
Leptomeningeal Carcinomatosis of a Poorly Differentiated Cervical Carcinoma Caused by Human Papillomavirus Type 18


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Material and Methods
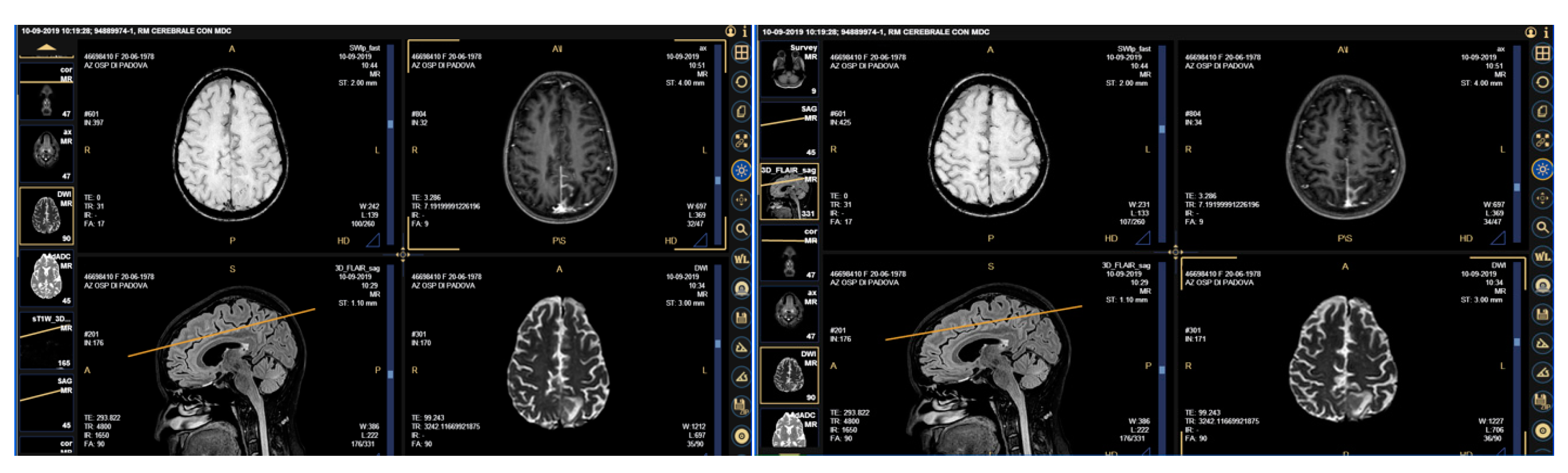
2.1. Case Presentation
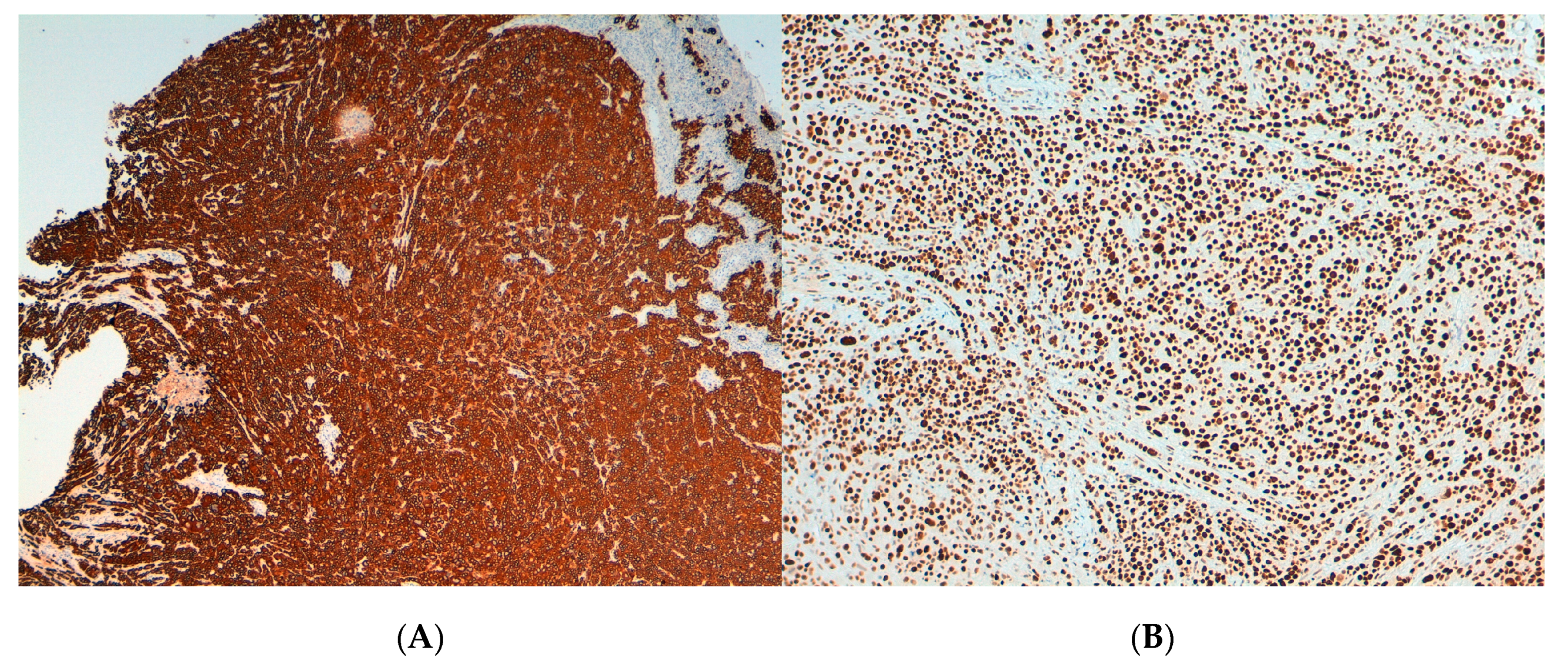
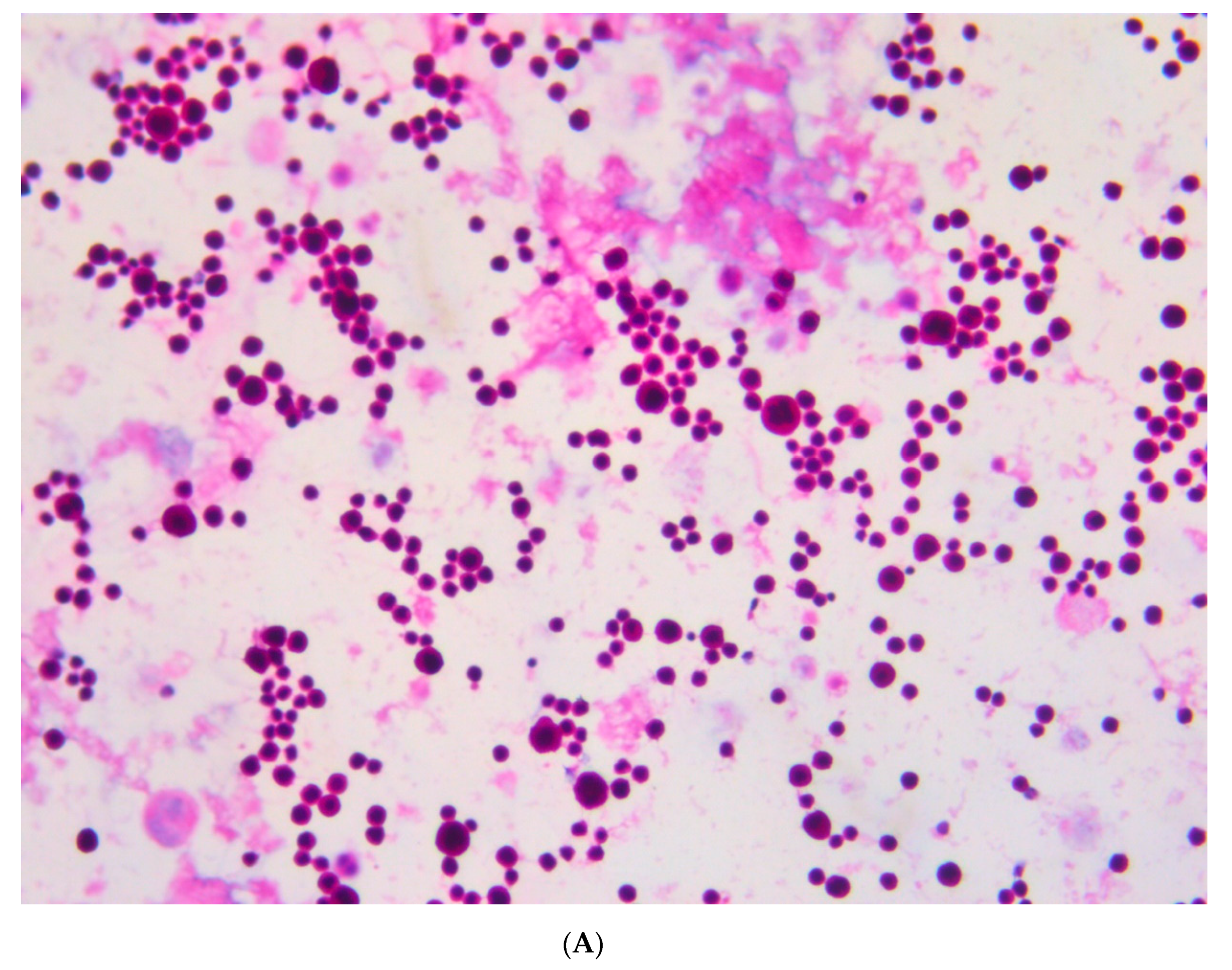
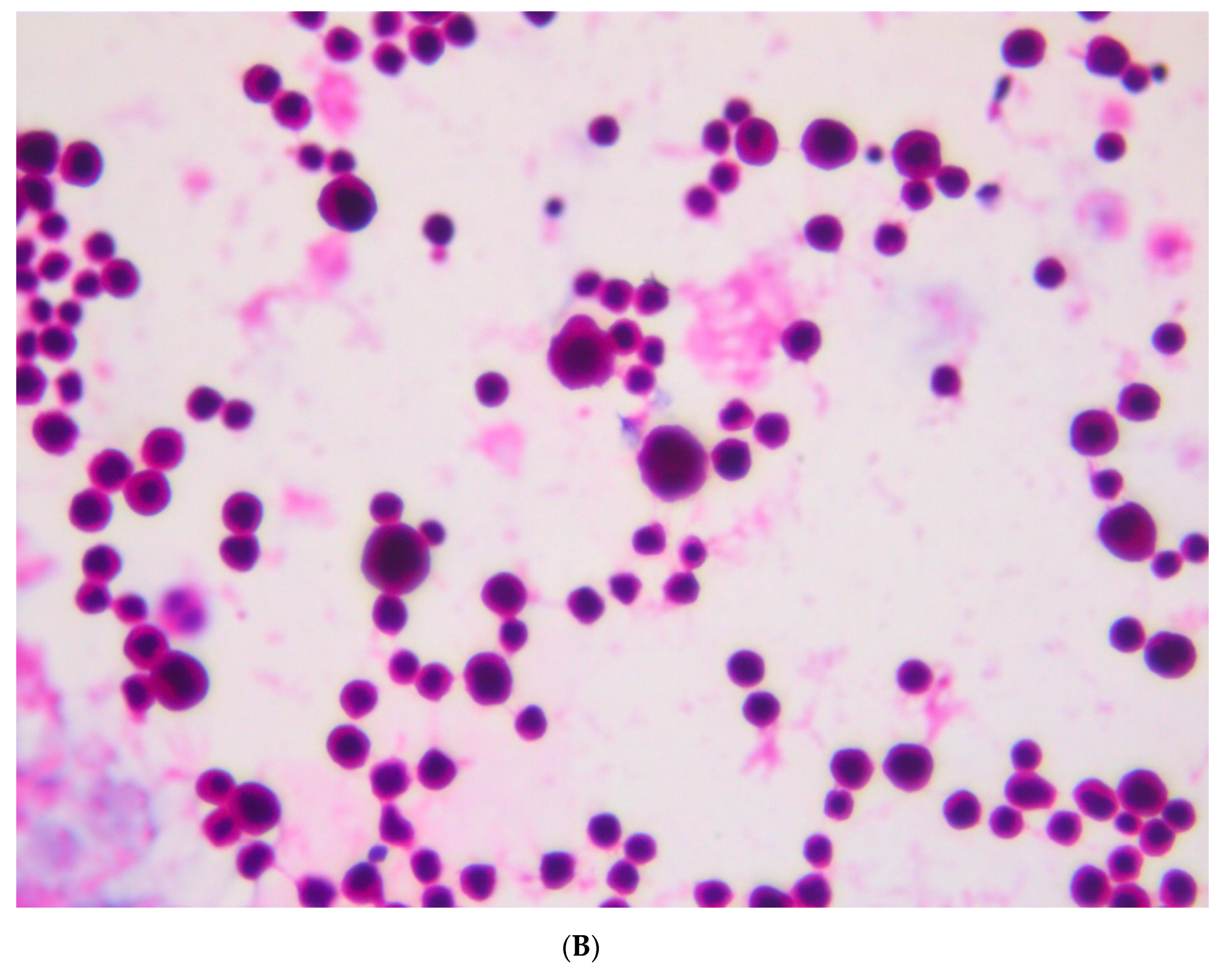
2.2. Histopathology and Immunohistochemistry (IHC)
2.3. Search and Typing of HPV Sequences
3. Results
3.1. Pathological and Immunohistochemical Findings
3.2. Virological Findings
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wojtyla, C.; Janik-Koncewicz, K.; La Vecchia, C. Cervical cancer mortality in young adult European women. Eur. J. Cancer 2020, 126, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Gomez, D.; Munoz, J.; Bosch, F.X.; de Sanjosé, S. ICO-IARC Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in the World. Summary Report. 17 June 2019. 2019. Available online: https://www.hpvcentre.net/statistics/reports/XWX.pdf (accessed on 12 January 2021).
- Ronco, G.; Dillner, J.; Elfström, K.M.; Tunesi, S.; Snijders, P.J.F.; Arbyn, M.; Kitchener, H.; Segnan, N.; Gilham, C.; Giorgi-Rossi, P.; et al. Efficacy of HPV-based screening for prevention of invasive cervical cancer: Follow-up of four European randomised controlled trials. Lancet 2014, 383, 524–532. [Google Scholar] [CrossRef]
- Von Karsa, L.; Arbyn, M.; De Vuyst, H.; Dillner, J.; Dillner, L.; Franceschi, S.; Patnick, J.; Ronco, G.; Segnan, N.; Suonio, E.; et al. European guidelines for quality assurance in cervical cancer screening. Summary of the supplements on HPV screening and vaccination. Papillomavirus Res. 2015, 1, 22–31. [Google Scholar] [CrossRef]
- Serraino, D.; Gini, A.; Taborelli, M.; Ronco, G.; Giorgi-Rossi, P.; Zappa, M.; Crocetti, E.; Franzo, A.; Falcini, F.; Visioli, C.B.; et al. Changes in cervical cancer incidence following the introduction of organized screening in Italy. Prev. Med. 2015, 75, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Sakuragi, N.; Kato, T.; Shimada, C.; Kaneuchi, M.; Todo, Y.; Mitamura, T.; Takeda, M.; Kudo, M.; Murakami, G.; Watari, H. Oncological Outcomes After Okabayashi-Kobayashi Radical Hysterectomy for Early and Locally Advanced Cervical Cancer. JAMA Netw. Open 2020, 3, e204307. [Google Scholar] [CrossRef] [PubMed]
- Yust-Katz, S.; Mathis, S.; Groves, M.D. Leptomeningeal metastases from genitourinary cancer: The University of Texas MD Anderson Cancer Center experience. Med Oncol. 2013, 30, 429. [Google Scholar] [CrossRef] [PubMed]
- Oike, T.; Ohno, T.; Noda, S.; Murata, T.; Hirakawa, T.; Hirato, J.; Furuya, M.; Sato, H.; Hirota, Y.; Minegishi, T.; et al. Leptomeningeal metastasis of uterine cervical cancer 17 years after primary tumor treatment. Clin. Case Rep. 2015, 4, 54–61. [Google Scholar] [CrossRef]
- Dey, M.; Fetcko, K.; Gondim, D.D.; Bonnin, J.M. Cervical cancer metastasis to the brain: A case report and review of literature. Surg. Neurol. Int. 2017, 8, 181. [Google Scholar] [CrossRef] [PubMed]
- Nobre, R.J.; De Almeida, L.P.; Martins, T.C. Complete genotyping of mucosal human papillomavirus using a restriction fragment length polymorphism analysis and an original typing algorithm. J. Clin. Virol. 2008, 42, 13–21. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Qu, W.; Jiang, G.; Cruz, Y.; Chang, C.J.; Ho, G.Y.; Klein, R.S.; Burk, R.D. PCR detection of human papillomavirus: Comparison between MY09/MY11 and GP5+/GP6+ primer systems. J. Clin. Microbiol. 1997, 35, 1304–1310. [Google Scholar] [CrossRef] [PubMed]
- Carozzi, F.; Iossa, A.; Scalisi, A.; Sideri, M.; Andersson, K.L.; Confortini, M.; Del Mistro, A.; Maina, G.; Ronco, G.; Raggi, P.; et al. hr-HPV testing in the management of women with ASC-US+ and in the follow-up of women with cytological abnormal-ities and negative colposcopy. Recommendations of the Italian group for cervical cancer screening (GISCi). Epidemiol. Prev. 2015, 39 (Suppl. S1), 84–90. [Google Scholar]
- Nayar, R.; Wilbur, D.C. The Pap test and Bethesda 2014. Cancer Cytopathol. 2015, 123, 271–281. [Google Scholar] [CrossRef]
- Norman, I.; Hjerpe, A.; Dillner, J. Risk of high-grade lesions after atypical glandular cells in cervical screening: A population-based cohort study. BMJ Open 2017, 7, e017070. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Franceschi, S.; Howell-Jones, R.; Snijders, P.J.; Clifford, G.M. Human papillomavirus type distribution in 30,848 invasive cervical cancers worldwide: Variation by geographical region, histological type and year of publication. Int. J. Cancer 2010, 128, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Castle, P.E.; Aslam, S.; Behrens, C. Cervical Precancer and Cancer Risk by Human Papillomavirus Status and Cytologic Interpretation: Implications for Risk-Based Management. Cancer Epidemiol. Biomark. Prev. 2016, 25, 1595–1599. [Google Scholar] [CrossRef]
- Ogembo, R.K.; Gona, P.N.; Seymour, A.J.; Park, H.S.-M.; Bain, P.A.; Maranda, L.; Ogembo, J.G. Prevalence of Human Papillomavirus Genotypes among African Women with Normal Cervical Cytology and Neoplasia: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0122488. [Google Scholar] [CrossRef] [PubMed]
- Shoja, Z.; Farahmand, M.; Hosseini, N.; Jalilvand, S. A Meta-Analysis on Human Papillomavirus Type Distribution among Women with Cervical Neoplasia in the WHO Eastern Mediterranean Region. Intervirology 2019, 62, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Rotondo, J.C.; Oton-Gonzalez, L.; Mazziotta, C.; Lanzillotti, C.; Iaquinta, M.R.; Tognon, M.; Martini, F. Simultaneous Detection and Viral DNA Load Quantification of Different Human Papillomavirus Types in Clinical Specimens by the High Analytical Droplet Digital PCR Method. Front. Microbiol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Sasieni, P.; Castanon, A.; Cuzick, J. Screening and adenocarcinoma of the cervix. Int. J. Cancer 2009, 125, 525–529. [Google Scholar] [CrossRef]
- Huang, C.-C.; Kashima, M.L.; Chen, H.; Shih, I.-M.; Kurman, R.J.; Wu, T.-C. HPV in situ hybridization with catalyzed signal amplification and polymerase chain reaction in establishing cerebellar metastasis of a cervical carcinoma. Hum. Pathol. 1999, 30, 587–591. [Google Scholar] [CrossRef]
- Ignatius, R.T.; Wills, S.M.; Nadeau, L.; DePeralta-Venturina, M.; Weiner, S. Leptomeningeal Carcinomatosis Due to Squamous Cell Carcinoma of the Uterine Cervix Associated With HPV-45. J. Clin. Oncol. 2008, 26, 154–156. [Google Scholar] [CrossRef] [PubMed]
- Wuntkal, R.; Maheshwari, A.; Kerkar, R.A.; Kane, S.V.; Tongaonkar, H.B. Carcinoma of uterine cervix primarily presenting as carcinomatous meningitis: A case report. Aust. N. Z. J. Obstet. Gynaecol. 2004, 44, 268–269. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, M.C. Neoplastic meningitis. Curr. Neurol. Neurosci. Rep. 2008, 8, 249–258. [Google Scholar] [CrossRef]
- Das, M. WHO launches strategy to accelerate elimination of cervical cancer. Lancet Oncol. 2021, 22, 20–21. [Google Scholar] [CrossRef]
- Arbyn, M.; Gultekin, M.; Morice, P.; Nieminen, P.; Cruickshank, M.; Poortmans, P.; Kelly, D.; Poljak, M.; Bergeron, C.; Ritchie, D.; et al. The European response to the WHO call to eliminate cervical cancer as a public health problem. Int. J. Cancer 2020, 148, 277–284. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zorzato, P.; Zambon, M.; Gori, S.; Frayle, H.; Gervasi, M.T.; Del Mistro, A. Leptomeningeal Carcinomatosis of a Poorly Differentiated Cervical Carcinoma Caused by Human Papillomavirus Type 18. Viruses 2021, 13, 307. https://doi.org/10.3390/v13020307
Zorzato P, Zambon M, Gori S, Frayle H, Gervasi MT, Del Mistro A. Leptomeningeal Carcinomatosis of a Poorly Differentiated Cervical Carcinoma Caused by Human Papillomavirus Type 18. Viruses. 2021; 13(2):307. https://doi.org/10.3390/v13020307
Chicago/Turabian StyleZorzato, Pierpaolo, Mattia Zambon, Silvia Gori, Helena Frayle, Maria Teresa Gervasi, and Annarosa Del Mistro. 2021. "Leptomeningeal Carcinomatosis of a Poorly Differentiated Cervical Carcinoma Caused by Human Papillomavirus Type 18" Viruses 13, no. 2: 307. https://doi.org/10.3390/v13020307
APA StyleZorzato, P., Zambon, M., Gori, S., Frayle, H., Gervasi, M. T., & Del Mistro, A. (2021). Leptomeningeal Carcinomatosis of a Poorly Differentiated Cervical Carcinoma Caused by Human Papillomavirus Type 18. Viruses, 13(2), 307. https://doi.org/10.3390/v13020307