
Side-By-Side Evaluation of Three Commercial ELISAs for the Quantification of SARS-CoV-2 IgG Antibodies

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
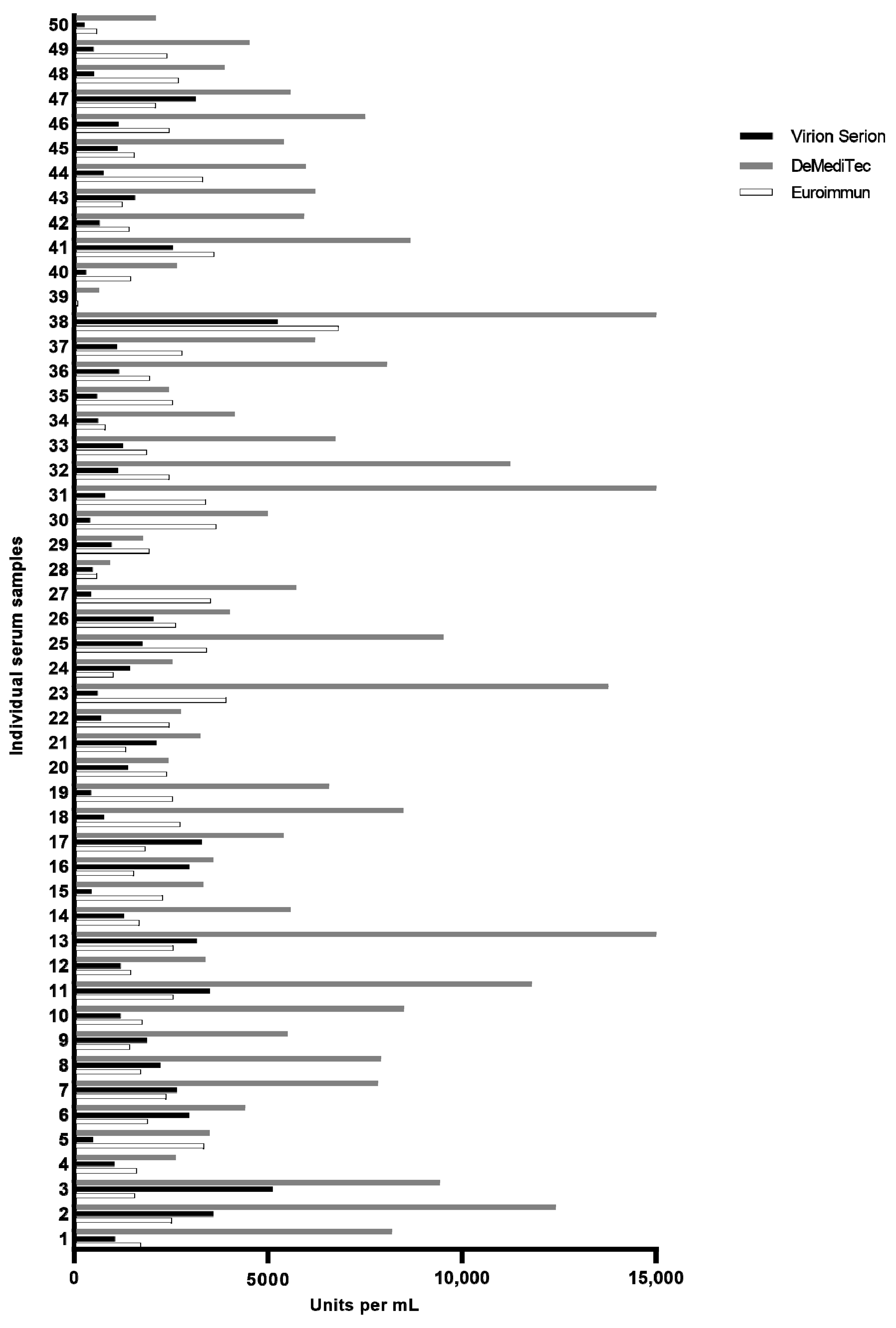
3.1. Comparability of Test Results
3.2. Correlation between Quantitative Values and Neutralizing Antibody Titers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethical Statement
References
- Knezevic, I.; Mattiuzzo, G.; Page, M.; Minor, P.; Griffiths, E.; Nuebling, M.; Moorthy, V. WHO International Standard for Evaluation of the Antibody Response to COVID-19 Vaccines: Call for Urgent Action by the Scientific Community. Lancet Microbe 2021, 3, e235–e240. [Google Scholar] [CrossRef]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of Protection against Symptomatic and Asymptomatic SARS-CoV-2 Infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- NIBSC Code: 20/136; National Institute for Biological Standards and Control First WHO International Standard for Anti-SARS-CoV-2 Immunoglobulin (Human); Instructions for Use (Version 2.0, Dated 17/12/2020); NIBSC: Potters Bar, UK, 2020.
- Müller, K.; Girl, P.; Giebl, A.; Gruetzner, S.; Antwerpen, M.; Khatamzas, E.; Wölfel, R.; von Buttlar, H. Sensitivity of Two SARS-CoV-2 Variants with Spike Protein Mutations to Neutralising Antibodies. Virus Genes 2021, 57, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Van Elslande, J.; Decru, B.; Jonckheere, S.; Van Wijngaerden, E.; Houben, E.; Vandecandelaere, P.; Indevuyst, C.; Depypere, M.; Desmet, S.; André, E.; et al. Antibody Response against SARS-CoV-2 Spike Protein and Nucleoprotein Evaluated by Four Automated Immunoassays and Three ELISAs. Clin. Microbiol. Infect. 2020, 26, 1557.e1–1557.e7. [Google Scholar] [CrossRef] [PubMed]
- Santiago, L.; Uranga-Murillo, I.; Arias, M.; González-Ramírez, A.M.; Macías-León, J.; Moreo, E.; Redrado, S.; García-García, A.; Taleb, V.; Lira-Navarrete, E.; et al. Determination of the Concentration of IgG against the Spike Receptor-Binding Domain That Predicts the Viral Neutralizing Activity of Convalescent Plasma and Serum against SARS-CoV-2. Biology 2021, 10, 208. [Google Scholar] [CrossRef] [PubMed]
- Mendrone-Junior, A.; Dinardo, C.L.; Ferreira, S.C.; Nishya, A.; Salles, N.A.; de Almeida Neto, C.; Hamasaki, D.T.; Facincani, T.; de Oliveira Alves, L.B.; Machado, R.R.G.; et al. Correlation between SARS-COV-2 Antibody Screening by Immunoassay and Neutralizing Antibody Testing. Transfusion 2021, 61, 1181–1190. [Google Scholar] [CrossRef] [PubMed]
- Lukaszuk, K.; Kiewisz, J.; Rozanska, K.; Dabrowska, M.; Podolak, A.; Jakiel, G.; Woclawek-Potocka, I.; Lukaszuk, A.; Rabalski, L. Usefulness of IVD Kits for the Assessment of SARS-CoV-2 Antibodies to Evaluate the Humoral Response to Vaccination. Vaccines 2021, 9, 840. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lee, J.H.; Ko, G.Y.; Ryu, J.H.; Jang, J.H.; Bae, H.; Yoo, S.-H.; Choi, A.-R.; Jung, J.; Lee, J.; et al. Quantitative SARS-CoV-2 Spike Antibody Response in COVID-19 Patients Using Three Fully Automated Immunoassays and a Surrogate Virus Neutralization Test. Diagnostics 2021, 11, 1496. [Google Scholar] [CrossRef] [PubMed]
- Higgins, V.; Fabros, A.; Kulasingam, V. Quantitative Measurement of Anti-SARS-CoV-2 Antibodies: Analytical and Clinical Evaluation. J. Clin. Microbiol. 2021, 59, e03149-20. [Google Scholar] [CrossRef] [PubMed]
- Perkmann, T.; Perkmann-Nagele, N.; Koller, T.; Mucher, P.; Radakovics, A.; Marculescu, R.; Wolzt, M.; Wagner, O.F.; Binder, C.J.; Haslacher, H. Anti-Spike Protein Assays to Determine SARS-CoV-2 Antibody Levels: A Head-to-Head Comparison of Five Quantitative Assays. Microbiol. Spectr. 2021, 9, e00247-21. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| MANUFACTURER | KIT ASSAY | TARGET ANTIGEN | METHOD | IMMUNOGLOBLIN DETECTED | UNITS | ALTERNATIVE WHO UNITS | CONVERSION FACTOR | CUT-OFF | DYNAMIC RANGE |
|---|---|---|---|---|---|---|---|---|---|
| Euroimmun | Anti-SARS-CoV-2 QuantiVac ELISA (IgG) | S1 1 | ELISA | IgG | RU/mL | BAU/mL | 3.2 | 32 | 19.2–256 |
| Virion Serion | SERION ELISA agile SARS-CoV-2 IgG | S 2 | ELISA | IgG | U/mL | BAU/mL | 2.1 | 31.5 | 10.5–525 |
| DeMediTec | COVID-19 (SARS-CoV-2) quantitative IgG ELISA | S 3 | ELISA | IgG | AU/mL | IU/mL | 4.5 | 49.5 | 43–690 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Girl, P.; Mantel, S.; von Buttlar, H.; Wölfel, R.; Müller, K. Side-By-Side Evaluation of Three Commercial ELISAs for the Quantification of SARS-CoV-2 IgG Antibodies. Viruses 2022, 14, 577. https://doi.org/10.3390/v14030577
Girl P, Mantel S, von Buttlar H, Wölfel R, Müller K. Side-By-Side Evaluation of Three Commercial ELISAs for the Quantification of SARS-CoV-2 IgG Antibodies. Viruses. 2022; 14(3):577. https://doi.org/10.3390/v14030577
Chicago/Turabian StyleGirl, Philipp, Sonja Mantel, Heiner von Buttlar, Roman Wölfel, and Katharina Müller. 2022. "Side-By-Side Evaluation of Three Commercial ELISAs for the Quantification of SARS-CoV-2 IgG Antibodies" Viruses 14, no. 3: 577. https://doi.org/10.3390/v14030577
APA StyleGirl, P., Mantel, S., von Buttlar, H., Wölfel, R., & Müller, K. (2022). Side-By-Side Evaluation of Three Commercial ELISAs for the Quantification of SARS-CoV-2 IgG Antibodies. Viruses, 14(3), 577. https://doi.org/10.3390/v14030577