Can Zika Virus Infection in High Risk Pregnant Women Be Differentiated on the Basis of Symptoms?

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
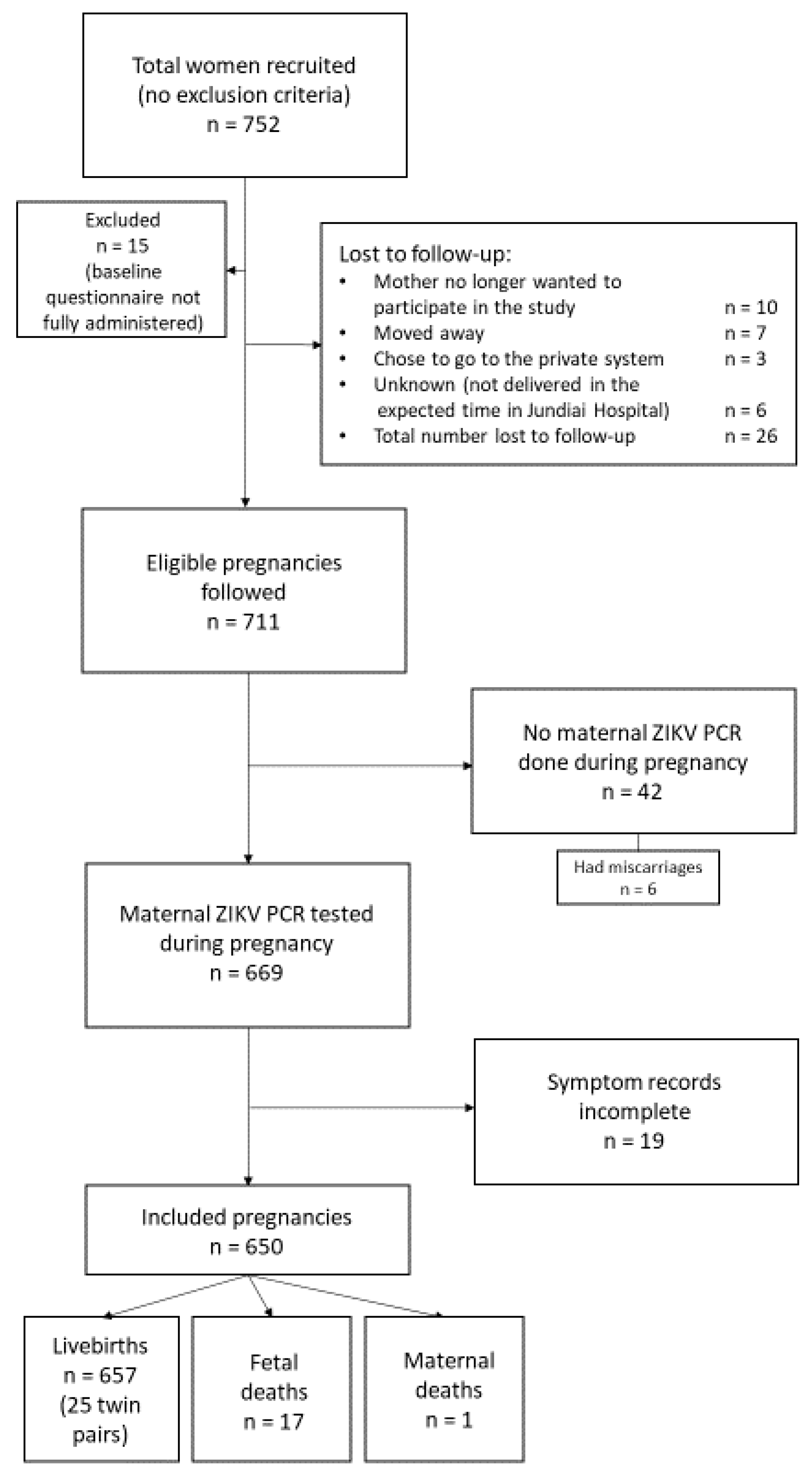
2.1. Study Design and Participants
2.2. Laboratory Procedures
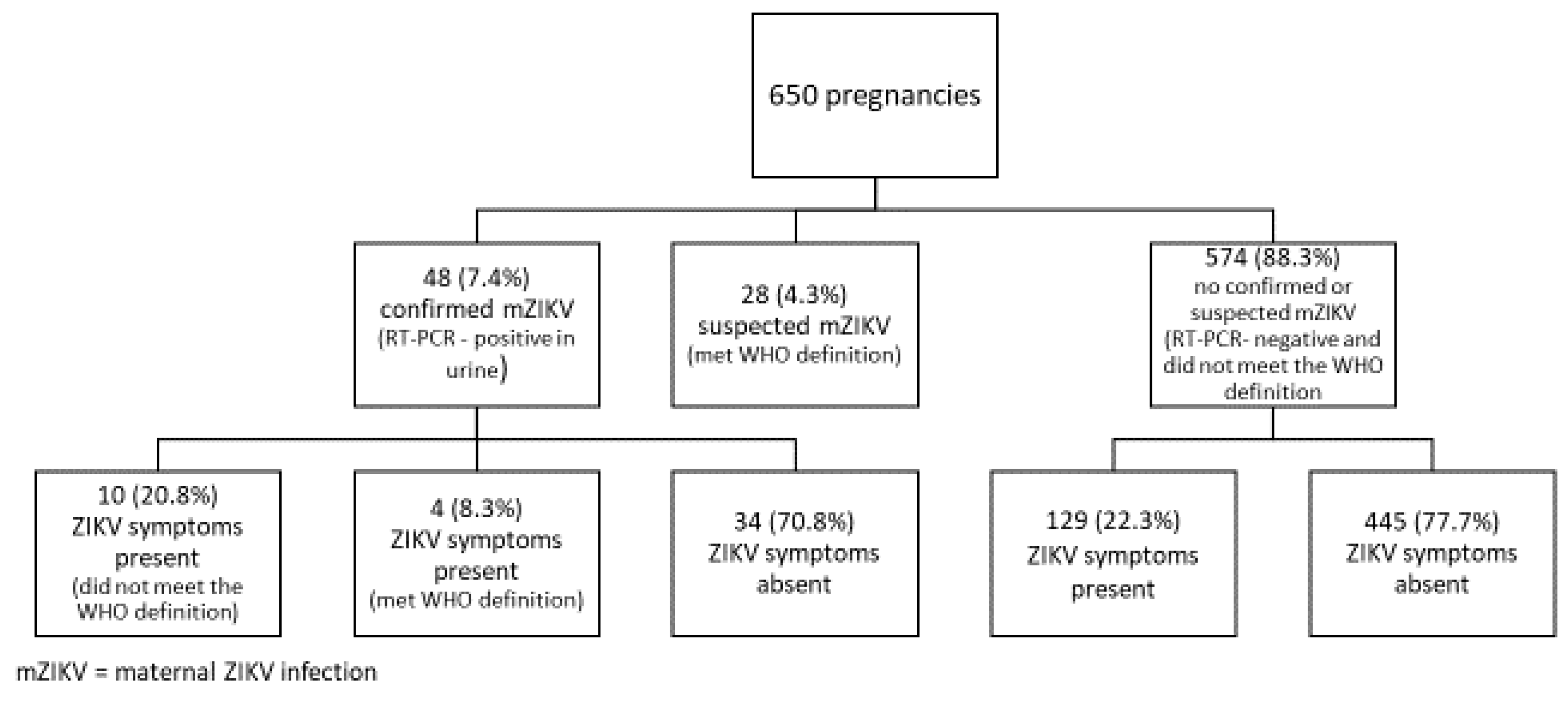
2.3. Neonatal Categorisation
2.4. Statistical Analysis
2.5. Sensitivity and Specificity
3. Results
3.1. Participant Characteristics
3.2. Additional Findings
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- ECDC. Rapid Risk Assessment. Zika Virus Epidemic in the Americas: Potential Association with Microcephaly and Guillain-Barre Syndrome; ECDC: Stockholm, Sweden, 2015. [Google Scholar]
- Duffy, M.R.; Chen, T.-H.; Hancock, W.T.; Powers, A.M.; Kool, J.L.; Lanciotti, R.S.; Pretrick, M.; Marfel, M.; Holzbauer, S.; DuBray, C.; et al. Zika virus outbreak on Yap Island, Federated States of Micronesia. N. Engl. J. Med. 2009, 360, 2536–2543. [Google Scholar] [CrossRef]
- Haby, M.M.; Pinart, M.; Elias, V.; Reveiz, L. Prevalence of asymptomatic Zika virus infection: A systematic review. Bull. World Heal. Organ. 2018, 96, 402–413D. [Google Scholar] [CrossRef] [PubMed]
- Flamand, C.; Fritzell, C.; Matheus, S.; Dueymes, M.; Carles, G.; Favre, A.; Enfissi, A.; Adde, A.; Demar, M.; Kazanji, M.; et al. The proportion of asymptomatic infections and spectrum of disease among pregnant women infected by Zika virus: Systematic monitoring in French Guiana, 2016. Eurosurveillance 2017, 22. [Google Scholar] [CrossRef] [PubMed]
- Brasil, P.; Pereira, J.P., Jr.; Moreira, M.E.; Ribeiro Nogueira, R.M.; Damasceno, L.; Wakimoto, M.; Rabello, R.S.; Valderramos, S.G.; Halai, U.-A.; Salles, T.S.; et al. Zika virus infection in pregnant women in Rio de Janeiro. N. Eng. J. Med. 2016, 375, 2321–2334. [Google Scholar] [CrossRef] [PubMed]
- Daudens-Vaysse, E.; Ledrans, M.; Gay, N.; Ardillon, V.; Cassadou, S.; Najioullah, F.; Leparc-Goffart, I.; Rousset, D.; Herrmann, C.; Cesaire, R.; et al. Zika emergence in the French Territories of America and description of first confirmed cases of Zika virus infection on Martinique, November 2015 to February 2016. Eurosurveillance 2016, 21. [Google Scholar] [CrossRef] [PubMed]
- Hoen, B.; Schaub, B.; Funk, A.L.; Ardillon, V.; Boullard, M.; Cabié, A.; Callier, C.; Carles, G.; Cassadou, S.; Césaire, R.; et al. Pregnancy outcomes after ZIKV infection in French Territories in the Americas. N. Eng. J. Med. 2018, 378, 985–994. [Google Scholar] [CrossRef]
- Nogueira, M.; Júnior, N.N.; Estofolete, C.; Terzian, A.B.; Guimarães, G.; Zini, N.; Da Silva, R.A.; Silva, G.D.; Franco, L.J.; Rahal, P.; et al. Adverse birth outcomes associated with Zika virus exposure during pregnancy in São José do Rio Preto, Brazil. Clin. Microbiol. Infect. 2018, 24, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Sardi, S.I.; Somasekar, S.; Naccache, S.N.; Bandeira, A.C.; Tauro, L.B.; Campos, G.S.; Chiu, C.Y. Coinfections of Zika and Chikungunya Viruses in Bahia, Brazil, identified by metagenomic next-generation sequencing. J. Clin. Microbiol. 2016, 54, 2348–2353. [Google Scholar] [CrossRef]
- Lobkowicz, L.; Ramond, A.; Clemente, N.S.; Ximenes, R.A.D.A.; Miranda-Filho, D.D.B.; Montarroyos, U.R.; Martelli, C.M.T.; De Araújo, T.V.B.; Brickley, E.B. The frequency and clinical presentation of Zika virus coinfections: A systematic review. BMJ Glob. Heal. 2020, 5, e002350. [Google Scholar] [CrossRef]
- WHO. Zika Virus Disease—Interim Case Definition. Available online: http://apps.who.int/iris/handle/10665/204381 (accessed on 27 March 2018).
- Paixao, E.; Leong, W.-Y.; Rodrigues, L.C.; Wilder-Smith, A. Asymptomatic prenatal Zika virus infection and Congenital Zika Syndrome. Open Forum Infect. Dis. 2018, 5. [Google Scholar] [CrossRef]
- Freitas, A.R.R.; Napimoga, M.H.; Donalisio, M.R. Could clinical symptoms be a predictor of complications in Zika virus infection? Lancet 2016, 388, 338. [Google Scholar] [CrossRef]
- Cauchemez, S.; Besnard, M.; Garel, C.; Fontanet, A.; Mallet, H.-P. Could clinical symptoms be a predictor of complications in Zika virus infection?—Authors’ reply. Lancet 2016, 388, 338–339. [Google Scholar] [CrossRef]
- NIH - Eunice Kennedy Shriver National Institute for Child Health and Human Development. High Risk Pregnancy. Available online: https://www.nichd.nih.gov/health/topics/high-risk (accessed on 27 March 2018).
- Lanciotti, R.S.; Kosoy, O.L.; Laven, J.J.; Velez, J.O.; Lambert, A.J.; Johnson, A.J.; Stanfield, S.M.; Duffy, M.R. Genetic and serologic properties of Zika Virus associated with an epidemic, Yap State, Micronesia, 2007. Emerg. Infect. Dis. 2008, 14, 1232–1239. [Google Scholar] [CrossRef]
- Bingham, A.M. Comparison of test results for Zika Virus RNA in Urine, Serum, and Saliva specimens from persons with travel-associated Zika virus disease—Florida, 2016. MMWR. Morb. Mortal. Wkly. Rep. 2016, 65, 475–478. [Google Scholar] [CrossRef]
- Paz-Bailey, G.; Rosenberg, E.S.; Doyle, K.; Muñoz-Jordán, J.L.; Santiago, G.A.; Klein, L.; Perez-Padilla, J.; Medina, F.A.; Waterman, S.H.; Gubern, C.G.; et al. Persistence of Zika virus in body fluids—Preliminary report. N. Eng. J. Med. 2017, 379, 1234–1243. [Google Scholar] [CrossRef]
- Lanciotti, R.S.; Lambert, A.J.; Holodniy, M.; Saavedra, S.; Signor, L.D.C.C. Phylogeny of Zika virus in Western Hemisphere, 2015. Emerg. Infect. Dis. 2016, 22, 933–935. [Google Scholar] [CrossRef]
- Intergrowth-21st. INTERGROWTH-21st Newborn Size at Birth Chart. Available online: https://intergrowth21.tghn.org/articles/intergrowth-21st-newborn-size-birth-chart/ (accessed on 7 October 2016).
- Intergrowth-21st. Newborn biometry by Intergrowth-21st standards/references. Online calculator. Available online: http://intergrowth21.ndog.ox.ac.uk (accessed on 1 July 2018).
- Villar, J.; Ismail, L.C.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef]
- Mor, G.; Cardenas, I. The immune system in pregnancy: A unique complexity. Am. J. Reprod. Immunol. 2010, 63, 425–433. [Google Scholar] [CrossRef]
- Wæhre, T.; Maagard, A.; Tappe, D.; Cadar, D.; Schmidt-Chanasit, J. Zika virus infection after travel to Tahiti, December 2013. Emerg. Infect. Dis. 2014, 20, 1412–1414. [Google Scholar] [CrossRef]
- CDC. Zika Virus. Symptoms, Testing and Treatment. Available online: https://www.cdc.gov/zika/symptoms/symptoms.html (accessed on 10 October 2018).
- Stettler, K.; Beltramello, M.; Espinosa, D.A.; Graham, V.; Cassotta, A.; Bianchi, S.; Vanzetta, F.; Minola, A.; Jaconi, S.; Mele, F.; et al. Specificity, cross-reactivity, and function of antibodies elicited by Zika virus infection. Science 2016, 353, 823–826. [Google Scholar] [CrossRef]
- Petridou, C.; Simpson, A.; Charlett, A.; Lyall, H.; Dhesi, Z.; Aarons, E. Zika virus infection in travellers returning to the United Kingdom during the period of the outbreak in the Americas (2016-17): A retrospective analysis. Travel Med. Infect. Dis. 2019, 29, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Clemente, N.S.; Brickley, E.B.; Paixão, E.S.; De Almeida, M.F.; Gazeta, R.E.; Vedovello, D.; Rodrigues, L.C.; Witkin, S.S.; Passos, S.D. Zika virus infection in pregnancy and adverse fetal outcomes in São Paulo State, Brazil: A prospective cohort study. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Case Definition | Description |
|---|---|
| Confirmed case | A person with laboratory confirmation of recent Zika virus infection:
|
| Suspected case | A person presenting with rash and/or fever and at least one of the following signs or symptoms:
|
| Variable | ZIKV Symptoms Present * (n = 171) | ZIKV Symptoms Absent (n = 479) | p-Value |
|---|---|---|---|
| Age | |||
| 13–19 years | 32 (18.7%) | 65 (13.6%) | 0.07 |
| 20–34 years | 112 (65.5%) | 305 (63.7%) | |
| 35–46 years | 27 (15.8%) | 109 (22.8%) | |
| Missing | 0 | 0 | |
| Education | |||
| ≤8 years | 30 (17.8%) | 78 (16.6%) | 0.96 |
| 9–11 years | 40 (23.7%) | 106 (22.6%) | |
| 12 years | 74 (43.8%) | 210 (44.8%) | |
| >12 years | 25 (14.8%) | 75 (16.0%) | |
| Missing | 2 (1.2%) | 9 (1.9%) | |
| Ethnicity/race | |||
| White | 94 (56.3%) | 246 (52.5%) | 0.86 $ |
| Mixed race | 55 (32.9%) | 165 (35.2%) | |
| Black | 15 (9.0%) | 49 (10.5%) | |
| Other (Asian/Indigenous) | 3 (1.8%) | 9 (1.9%) | |
| Missing | 4 (2.3%) | 10 (2.1%) | |
| Relationship with partner | |||
| Married/co-habiting | 129 (76.3%) | 361 (76.7%) | 0.93 |
| Single/divorced/widowed | 40 (23.7%) | 111 (23.4%) | |
| Missing | 2 (1.2%) | 8 (1.7%) | |
| Type of delivery | |||
| Vaginal/forceps | 75 (51.4%) | 200 (50.4%) | 0.84 |
| C-section | 71 (48.6%) | 197 (49.6%) | |
| Missing | 2 (1.4%) | 1 (0.25%) | |
| ZIKV RT–PCR status | |||
| Positive in urine | 14 (8.2%) | 34 (7.1%) | 0.64 |
| Negative in urine | 157 (91.8%) | 445 (92.9) |
| No. (%) Positive | ||||
|---|---|---|---|---|
| Signs/Symptoms | PCR-Positive n = 48 | PCR-Negative n = 602 | p-Value ** | |
| WHO criteria | Fever | 8 (16.7) | 82 (13.6) | 0.55 |
| Arthralgia/arthritis | 5 (10.4) | 68 (11.3) | 0.85 | |
| Rash | 2 (4.2) | 32 (5.3) | 0.73 | |
| Conjunctivitis | 1 (2.1) | 19 (3.2) | 0.68 | |
| Other symptoms | Myalgia | 4 (8.3) | 74 (12.3) | 0.42 |
| Headache | 25 (52.1) | 320 (53.2) | 0.89 | |
| Lymphadenopathy | 1 (2.1) | 33 (5.5) | 0.31 | |
| Total symptomatic | Fulfilled required WHO criteria * | 4 (8.3) | 28 (4.7) | 0.20 |
| Did not fulfill WHO criteria Total symptomatic | 10 (20.8) 14 (29.2) | 129 (21.4) 157 (26.1) | 0.20 0.69 | |
| No symptoms | 34 (70.8) | 445 (73.9) | 0.64 | |
| Symptomatic Women with the ZIKV Infection | ||||
|---|---|---|---|---|
| ZIKV RT–PCR-Positive | ZIKV RT–PCR-Negative | |||
| Have symptoms that fulfill the WHO standard case definition | Yes | 4 (TP) | 28 (FP) | PPV = TP / (TP + FP) = 12.5% |
| No | 10 (FN) | 157 (TN) | NPV = TN / (TN + FN) = 94.0% | |
| Sensitivity = TP / (TP + FN) = 28.6% | Specificity = TN / (FP + TN) = 84.9% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanchez Clemente, N.; Brickley, E.B.; Furquim de Almeida, M.; Witkin, S.S.; Duarte Passos, S.; the Jundiai Zika Cohort Group. Can Zika Virus Infection in High Risk Pregnant Women Be Differentiated on the Basis of Symptoms? Viruses 2020, 12, 1263. https://doi.org/10.3390/v12111263
Sanchez Clemente N, Brickley EB, Furquim de Almeida M, Witkin SS, Duarte Passos S, the Jundiai Zika Cohort Group. Can Zika Virus Infection in High Risk Pregnant Women Be Differentiated on the Basis of Symptoms? Viruses. 2020; 12(11):1263. https://doi.org/10.3390/v12111263
Chicago/Turabian StyleSanchez Clemente, Nuria, Elizabeth B. Brickley, Marcia Furquim de Almeida, Steven S. Witkin, Saulo Duarte Passos, and the Jundiai Zika Cohort Group. 2020. "Can Zika Virus Infection in High Risk Pregnant Women Be Differentiated on the Basis of Symptoms?" Viruses 12, no. 11: 1263. https://doi.org/10.3390/v12111263
APA StyleSanchez Clemente, N., Brickley, E. B., Furquim de Almeida, M., Witkin, S. S., Duarte Passos, S., & the Jundiai Zika Cohort Group. (2020). Can Zika Virus Infection in High Risk Pregnant Women Be Differentiated on the Basis of Symptoms? Viruses, 12(11), 1263. https://doi.org/10.3390/v12111263