Molecular Epidemiology of HIV-1 Infected Migrants Followed Up in Portugal: Trends between 2001–2017

 , , , ,
, , , ,  , , , and
, , , and
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. HIV-1 Subtype Assignment
2.3. Drug Resistance Profile
2.4. Statistic Analyses
2.5. Ethics Statement
3. Results
3.1. Clinical Characteristics of Study Participants
3.2. HIV-1 Subtype Determination
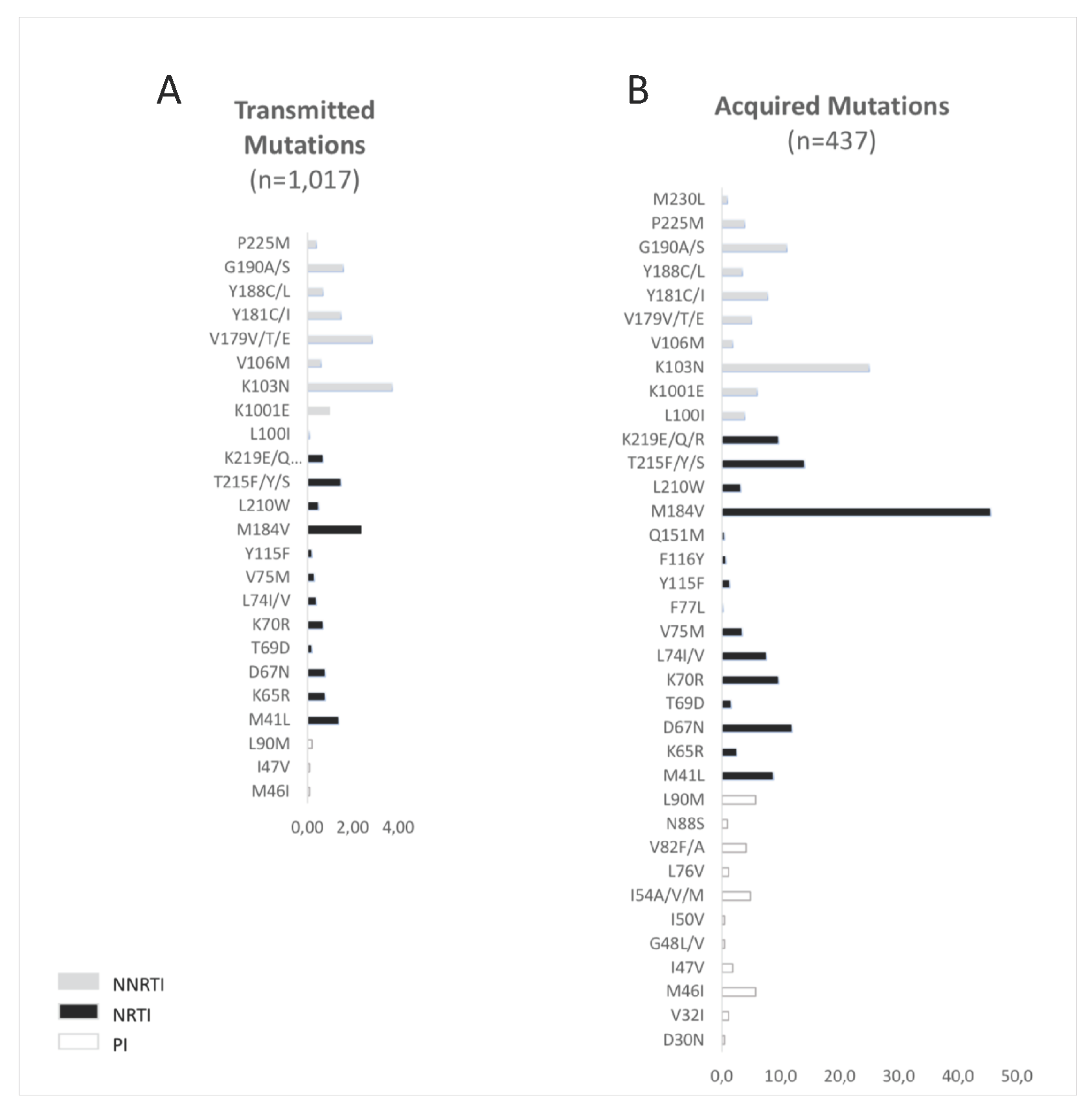
3.3. Resistance Profile in Drug Naïve (DN) Patients
3.4. Resistance Profile in Treated Patients
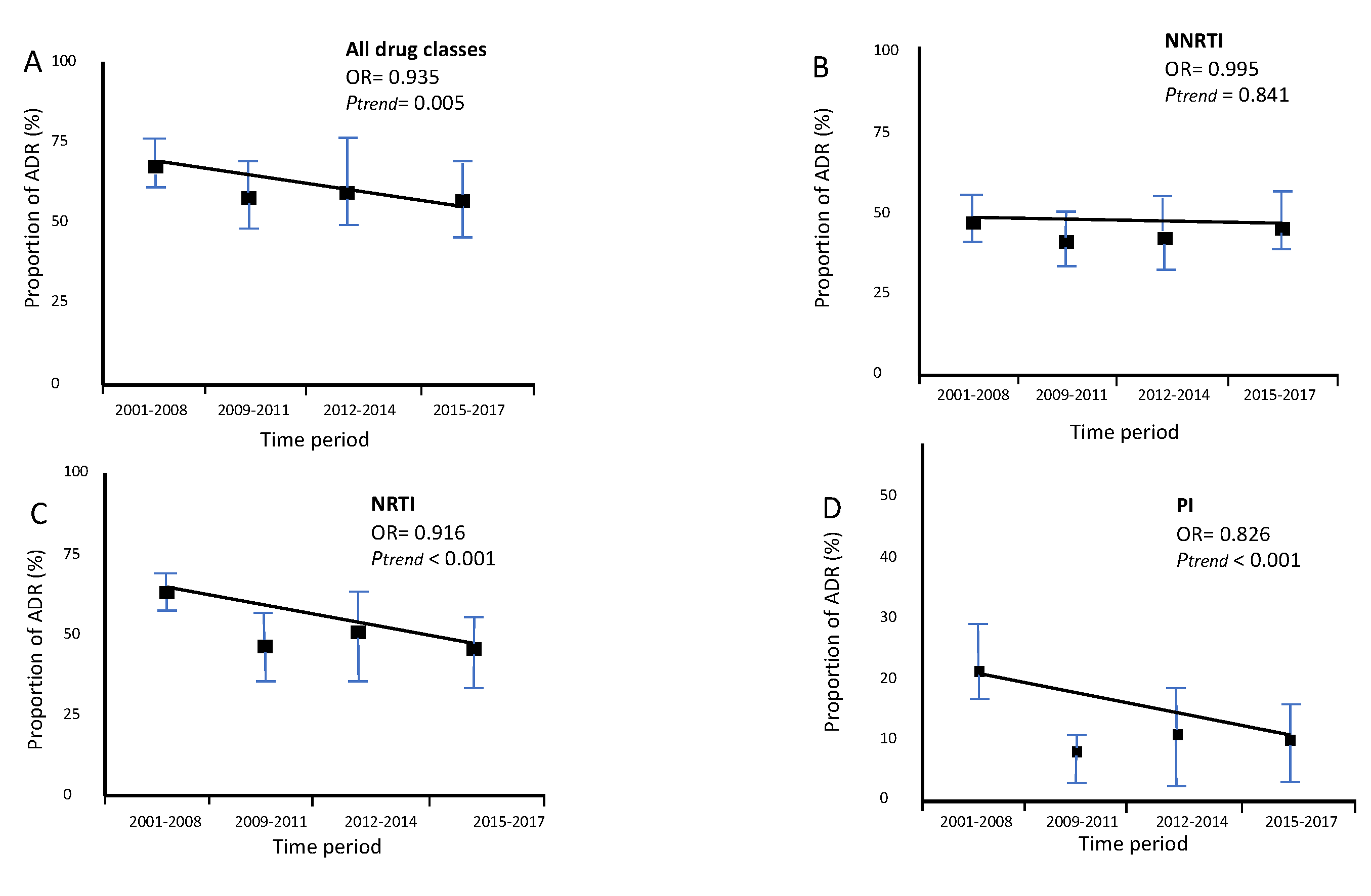
3.5. Drug Resistance Outcome
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Aldridge, R.W.; Nellums, L.B.; Bartlett, S.; Barr, A.L.; Patel, P.; Burns, R.; Hargreaves, S.; Miranda, J.J.; Tollman, S.; Friedland, J.S.; et al. Global patterns of mortality in international migrants: A systematic review and meta-analysis. Lancet 2018, 392, 2553–2566. [Google Scholar] [CrossRef]
- HIV/AIDS Surveillance in Europe. 2018. Available online: http://www.euro.who.int/pubrequest (accessed on 3 September 2019).
- Pottie, K.; Lotfi, T.; Kilzar, L.; Howeiss, P.; Rizk, N.; Akl, E.A.; Dias, S.M.F.; Biggs, B.-A.; Christensen, R.; Rahman, P.; et al. The Effectiveness and Cost-Effectiveness of Screening for HIV in Migrants in the EU/EEA: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 1700. [Google Scholar] [CrossRef] [PubMed]
- Cortes Martins, H.; Ricardo Jorge Isabel Aldir, D.; Nacional Para, P.; Novembro Doutor Ricardo Jorge, L. VIH e SIDA: A situação em _Portugal a de dezembro de _Documento no 149 Nacional de Saúde _ Instituto. Available online: www.insa.pt (accessed on 7 February 2019).
- Mengesha, Z.B.; Perz, J.; Dune, T.; Ussher, J. Refugee and migrant women’s engagement with sexual and reproductive health care in Australia: A socio-ecological analysis of health care professional perspectives. PLoS ONE 2017, 12, e0181421. [Google Scholar] [CrossRef] [PubMed]
- Zazzi, M.; Hu, H.; Prosperi, M. The global burden of HIV-1 drug resistance in the past 20 years. PeerJ 2018, 6, e4848. [Google Scholar] [CrossRef] [PubMed]
- Drescher, S.M.; von Wyl, V.; Yang, W.L.; Böni, J.; Yerly, S.; Shah, C.; Aubert, V.; Klimkait, T.; Taffé, P.; Furrer, H.; et al. Treatment-Naive Individuals Are the Major Source of Transmitted HIV-1 Drug Resistance in Men Who Have Sex With Men in the Swiss HIV Cohort Study. Clin. Infect. Dis. 2013, 58, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.E.; Camacho, R.J.; Otelea, D.; Kuritzkes, D.R.; Fleury, H.; Kiuchi, M.; Heneine, W.; Kantor, R.; Jordan, M.R.; Schapiro, J.M.; et al. Drug Resistance Mutations for Surveillance of Transmitted HIV-1 Drug-Resistance: 2009 Update. PLoS ONE 2009, 4, e4724. [Google Scholar] [CrossRef]
- Paraskevis, D.; Kostaki, E.; Gargalianos, P.; Xylomenos, G.; Lazanas, M.; Chini, M.; Skoutelis, A.; Papastamopoulos, V.; Paraskeva, D.; Antoniadou, A.; et al. Transmission Dynamics of HIV-1 Drug Resistance among Treatment-Naïve Individuals in Greece: The Added Value of Molecular Epidemiology to Public Health. Genes 2017, 8, 322. [Google Scholar] [CrossRef]
- Clutter, D.S.; Jordan, M.R.; Bertagnolio, S.; Shafer, R.W. HIV-1 Drug Resistance and Resistance Testing. Infect. Genet. Evol. 2016, 46, 292–307. [Google Scholar] [CrossRef]
- Iyidogan, P.; Anderson, K.S. Current Perspectives on HIV-1 Antiretroviral Drug Resistance. Viruses 2014, 6, 4095–4139. [Google Scholar] [CrossRef]
- Theys, K.; Libin, P.; Pineda-Peña, A.-C.; Nowé, A.; Vandamme, A.-M.; Abecasis, A.B. The impact of HIV-1 within-host evolution on transmission dynamics. Curr. Opin. Virol. 2018, 28, 92–101. [Google Scholar] [CrossRef]
- Dias, S.; Marques, A.; Gama, A.F.; Martins, M. HIV Risky Sexual Behaviors and HIV Infection among Immigrants: A Cross-Sectional Study in Lisbon, Portugal. Int. J. Environ. Res. Public Health 2014, 11, 8552–8566. [Google Scholar] [CrossRef] [PubMed]
- Libin, P.; Beheydt, G.; Deforche, K.; Imbrechts, S.; Ferreira, F.; Van Laethem, K.; Theys, K.; Carvalho, A.P.; Cavaco-Silva, J.; Lapadula, G.; et al. RegaDB: Community-driven data management and analysis for infectious diseases. Bioinformatics 2013, 29, 1477–1480. [Google Scholar] [CrossRef] [PubMed]
- Pineda-Peña, A.-C.; Faria, N.R.; Imbrechts, S.; Libin, P.; Abecasis, A.B.; Deforche, K.; Gómez-López, A.; Camacho, R.; De Oliveira, T.; Vandamme, A.-M. Automated subtyping of HIV-1 genetic sequences for clinical and surveillance purposes: Performance evaluation of the new REGA version 3 and seven other tools. Infect. Genet. Evol. 2013, 19, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Alcantara, L.C.J.; Cassol, S.; Libin, P.; Deforche, K.; Pybus, O.G.; Van Ranst, M.; Galvão-Castro, B.; Vandamme, A.-M.; De Oliveira, T. A standardized framework for accurate, high-throughput genotyping of recombinant and non-recombinant viral sequences. Nucleic Acids Res. 2009, 37, W634–W642. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Schultz, A.-K.; Calef, C.; Kuiken, C.; Leitner, T.; Korber, B.T.; Morgenstern, B.; Stanke, M. jpHMM at GOBICS: A web server to detect genomic recombinations in HIV-1. Nucleic Acids Res. 2006, 34, W463–W465. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Struck, D.; Lawyer, G.; Ternes, A.-M.; Schmit, J.-C.; Bercoff, D.P. COMET: Adaptive context-based modeling for ultrafast HIV-1 subtype identification. Nucleic Acids Res. 2014, 42, e144. [Google Scholar] [CrossRef]
- Andersson, E.; Nordquist, A.; Esbjörnsson, J.; Flamholc, L.; Gisslen, M.; Hejdeman, B.; Marrone, G.; Norrgren, H.; Svedhem, V.; Wendahl, S.; et al. Increase in transmitted drug resistance in migrants from Sub Saharan Africa diagnosed with HIV-1 in Sweden. AIDS 2018, 32, 877–884. [Google Scholar] [CrossRef]
- Del Amo, J.; Likatavičius, G.; Pérez-Cachafeiro, S.; Hernando, V.; Gonzalez, C.; Jarrín, I.; Noori, T.; Hamers, F.F.; Bolúmar, F. The epidemiology of HIV and AIDS reports in migrants in the 27 European Union countries, Norway and Iceland: 1999–2006. Eur. J. Public Health 2010, 21, 620–626. [Google Scholar] [CrossRef]
- Afonso, J.M.; Bello, G.; Guimarães, M.L.; Sojka, M.; Morgado, M.G. HIV-1 Genetic Diversity and Transmitted Drug Resistance Mutations among Patients from the North, Central and South Regions of Angola. PLoS ONE 2012, 7, e42996. [Google Scholar] [CrossRef]
- Abecasis, A.; Paraskevis, D.; Epalanga, M.; Fonseca, M.; Burity, F.; Bartolomeu, J.; Carvalho, A.; Gomes, P.; Vandamme, A.-M.; Camacho, R. HIV-1 genetic variants circulation in the North of Angola. Infect. Genet. Evol. 2005, 5, 231–237. [Google Scholar] [CrossRef]
- de Pina-Araujo, I.I.M.; Guimarães, M.L.; Bello, G.; Vicente, A.C.P.; Morgado, M.G. Profile of the HIV Epidemic in Cape Verde: Molecular Epidemiology and Drug Resistance Mutations among HIV-1 and HIV-2 Infected Patients from Distinct Islands of the Archipelago. PLoS ONE 2014, 9, e96201. [Google Scholar] [CrossRef] [PubMed]
- Bello, G.; Eyer-Silva, W.A.; Couto-Fernandez, J.C.; Guimarães, M.L.; Chequer-Fernandez, S.L.; Teixeira, S.L.; Morgado, M.G.; Eyer-Silva, W.D.A.; Bello, G. Demographic history of HIV-1 subtypes B and F in Brazil. Infect. Genet. Evol. 2007, 7, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Leite, T.C.N.F.; Campos, D.P.; Coelho, A.B.; Teixeira, S.L.M.; Veloso, V.; Morgado, M.G.; Guimarães, M. Impact of HIV-1 Subtypes on AIDS Progression in a Brazilian Cohort. AIDS Res. Hum. Retroviruses 2017, 33, 41–48. [Google Scholar] [CrossRef]
- Sabino, E.C.; Diaz, R.S.; Brigido, L.F.; Learn, G.H.; Mullins, J.I.; Reingold, A.L.; Duarte, A.J.; Mayer, A.; Busch, M.P. Distribution of HIV-1 subtypes seen in an AIDS clinic in Sao Paulo City, Brazil. AIDS 1996, 10, 1579–1584. [Google Scholar] [CrossRef] [PubMed]
- Brindeiro, R.M.; Diaz, R.S.; Sabino, E.C.; Morgado, M.G.; Pires, I.L.; Brigido, L.; Dantas, M.C.; Barreira, D.; Teixeira, P.R.; Tanuri, A. Brazilian Network for HIV Drug Resistance Surveillance (HIV-BResNet): A survey of chronically infected individuals. AIDS 2003, 17, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Palma, A.C.; Abecasis, A.B.; Vercauteren, J.; Carvalho, A.P.; Cabanas, J.; Vandamme, A.-M.; Camacho, R. Effect of human immunodeficiency virus type 1 protease inhibitor therapy and subtype on development of resistance in subtypes B and G. Infect. Genet. Evol. 2010, 10, 373–379. [Google Scholar] [CrossRef]
- Aghokeng, A.F.; Vergne, L.; Mpoudi-Ngole, E.; Mbangue, M.; Deoudje, N.; Mokondji, E.; Nambei, W.S.; Peyou-Ndi, M.M.; Moka, J.-J.L.; Delaporte, E.; et al. Evaluation of transmitted HIV drug resistance among recently-infected antenatal clinic attendees in four Central African countries. Antivir. Ther. 2009, 14, 401–411. [Google Scholar]
- Olson, A.; Bannert, N.; Sönnerborg, A.; de Mendoza, C.; Price, M.; Zangerle, R.; Chaix, M.-L.; Prins, M.; Kran, A.-M.B.; Gill, J.; et al. Temporal trends of transmitted HIV drug resistance in a multinational seroconversion cohort. AIDS 2017, 32, 161–169. [Google Scholar] [CrossRef]
- Günthard, H.F.; Calvez, V.; Paredes, R.; Pillay, D.; Shafer, R.W.; Wensing, A.M.; Jacobsen, D.M.; Richman, U.D. Human Immunodeficiency Virus Drug Resistance: 2018 Recommendations of the International Antiviral Society–USA Panel. Clin. Infect. Dis. 2018, 68, 177–187. [Google Scholar] [CrossRef]
- Coelho, L.P.O.; Matsuda, E.M.; Nogueira, R.S.; de Moraes, M.J.; Jamal, L.F.; Madruga, J.V.R.; Tancredi, M.V.; de Leão, A.C.Q.; Soldi, G.D.F.R.; de Macedo Brígido, L.F.; et al. Prevalence of HIV-1 transmitted drug resistance and viral suppression among recently diagnosed adults in São Paulo, Brazil. Arch. Virol. 2019, 164, 699–706. [Google Scholar] [CrossRef]
- Gupta, R.K.; Gregson, J.; Parkin, N.; Haile-Selassie, H.; Tanuri, A.; Andrade Forero, L.; Kaleebu, P.; Watera, C.; Aghokeng, A.; Mutenda, N.; et al. HIV-1 drug resistance before initiation or re-initiation of first-line antiretroviral therapy in low-income and middle-income countries: A systematic review and meta-regression analysis. Lancet Infect. Dis. 2018, 18, 346–355. [Google Scholar] [CrossRef]
- Ávila-Ríos, S.; Sued, O.; Rhee, S.-Y.; Shafer, R.W.; Reyes-Terán, G.; Ravasi, G. Surveillance of HIV Transmitted Drug Resistance in Latin America and the Caribbean: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158560. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B.G.; Ibanescu, R.-I.; Hardy, I.; Roger, M. Genotypic and Phylogenetic Insights on Prevention of the Spread of HIV-1 and Drug Resistance in “Real-World” Settings. Viruses 2018, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Tebit, D.M.; Arts, E.J. Tracking a century of global expansion and evolution of HIV to drive understanding and to combat disease. Lancet Infect. Dis. 2011, 11, 45–56. [Google Scholar] [CrossRef]
- Bila, D.C.A.; Boullosa, L.T.; Vubil, A.S.; Mabunda, N.J.; Abreu, C.M.; Ismael, N.; Jani, I.; Tanuri, A. Trends in Prevalence of HIV-1 Drug Resistance in a Public Clinic in Maputo, Mozambique. PLoS ONE 2015, 10, e0130580. [Google Scholar] [CrossRef]
- Bila, D.C.A.; Young, P.; Merks, H.; Vubil, A.S.; Mahomed, M.; Augusto, A.; Abreu, C.M.; Mabunda, N.J.; Brooks, J.I.; Tanuri, A.; et al. Evolution of Primary HIV Drug Resistance in a Subtype C Dominated Epidemic in Mozambique. PLoS ONE 2013, 8, e68213. [Google Scholar] [CrossRef]
- Praticò, L.; Pizzol, D. Health-care services for young people with HIV in Mozambique. Lancet Child Adolesc. Health 2018, 2, e12. [Google Scholar] [CrossRef]
- Castelbranco, E.P.A.F.; da Silva Souza, E.; Cavalcanti, A.M.S.; Martins, A.N.; de Alencar, L.C.A.; Tanuri, A. Frequency of Primary Resistance to Antiretroviral Drugs and Genetic Variability of HIV-1 Among Infected Pregnant Women Recently Diagnosed in Luanda-Angola. AIDS Res. Hum. Retroviruses 2010, 26, 1313–1316. [Google Scholar] [CrossRef]
- Wilhelmson, S.; Mansson, F.; Lopatko Lindman, J.; Biai, A.; Esbjörnsson, J.; Norrgren, H.; Jansson, M.; Medstrand, P. Prevalence of HIV-1 pretreatment drug resistance among treatment naïve pregnant women in Bissau, Guinea Bissau. PLoS ONE 2018, 13, e0206406. [Google Scholar] [CrossRef]
- Schmidt, D.; Kollan, C.; Fätkenheuer, G.; Schülter, E.; Stellbrink, H.-J.; Noah, C.; Jensen, B.-E.O.; Stoll, M.; Bogner, J.R.; Eberle, J.; et al. Estimating Trends in the Proportion of Transmitted and Acquired HIV Drug Resistance in a Long Term Observational Cohort in Germany. PLoS ONE 2014, 9, e104474. [Google Scholar] [CrossRef]
- Rojas Sánchez, P.; Domínguez, S.; Jiménez De Ory, S.; Prieto, L.; Rojo, P.; Mellado, P.; Navarro, M.; Delgado, R.; Ramos, J.T.; Holguín, Á. Trends in Drug Resistance Prevalence, HIV-1 Variants and Clinical Status in HIV-1-infected Pediatric Population in Madrid. Pediatr. Infect. Dis. J. 2018, 37, e48–e57. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, E.; Chan, Y.-T.; Aghaizu, A.; Bibby, D.F.; Murphy, G.; Tosswill, J.; Harris, R.J.; Myers, R.; Field, N.; Delpech, V.; et al. Enhanced surveillance of HIV-1 drug resistance in recently infected MSM in the UK. J. Antimicrob. Chemother. 2016, 72, 227–234. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Naive | Treatment Experienced | p | ||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | Overall (n = 5177) | Total (n = 3552) | No TDR (n = 3210) | With TDR (n =342) | Total (n = 1589) | No ADR (n = 609) | With ADR (n = 980) | |
| Age | ||||||||
| median ± IQR | 39 (32–489) | 39 (31–49) | 39 (31–48) | 40 (31–49) | 40 (33–47) | 39 (33–46) | 40 (34–48) | 0.088 |
| Gender | ||||||||
| Number (%) | 0.077 | |||||||
| Male | 3294 (63.4) | 2288 (64.4) | 2060 (64.2) | 228 (66.7) | 983 (61.9) | 352 (57.8) | 631 (64.4) | |
| Female | 1839 (35.5) | 1233 (34.7) | 1124(35) | 109 (31.9) | 593 (37.63) | 248 (40.7) | 345 (35.2) | |
| Unknown | 44 (0.8) | 31 (0.9) | 26 (0.8) | 5 (1.5) | 13 (0.8) | 9 (1.5) | 4 (0.4) | |
| geographical origin | 0.004 | |||||||
| PALOPS | 1281 (24.7) | 853 (24) | 774 (24.1) | 79 (23.1) | 395 (24.9) | 153 (25.1) | 242 (24.7) | |
| Brazil | 209 (4) | 164 (4.6) | 150 (4.7) | 14 (4.1) | 42 (2.6) | 15 (2.5) | 27 (2.8) | |
| Portugal | 3687 (71.2) | 2535 (71.4) | 2286 (71.2) | 249 (72.8) | 1152 (72.5) | 441 (72.4) | 711 (72.6) | |
| HIV-1 RNA level (Log10 copies/mL) | ||||||||
| median ± IQR | 4.64 (3.9–5.2) | 4.8 (4.1–5.3) | 4.8 (4.2–5.3) | 4.64 (4.09–5.1) | 4.33 (3.6–4.9) | 4.65 (3.8–5.2) | 4.15 (3.5–4.7) | p< 0.0001 |
| CD4 countss (cells/µL) | ||||||||
| median ± IQR | 281 (128–461) | 323(133–498) | 319 (129–493) | 3170 (209–549) | 244 (121–408) | 229 (125–386) | 248 (118–420.7) | p < 0.0001 |
| Overall (n = 5177) | Host Country (n = 3687) | Migrants (n = 1490) | p | ||
|---|---|---|---|---|---|
| Variables | Portugal | Brazil | PALOP | ||
| Agemedian ± IQR | 39 (32–48) | 39 (32–47) | 34 (28–41) | 41 (33–50) | <0.0001 |
| Gender(number (%) | <0.0001 | ||||
| Male | 3294 (64) | 2563/3687(70) | 137/209 (66) | 594/1267 (46.9) | |
| Female | 1839 (36) | 1095/3687 (30) | 71/209 (34) | 673/1267 (53.1) | |
| Subtype(number (%) | <0.0001 | ||||
| 02_AG | 499/5177 (9.6) | 148/3687 (4) | 4/209 (1.9) | 347/1281 (27) | |
| A | 174/5177 (3.4) | 98/3687 (2.7) | 6/209 (2.9) | 70/1281 (5.5) | |
| B | 1853/5177 (35.8) | 1623/3687 (44) | 122/209 (59) | 108/1281 (8.4) | |
| C | 361/5177 (7) | 126/3687 (3.4) | 25/209 (12) | 210/1281 (16.4) | |
| D | 42/5177 (0.8) | 15/3687 (0.4) | 1/209 (0.5) | 26/1281 (2) | |
| F1 | 185/5177 (3.6) | 116/3687 (3.1) | 12/209 (5.7) | 57/1281 (4.4) | |
| G | 1382/5177 (26.7) | 1143/3687 (31) | 18/209 (8.6) | 221/1281 (17.3) | |
| Others | 18/5177 (0.4) | 5/3687 (0.1) | 0 | 13/1281 (1) | |
| Recombinants | 663/5177 (12.8) | 413/3687 (11.2) | 21/209 (10) | 229/1281 (17.9) | |
| ANY_TDR(number (%) | 342/3552 (9.6, 8.6–10.7) | 249/2535 (9.8, 8.6–10.9) | 14/164 (8.5, 4.2–10.7) | 79/853 (9.2, 7.2–11.1) | 0.795 |
| NRT(number (%) | 144/3552 (4.1, 3.4–4.7) | 98/2535 (3.9, 3.1–4.6) | 4/164 (2.4, 0.9–6.1) | 42/853(4.9, 3.4–6.3) | 0.224 |
| NNRT(number (%) | 186/3552 (5.2, 4.4–5.9) | 121/2535 (4.8, 4–5.6) | 90.055 (5.5, 2.9–10) | 56/853 (6.5, 5–8.4) | 0.125 |
| PI(number (%) | 103/3552 (2.9, 2.4–3.5) | 95/2535 (3.7, 2.9–4.4) | 2/164 (1.2, 0.4–2.9) | 6/853 (0.7, 0.1- 1.2) | <0.0001 |
| ANY _ADR(number (%) | 980/1589(61.7, 58.6–63.4) | 711/1152(62, 59.2–64.8) | 27/42 (64, 49.5–78.5) | 242/395(61, 56.2–65.8) | 0.676 |
| VLmedian ± IQR | 4.6 (3.9–5.2) | 4.66(3.9 – 5.2) | 4.7 (4.04– 5.28) | 4.5 (3.8–5.2) | 0,29 |
| CD4median ± IQR | 281(128–461) | 289 (130 – 470) | 370(130–529) | 217 (113–369) | <0.0001 |
| Variables | Naïve | Treated | ||||
|---|---|---|---|---|---|---|
| Any TDR | Susceptible | p | Any ADR | Susceptible | p | |
| Agemedian ± IQR | 41.2 (31.7–49) | 40.4 (31–48) | 0.47 | 41.2 (34–48) | 40 (33–46) | 0.0225 |
| Gender(number (%) | 0.281 | 0.018 | ||||
| Male | 228/2288 (9.9, 8.6.11.1) | 91.1% | 631/983 (64.1, 61.1–67.1) | 39% | ||
| Female | 109/1233 (8.8, 7.2–10.3) | 90.1% | 345/593 (58.1, 54.1–62) | 37% | ||
| Countries(number (%) | 0.1614 | 0.416 | ||||
| Angola | 21/212 (9.9, 5.88–13.9) | 90.1% | 92/144 (63.8, 55.9–71.6) | 36.2% | ||
| Brazil | 14/164 (8.5, 4.23–12.7)) | 91.5% | 27/42 (64, 49.4–78.5) | 36% | ||
| Cape Verde | 14/186 (7.6, 3.79–11.4)) | 92.4% | 72/107 (67.2, 58.3–76.1) | 32.8% | ||
| Guinea-Bissau | 24/307 (7.8, 4.8–10.8) | 92.2% | 49/95 (51.5, 41.4–61.5) | 48.5% | ||
| Mozambique | 16/92 (17.4, 9.6- 25.1) | 82.6% | 17/29 (58.6, 40.6–76.5) | 41.4% | ||
| Sao Tome and Principe | 4/56 (7.1, 3.7–13.8) | 92.9% | 12/20 (60, 38.5–81.4) | 40% | ||
| Portugal | 249/2535 (9.8, 8.6–10.9) | 90.2% | 711/1152 (61.7, 58.9–64.5) | 38.3% | ||
| Subtype(number (%) | 0.005 | 0.02 | ||||
| 02_AG | 30/365 (8.2, 4.2–10.7) | 92.5% | 61/120 (50.2, 41.2–59.1) | 51.2% | ||
| A | 7/144(4.9, 1.3–8.2) | 95.2% | 16/28 (57, 38.6–75.3) | 43% | ||
| B | 141/1278 (11, 9.8–13.2) | 88.5% | 385/570 (67.2, 63.3–71) | 32.8% | ||
| C | 36/261 (13.7, 9.6–18) | 86.2% | 54/92 (58.6, 48.5–68.6) | 41.4% | ||
| D | 3/31(9.6, 0.7–19.9) | 90.4% | 8/11 (72.7, 46.3–99) | 27.3% | ||
| F1 | 17/153 (11, 6–16) | 89% | 18/31 (58, 40.6–75.3) | 42% | ||
| G | 57/843 (6.8, 5.1.8.5) | 93.2% | 317/537 (59, 54.8–63.1) | 41% | ||
| Recombinants | 51/464 (10.9, 8.1–13.2) | 89.3% | 119/195 (61, 54.1–67.8) | 39.8% | ||
| VLmedian ± IQR | 4.6 (4.0 – 5.1) | 4.7 (4.2– 5.4) | 0.011 | 4.1 (3.5 – 4.7) | 4.5 (3.8–5.2) | <0.0001 |
| CD4median ± IQR | 388 (209 – 549) | 345 (129–493) | 0.024 | 291 (118 – 420) | 287 (125–386) | 0.452 |
| Naive | adjusted | Treated | Adjusted | |||||
|---|---|---|---|---|---|---|---|---|
| Variables | Sig | OR (95% C.I Expected) | Sig | OR (95% C.I Expected) | Sig | OR (95% C.I Expected) | Sig | OR (95% C.I Expected) |
| Gender (Female(a)/Male, n = 1475) | 0.913 | 1.024(0.666–1.576) | 0.148 | 1.332(0.903–1.966) | ||||
| Age (n = 1465) | 0.026 | 1.021(1.0029–1.002) | 0.938 | 1.001(0.985–1.016) | 0.001 | 1.032(1.013–1.053) | 0.003 | 1.043(1.014–1.072) |
| Country (n = 1490) | ||||||||
| Angola (No(a)/Yes) | 0.666 | 1.119(0.671–1.867) | 0.482 | 1.159(0.767–1.752) | ||||
| Brazil (No(a)/Yes) | 0.768 | 0.914(0.505–1.657) | 0.724 | 1.138(0.587–2.208) | ||||
| Cape Verde (No(a)/Yes) | 0,398 | 0.775(0.429–1.401) | 0.162 | 1.389(0.877–2.200) | ||||
| Guinea (No(a)/Yes) | 0.335 | 0.788(0.485–1.280) | 0.025 | 0.591(0.373–0.935) | 0.932 | 1.030(0.521–2.036) | ||
| Mozambique (No(a)/Yes) | 0.005 | 2.319(1.289–4.172) | <0.001 | 2.71(1.605–2.730) | 0.737 | 0.877(0.408–1.886) | ||
| Sao Tome (No(a)/Yes) | 0.594 | 0.754(0.266–2.133) | 0.884 | 0.934(0.374–2.334) | ||||
| Subtype (n = 1490) | ||||||||
| CRF02_AG (No(a)/Yes) | 0.320 | 0.766(0.453–1.290) | 0.007 | 0.521(0.324–0.839) | ||||
| A (No(a)/Yes) | 0.180 | 0.376(0.090–1.570) | 0.670 | 0.825(0.340–2.002) | ||||
| B (No(a)/Yes) | 0.027 | 1.780(1.067–2.969) | 0.022 | 1.719(1.082–2.730) | 0.011 | 2.169(1.191–3.950) | 0.019 | 2.687(1.175–6.143) |
| C (No(a)/Yes) | 0.141 | 1.484(0.877–2.510) | 0.437 | 0.8707(0.470–1.386) | ||||
| D (No(a)/Yes) | 0.599 | 0.580(0.076–4.407) | 0.324 | 2.2183(0.455–10.803) | ||||
| F (No(a)/Yes) | 0.061 | 2.045(0.967–4.323) | 0.254 | 0.525(0.173–1.589) | ||||
| G (No(a)/Yes) | 0.112 | 0.545(0.258–1.151) | 0.168 | 1.407(0.866–2.286) | ||||
| Rec (No(a)/Yes) | 0.377 | 0.752(0.400–1.414) | 0.701 | 1.102(0.670–1-813) | ||||
| CD4 (n = 375) | 0.355 | 1.001(0.999–1.003) | 0.231 | 1.000(0.999–1.003) | ||||
| VL(731) | 0.294 | 0.803(0.532–1.210) | 0.002 | 0.634(0.477–0.842) | 0.001 | 0,600(0.446–0.808) | ||
| Sampling year | 0.003 | 1.085(1.029–1.145) | 0.007 | 1.078(1.021–1.139) | 0.005 | 0.935(0.892–0.979) | 0.001 | 0.821(0.734–0.919) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pimentel, V.; Pingarilho, M.; Alves, D.; Diogo, I.; Fernandes, S.; Miranda, M.; Pineda-Peña, A.-C.; Libin, P.; Martins, M.R.O.; Vandamme, A.-M.; et al. Molecular Epidemiology of HIV-1 Infected Migrants Followed Up in Portugal: Trends between 2001–2017. Viruses 2020, 12, 268. https://doi.org/10.3390/v12030268
Pimentel V, Pingarilho M, Alves D, Diogo I, Fernandes S, Miranda M, Pineda-Peña A-C, Libin P, Martins MRO, Vandamme A-M, et al. Molecular Epidemiology of HIV-1 Infected Migrants Followed Up in Portugal: Trends between 2001–2017. Viruses. 2020; 12(3):268. https://doi.org/10.3390/v12030268
Chicago/Turabian StylePimentel, Victor, Marta Pingarilho, Daniela Alves, Isabel Diogo, Sandra Fernandes, Mafalda Miranda, Andrea-Clemencia Pineda-Peña, Pieter Libin, M. Rosário O. Martins, Anne-Mieke Vandamme, and et al. 2020. "Molecular Epidemiology of HIV-1 Infected Migrants Followed Up in Portugal: Trends between 2001–2017" Viruses 12, no. 3: 268. https://doi.org/10.3390/v12030268
APA StylePimentel, V., Pingarilho, M., Alves, D., Diogo, I., Fernandes, S., Miranda, M., Pineda-Peña, A.-C., Libin, P., Martins, M. R. O., Vandamme, A.-M., Camacho, R., Gomes, P., & Abecasis, A. (2020). Molecular Epidemiology of HIV-1 Infected Migrants Followed Up in Portugal: Trends between 2001–2017. Viruses, 12(3), 268. https://doi.org/10.3390/v12030268