, 211–216. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Infectious Diseases (NIID). Scrub typhus and Japanese spotted fever in Japan 2007–2016. Infect. Agent Surveill. Rep. 2017, 38, 109–112. [Google Scholar]
- National Institute of Infectious Diseases (NIID). Infectious Agent Surveillance Report. Reporting Criteria of Severe Fever with Thrombocytopenia Syndrome (SFTS) Report. Available online: https://www.niid.go.jp/niid/images/iasr/35/408/de4081.pdf (accessed on 29 June 2022).
- National Institute of Infectious Diseases (NIID). Infectious Agent Surveillance Report. Reporting Criteria for Japanese Spotted Fever. Available online: https://www.niid.go.jp/niid/images/iasr/38/448/de4482.pdf (accessed on 29 June 2022).
- Li, Z.; Bao, C.; Hu, J.; Liu, W.; Wang, X.; Zhang, L.; Ji, Z.; Feng, Z.; Li, L.; Shen, A.; et al. Ecology of the Tick-Borne Phlebovirus Causing Severe Fever with Thrombocytopenia Syndrome in an Endemic Area of China. PLoS Negl. Trop. Dis. 2016, 10, e0004574. [Google Scholar] [CrossRef]
- Luo, L.M.; Zhao, L.; Wen, H.L.; Zhang, Z.T.; Liu, J.W.; Fang, L.Z.; Xue, Z.F.; Ma, D.Q.; Zhang, X.S.; Ding, S.J.; et al. Haemaphysalis Longicornis Ticks as Reservoir and Vector of Severe Fever with Thrombocytopenia Syndrome Virus in China. Emerg. Infect. Dis. 2015, 21, 1770–1776. [Google Scholar] [CrossRef]
- Uchida, T.; Yan, Y.; Kitaoka, S. Detection of Rickettsia japonica in Haemaphysalis longicornis ticks by restriction fragment length polymorphism of PCR product. J. Clin. Microbiol. 1995, 33, 824–828. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Heo, S.T.; Oh, H.; Oh, S.; Lee, K.H.; Yoo, J.R. Prognostic Factors of Severe Fever with Thrombocytopenia Syndrome in South Korea. Viruses 2020, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Lu, Q.-B.; Xing, B.; Zhang, S.-F.; Liu, K.; Du, J.; Li, X.-K.; Cui, N.; Yang, Z.-D.; Wang, L.-Y.; et al. Epidemiological and clinical features of laboratory-diagnosed severe fever with thrombocytopenia syndrome in China, 2011–2017: A prospective observational study. Lancet Infect. Dis. 2018, 18, 1127–1137. [Google Scholar] [CrossRef]
- Gai, Z.; Liang, M.; Zhang, Y.; Zhang, S.; Jin, C.; Wang, S.W.; Sun, L.; Zhou, N.; Zhang, Q.; Sun, Y.; et al. Person-to-person transmission of severe fever with thrombocytopenia syndrome bunyavirus through blood contact. Clin. Infect. Dis. 2012, 54, 249–252. [Google Scholar] [CrossRef]
- Kim, W.Y.; Choi, W.; Park, S.W.; Wang, E.B.; Lee, W.J.; Jee, Y.; Lim, K.S.; Lee, H.J.; Kim, S.M.; Lee, S.O.; et al. Nosocomial transmission of severe fever with thrombocytopenia syndrome in Korea. Clin. Infect. Dis. 2015, 60, 1681–1683. [Google Scholar] [CrossRef]
- Yoo, J.R.; Lee, K.H.; Heo, S.T. Surveillance results for family members of patients with severe fever with thrombocytopenia syndrome. Zoonoses Public Health 2018, 65, 903–907. [Google Scholar] [CrossRef]
- Koga, S.; Takazono, T.; Ando, T.; Hayasaka, D.; Tashiro, M.; Saijo, T.; Kurihara, S.; Sekino, M.; Yamamoto, K.; Imamura, Y.; et al. Severe Fever with Thrombocytopenia Syndrome Virus RNA in Semen, Japan. Emerg. Infect. Dis. 2019, 25, 2127–2128. [Google Scholar] [CrossRef]
- Ashizawa, H.; Yamamoto, K.; Ashizawa, N.; Takeda, K.; Iwanaga, N.; Takazono, T.; Sakamoto, N.; Sumiyoshi, M.; Ide, S.; Umemura, A.; et al. Associations between Chest CT Abnormalities and Clinical Features in Patients with the Severe Fever with Thrombocytopenia Syndrome. Viruses 2022, 14, 279. [Google Scholar] [CrossRef]
- Robinson, M.T.; Satjanadumrong, J.; Hughes, T.; Stenos, J.; Blacksell, S.D. Diagnosis of spotted fever group Rickettsia infections: The Asian perspective. Epidemiol. Infect. 2019, 147, e286. [Google Scholar] [CrossRef]
- Yumoto, T.; Naito, H.; Yorifuji, T.; Aokage, T.; Fujisaki, N.; Nakao, A. Association of Japan Coma Scale score on hospital arrival with in-hospital mortality among trauma patients. BMC Emerg. Med. 2019, 19, 65. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N.; Group, K.A.G.W. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Astor, B.C.; Fox, C.H.; Isakova, T.; Lash, J.P.; Peralta, C.A.; Kurella Tamura, M.; Feldman, H.I. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am. J. Kidney Dis. 2014, 63, 713–735. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Saitoh, D.; Ogura, H.; Fujishima, S.; Mayumi, T.; Araki, T.; Ikeda, H.; Kotani, J.; Kushimoto, S.; Miki, Y.; et al. A multicenter, prospective validation study of the Japanese Association for Acute Medicine disseminated intravascular coagulation scoring system in patients with severe sepsis. Crit. Care 2013, 17, R111. [Google Scholar] [CrossRef]
- Henter, J.I.; Horne, A.; Arico, M.; Egeler, R.M.; Filipovich, A.H.; Imashuku, S.; Ladisch, S.; McClain, K.; Webb, D.; Winiarski, J.; et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr. Blood Cancer 2007, 48, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Suemori, K.; Saijo, M.; Yamanaka, A.; Himeji, D.; Kawamura, M.; Haku, T.; Hidaka, M.; Kamikokuryo, C.; Kakihana, Y.; Azuma, T.; et al. A multicenter non-randomized, uncontrolled single arm trial for evaluation of the efficacy and the safety of the treatment with favipiravir for patients with severe fever with thrombocytopenia syndrome. PLoS Negl. Trop. Dis. 2021, 15, e0009103. [Google Scholar] [CrossRef]
- Satoh, M.; Akashi, S.; Ogawa, M.; Wakeyama, T.; Ogawa, H.; Fukuma, A.; Taniguchi, S.; Tani, H.; Kurosu, T.; Fukushi, S.; et al. Retrospective survey of severe fever with thrombocytopenia syndrome in patients with suspected rickettsiosis in Japan. J. Infect. Chemother. 2017, 23, 45–50. [Google Scholar] [CrossRef]
- Bae, S.; Hwang, H.J.; Kim, M.Y.; Kim, M.J.; Chong, Y.P.; Lee, S.O.; Choi, S.H.; Kim, Y.S.; Woo, J.H.; Kim, S.H. Invasive Pulmonary Aspergillosis in Patients With Severe Fever With Thrombocytopenia Syndrome. Clin. Infect. Dis. 2020, 70, 1491–1494. [Google Scholar] [CrossRef]
- Matsuura, H. Japanese spotted fever and rickettsial pneumonia. QJM Int. J. Med. 2021, 114, 261–262. [Google Scholar] [CrossRef]
- Kodama, K.; Noguchi, T.; Chikahira, Y. Japanese spotted fever complicated by acute respiratory failure. Kansenshogaku Zasshi 2000, 74, 162–165. (In Japanese) [Google Scholar] [CrossRef]
- Sando, E.; Suzuki, M.; Katoh, S.; Fujita, H.; Taira, M.; Yaegashi, M.; Ariyoshi, K. Distinguishing Japanese Spotted Fever and Scrub Typhus, Central Japan, 2004–2015. Emerg. Infect. Dis. 2018, 24, 1633–1641. [Google Scholar] [CrossRef]
- Kinoshita, H.; Arima, Y.; Shigematsu, M.; Sunagawa, T.; Saijo, M.; Oishi, K.; Ando, S. Descriptive epidemiology of rickettsial infections in Japan: Scrub typhus and Japanese spotted fever, 2007–2016. Int. J. Infect. Dis. 2021, 105, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Nagasaki Prefectural Goverment. Prevention of Tick-Borne Infections. Available online: https://www.pref.nagasaki.jp/object/kenkaranooshirase/oshirase/299534.html (accessed on 29 June 2022). (In Japanese)
- Nagasaki Prefectural Goverment. Outbreak of Severe Fever with Thrombocytopenia Syndrome (SFTS) Patients. Available online: https://www.pref.nagasaki.jp/shared/uploads/2021/07/1625713522.pdf (accessed on 29 June 2022). (In Japanese)
- Kim, M.C.; Chong, Y.P.; Lee, S.O.; Choi, S.H.; Kim, Y.S.; Woo, J.H.; Kim, S.H. Differentiation of Severe Fever With Thrombocytopenia Syndrome From Scrub Typhus. Clin. Infect. Dis. 2018, 66, 1621–1624. [Google Scholar] [CrossRef] [PubMed]
- Sul, H.; Yun, N.R.; Kim, D.-M.; Kim, Y.K.; Kim, J.; Hur, J.; Jung, S.I.; Ryu, S.Y.; Lee, J.Y.; Huh, K.; et al. Development of a Scoring System to Differentiate Severe Fever with Thrombocytopenia Syndrome from Scrub Typhus. Viruses 2022, 14, 1093. [Google Scholar] [CrossRef] [PubMed]
- Heo, D.H.; Kang, Y.M.; Song, K.H.; Seo, J.W.; Kim, J.H.; Chun, J.Y.; Jun, K.I.; Kang, C.K.; Moon, S.M.; Choe, P.G.; et al. Clinical Score System to Differentiate Severe Fever with Thrombocytopenia Syndrome Patients from Patients with Scrub Typhus or Hemorrhagic Fever with Renal Syndrome in Korea. J. Korean Med. Sci. 2020, 35, e77. [Google Scholar] [CrossRef] [PubMed]


| All (n = 61) | SFTS (n = 23) | JSF (n = 38) | p Value | |
|---|---|---|---|---|
| Age (years) | 69.5 ± 11.0 | 70.6 ± 10.3 | 68.8 ± 11.5 | 0.536 |
| Male Gender | 33 (54.1) | 15 (65.2) | 18 (47.4) | 0.197 |
| Farmers, hunters, living or working in wooded and hilly areas | 21/58 (36.2) | 11/22 (50.0) | 10/36 (27.8) | 0.101 |
| Underlying diseases | ||||
| Hypertension | 30 (49.2) | 11 (47.8) | 19 (50.0) | 1.000 |
| Cardiovascular diseases | 9 (14.8) | 4 (17.4) | 5 (13.2) | 0.718 |
| Chronic kidney diseases | 6/57 (10.5) | 1/21 (4.8) | 5/36 (13.9) | 0.397 |
| Hemodialysis | 1 (1.6) | 1 (4.4) | 0 | 0.377 |
| Chronic liver diseases | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Diabetes mellitus | 9 (14.8) | 5 (21.7) | 4 (10.5) | 0.278 |
| Solid cancer | 7 (11.5) | 3 (13.0) | 4 (10.5) | 1.000 |
| Autoimmune disease | 1 (1.6) | 1 (4.4) | 0 (0.0) | 0.377 |
| Immunosuppressant use | 2 (3.3) | 2 (8.7) | 0 (0.0) | 0.138 |
| Seasonal incidence | 0.047 | |||
| Spring (March–May) | 20 (32.8) | 11 (47.8) | 9 (23.7) | |
| Summer (June–August) | 26 (42.6) | 10 (43.5) | 16 (42.1) | |
| Autumn (September–November) | 15 (24.6) | 2 (8.7) | 13 (34.2) |
| All (n = 61) | SFTS (n = 23) | JSF (n = 38) | p Value | |
|---|---|---|---|---|
| Time from onset to admission (days) | 5.7 ± 3.5 | 5.3 ± 4.3 | 5.9 ± 2.9 | 0.148 |
| General Symptoms | ||||
| Fatigue | 28/60 (46.7) | 12/22 (54.6) | 16/38 (42.1) | 0.425 |
| Headache | 13/60 (21.7) | 5/22 (22.7) | 8/38 (21.1) | 1.000 |
| Altered mental status | 22 (36.1) | 14 (60.9) | 8 (21.1) | 0.003 † |
| Myalgia | 4/60 (6.7) | 1/22 (4.6) | 3/38 (7.9) | 1.000 |
| Respiratory symptoms | ||||
| Cough | 3 (4.9) | 1 (4.4) | 2 (5.3) | 1.000 |
| Sputum | 2 (3.3) | 1 (4.4) | 1 (2.6) | 1.000 |
| Dyspnea | 11 (18.0) | 8 (34.8) | 3 (7.9) | 0.014 |
| Rales | 6 (9.8) | 3 (13.0) | 3 (7.9) | 0.664 |
| Gastrointestinal symptoms | ||||
| Nausea | 7/59 (11.9) | 5/22 (22.7) | 2/37 (5.4) | 0.090 |
| Anorexia | 29/59 (49.2) | 10/22 (45.5) | 19/37 (51.4) | 0.789 |
| Diarrhea | 15/59 (25.4) | 11/21 (52.4) | 4/38 (10.5) | 0.001 † |
| Skin and other symptoms | ||||
| Skin rash | 46 (75.4) | 8 (34.8) | 38 (100.0) | <0.0001 † |
| Tick bite | 41/57 (71.9) | 9/21 (42.9) | 32/36 (88.9) | 0.001 † |
| Lymphadenopathy | 16/60 (26.7) | 10/22 (45.5) | 6/38 (15.8) | 0.017 |
| Vital signs | ||||
| Body temperature (°C) | 38.5 ± 0.9 | 38.2 ± 0.9 | 38.6 ± 0.9 | 0.127 |
| Systolic blood pressure(mmHg) | 116.7 ± 21.7 | 126.1 ± 19.1 | 110.9 ± 21.3 | 0.007 |
| Heart rate (/min) | 90.8 ± 17.9 | 84.0 ± 15.7 | 95.0 ± 18.2 | 0.020 |
| Respiratory rate (/min) * | 20.1 ± 6.54 | 20.0 ± 6.4 | 20.2 ± 6.8 | 0.933 |
| SpO2/FiO2 ratio | 427.9 ± 73.7 | 414.3 ± 83.3 | 436.7 ± 66.6 | 0.888 |
| qSOFA score * | 1.1 ± 0.9 | 1.1 ± 0.6 | 1.1 ± 1.0 | 0.936 |
| Reference Value | All (n = 61) | SFTS (n = 23) | JSF (n = 38) | p Value | |
|---|---|---|---|---|---|
| Complete blood count | |||||
| WBCs (/μL) | 3300–8600 | 5286.6 ± 3514.4 | 1821.3 ± 1028.8 | 7383.9 ± 2723.4 | <0.0001 † |
| Neutrophils (/μL) | 1830–7250 | 4265.0 ± 3246.0 | 1190.8 ± 833.0 | 6176.0 ± 2655.8 | <0.0001 † |
| Lymphocytes (/μL) | 1500–4000 | 701.7 ± 556.4 | 460.5 ± 281.3 | 851.7 ± 631.5 | 0.002 |
| Atypical lymphocytes (%) | 0 | 0.9 ± 2.3 | 2.0 ± 3.4 | 0.2 ± 0.5 | 0.001 † |
| Platelets (×103/μL) | 158–348 | 92.4 ± 56.9 | 58.4 ± 40.1 | 113.1 ± 56.0 | 0.001 † |
| Hb (g/dL) | 13.7–16.8 | 13.7 ± 1.7 | 14.0 ± 2.0 | 13.5 ± 1.5 | 0.245 |
| Biochemical examination | |||||
| CRP (mg/dL) | <0.17 | 8.0 ± 8.2 | 0.8 ± 1.2 | 12.3 ± 7.5 | <0.0001 † |
| PCT (ng/mL) * | <0.05 | 1.3 ± 2.4 | 0.3 ± 0.3 | 2.7 ± 3.3 | 0.005 |
| sIL-2R (IU/L) * | 127–582 | 2073.7 ± 1754.8 | 1451.6 ± 631.8 | 4521.0 ± 2755.7 | 0.017 |
| Ferritin (ng/mL) * | 40–465 | 6927.7 ± 9422.6 | 10,205.6 ± 11,311.8 | 2389.1 ± 1502.4 | 0.004 |
| IgG (mg/dL) * | 870–1700 | 1055.5 ± 296.3 | 1181.5 ± 307.2 | 906.7 ± 209.2 | 0.020 |
| Alb (g/dL) | 4.1–5.1 | 3.2 ± 0.6 | 3.3 ± 0.5 | 3.1 ± 0.7 | 0.300 |
| AST (IU/L) | 13–40 | 179.2 ± 226.1 | 328.3 ± 308.2 | 88.9 ± 65.0 | <0.0001 † |
| ALT (IU/L) | 10–42 | 76.5 ± 64.0 | 113.5 ± 83.5 | 54.2 ± 33.7 | 0.001 † |
| LDH (IU/L) | 124–222 | 544.8 ± 352.3 | 801.5 ± 431.9 | 389.4 ± 156.9 | 0.001 † |
| CK (IU/L) | 59–248 | 1266.4 ± 2938.7 | 2447.4 ± 4331.0 | 524.0 ± 1081.1 | 0.004 |
| BUN (mg/dL) | 8–20 | 25.5 ± 19.4 | 26.1 ± 17.0 | 25.2 ± 20.9 | 0.857 |
| Cre (mg/dL) | 0.65–1.07 | 1.1 ± 0.7 | 1.0 ± 0.6 | 1.2 ± 0.8 | 0.459 |
| Acute Kidney Injury | 24/60 (40.0) | 10/22 (45.5) | 14 / 38 (36.8) | 0.589 | |
| Na (mEq/L) | 138–145 | 132.8 ± 5.5 | 132.5 ± 6.2 | 132.9 ± 5.1 | 0.790 |
| K (mEq/L) | 3.6–4.8 | 3.9 ± 0.5 | 4.0 ± 0.6 | 3.9 ± 0.5 | 0.575 |
| Cl (mEq/L) | 101–108 | 98.8 ± 6.2 | 99.7 ± 6.5 | 98.3 ± 6.0 | 0.370 |
| Blood coagulation test | |||||
| APTT (s) | 25.2–34.4 | 41.2 ± 13.3 | 48.0 ± 14.9 | 36.9 ± 10.4 | 0.001 † |
| PT-INR | 0.85–1.22 | 1.1 ± 0.1 | 1.1 ± 0.1 | 1.1 ± 0.1 | 0.519 |
| D-dimer (μg/mL) | <1.0 | 16.1 ± 18.3 | 14.4 ± 14.7 | 17.1 ± 20.2 | 0.601 |
| FDP (μg/mL) | <5 | 33.8 ± 41.8 | 28.5 ± 29.2 | 37.1 ± 48.1 | 0.563 |
| Fibrinogen * (mg/dL) | 168–329 | 320.8 ± 133.4 | 212.7 ± 33.4 | 382.6 ± 129.8 | 0.001 † |
| DIC score | 0 | 3.4 ± 2.5 | 4.1 ± 2.2 | 3.0 ± 2.5 | 0.095 |
| Urinalysis | |||||
| Proteinuria | - | 45/52 (86.5) | 21/22 (95.5) | 24/30 (80.0) | 0.217 |
| Hematuria | - | 41/52 (78.9) | 21/22 (95.5) | 20/30 (66.7) | 0.016 |
| All (n = 39) | SFTS (n = 22) | JSF (n = 17) | p Value | |
|---|---|---|---|---|
| Time from symptoms onset to chest CT, days ± SD | 5.6 ± 3.5 | 5.8 ± 4.2 | 5.3 ± 2.3 | 0.942 |
| Time from admission to chest CT, days ± SD | 0.1 ± 0.3 | 0.2 ± 0.4 | 0.0 ± 0.0 | 0.071 |
| Abnormal chest CT findings | 32 (82.1) | 19 (86.4) | 13 (76.5) | 0.677 |
| Consolidation | 8 (20.5) | 5 (22.7) | 3 (17.7) | 1.000 |
| Ground glass opacity (GGO) | 21 (53.9) | 12 (54.6) | 9 (52.9) | 1.000 |
| Interstitial septal thickening | 26 (66.7) | 15 (68.2) | 11 (64.7) | 1.000 |
| Centrilobular nodule | 10 (25.6) | 8 (36.4) | 2 (11.8) | 0.140 |
| Bronchial wall thickening | 9 (23.1) | 8 (36.4) | 1 (5.9) | 0.052 |
| Cardiomegaly | 19 (32.8) | 7 (31.8) | 12 (33.3) | 1.000 |
| Pleural effusion | 15 (38.5) | 5 (22.7) | 10 (58.8) | 0.045 |
| Pericardial effusion | 6 (15.4) | 4 (18.2) | 2 (11.8) | 0.679 |
| Mediastinal lymph node enlargement | 3 (7.7) | 3 (13.6) | 0 (0.0) | 0.243 |
| Hepatomegaly | 12 (30.8) | 6 (27.3) | 6 (35.3) | 0.730 |
| Splenomegaly | 5 (12.8) | 3 (13.6) | 2 (11.8) | 1.000 |
| Training Cohort (n = 44) | Validation Cohort (n = 17) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| SFTS (n = 17) | JSF (n = 27) | SFTS (n = 6) | JSF (n = 11) | AUC | Sensitivity | Specificity | PPV | NPV | p Value | |
| Altered mental status | 10 (58.8) | 6 (22.2) | 4 (66.7) | 2(18.2) | 0.742 | 0.667 | 0.818 | 0.667 | 0.818 | 0.045 |
| Diarrhea | 9/15 (60.0) | 2 (7.4) | 2 (33.3) | 2 (18.2) | 0.576 | 0.333 | 0.818 | 0.500 | 0.692 | 0.488 |
| Absent of skin rash | 12 (70.6) | 0 (0.0) | 3 (50.0) | 0 (0.0) | 0.750 | 0.500 | 1.000 | 1.000 | 0.786 | 0.006 |
| WBCs < 4000 (/μL) | 16 (94.1) | 0 (0.0) | 6 (100.0) | 0 (0.0) | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | <0.0001 |
| Neutrophils < 2042(/μL) | 15 (88.2) | 0 (0.0) | 6 (100.0) | 0 (0.0) | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | <0.0001 |
| Atypical lymphocyte ≥ 2% | 5 (29.4) | 1 (3.9) | 3 (50.0) | 1 (9.1) | 0.750 | 0.500 | 1.000 | 1.000 | 0.786 | 0.006 |
| Platelets < 64 (×103/μL) | 10 (58.8) | 4 (14.8) | 6 (100.0) | 4 (36.5) | 0.818 | 1.000 | 0.636 | 0.600 | 1.000 | 0.003 |
| AST ≥ 261 (IU/L) | 9 (52.9) | 0 (0.0) | 4 (66.7) | 2 (18.2) | 0.742 | 0.667 | 0.818 | 0.667 | 0.818 | 0.045 |
| ALT ≥ 97 (IU/L) | 8 (47.1) | 2 (7.4) | 4 (66.7) | 3 (27.3) | 0.697 | 0.667 | 0.727 | 0.571 | 0.800 | 0.113 |
| LDH ≥ 731 (IU/L) | 10 (58.8) | 0 (0.0) | 4 (66.7) | 2 (18.2) | 0.742 | 0.667 | 0.818 | 0.667 | 0.818 | 0.045 |
| CRP < 4.17 (mg/dL) | 17 (100.0) | 2 (7.4) | 5 (83.4) | 1 (9.1) | 0.871 | 0.833 | 0.909 | 0.833 | 0.909 | 0.002 |
| APTT ≥ 51.4 (s) | 6 (35.3) | 0 (0.0) | 2 (33.3) | 1/10(10.0) | 0.617 | 0.333 | 0.900 | 0.667 | 0.692 | 0.254 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakada, N.; Yamamoto, K.; Tanaka, M.; Ashizawa, H.; Yoshida, M.; Umemura, A.; Fukuda, Y.; Katoh, S.; Sumiyoshi, M.; Mihara, S.; et al. Clinical Differentiation of Severe Fever with Thrombocytopenia Syndrome from Japanese Spotted Fever. Viruses 2022, 14, 1807. https://doi.org/10.3390/v14081807
Nakada N, Yamamoto K, Tanaka M, Ashizawa H, Yoshida M, Umemura A, Fukuda Y, Katoh S, Sumiyoshi M, Mihara S, et al. Clinical Differentiation of Severe Fever with Thrombocytopenia Syndrome from Japanese Spotted Fever. Viruses. 2022; 14(8):1807. https://doi.org/10.3390/v14081807
Chicago/Turabian StyleNakada, Nana, Kazuko Yamamoto, Moe Tanaka, Hiroki Ashizawa, Masataka Yoshida, Asuka Umemura, Yuichi Fukuda, Shungo Katoh, Makoto Sumiyoshi, Satoshi Mihara, and et al. 2022. "Clinical Differentiation of Severe Fever with Thrombocytopenia Syndrome from Japanese Spotted Fever" Viruses 14, no. 8: 1807. https://doi.org/10.3390/v14081807
APA StyleNakada, N., Yamamoto, K., Tanaka, M., Ashizawa, H., Yoshida, M., Umemura, A., Fukuda, Y., Katoh, S., Sumiyoshi, M., Mihara, S., Kobayashi, T., Ito, Y., Ashizawa, N., Takeda, K., Ide, S., Iwanaga, N., Takazono, T., Tashiro, M., Tanaka, T., ... Mukae, H. (2022). Clinical Differentiation of Severe Fever with Thrombocytopenia Syndrome from Japanese Spotted Fever. Viruses, 14(8), 1807. https://doi.org/10.3390/v14081807