1. Introduction
Hepatitis C virus (HCV) is a hepatotropic RNA virus and a major cause of chronic hepatitis C (CHC) worldwide [
1]. The importance of interactions between HCV virions and hepatocytes is significant for a better understanding of immunoreactions and immunopathogenesis in HCV infection [
2]. Treatment of HCV infection is based on the use of direct-acting antivirals (DAA) that inhibit different phases of the HCV replication cycle and allow viral eradication in more than 95% of infected individuals [
3]. In general, DAAs can be divided into three major classes based on their molecular targets: the nonstructural protein 3/4A (NS3/4A) protease inhibitors, NS5A inhibitors and NS5B polymerase inhibitors, the combination of which is used for CHC treatment [
4]. Replication of HCV in hepatocytes and the inflammatory response of the immune system during chronic infection activate numerous mechanisms that lead to fibrosis, cirrhosis and ultimately hepatocellular carcinoma (HCC), as a complication of CHC [
5].
Chronic HCV infection is characterized by direct modulation of signaling and metabolic pathways mediated by viral proteins, as well as the induction of antiviral immune responses which lead to chronic inflammation and the development of liver fibrogenesis [
6]. Liver fibrosis is a complex pathological process that represents the accumulation of connective tissue in the liver in response to hepatocellular damage that occurs due to strong formation or insufficient degradation of the extracellular matrix (ECM). A major starting event in the development of fibrosis is the activation of liver stellate cells (HSC), which are the primary source of ECM. In response to cell injury, ECM activation mediates various biological response modifiers, including reactive species oxygen, lipid peroxides, inflammatory cytokines and growth factors [
7,
8]. Despite evidence of fibrosis reversibility after HCV eradication, exact mechanisms are currently unknown [
8].
Cytokines are glycoproteins that mediate intercellular interactions and promote proliferation, differentiation, growth or apoptosis of target cells, regulate the host immune response and play an important role in the pathogenesis of various diseases [
9]. Inflammatory responses caused by HCV infection can cause progressive liver disease. Some inflammatory cytokines may serve as biomarkers for monitoring disease progression and treatment outcome in patients with CHC [
10]. The pathogenesis of HCV-infected patients is complicated and includes classical pathogen recognition, inflammatory activation, intrahepatic inflammatory cascade response, oxidative stress and endoplasmic reticulum stress. Persistent replication of HCV in hepatocytes leads to uncontrolled inflammation. Cytokines, as inflammatory agents, can cause inflammation in the liver leading to liver tissue damage and progression of liver disease [
7]. The interaction of liver parenchymal, non-parenchymal cells and immune cells migrating to the liver during CHC is mediated by biological response modulators such as cytokines and growth factors. Both hepatic parenchymal and nonparenchymal cells are involved in the initiation and progression of liver fibrosis and cirrhosis [
11].
Growth factors play an important role in the immunopathogenesis of liver fibrosis and show profibrotic and antifibrotic effects in patients with CHC. They can contribute to fibrogenesis and the development of cirrhosis. However, they can also play a part in liver regeneration and tissue repair [
12]. Further research is essential to gain a better understanding of molecular mechanisms associated with the pathogenesis of fibrosis and the effect of virus elimination using DAA in CHC patients.
This study aimed to evaluate the effect of HCV eradication using antiviral drugs on the serum cytokine and growth factor profiles of CHC patients. This would allow for a better understanding of the physiology of immunoreactions and the mechanisms of fibrosis in CHC.
2. Materials and Methods
2.1. Patients
This study is a retrospective analysis of cytokine and growth factor levels in patients with CHC who received clinical care at the Croatian Reference Center for Viral Hepatitis, University Hospital for Infectious Diseases (UHID) in Zagreb, Croatia. The study enrolled 56 CHC patients (≥18 years old, treated with DAA) and an age and sex-matched control group of 15 healthy individuals. All patients achieved sustained virological response (SVR) defined as undetectable HCV RNA at 12 weeks after therapy completion. Patients with known hematological, malignant (incl. hepatocellular carcinoma) or autoimmune diseases were excluded from the study. Ethics committees of the UHID approved the study (code 01-673-1-2021) and all subjects signed a consent form.
Liver fibrosis was analysed with noninvasive transient elastography (TE) using FibroScan devices (Echosens, France). Fibrosis stages were classified according to METAVIR score as: F0/F1 < 7.0 kPa, F2 7.0–9.5 kPa, F3 > 9.5 kPa and F4 > 12.5 kPa [
13].
2.2. Serum Sample Collection and Virological Monitoring
Cytokine and growth factor concentrations in patients with CHC were determined at four different time points. The first time point represented serum samples obtained from patients with CHC before antiviral treatment. Serum samples from the same patients were also collected after four, eight and 12 weeks of treatment (second, third and fourth time point). The samples were stored at −80 °C to avoid repeated freeze and thaw cycles. Quantification of HCV RNA was performed with COBAS AmpliPrep/COBAS TaqMan HCV Test (Roche Diagnostics, Manheim, Germany) as recommended by the manufacturer.
2.3. Bead-Based Cytometry for Cytokine and Growth Factors Levels Analysis
In this study, we measured the serum levels of 12 cytokines (interleukin 5 (IL-5), IL-13, IL-2, IL-6, IL-9, IL-10, interferon-gamma (IFN-γ), tumor necrosis factor-alpha (TNF-α), IL-17A, IL-17F, IL-4 and IL-22) and 13 growth factors (angiopoietin-2 (Ang-2), epidermal growth factor (EGF), erythropoietin (EPO), fibroblast growth factor-basic (FGF-basic), granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), hepatocyte growth factor (HGF), macrophage colony-stimulating factor (M-CSF), platelet-derived growth factor (PDGF-AA), PDGF-BB, stem cell factor (SCF), transforming growth factor-alpha (TGF-α) and vascular endothelial growth factor (VEGF). Human Th Cytokine Panel (12 plex) with Filter Plate (Biolegend, San Diego, CA, USA) was used to determine cytokine concentrations and Human Growth Factor Panel (13 plex) with Filter Rate (Biolegend, San Diego, CA, USA) was used to determine growth factor levels according to manufacturer instructions. These beads were mixed with 25 mL of serum samples. After incubation, the biotin-conjugated second antibody was added and analyzed cytokines and growth factors were detected using streptavidin-phycoerythrin which binds to the biotin conjugate and emits a fluorescent signal. The detection process was carried out on flow cytometer BD FACSCanto II (Beckton Dickinson, Franklin Lakes, NJ, USA). Finally, the concentrations of the analysed cytokines and growth factors were determined using LEGENDplex (version 8.0., Biolegend, San Diego, CA, USA) software.
2.4. Statistical Analysis
Data visualization and analysis were done in R (version 4.1.0., R Core Team 2022, Vienna, Austria) [
14]. Cytokine and growth factor levels at different time points were compared using the Friedman test and the Wilcoxon signed-rank test. The Mann–Whitney U test was used when comparing cytokine and growth factor levels between patients and healthy individuals. The correlation between cytokine and growth factor levels was evaluated with Spearman’s correlation coefficient and correlation test. Using cytokine and growth factor levels, random forest models were utilized to classify subjects into patient and healthy control groups. The number of trees was set to 10,000 and five variables were considered at every split point. Models’ performance was evaluated with out-of-bag error estimates and predictor importance was estimated by calculating the average Gini index reduction for every predictor. Cytokine and growth factor levels in patients with different liver fibrosis stages were compared with the Mann-Whitney U test. Patients were classified by liver fibrosis levels using binary logistic regression, where predictors were chosen by best subset selection. The model was evaluated with five-fold cross-validation and receiver operating characteristic (ROC) curve. Predictor cut-off points were determined using single dichotomization with the maximal Youden index criterium. All statistical tests were two-tailed with a significance level of 95%.
p-values were corrected for multiple testing with the Hommel method.
4. Discussion
In this study, we analyzed the dynamics of cytokines and growth factors of interest in CHC patients at four time points after DAA treatment. Interestingly, the levels of pro-inflammatory cytokines (IL-6 and TNF-α), Th1 cytokines (IL-2 and IFN-γ), Th2 cytokines (IL-4, IL-5 and IL-13), Th 9 cytokines (IL-9) and Th17 cytokines (IL-17A, IL-17F, and IL-22) were relatively low and did not significantly change in response to virus eradication by DAA. However, we showed a continuous decrease in serum IL-10 levels across the four disease stages. It is known that decreased IL-10 expression in the liver is associated with greater inflammatory response and infiltration of activated cells of the innate and specific immune system. These conditions can ultimately lead to fibrosis progression and cirrhosis [
15]. However, the stable and relatively low levels of other analysed cytokines suggest that DAA treatment did not induce significant changes in the immune response of CHC patients, including a pro-inflammatory response that could promote tumorigenesis. This is especially important when considering the evidence for tumor recurrence in CHC patients that achieved SVR [
16].
When comparing cytokine levels in CHC patients and healthy individuals, we found that CHC patients showed lower levels of proinflammatory cytokine TNF-α, anti-inflammatory cytokine IL-10, Th2 cytokines (IL-4, IL-5 and IL-13), Th22 cytokines (IL-22) and Th9 cytokines (IL-9) before starting DAA treatment and after achieving SVR. This finding partially goes in line with a study showing significantly reduced concentrations of IL-5, IL-9 and IL-10 in patients with CHC compared to healthy controls [
17]. In addition, Riberio et al. suggested that lower levels of IL-5 could be a universal biomarker of DAA treatment and an important factor in the case of HCV re-infection [
17]. Furthermore, Baskic et al. showed that lower but sustained IL-4 production refers to Th2 predominance in higher stages of fibrosis [
18]. Considering that CHC is generally characterised by a strong proinflammatory response, these findings provide more evidence for the potential inhibition of inflammatory mechanisms during DAA treatment of CHC patients. Notably, Riberio et al. found elevated serum concentrations of IL-4, TNF-alpha, FGF, PDGF and GM-CSF in patients with CHC compared to healthy controls [
17]. This discrepancy could potentially be attributed to higher age and higher fibrosis levels of patients analysed in the Brazilian study. All in all, our results suggest the inability of DAA treatment to completely restore altered cytokine levels in CHC, as already suggested by other studies [
19].
When analysing growth factor levels in different stages, CHC, EGF, HGF and VEGF exhibited a significant increase four weeks after antiviral treatment when compared to their respective levels before DAA treatment. Cienfuegos et al. demonstrated that EGF is effective in liver regeneration [
20]. Considering that the concentration of EGF in our study was the highest after the treatment of CHC infection, our findings could indicate liver tissue repair after treatment with DAA. Likewise, HGF is a pleiotropic cytokine produced by hepatic stellate cells (HSC) and involved in liver regeneration during acute and chronic damage and fibrosis [
21]. Serum HGF concentrations depend on the degree of liver damage and indicate the degree of hepatocellular dysfunction. Additionally, Marín-Serrano et al., found that HGF concentration was an independent factor associated with the degree of fibrosis in CHC [
22]. Our study showed that the concentration of HGF is the highest after achieving SVR, indicating the possibility that increased concentrations of HGF after treatment are a consequence of liver damage and affect the regeneration of liver tissue. Growth factor VEGF also plays an important role in the immunopathogenesis of liver fibrosis, especially in the wound healing process that is common in chronic liver disease [
23]. Although VEGF levels mildly increased during DAA treatment, they were not significantly different from the VEGF levels of healthy individuals. Taken together, the recorded increase of EGF and HGF levels suggests a considerable degree of liver tissue remodeling and regeneration in CHC patients during DAA treatment.
When considering growth factor level differences between CHC patients and the control group, we found that serum levels of Ang-2, HGF and SCF were higher both before starting antiviral treatment and after SVR when compared to healthy individuals. Similarly, we found that EGF levels were significantly higher only after reaching SVR when compared to healthy controls. These findings add another piece of evidence to the hypothesis of EGF and HGF being important contributors to liver regeneration in CHC patients during DAA treatment. Although Ang-2 and SCF levels did not significantly change in response to DAA therapy, the levels of these growth factors significantly increased compared to those of healthy individuals. These findings suggest that Ang-2 and SCF contribute to liver repair in CHC, regardless of DAA treatment.
By analyzing the correlation matrix of cytokine and growth factor expression before initiating treatment, a significant correlation was demonstrated between the expression of cytokine IFN-γ and growth factors FGF-basic, G-CSF, GM-CSF as well as between cytokine IL-17A and growth factor FGF-basic. This could be explained by a strong coherence between pro-inflammatory and pro-fibrotic factors before DAA treatment. However, this hypothesis should be further evaluated.
Using the random forest algorithm, we classified patients and healthy individuals by their cytokine and growth factor levels with high accuracy. Moreover, models classifying patients before starting treatment and patients after achieving SVR exhibited remarkably high levels of sensitivity and specificity. The most important biological modulators in classifying patients and healthy individuals in both models were IL-4, SCF and IL-5, underlining the already discussed importance of these cytokines and growth factors in CHC pathology. This finding points towards a possible usage of IL-4, SCF and IL-5 as biomarkers for DAA treatment of CHC.
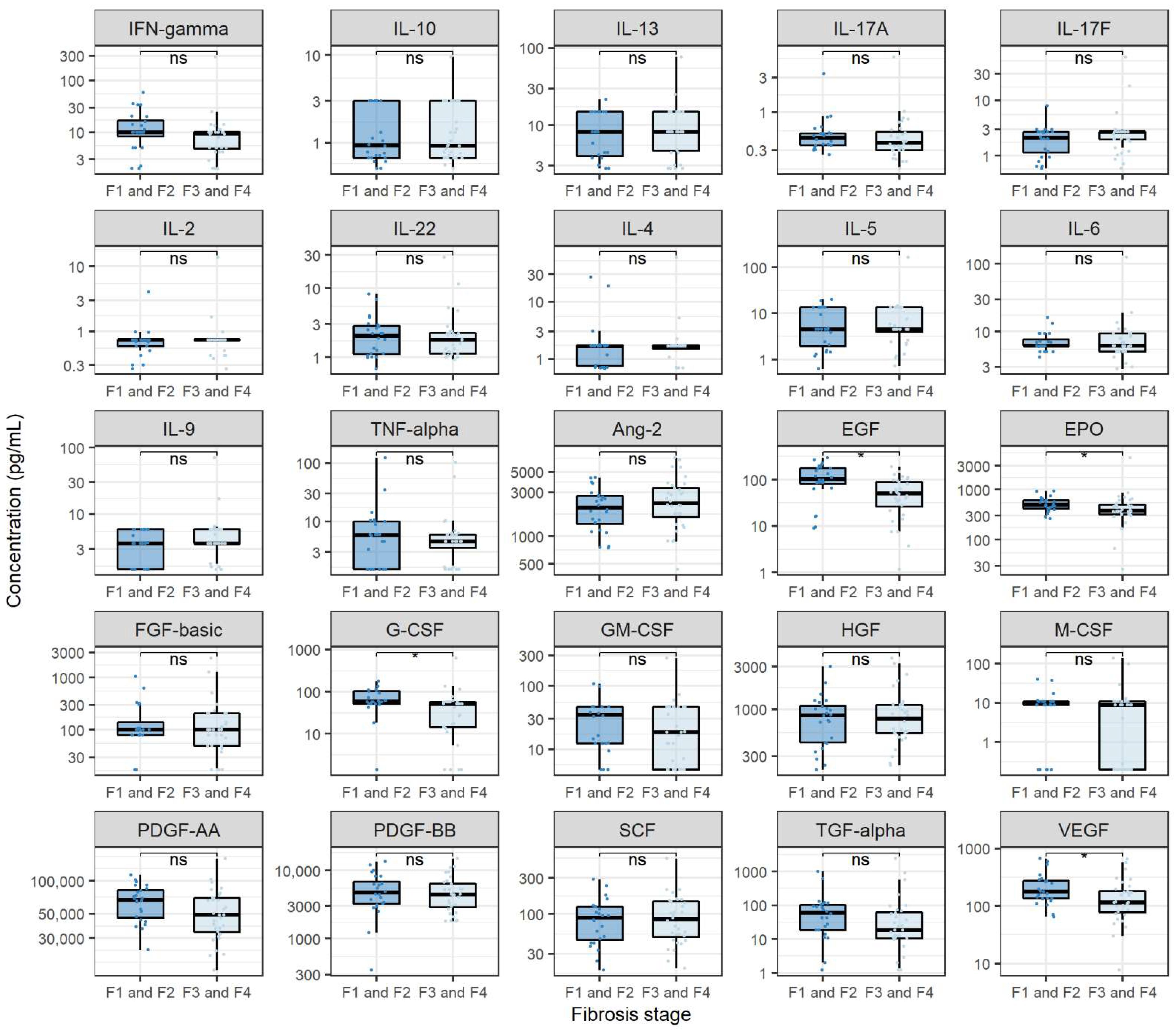
Finally, we sought to assess the relationship between analysed biological modulators and CHC severity. When comparing cytokine levels before antiviral treatment in patients with varying stages of fibrosis, we found no significant differences. This finding goes in hand with the already discussed low pro-inflammatory cytokine expression and suggests a mechanism of fibrosis formation in CHC independent of inflammation, which has already been shown in experimental models [
24]. Considering that various studies report a significant correlation between inflammation and fibrosis in CHC, this represents a novel finding [
25]. When analysing growth factor levels, we found that patients with higher fibrosis levels exhibited higher Ang-2 levels and lower EGF, G-CSF, PDGF-AA and VEGF levels. It is known that Ang-2 plays a crucial role in angiogenesis and is, therefore, an important contributor to HCC progression. Hernández-Bartolomé et al. showed that the ratio of Ang-2 and Ang-1 concentrations is significantly correlated with the degree of fibrosis in patients with CHC [
26]. This finding goes in line with our results and shows that Ang-2 could be important in severe HCC pathogenesis [
26]. To our knowledge, the finding of lower EGF levels in severe fibrosis is novel and has not been discussed in the literature. Even though the research on G-CSF in the context of liver fibrosis has been scarce, Meng et al., showed that G-CSF is one of the important factors in remodeling liver tissue with EPO, SCF and GM-CSF [
27]. Furthermore, it has been suggested that the administration of G-CSF reduces the mortality of chronic liver failure. In the context of EGF and G-CSF, our results could suggest a lower degree of tissue remodeling in patients with higher fibrosis levels. Finally, it has been shown that increased PDGF expression is important in the development of fibrosis [
28]. Our results contradict this hypothesis and imply differing roles of PDGF-AA in liver fibrosis.
The binary logistic regression model was used to classify patients by liver fibrosis levels before receiving antiviral treatment (F1/F2 vs. F3/F4). This analysis revealed an independent association of EGF, Ang-2 and male sex with the degree of fibrosis. Therefore, the logistic regression confirms the importance of EGF and Ang-2 found in the bivariate analysis. Finally, male patients were more likely to exhibit F3 or F4 fibrosis stage than female patients. If not due to higher alcohol consumption and poor diet in the studied male patient group, this new finding should be evaluated in future research. Notably, our regression model with EGF as a sole predictor of severe fibrosis achieved relatively high accuracy in classifying patients by their fibrosis levels, which points towards a potential usage of EGF as a biomarker of severe fibrosis in CHC.
The main limitation of this study is the lack of cytokine and growth factor level monitoring after SVR. This could allow for a more detailed immune response and liver remodeling assessment. Another shortfall of this study is a small percentage of HCV genotypes 2 and 4 among analysed patients, which did not allow for the evaluation of the effect of HCV genotype on cytokine and growth factor levels. However, considering that the HCV genotype ratios of patients included in this study reflect the HCV genotype ratio in the population, we believe that this did not significantly affect the conclusions of our study.

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}