
Analytical Sensitivity of Six SARS-CoV-2 Rapid Antigen Tests for Omicron versus Delta Variant

 , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
- -
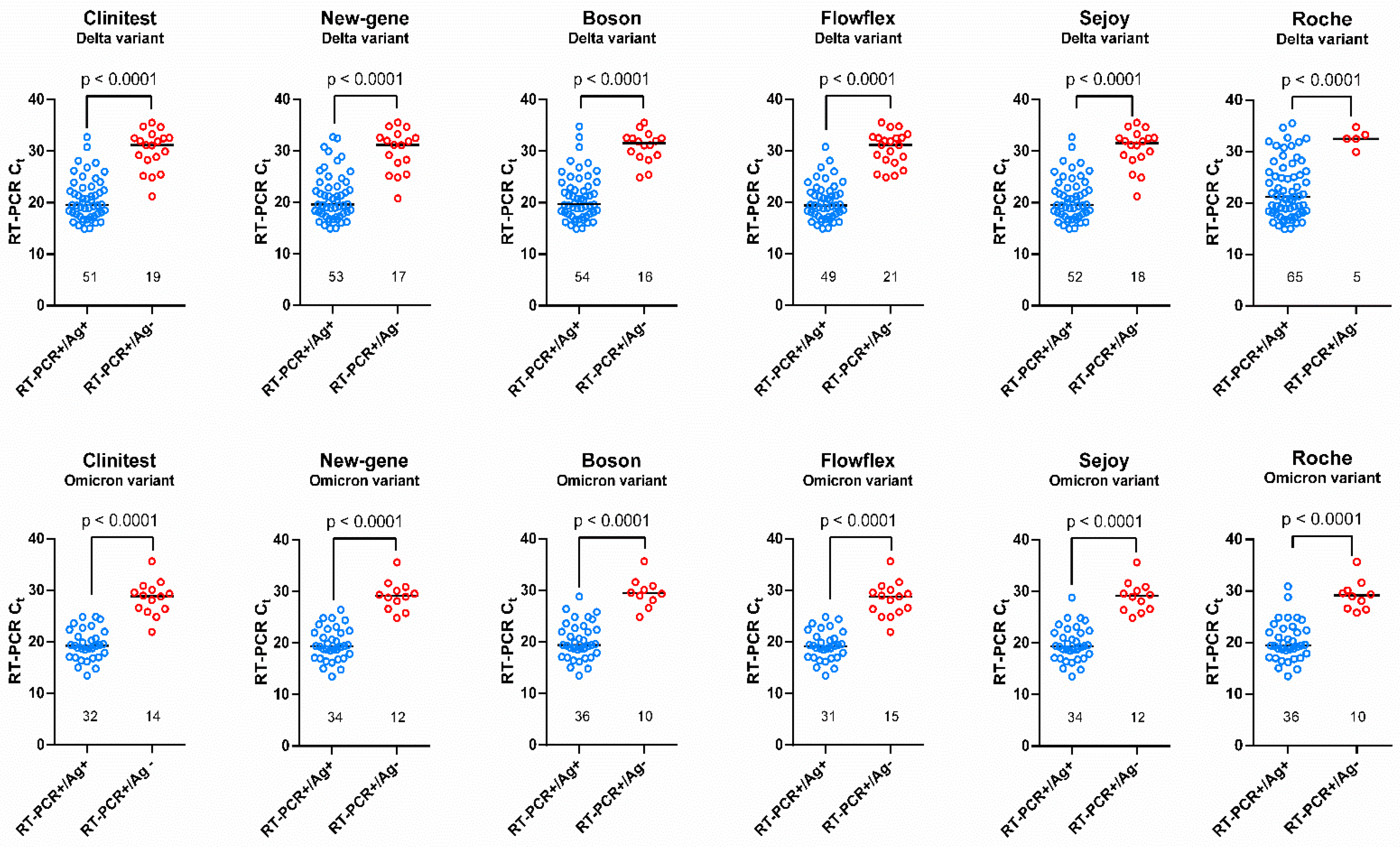
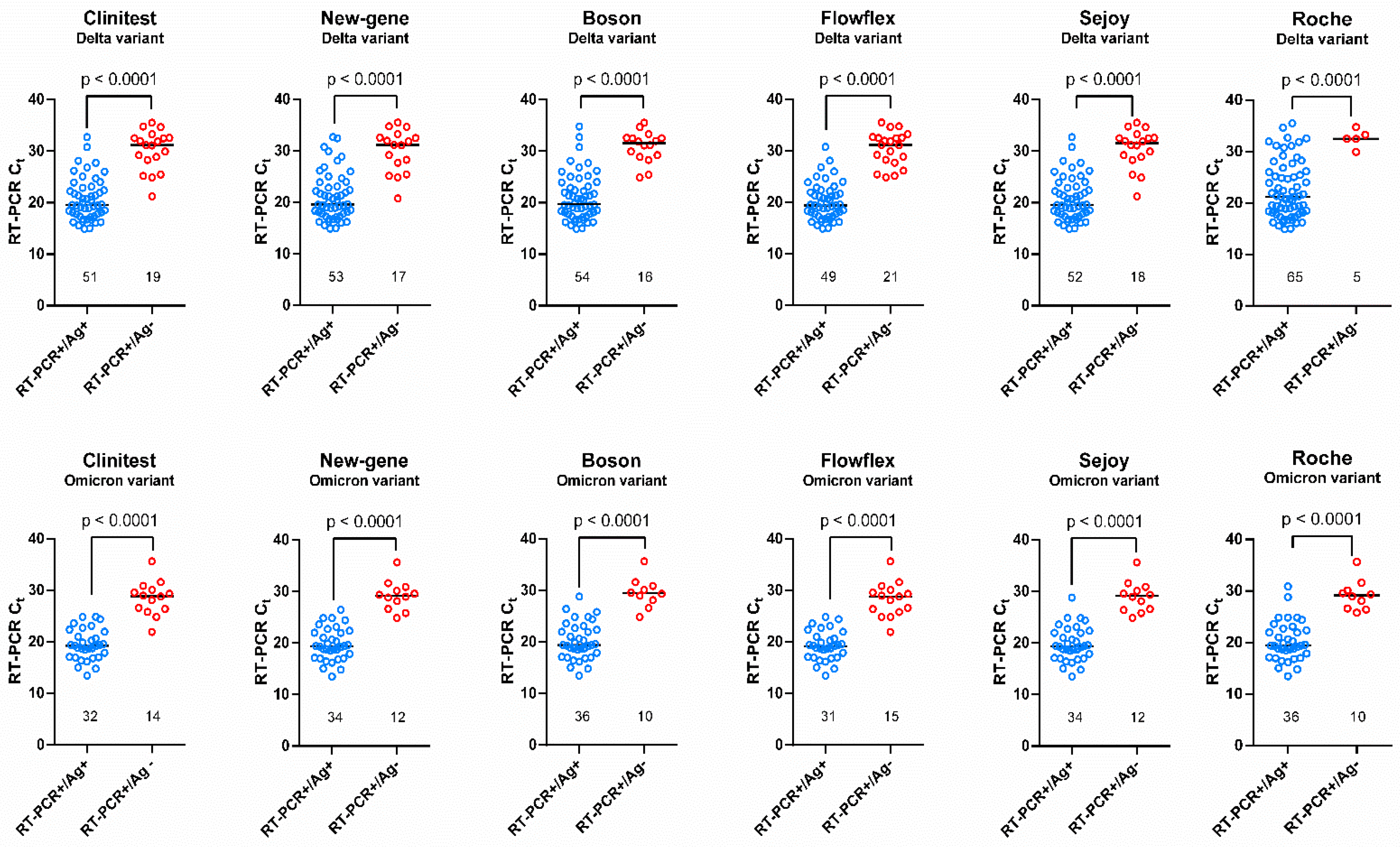
- Weakly positive: <103 RNA copies/mL (Ct > 32.29);
- -
- Moderately positive: ≥103 RNA copies/mL (Ct ≤ 32.29) to <105 RNA copies/mL (Ct > 28.48);
- -
- Strongly positive: ≥105 RNA copies/mL (Ct ≤ 28.48) to <107 RNA copies/mL (Ct > 17.04);
- -
- Very strongly positive: ≥107 RNA copies/mL (Ct ≤ 17.04).
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peeling, R.W.; Olliaro, P.L.; Boeras, D.I.; Fongwen, N. Scaling up COVID-19 rapid antigen tests: Promises and challenges. Lancet Infect. Dis. 2021, 21, e290–e295. [Google Scholar] [CrossRef]
- Caruana, G.; Croxatto, A.; Kampouri, E.; Kritikos, A.; Opota, O.; Foerster, M.; Brouillet, R.; Senn, L.; Lienhard, R.; Egli, A. ImplemeNting SARS-CoV-2 Rapid antigen testing in the Emergency wArd of a Swiss univErsity hospital: The INCREASE study. Microorganisms 2021, 9, 798. [Google Scholar] [CrossRef] [PubMed]
- EU Health Preparedness: A Common List of COVID-19 Rapid Antigen Tests; A Common Standardised Set of Data to Be Included in COVID-19 Test Result Certificates; and a Common List of COVID-19 Laboratory based Antigenic Assays. Available online: https://ec.europa.eu/health/sites/default/files/preparedness_response/docs/COVID-19_rat_common-list_en.pdf (accessed on 16 February 2022).
- Favresse, J.; Gillot, C.; Oliveira, M.; Cadrobbi, J.; Elsen, M.; Eucher, C.; Laffineur, K.; Rosseels, C.; Van Eeckhoudt, S.; Nicolas, J.-B. Head-to-head comparison of rapid and automated antigen detection tests for the diagnosis of SARS-CoV-2 infection. J. Clin. Med. 2021, 10, 265. [Google Scholar] [CrossRef] [PubMed]
- Salcedo, N.; Nandu, N.; Boucau, J.; Herrera, B.B. Detection of SARS-CoV-2 Omicron, Delta, Alpha and Gamma variants using a rapid antigen test. medRxiv 2022, 1–17. [Google Scholar] [CrossRef]
- Agency USFD. SARS-CoV-2 Viral Mutations: Impact on COVID-19 Tests. Available online: https://www.fda.gov/medical-devices/coronavirus-COVID-19-and-medical-devices/SARS-CoV-2-viral-mutations-impact-COVID-19-tests#omicronvariantimpact (accessed on 18 February 2022).
- Adamson, B.J.; Sikka, R.; Wyllie, A.L.; Premsrirut, P.K. Discordant SARS-CoV-2 PCR and Rapid Antigen Test Results When Infectious: A December 2021 Occupational Case Series. medRxiv 2022, 1–14. [Google Scholar] [CrossRef]
- Bohn, M.K.; Mancini, N.; Loh, T.P.; Wang, C.-B.; Grimmler, M.; Gramegna, M.; Yuen, K.-Y.; Mueller, R.; Koch, D.; Sethi, S. IFCC interim guidelines on molecular testing of SARS-CoV-2 infection. Clin. Chem. Lab. Med. 2020, 58, 1993–2000. [Google Scholar] [CrossRef]
- Freed, N.E.; Vlková, M.; Faisal, M.B.; Silander, O.K. Rapid and inexpensive whole-genome sequencing of SARS-CoV-2 using 1200 bp tiled amplicons and Oxford Nanopore Rapid Barcoding. Biol. Methods Protoc. 2020, 5, bpaa014. [Google Scholar] [CrossRef]
- Nextclade v1.14.0, Clade Assignment, Mutation Calling, and Sequence Quality Checks. Available online: https://clades.nextstrain.org/ (accessed on 15 February 2022).
- Bekliz, M.; Adea, K.; Alvarez, C.; Essaidi-Laziosi, M.; Escadafal, C.; Kaiser, L.; Eckerle, I. Analytical sensitivity of seven SARS-CoV-2 antigen-detecting rapid tests for Omicron variant. medRxiv 2021, 1–17. [Google Scholar] [CrossRef]
- Chan, M.C.; Hui, K.P.; Ho, J.; Cheung, M.-C.; Ng, K.-C.; Ching, R.; Lai, K.-L.; Kam, T.; Gu, H.; Sit, K.-Y. SARS-CoV-2 Omicron variant replication in human respiratory tract ex vivo. Res. Sq. 2021, 1–20. [Google Scholar] [CrossRef]
- Peacock, T.P.; Brown, J.C.; Zhou, J.; Thakur, N.; Newman, J.; Kugathasan, R.; Sukhova, K.; Kaforou, M.; Bailey, D.; Barclay, W.S. The SARS-CoV-2 variant, Omicron, shows rapid replication in human primary nasal epithelial cultures and efficiently uses the endosomal route of entry. BioRxiv 2022, 1–24. [Google Scholar] [CrossRef]
- Marais, G.J.K.; Hsiao, N.-Y.; Iranzadeh, A.; Doolabh, D.; Enoch, A.; Chu, C.Y.; Williamson, C.; Brink, A.; Hardie, D.R. Saliva swabs are the preferred sample for Omicron detection. medRxiv 2021, 1–13. [Google Scholar] [CrossRef]
- Goodall, B.L.; LeBlanc, J.J.; Hatchette, T.F.; Barrett, L.; Patriquin, G. Investigating sensitivity of nasal or throat (ISNOT): A combination of both swabs increases sensitivity of SARS-CoV-2 rapid antigen tests. medRxiv 2022, 1–26. [Google Scholar] [CrossRef]
- Schrom, J.; Marquez, C.; Pilarowski, G.; Wang, G.; Mitchell, A.; Puccinelli, R.; Black, D.; Rojas, S.; Riberio, S.; Martinez, J. Direct Comparison of SARS Co-V-2 Nasal RT-PCR and Rapid Antigen Test (BinaxNOW (TM)) at a Community Testing Site During an Omicron Surge. medRxiv 2022, 1–11. [Google Scholar] [CrossRef]
- Krüttgen, A.; Cornelissen, C.G.; Dreher, M.; Hornef, M.W.; Imöhl, M.; Kleines, M. Comparison of the SARS-CoV-2 Rapid antigen test to the real star SARS-CoV-2 RT PCR kit. J. Virol. Methods 2021, 288, 114024. [Google Scholar] [CrossRef]
- Kanjilal, S.; Chalise, S.; Shah, A.S.; Cheng, C.-A.; Senussi, Y.; Springer, M.; Walt, D.R. Analytic sensitivity of the Abbott BinaxNOW lateral flow immunochromatographic assay for the SARS-CoV-2 Omicron variant. medRxiv 2022, 1–11. [Google Scholar] [CrossRef]
- de Michelena, P.; Torres, I.; Ramos-Garcia, A.; Gosalbes, V.; Ruiz, N.; Sanmartin, A.; Botija, P.; Puojois, S.; Huntley, D.; Albert, E. Real-life performance of a COVID-19 rapid antigen detection test targeting the SARS-CoV-2 nucleoprotein for diagnosis of COVID-19 due to the Omicron variant. J. Infect. 2022; in press, journal pre-proof. [Google Scholar]
- Lee, J.; Song, J.-U.; Shim, S.R. Comparing the diagnostic accuracy of rapid antigen detection tests to real time polymerase chain reaction in the diagnosis of SARS-CoV-2 infection: A systematic review and meta-analysis. J. Clin. Virol. 2021, 144, 104985. [Google Scholar] [CrossRef]
- Landaverde, L.; Turcinovic, J.; Doucette-Stamm, L.; Gonzales, K.; Platt, J.; Connor, J.H.; Klapperich, C.M. Comparison of BinaxNOW TM and SARS-CoV-2 qRT-PCR detection of the Omicron Variant from Matched Anterior Nares Swabs. medRxiv 2022, 1–17. [Google Scholar] [CrossRef]
- Fernandez-Montero, A.; Argemi, J.; Rodríguez, J.A.; Ariño, A.H.; Moreno-Galarraga, L. Validation of a rapid antigen test as a screening tool for SARS-CoV-2 infection in asymptomatic populations. Sensitivity, specificity and predictive values. EClinicalMedicine 2021, 37, 100954. [Google Scholar] [CrossRef]
- Baro, B.; Rodo, P.; Ouchi, D.; Bordoy, A.E.; Amaro, E.N.S.; Salsench, S.V.; Molinos, S.; Alemany, A.; Ubals, M.; Corbacho-Monné, M. Performance characteristics of five antigen-detecting rapid diagnostic test (Ag-RDT) for SARS-CoV-2 asymptomatic infection: A head-to-head benchmark comparison. J. Infect. 2021, 82, 269–275. [Google Scholar] [CrossRef]
- Weishampel, Z.; Young, J.; Fischl, M.; Fischer, R.; Owusu, I.O.; Riopelle, J.; Schulz, J.; Port, J.R.; Saturday, T.; van Doremalen, N. OraSure InteliSwab Rapid Antigen Test performance with the SARS-CoV-2 Variants of Concern Alpha, Beta, Gamma, Delta, and Omicron. Viruses 2022, 14, 543. [Google Scholar] [CrossRef]
- Osterman, A.; Iglhaut, M.; Lehner, A.; Späth, P.; Stern, M.; Autenrieth, H.; Muenchhoff, M.; Graf, A.; Krebs, S.; Blum, H. Comparison of four commercial, automated antigen tests to detect SARS-CoV-2 variants of concern. Med. Microbiol. Immunol. 2021, 210, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Jian, M.-J.; Chung, H.-Y.; Chang, C.-K.; Lin, J.-C.; Yeh, K.-M.; Chen, C.-W.; Lin, D.-Y.; Chang, F.-Y.; Hung, K.-S.; Perng, C.-L. SARS-CoV-2 variants with T135I nucleocapsid mutations may affect antigen test performance. Int. J. Infect. Dis. 2022, 114, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Bourassa, L.; Perchetti, G.A.; Phung, Q.; Lin, M.J.; Mills, M.G.; Roychoudhury, P.; Harmon, K.G.; Reed, J.C.; Greninger, A.L. A SARS-CoV-2 nucleocapsid variant that affects antigen test performance. J. Clin. Virol. 2021, 141, 104900. [Google Scholar] [CrossRef] [PubMed]
- Del Vecchio, C.; Brancaccio, G.; Brazzale, A.R.; Lavezzo, E.; Onelia, F.; Franchin, E.; Manuto, L.; Bianca, F.; Cianci, V.; Cattelan, A. Emergence of N antigen SARS-CoV-2 genetic variants escaping detection of antigenic tests. medRxiv 2021, 1–24. [Google Scholar] [CrossRef]

{kind=link}
| Population | Variant | Clinitest | New-Gene | Boson | Flowflex | Sejoy | Roche |
|---|---|---|---|---|---|---|---|
| Total cohort | Delta | 72.9% | 75.7% | 77.1% | 70.0% | 74.3% | 92.9% |
| (n = 70) | (60.9–82.8) | (64.0–85.2) | (65.6–86.3) | (57.9–80.4) | (62.4–84.0) | (84.1–97.6) | |
| Omicron | 69.6% | 73.9% | 78.3% | 67.4% | 73.9% | 78.3% | |
| (n = 46) | (54.3–82.3) | (58.9–85.7) | (63.6–89.1) | (52.0–80.5) | (58.9–85.7) | (63.6–89.1) | |
| Ct ≤ 25 | Delta | 95.6% | 95.6% | 97.8% | 97.8% | 95.6% | 100% |
| (n = 45) | (84.9–99.5) | (84.9–99.5) | (88.2–99.9) | (88.2–99.9) | (84.9–99.5) | (92.1–100) | |
| Omicron | 94.1% | 97.1% | 97.1% | 91.2% | 97.1% | 100% | |
| (n = 33) | (80.3–99.3) | (84.7–99.9) | (84.7–99.9) | (76.3–98.1) | (84.7–99.9) | (89.4–100) | |
| Ct > 25 | Delta | 32.0% | 40.0% | 40.0% | 20.0% | 36.0% | 80.0% |
| (n = 25) | (15.0–53.5) | (21.1–61.3) | (21.1–61.3) | (6.8–40.7) | (18.0–57.5) | (59.3–93.2) | |
| Omicron | 0.0% | 7.7% | 23.1% | 0.0% | 7.7% | 23.1% | |
| (n = 13) | (0.0–24.7) | (0.2–36.0) | (5.0–5.38) | (0.0–24.7) | (0.2–36.0) | (5.0–53.8) | |
| Asymptomatic | Delta | 35.3% | 23.5% | 41.2% | 23.5% | 35.3% | 82.4% |
| (n = 17) | (14.2–61.7) | (6.8–49.9) | (18.4–67-1) | (6.8–49.9) | (14.2–61.7) | (56.6–96.2) | |
| Omicron | 31.3% | 37.5% | 50.0% | 31.3% | 43.8% | 56.3% | |
| (n = 16) | (11.0–58.7) | (15.2–64.6) | (24.7–75.4) | (11.0–58.7) | (19.8–70.1) | (29.9–80.3) | |
| Symptomatic | Delta | 84.9% | 92.5% | 88.7% | 84.9% | 86.8% | 96.2% |
| (n = 53) | (72.4–93.3) | (81.8–97.9) | (77.0–95.7) | (72.4–93.3) | (76.7–94.5) | (87.0–99.5) | |
| Omicron | 90.0% | 93.3% | 93.3% | 86.7% | 90.0% | 90.0% | |
| (n = 30) | (73.5–97.9) | (77.9–99.2) | (77.9–99.2) | (69.3–96.2) | (73.5–97.9) | (73.5–97.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bayart, J.-L.; Degosserie, J.; Favresse, J.; Gillot, C.; Didembourg, M.; Djokoto, H.P.; Verbelen, V.; Roussel, G.; Maschietto, C.; Mullier, F.; et al. Analytical Sensitivity of Six SARS-CoV-2 Rapid Antigen Tests for Omicron versus Delta Variant. Viruses 2022, 14, 654. https://doi.org/10.3390/v14040654
Bayart J-L, Degosserie J, Favresse J, Gillot C, Didembourg M, Djokoto HP, Verbelen V, Roussel G, Maschietto C, Mullier F, et al. Analytical Sensitivity of Six SARS-CoV-2 Rapid Antigen Tests for Omicron versus Delta Variant. Viruses. 2022; 14(4):654. https://doi.org/10.3390/v14040654
Chicago/Turabian StyleBayart, Jean-Louis, Jonathan Degosserie, Julien Favresse, Constant Gillot, Marie Didembourg, Happy Phanio Djokoto, Valérie Verbelen, Gatien Roussel, Céline Maschietto, François Mullier, and et al. 2022. "Analytical Sensitivity of Six SARS-CoV-2 Rapid Antigen Tests for Omicron versus Delta Variant" Viruses 14, no. 4: 654. https://doi.org/10.3390/v14040654
APA StyleBayart, J.-L., Degosserie, J., Favresse, J., Gillot, C., Didembourg, M., Djokoto, H. P., Verbelen, V., Roussel, G., Maschietto, C., Mullier, F., Dogné, J.-M., & Douxfils, J. (2022). Analytical Sensitivity of Six SARS-CoV-2 Rapid Antigen Tests for Omicron versus Delta Variant. Viruses, 14(4), 654. https://doi.org/10.3390/v14040654