


Assessing the Impact of Patient Characteristics on Genetic Clinical Pathways: A Regression Approach



Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
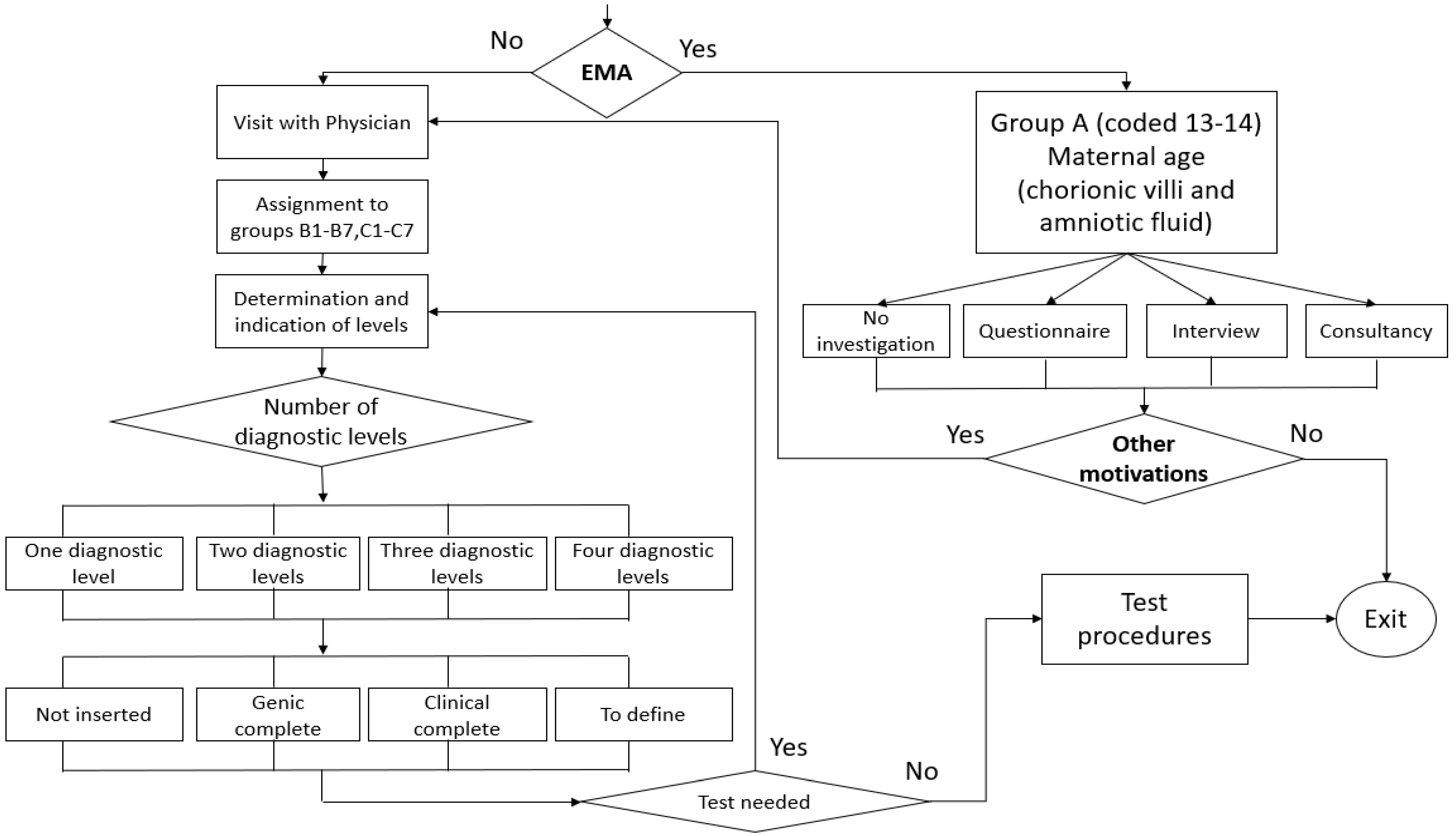
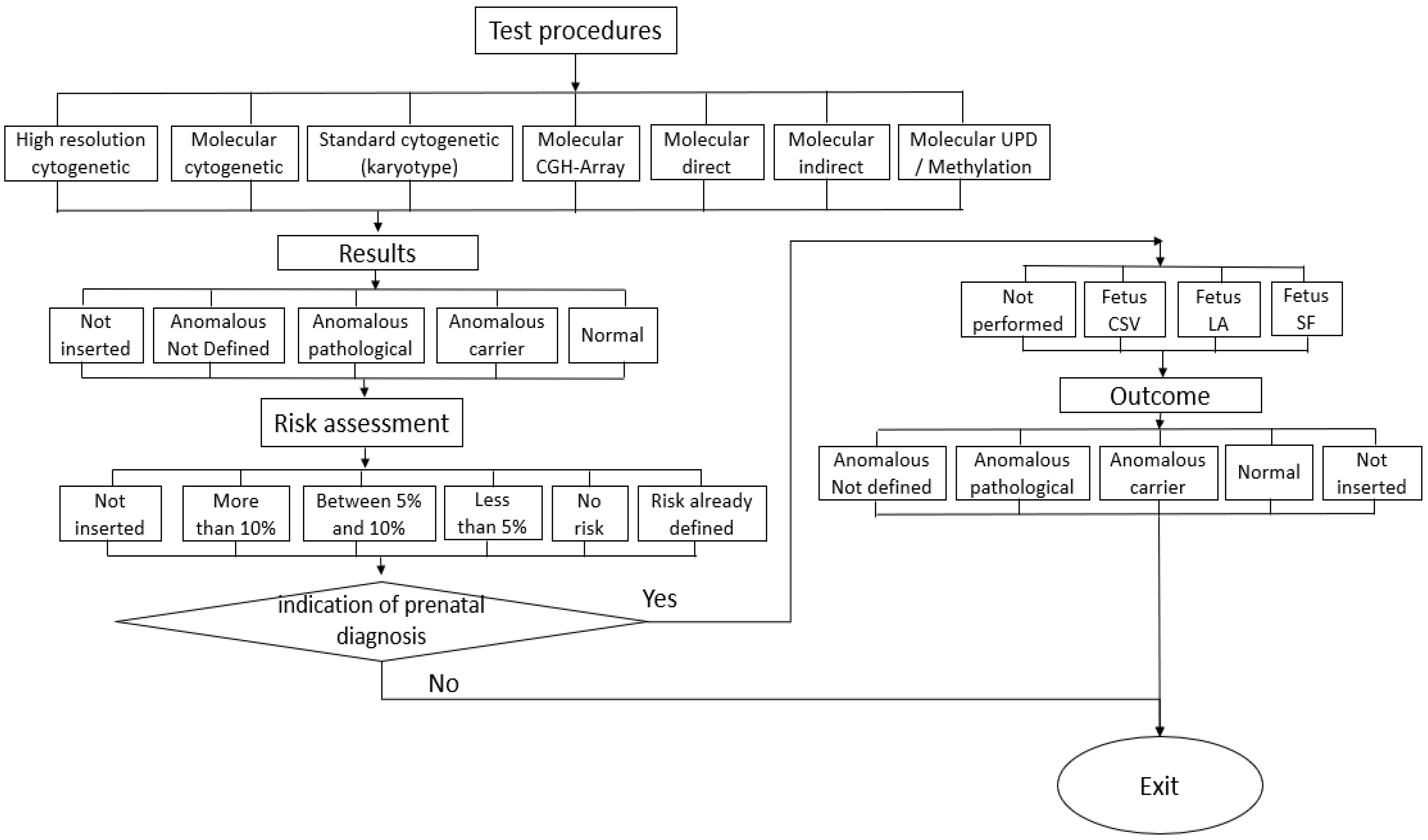
2.2. Pathways Identification
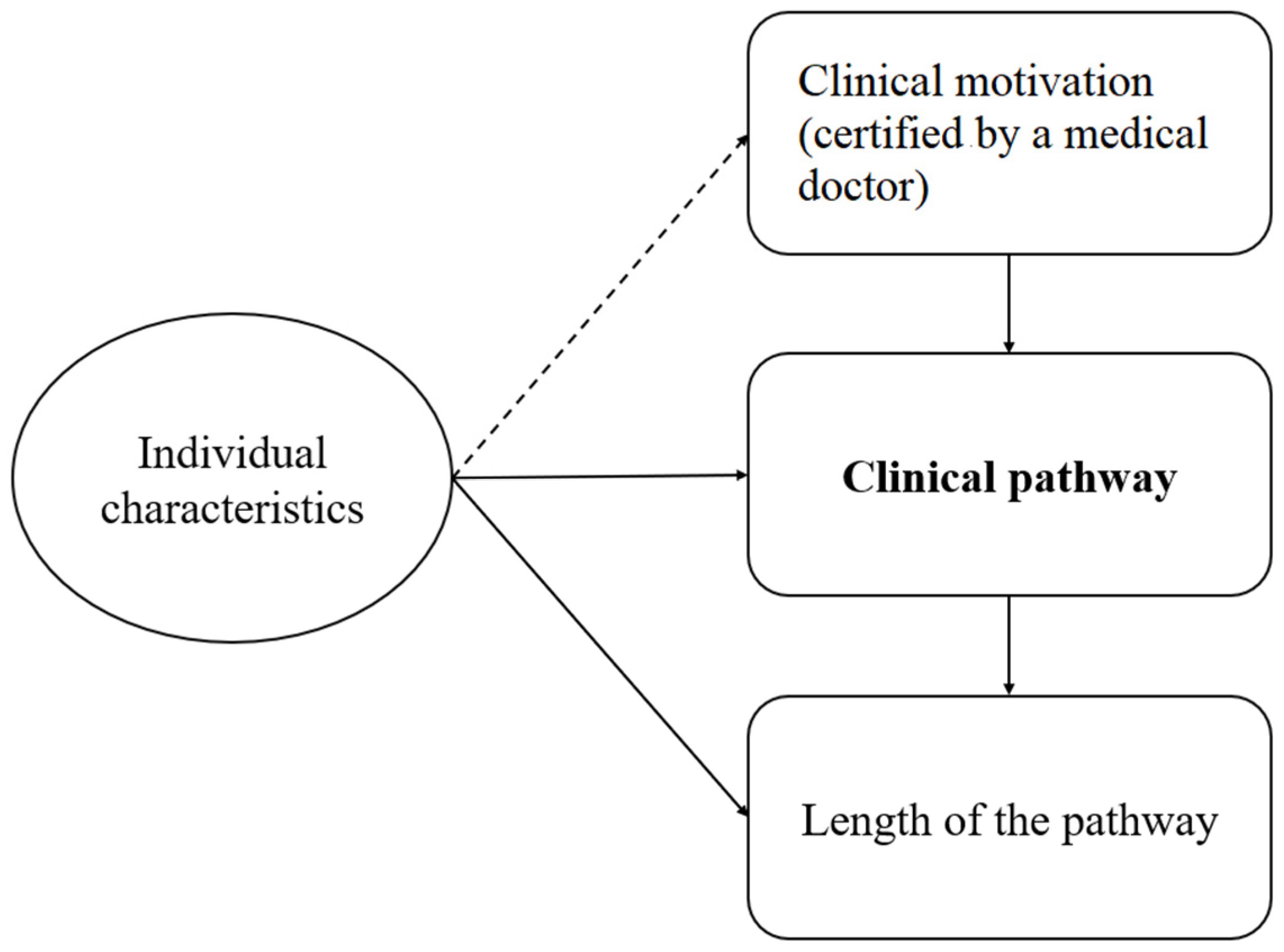
2.3. Analysis of the Determinants of Variability between and within Pathways
3. Results
3.1. Identification of Clinical Pathways
3.2. Main Descriptors and Indicators by Clinical Pathway and Nationality
3.3. The Definition of Clinical Pathways
3.4. Analysis of Variability between and within Pathways
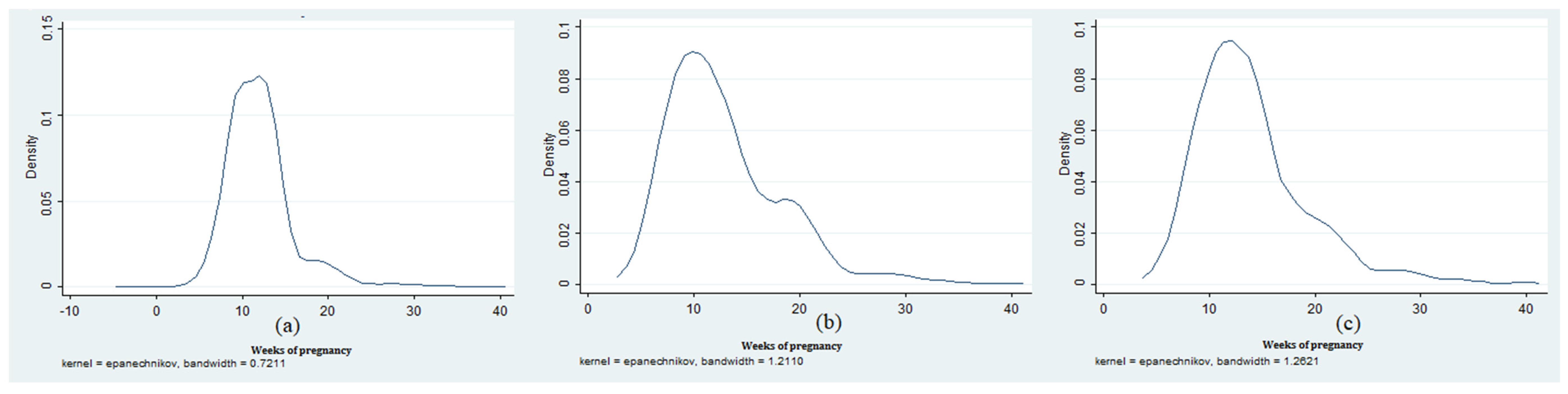
Descriptive Statistics
3.5. Statistical Analyses
3.5.1. Binary Models: Assignment to a Clinical Pathway—Full Sample
3.5.2. Pseudo-Poisson Maximum Likelihood and OLS: The Length of the Clinical Pathway—Full Sample
3.5.3. Binary Models: Assignment to a Clinical Pathway—Not-EMA Sample
3.5.4. Pseudo-Poisson Maximum Likelihood and OLS: The Length of the Clinical Pathway—Not-EMA Sample
3.5.5. Binary Models: Assignment to a Clinical Pathway: Foreign Mother Sample
3.5.6. Pseudo-Poisson Maximum Likelihood and OLS: The Length of the Clinical Pathway—Foreign Women Sample
3.5.7. Clinical Pathway Length: Individual Characteristics vs. Clinical Pathway
4. Discussion and Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gartner, J.B.; Abasse, K.S.; Bergeron, F.; Landa, P.; Lemaire, C.; Côté, A. Definition and conceptualization of the patient-centered care pathway, a proposed integrative framework for consensus: A Concept analysis and systematic review. BMC Health Serv. Res. 2022, 22, 558. [Google Scholar] [CrossRef] [PubMed]
- De Blaser, L.; Depreitere, R.; De Waele, K.; Vanhaecht, K.; Vlayen, J.; Sermeus, W. Defining pathways. J. Nurs. Manag. 2006, 14, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Ministerial Commission for Genetics in the Italian National Health Service. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_908_allegato.pdf (accessed on 15 July 2023).
- Vanhaecht, K.; Panella, M.; van Zelm, R.; Sermeus, W. An overview on the history and concept of care pathways as complex interventions. Int. J. Care Pathw. 2010, 14, 117–123. [Google Scholar] [CrossRef]
- Aspland, E.; Gartner, D.; Harper, P. Clinical pathway modelling: A literature review. Health Syst. 2021, 10, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Manktelow, M.; Iftikhar, A.; Bucholc, M.; McCann, M.; O’Kane, M. Clinical and operational insights from data-driven care pathway mapping: A systematic review. BMC Med. Inform. Decis. Mak. 2022, 22, 43. [Google Scholar] [CrossRef]
- Erdogan, T.G.; Tarhan, A. A goal-driven evaluation method based on process mining for healthcare processes. Appl. Sci. 2018, 8, 894. [Google Scholar] [CrossRef]
- Erdogan, T.G.; Tarhan, A. Systematic mapping of process mining studies in healthcare. IEEE Access 2018, 6, 24543–24567. [Google Scholar] [CrossRef]
- Gooch, P.; Roudsari, A. Computerization of workflows, guidelines, and care pathways: A review of implementation challenges for process-oriented health information systems. J. Am. Med. Inform. Assoc. 2011, 18, 738–748. [Google Scholar] [CrossRef]
- Kreys, E.D.; Koeller, J.M. Role of clinical pathways in health care provision: Focus on cancer treatment. Am. J. Health-Syst. Pharm. 2013, 70, 1081–1085. [Google Scholar] [CrossRef] [PubMed]
- Sisk, B.A.; Kerr, A.; King, K.A. Factors affecting pathways to care for children and adolescents with complex vascular malformations: Parental perspectives. Orphanet. J. Rare Dis. 2022, 17, 271. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.; Chou, S.; Pan, S.; Chen, Y. Mining time dependency patterns in clinical pathways. Int. J. Med. Inform. 2001, 62, 11–25. [Google Scholar] [CrossRef]
- Prokofyeva, E.S.; Zaytsev, R.D. Clinical pathways analysis of patients in medical institutions based on hard and fuzzy clustering methods. Bus. Inform. 2020, 14, 19–31. [Google Scholar] [CrossRef]
- He, J.A.; Yang, W. Clinical pathways in China—An evaluation. Int. J. Health Care Qual. Assur. 2015, 28, 394–411. [Google Scholar] [CrossRef] [PubMed]
- Zeleke, A.J.; Moscato, S.; Miglio, R.; Chiari, L. Length of Stay Analysis of COVID-19 Hospitalizations Using a Count Regression Model and Quantile Regression: A Study in Bologna, Italy. Int. J. Environ. Res. Public Health 2022, 19, 2224. [Google Scholar] [CrossRef] [PubMed]
- American College of Medical Genetics. Manual on Reimbursement for Medical Genetics Services; Williams, M.S., Ed.; Kendall Hunt: Dubuque, IW, USA, 2002. [Google Scholar]
- Monitoring and Evaluation of Diagnostic-Therapeutic Care Pathways. Methodology for Calculating Indicators, 23 July 2018 Directorate General for Health Programming, Italian Ministry of Health 23 July 2018. Available online: https://www.salute.gov.it/imgs/C_17_pagineAree_5238_3_file.pdf (accessed on 15 July 2023).
- Motta, V. Estimating Poisson pseudo-maximum-likelihood rather than log-linear model of a log-transformed dependent variable. RAUSP Manag. J. 2019, 54, 508–518. [Google Scholar] [CrossRef]
- Tolles, J.; Meurer, W.J. Logistic Regression: Relating Patient Characteristics to Outcomes. JAMA 2016, 316, 533–534. [Google Scholar] [CrossRef] [PubMed]
- Zwinderman, A.H.; Glas, A.S.; Bossuyt, P.M.; Florie, J.; Bipat, S.; Stoker, J. Statistical models for quantifying diagnostic accuracy with multiple lesions per patient. Biostatistics 2008, 9, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Santos Silva, J.M.C.; Tenreyro, S. The Log of Gravity. Rev. Econ. Stat. 2006, 88, 641–658. [Google Scholar] [CrossRef]
- Heneghan, C. EBM Guidelines: Evidence-Based Medicine. BMJ Evid. Based Med. 2004, 9, 61. [Google Scholar] [CrossRef][Green Version]
- Masic, I.; Miokovic, M.; Muhamedagic, B. Evidence based medicine—New approaches and challenges. Acta Inform. Med. 2008, 16, 219–225. [Google Scholar] [CrossRef]
- Campbell, H.H.R.; Bradshaw, N.; Porteous, M. Integrated care pathways. Br. Med. J. 1998, 316, 133–144. [Google Scholar] [CrossRef]
- Rotter, T.; de Jong, R.B.; Lacko, S.E.; Ronellenfitsch, U.; Kinsman, L. Clinical pathways as a quality strategy. In Improving Healthcare Quality in Europe: Characteristics, Effectiveness and Implementation of Different Strategies [Internet]; Busse, R., Klazinga, N., Panteli, D., Quentin, W., World Health Organization, Eds.; European Observatory on Health Systems and Policies: Copenhagen, Denmark, 2019; (Health Policy Series, No. 53.) 12. Available online: https://www.ncbi.nlm.nih.gov/books/NBK549262/ (accessed on 12 July 2023).
- Hughes, R.G. Tools and Strategies for Quality Improvement and Patient Safety. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Hughes, R.G., Ed.; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2008; Chapter 44. Available online: https://www.ncbi.nlm.nih.gov/books/NBK2682/ (accessed on 10 August 2023).
- Asadi, M.J.; Baltz, W.A. Activity-based costing for clinical paths. An example to improve clinical cost & efficiency. J. Soc. Health Syst. 1996, 5, 1–7. [Google Scholar]
- Dubron, K.; Verschaeve, M.; Roodhooft, F. A time-driven activity-based costing approach for identifying variability in costs of childbirth between and within types of delivery. BMC Pregnancy Childbirth 2021, 21, 705. [Google Scholar] [CrossRef]
- Braun, R.; Schlieter, H.; Burwitz, M.; Esswein, W. BPMN4CP: Design and implementation of a BPMN extension for clinical pathways. In Proceedings of the 2014 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Belfast, UK, 2–5 November 2014; pp. 9–16. [Google Scholar] [CrossRef]
- Kassim, S.A.; Gartner, J.B.; Labbé, L.; Landa, P.; Paquet, C.; Bergeron, F.; Lemaire, C.; Côté, A. Benefits and limitations of business process model notation in modelling patient healthcare trajectory: A scoping review protocol. BMJ Open 2022, 12, e060357. [Google Scholar] [CrossRef] [PubMed]
- Pufahl, L.; Zerbato, F.; Weber, B.; Weber, I. BPMN in healthcare: Challenges and best practices. Inf. Syst. 2022, 107, 102013. [Google Scholar] [CrossRef]
- Shitkova, M.; Taratukhin, V.; Becker, J. Towards a methodology and a tool for modeling clinical pathways. Procedia Comput. Sci. 2015, 63, 205–212. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Motivation | Description of the Motivation for the Diagnosis |
|---|---|
| 1 | Gene pathology in the family |
| 2 | Chromosomal pathology in the family |
| 3 | Multifactorial/heterogeneous pathology in the family |
| 4 | Undefined or other pathology in the family |
| 5 | Fetal ultrasound pathology |
| 6 | Cytogenetic fetal pathology |
| 7 | Fetal screening |
| 8 | Maternal exposure to radiation |
| 9 | Maternal exposure to drugs |
| 10 | Maternal environmental exposure |
| 11 | Maternal infection exposure |
| 12 | Consanguinity |
| 13 | Maternal age (EMA)—Chorionic villi |
| 14 | Maternal age (EMA)—Amniotic fluid |
| 15 | Non-specific indication |
| Motivations Assigned to Patients | Number of Patients |
|---|---|
| One motivation | 1866 |
| Two motivations | 239 |
| Three motivations | 13 |
| Four motivations | 1 |
| Total | 2119 |
| Composition of Motivation Codes | Number of Patients |
|---|---|
| (Maternal age (EMA)—Chorionic villi OR Maternal age (EMA)—Amniotic fluid) AND Other = Other | 149 |
| (Maternal exposure to radiation OR Maternal exposure to drugs OR Maternal environmental exposure OR Maternal infection exposure) AND Other = Other | 12 |
| Non-specific indication AND Other = Other | 48 |
| Double motivation with the same code = Code | 1 |
| Total | 210 |
| Clinical Pathway | Motivation Codes | Number of Patients |
|---|---|---|
| A1 | Maternal age (EMA)—Chorionic villi | 491 |
| A2 | Maternal age (EMA)—Amniotic fluid | 775 |
| B1 | Gene pathology in the family OR Chromosomal pathology in the family | 370 |
| B2 | Chromosomal pathology in the family | 47 |
| B3 | Multifactorial/heterogeneous pathology in the family | 71 |
| B4 | Undefined or other pathology in the family | 9 |
| B5 | Fetal ultrasound pathology OR Cytogenetic fetal pathology OR Fetal screening | 194 |
| B6 | Maternal exposure to radiation OR Maternal exposure to drugs OR Maternal environmental exposure OR Maternal infection exposure | 115 |
| B7 | Non-specific indication | 4 |
| C1 | Gene pathology in the family AND Chromosomal pathology in the family | 5 |
| C2 | Gene pathology in the family AND Multifactorial/heterogeneous pathology in the family | 17 |
| C3 | Gene pathology in the family AND (Fetal ultrasound pathology OR Cytogenetic fetal pathology OR Fetal screening) | 8 |
| C4 | Chromosomal pathology in the family AND Multifactorial/heterogeneous pathology in the family | 1 |
| C5 | Multifactorial/heterogeneous pathology in the family AND (Fetal ultrasound pathology OR Cytogenetic fetal pathology OR Fetal screening) | 7 |
| C6 | Gene pathology in the family AND Chromosomal pathology in the family AND Multifactorial/heterogeneous pathology in the family | 4 |
| C7 | Gene pathology in the family AND Multifactorial/heterogeneous pathology in the family AND Fetal ultrasound pathology | 1 |
| Total | 2119 |
| Age | A1 | A2 | B1 | B2 | B3 | B4 | B5 | B6 | B7 | C1–C7 | Total | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | ||
| Bologna | 351 | 25 | 305 | 32 | 78 | 18 | 20 | 1 | 23 | 4 | 3 | 0 | 73 | 9 | 1 | 0 | 0 | 0 | 4 | 1 | 351 |
| Ferrara | 88 | 11 | 239 | 14 | 152 | 105 | 11 | 2 | 21 | 8 | 2 | 0 | 76 | 11 | 92 | 21 | 4 | 0 | 26 | 8 | 88 |
| Imola | 15 | 1 | 159 | 26 | 12 | 5 | 9 | 4 | 12 | 3 | 3 | 1 | 16 | 9 | 0 | 1 | 0 | 0 | 3 | 0 | 15 |
| Total | 454 | 37 | 703 | 72 | 242 | 128 | 40 | 7 | 56 | 15 | 8 | 1 | 165 | 29 | 93 | 22 | 4 | 0 | 34 | 9 | 2119 |
| % total | 21 | 2 | 33 | 3 | 11 | 6 | 2 | 0.5 | 3 | 1 | 0.5 | 0 | 8 | 1 | 4 | 1 | 0 | 0 | 2 | 1 | 100 |
| % path | 92 | 8 | 91 | 9 | 65 | 35 | 85 | 15 | 79 | 21 | 89 | 11 | 85 | 15 | 81 | 19 | 100 | 0 | 79 | 21 | |
| Age | A1 | A2 | B1 | B2 | B3 | B4 | B5 | B6 | B7 | C1–C7 | Total | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | ||
| 15–24 | 0 | 1 | 0 | 0 | 15 | 30 | 3 | 0 | 4 | 3 | 0 | 0 | 9 | 2 | 11 | 5 | 0 | 0 | 8 | 3 | 94 |
| 25–34 | 19 | 1 | 69 | 8 | 113 | 72 | 21 | 6 | 28 | 9 | 6 | 1 | 65 | 10 | 50 | 12 | 3 | 0 | 17 | 6 | 516 |
| >35 | 435 | 35 | 634 | 64 | 114 | 26 | 16 | 1 | 24 | 3 | 2 | 0 | 91 | 17 | 32 | 5 | 1 | 0 | 9 | 0 | 1509 |
| Total | 454 | 37 | 703 | 72 | 242 | 128 | 40 | 7 | 56 | 15 | 8 | 1 | 165 | 29 | 93 | 22 | 4 | 0 | 34 | 9 | 2119 |
| Anamnestic Data | A1 | A2 | B1 | B2 | B3 | B4 | B5 | B6 | B7 | C1–C7 | Total | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | ||
| Live birth | 44 | 8 | 41 | 30 | 24 | 38 | 8 | 3 | 13 | 4 | 3 | 1 | 34 | 25 | 4 | 1 | 1 | 0 | 17 | 3 | 302 |
| Stillborn | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 6 |
| Term birth | 21 | 6 | 19 | 10 | 11 | 9 | 4 | 1 | 4 | 2 | 0 | 0 | 19 | 15 | 0 | 0 | 0 | 0 | 3 | 1 | 125 |
| Preterm birth | 1 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3 |
| Miscarriage | 35 | 7 | 31 | 13 | 7 | 18 | 12 | 3 | 8 | 13 | 1 | 0 | 18 | 13 | 0 | 0 | 1 | 0 | 11 | 5 | 196 |
| VPI | 6 | 1 | 6 | 3 | 6 | 8 | 3 | 3 | 2 | 0 | 0 | 0 | 10 | 3 | 1 | 0 | 0 | 0 | 3 | 0 | 55 |
| Total | 108 | 22 | 98 | 58 | 48 | 73 | 27 | 10 | 27 | 20 | 5 | 1 | 81 | 56 | 5 | 1 | 2 | 0 | 35 | 10 | 687 |
| Genetic Test (with Fetus) | B1 | B2 | B3 | B4 | B5 | B6 | B7 | C1–C7 | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | ||
| Not inserted | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 |
| High resolution cytogenetic | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 4 | 2 | 6 |
| Molecular cytogenetic | 1 | 0 | 25 | 0 | 3 | 0 | 0 | 0 | 3 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 11 |
| Standard cytogenetic (karyotype) | 39 | 19 | 0 | 3 | 13 | 6 | 3 | 0 | 96 | 23 | 1 | 1 | 1 | 0 | 24 | 10 | 260 |
| Molecular CGH-Array | 1 | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 5 |
| Molecular direct | 325 | 273 | 0 | 0 | 26 | 2 | 1 | 29 | 6 | 0 | 0 | 0 | 0 | 55 | 17 | 728 | |
| Molecular indirect | 1 | 1 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 |
| Molecular UPD/Methylation | 0 | 0 | 0 | 3 | 0 | 0 | 0 | 9 | 2 | 0 | 0 | 0 | 0 | 3 | 0 | 21 | |
| Total | 368 | 295 | 34 | 3 | 45 | 8 | 4 | 0 | 143 | 32 | 1 | 1 | 1 | 0 | 87 | 29 | 1035 |
| Genetic Test (no Fetus) | B1 | B2 | B3 | B4 | B5 | B6 | B7 | C1–C7 | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | ||
| Not inserted | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 |
| High resolution cytogenetic | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 5 |
| Molecular cytogenetic | 0 | 0 | 1 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 5 |
| Standard cytogenetic (karyotype) | 1 | 0 | 13 | 3 | 9 | 4 | 3 | 0 | 23 | 12 | 0 | 0 | 0 | 0 | 9 | 6 | 83 |
| Molecular CGH-Array | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 |
| Molecular direct | 249 | 239 | 0 | 0 | 24 | 2 | 1 | 0 | 23 | 5 | 0 | 0 | 0 | 0 | 42 | 16 | 601 |
| Molecular indirect | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Molecular UPD/Methylation | 0 | 0 | 2 | 0 | 3 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 9 |
| Total | 252 | 242 | 17 | 3 | 39 | 6 | 4 | 0 | 50 | 17 | 0 | 0 | 0 | 0 | 54 | 24 | 708 |
| Outcome (with Fetus) | B1 | B2 | B3 | B4 | B5 | B6 | B7 | C1–C7 | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | ||
| Not inserted | 28 | 6 | 5 | 0 | 2 | 3 | 0 | 0 | 12 | 0 | 0 | 1 | 0 | 0 | 7 | 3 | 67 |
| Anomalous not defined | 5 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 10 |
| Anomalous pathological | 17 | 16 | 1 | 0 | 2 | 0 | 0 | 0 | 8 | 2 | 0 | 0 | 0 | 0 | 4 | 1 | 51 |
| Anomalous carrier | 153 | 145 | 6 | 0 | 2 | 0 | 0 | 0 | 13 | 6 | 0 | 0 | 0 | 0 | 16 | 1 | 342 |
| Normal | 165 | 127 | 22 | 3 | 39 | 5 | 4 | 0 | 108 | 23 | 1 | 0 | 1 | 0 | 44 | 23 | 565 |
| Total | 368 | 295 | 34 | 3 | 45 | 8 | 4 | 0 | 143 | 32 | 1 | 1 | 1 | 0 | 71 | 29 | 1035 |
| Outcome (no Fetus) | B1 | B2 | B3 | B4 | B5 | B6 | B7 | C1–C7 | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | F | I | F | I | F | I | F | I | F | I | F | I | F | I | F | ||
| Not inserted | 23 | 5 | 3 | 0 | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 6 | 2 | 43 |
| Anomalous not defined | 4 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 7 |
| Anomalous pathological | 5 | 6 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 13 |
| Anomalous carrier | 119 | 130 | 3 | 0 | 2 | 0 | 0 | 0 | 13 | 5 | 0 | 0 | 0 | 0 | 12 | 1 | 285 |
| Normal | 101 | 100 | 11 | 3 | 34 | 4 | 4 | 0 | 36 | 12 | 0 | 0 | 0 | 0 | 36 | 19 | 360 |
| Total | 252 | 242 | 17 | 3 | 39 | 6 | 4 | 0 | 50 | 17 | 0 | 0 | 0 | 0 | 54 | 24 | 708 |
| Mean | Median | St. Dev. | Min | Max | |
|---|---|---|---|---|---|
| Sample size = 2119 | |||||
| Weeks of pregnancy | 11.97 | 12 | 4.01 | 4 | 40 |
| Age | 35.45 | 36 | 4.92 | 15 | 48 |
| Sample size = 853—Not-EMA | |||||
| Weeks of pregnancy | 12.85 | 12 | 5.46 | 4 | 37 |
| Age | 32.38 | 33 | 5.81 | 16 | 48 |
| Sample size = 321—Foreign women | |||||
| Weeks of pregnancy | 13.99 | 13 | 5.35 | 4 | 40 |
| Age | 32.56 | 34 | 6.27 | 15 | 46 |
| Previous Pregnancies | Live Births (Quantity and %) | Spontaneous Abortions (Quantity and %) | VPI (Quantity and %) |
|---|---|---|---|
| 0 | 1209 | 1640 | 2046 |
| 0.570 | 0.773 | 0.965 | |
| 1 | 709 | 361 | 71 |
| 0.334 | 0.170 | 0.033 | |
| 2 | 166 | 93 | 2 |
| 0.078 | 0.043 | 0.000 | |
| 3 | 30 | 23 | - |
| 0.014 | 0.010 | - | |
| 4 | 5 | 2 | - |
| 0.002 | 0.000 | - | |
| 5 | - | 1 | - |
| - | 0.000 | - | |
| Total | 2119 | 2119 | 2119 |
| 1 | 1 | 1 |
| Referring Medical Doctor | Frequency | (%) |
|---|---|---|
| General practitioner | 559 | 26.38 |
| NHS specialist | 265 | 12.51 |
| Consultant specialist | 310 | 14.63 |
| Unidentified specialist | 94 | 4.44 |
| Hospital specialist | 432 | 20.39 |
| Private specialist | 140 | 6.61 |
| Other | 319 | 15.06 |
| Total | 2119 | 100 |
| Pathway Length (Days) | Mean | Median | St. Dev. | Min | Max |
|---|---|---|---|---|---|
| Sample size = 2119 | 6.77 | 0 | 16.03 | 0 | 259 |
| Sample size = 853—Not-EMA | 16.27 | 8 | 21.57 | 0 | 259 |
| Sample size = 321 Foreign women | 13.24 | 2 | 22.26 | 0 | 195 |
| Clinical Pathway | Frequency | (%) |
|---|---|---|
| A1 | 491 | 0.2317 |
| A2 | 775 | 0.3657 |
| B1 | 370 | 0.1746 |
| B2 | 47 | 0.0222 |
| B3 | 71 | 0.0335 |
| B4 | 9 | 0.0042 |
| B5 | 194 | 0.0916 |
| B6 | 115 | 0.0543 |
| B7 | 4 | 0.0019 |
| C1 | 5 | 0.0024 |
| C2 | 17 | 0.0080 |
| C3 | 8 | 0.0038 |
| C4 | 1 | 0.0005 |
| C5 | 7 | 0.0033 |
| C6 | 4 | 0.0019 |
| C7 | 1 | 0.0005 |
| Total | 2119 | 1 |
| Variables | (1) B1 | (2) B2 | (3) B3 | (4) B4 | (5) B5 | (6) B6 | (7) B7 | (8) C | (9) A |
|---|---|---|---|---|---|---|---|---|---|
| Weeks of pregnancy | 0.00245 (1.373) | −0.00233 *** (−2.979) | −0.00425 *** (−5.358) | −0.000678 ** (−2.221) | 0.0126 *** (9.328) | −0.00243 *** (−2.803) | 0.000538 (0.721) | −4.24 × 10−5 (−0.0693) | −0.0168 *** (−5.981) |
| Foreign | 0.235 *** (8.119) | 0.00267 (0.342) | 0.0219 * (1.840) | 0.000243 (0.0851) | −0.0410 *** (−5.404) | 0.00469 (1.148) | - - | 0.00648 (0.806) | −0.274 *** (−8.184) |
| Live births | −0.00879 (−0.796) | −0.00477 (−1.592) | −0.00378 (−0.888) | −0.000195 (−0.146) | −1.29 × 10−5 (−0.00241) | −0.0202 *** (−3.203) | −0.00634 (−0.665) | −0.00162 (−0.522) | 0.0769 *** (4.467) |
| Miscarriages | −0.0619 *** (−4.572) | 0.00494 (1.630) | 0.00735 (1.624) | −0.00181 (−0.876) | 0.00934 * (1.743) | - - | −0.00197 (−0.243) | 0.00281 (0.661) | 0.0613 *** (3.154) |
| VPI | 0.0549 * (1.814) | 0.0175 ** (2.550) | 0.00654 (0.569) | - - | 0.0495 *** (3.138) | −0.00719 (−1.010) | - - | 0.00740 (0.769) | −0.266 *** (−4.140) |
| General practitioner | −0.132 *** (−7.891) | −0.00275 (−0.369) | −0.0100 (−1.153) | −0.00134 (−0.446) | −0.0461 *** (−4.990) | −0.0119 ** (−2.118) | - - | −0.0194 *** (−3.661) | 0.298 *** (11.11) |
| Hospital specialist | −0.0188 (−0.914) | 0.00290 (0.317) | 0.00937 (0.798) | 0.00479 (0.749) | 0.0352 ** (2.355) | 0.0335 * (1.723) | - - | 0.00173 (0.264) | −0.133 *** (−3.744) |
| Private specialist | 0.0348 (1.011) | −0.00134 (−0.126) | 0.0149 (0.820) | 0.00218 (0.305) | 0.00730 (0.446) | 0.0867 * (1.670) | - - | −0.00414 (−0.523) | −0.236 *** (−4.636) |
| Consultant specialist | −0.0100 (−0.460) | −0.00935 (−1.343) | −0.00990 (−1.052) | - - | −0.0316 *** (−3.127) | 0.116 ** (2.090) | - - | −0.000813 (−0.123) | −0.0948 ** (−2.448) |
| NHS specialist | −0.0601 *** (−2.950) | 0.0261 (1.582) | 0.0107 (0.765) | 0.00417 (0.618) | −0.0219 ** (−2.142) | −0.00209 (−0.318) | - - | −0.0136 *** (−2.804) | 0.103 *** (2.826) |
| No. obs. | 2119 | 2119 | 2119 | 1745 | 2119 | 1639 | 350 | 2119 | 2119 |
| Variables | (1) PPML | (2) PPML | (3) PPML | (4) OLS | (5) OLS Reset | (6) OLS Bootstrap |
|---|---|---|---|---|---|---|
| Weeks of pregnancy | 0.0286 ** (2.118) | 0.0125 (0.998) | 0.0117 (0.955) | 0.219 * (1.716) | 0.0429 (0.337) | 0.219 * (1.753) |
| Foreign | 0.782 *** (6.373) | 0.446 *** (3.540) | 0.433 *** (3.469) | 6.529 *** (5.145) | 0.853 (0.278) | 6.529 *** (5.686) |
| Live births | - | −0.147 ** (−2.136) | −0.139 ** (−1.992) | −1.663 *** (−3.957) | −0.739 (−1.254) | −1.663 *** (−3.916) |
| Miscarriages | - | −0.0328 (−0.419) | −0.0136 (−0.175) | −0.668 (−1.482) | −0.288 (−0.586) | −0.668 (−1.492) |
| VPI | - | 0.440 ** (2.330) | 0.418 ** (2.219) | 4.647 * (1.855) | 0.0417 (0.0118) | 4.647 * (1.870) |
| General practitioner | - | - | −0.465 ** (−2.021) | −2.416 *** (−2.895) | −1.769 (−1.633) | −2.416 *** (−2.752) |
| Hospital specialist | - | - | 0.381 *** (2.664) | 3.082 *** (3.062) | 1.187 (0.736) | 3.082 *** (2.937) |
| Private specialist | - | - | 0.615 *** (3.418) | 6.190 *** (3.532) | 1.532 (0.447) | 6.190 *** (3.396) |
| Consultant specialist | - | - | 0.244 (1.550) | 2.958 ** (2.473) | 0.930 (0.575) | 2.958 ** (2.428) |
| NHS specialist | - | - | 0.530 *** (2.960) | 5.117 *** (3.124) | 1.515 (0.547) | 5.117 *** (3.069) |
| Squares of estimated values | - | - | - | - | 0.0371 (0.673) | - |
| Cubes of estimated values | - | - | - | - | 0.000438 (0.190) | - |
| Constant | 1.389 *** (8.265) | 2.411 *** (15.85) | 2.181 *** (11.73) | 2.958 * (1.838) | 3.787 ** (2.123) | 2.958 * (1.819) |
| No. obs. | 2119 | 2119 | 2119 | 2119 | 2119 | 2119 |
| R squared | 0.037 | 0.114 | 0.126 | 0.073 | 0.077 | 0.073 |
| Variables | (1) B1 | (2) B2 | (3) B3 | (4) B4 | (5) B5 | (6) B6 | (7) C | (8) A |
|---|---|---|---|---|---|---|---|---|
| Age | −0.00574 * (−1.718) | −0.00111 (−1.288) | −0.00212 * (−1.702) | −2.05 × 10−5 (−0.589) | 0.0120 *** (4.423) | 0.00237 * (1.673) | 0.000175 (0.175) | −0.00371 *** (−4.076) |
| Weeks of pregnancy | −0.00505 (−1.487) | −0.00428 *** (−3.594) | −0.00868 *** (−5.902) | −0.000155 *** (−3.143) | 0.0282 *** (8.317) | −0.0112 *** (−4.007) | −0.000709 (−0.410) | −0.000872 (−0.743) |
| Foreign | 0.249 *** (5.643) | −0.0133 (−1.040) | 0.00325 (0.170) | −0.000294 (−0.464) | −0.159 *** (−5.931) | −0.00713 (−0.370) | - | −0.0148 (−1.138) |
| Live births | 0.0567 ** (2.245) | −0.00201 (−0.328) | 0.00593 (0.624) | 0.000179 (0.464) | −0.00395 (−0.231) | −0.111 *** (−4.823) | −0.0191 (−0.508) | 0.0121 (1.563) |
| Miscarriages | −0.110 *** (−3.421) | 0.0173 *** (2.855) | 0.0288 *** (2.746) | −0.0003 (−0.523) | 0.0493 ** (2.045) | - | −0.00188 (−0.0555) | 0.0163 * (1.702) |
| VPI | −0.0271 (−0.428) | 0.0200 (1.461) | −0.0141 (−0.528) | - | 0.0840 ** (2.031) | −0.0664 (−1.498) | - | −6.02 × 10−5 (−0.00238) |
| General practitioner | 0.0302 (0.404) | 0.0409 (1.140) | 0.0610 (1.295) | 0.994 *** (166.0) | −0.0756 ** (−2.369) | −0.0454 * (−1.736) | - | 0.0200 (0.456) |
| Hospital specialist | −0.0980 * (−1.763) | −0.00939 (−0.604) | −0.00158 (−0.0647) | 0.877 *** (13.96) | 0.00502 (0.137) | 0.0936 * (1.764) | - | 0.0354 (1.055) |
| Private specialist | −0.0373 (−0.527) | −0.0171 (−1.172) | −0.000514 (−0.0174) | 0.991 *** (87.09) | −0.0750 ** (−2.389) | 0.201 * (1.885) | - | 0.0126 (0.331) |
| Consultant specialist | −0.0677 (−1.108) | −0.0286 ** (−2.197) | −0.0382 * (−1.859) | −0.123 *** (−3.902) | 0.354 *** (3.174) | 0.0281 (0.784) | ||
| NHS specialist | −0.0102 (−0.141) | 0.0716 (1.563) | 0.0497 (1.131) | 0.996 *** (343.5) | −0.0885 *** (−3.012) | −0.0234 (−0.688) | −0.00207 (−0.0646) | |
| No. obs. | 853 | 853 | 853 | 641 | 853 | 646 | 93 | 853 |
| Variables | (1) PPML | (2) PPML | (3) PPML | (4) OLS | (5) OLS reset | (6) OLS Bootstrap |
|---|---|---|---|---|---|---|
| Age | −0.0153 * (−1.942) | −0.0104 (−0.985) | −0.0119 (−1.098) | −0.226 * (−1.704) | 4.086 * (1.713) | −0.226 * (−1.696) |
| Weeks of pregnancy | −0.00247 (−0.253) | −0.000820 (−0.0820) | 0.000752 (0.0756) | 0.0130 (0.0783) | −0.229 (−1.218) | 0.0130 (0.0811) |
| Foreign | 0.232 * (1.914) | 0.242 ** (2.039) | 0.261 ** (2.233) | 4.532 ** (2.128) | −82.27 * (−1.713) | 4.532 ** (2.194) |
| Live births | - | −0.0818 (−1.434) | −0.0819 (−1.390) | −1.279 (−1.433) | 22.66 * (1.714) | −1.279 (−1.413) |
| Miscarriages | - | 0.00873 (0.119) | 0.0107 (0.144) | 0.199 (0.162) | −3.477 (−1.413) | 0.199 (0.164) |
| VPI | - | 0.178 (1.040) | 0.162 (0.943) | 2.879 (0.824) | −51.48 * (−1.738) | 2.879 (0.817) |
| General practitioner | - | - | 0.138 (0.642) | 2.008 (0.619) | −35.47 * (−1.743) | 2.008 (0.621) |
| Hospital specialist | - | - | 0.130 (1.026) | 1.872 (1.008) | −32.99 * (−1.694) | 1.872 (1.022) |
| Private specialist | - | - | 0.276 * (1.708) | 4.316 (1.623) | −77.55 * (−1.696) | 4.316 (1.626) |
| Consultant specialist | - | - | 0.0861 (0.585) | 1.179 (0.526) | −20.61 * (−1.656) | 1.179 (0.532) |
| NHS specialist | - | - | 0.301 (1.399) | 4.797 (1.281) | −85.85 * (−1.751) | 4.797 (1.279) |
| Squares of estimated values | - | - | - | - | 1.138 * (1.750) | - |
| Cubes of estimated values | - | - | - | - | −0.0220 * (−1.687) | - |
| Constant | 3.248 *** (12.54) | 3.105 *** (9.502) | 2.973 *** (8.572) | 20.46 *** (4.320) | −267.1 * (−1.657) | 20.46 *** (4.181) |
| No. obs. | 853 | 853 | 853 | 853 | 853 | 853 |
| R squared | 0.013 | 0.017 | 0.021 | 0.021 | 0.025 | 0.021 |
| Variables | (1) B1 | (2) B2 | (3) B3 | (4) B4 | (5) B5 | (6) B6 | (7) C | (8) DA |
|---|---|---|---|---|---|---|---|---|
| Weeks of pregnancy | 0.0196 *** (2.901) | −0.00242 (−0.882) | −0.00594 *** (−2.617) | −0.00834 (−0.988) | 0.00578 *** (2.804) | −0.00602 * (−1.654) | −0.00101 (−0.402) | −0.0315 *** (−5.393) |
| Live births | 0.0821 ** (2.185) | −0.0193 (−1.422) | −0.00525 (−1.025) | 0.00727 (0.663) | 0.00466 (0.509) | −0.0558 ** (−2.041) | −0.0137 (−1.236) | 0.0321 (0.997) |
| Miscarriages | −0.0601 (−1.225) | −0.00437 (−0.337) | 0.0136 * (1.878) | - | 0.0139 (1.259) | - | 0.00878 (0.644) | 0.00905 (0.254) |
| VPI | 0.149 (1.459) | 0.0644 * (1.911) | - | - | 0.00869 (0.389) | - | - | −0.143 (−0.975) |
| General practitioner | −0.181 * (−1.901) | 0.0195 (0.486) | - | - | −0.0386 * (−1.649) | - | −0.0196 (−0.713) | 0.412 *** (4.085) |
| Hospital specialist | −0.110 (−1.182) | - | 0.0370 (1.208) | - | 0.0327 (0.890) | 0.0342 (0.604) | 0.00298 (0.0966) | −0.0371 (−0.439) |
| Private specialist | 0.110 (0.636) | 0.0109 (0.174) | - | - | 0.0252 (0.343) | 0.0575 (0.531) | - | −0.175 * (−1.744) |
| Consultant specialist | 0.00887 (0.0910) | - | −0.0133 (−0.891) | - | −0.0696 *** (−2.953) | 0.0936 (1.055) | 0.00859 (0.284) | −0.125 (−1.554) |
| NHS specialist | −0.211 ** (−2.317) | 0.0378 (0.761) | 0.00196 (0.0956) | - | −0.00798 (−0.272) | −0.00387 (−0.127) | - | 0.264 ** (2.214) |
| No. obs. | 321 | 153 | 242 | 26 | 321 | 191 | 257 | 321 |
| Variables | (1) PPML | (2) PPML | (3) PPML | (4) OLS | (5) OLS Reset | (6) OLS Bootstrap |
|---|---|---|---|---|---|---|
| Weeks of pregnancy | 0.0411 *** (2.901) | 0.0428 *** (2.887) | 0.0344 ** (2.337) | 0.561 ** (2.171) | 0.902 (0.698) | 0.561 ** (2.268) |
| Live births | - | −0.135 (−1.591) | −0.0924 (−1.061) | −1.304 (−1.238) | −2.009 (−0.679) | −1.304 (−1.229) |
| Miscarriages | - | −0.0965 (−0.753) | −0.0279 (−0.230) | −0.716 (−0.490) | −1.209 (−0.451) | −0.716 (−0.481) |
| VPI | - | 0.504 ** (2.022) | 0.469 * (1.749) | 9.046 (1.266) | 14.97 (0.535) | 9.046 (1.027) |
| General practitioner | - | - | −0.833 (−1.333) | −8.004 * (−1.894) | −11.59 (−0.861) | −8.004 * (−1.823) |
| Hospital specialist | - | - | −0.193 (−0.845) | −3.104 (−0.963) | −4.983 (−0.583) | −3.104 (−0.970) |
| Private specialist | - | - | 0.391 (1.272) | 6.891 (1.118) | 11.44 (0.630) | 6.891 (1.082) |
| Consultant specialist | - | - | 0.161 (0.718) | 2.848 (0.746) | 4.707 (0.557) | 2.848 (0.779) |
| NHS specialist | - | - | −0.927 *** (−2.811) | −9.294 *** (−3.013) | −13.49 (−0.733) | −9.294 *** (−3.112) |
| Squares of estimated values | - | - | - | - | −0.0266 (−0.222) | - |
| Cubes of estimated values | - | - | - | - | 0.000287 (0.162) | - |
| Constant | 1.982 *** (7.598) | 2.021 *** (7.823) | 2.251 *** (7.701) | 8.055 * (1.840) | 9.028 (1.141) | 8.055 * (1.951) |
| No. obs. | 321 | 321 | 321 | 321 | 321 | 321 |
| R squared | 0.025 | 0.043 | 0.081 | 0.088 | 0.089 | 0.088 |
| Clinical Pathway | Full Sample | Not-EMA Sample | Foreign Women Sample |
|---|---|---|---|
| Weeks of pregnancy | 0.0789 (0.608) | 0.138 (0.736) | 0.116 (0.421) |
| Foreign | 1.013 (0.886) | 1.547 (0.778) | - |
| Live births | −1.175 *** (−3.385) | −2.783 *** (−3.314) | −1.439 (−1.529) |
| Miscarriages | 0.0936 (0.226) | 0.0697 (0.0564) | - |
| Voluntary pregnancy interruptions | 1.586 (0.703) | 2.836 (0.846) | −0.977 (−0.571) |
| General practitioner | 0.702 (0.946) | 0.0644 (0.0202) | 7.091 (1.135) |
| Hospital specialist | 1.270 (1.605) | 3.271 ** (2.042) | −0.945 (−0.208) |
| Private specialist | 3.267 ** (2.304) | 6.046 ** (2.537) | −2.667 (−0.974) |
| Consultant specialist | 2.203 ** (2.104) | 4.285 ** (2.005) | 6.244 (1.424) |
| NHS specialist | 1.202 (0.973) | 3.774 (1.061) | 1.813 (0.462) |
| DB1 | 20.63 *** (11.99) | 19.04 *** (8.357) | −3.199 (−1.400) |
| DB2 | 11.25 *** (3.855) | 9.807 *** (2.626) | 21.98 ** (2.373) |
| DB3 | 16.41 *** (4.425) | 15.06 *** (3.613) | 7.120 (0.582) |
| DB4 | 15.95 *** (2.615) | 14.36 ** (2.190) | 19.55 * (1.651) |
| DB5 | 6.135 ** (2.524) | 4.507 (1.316) | 15.91 * (1.853) |
| DB6 | 1.383 (0.962) | −1.319 (−0.583) | 6.205 (0.552) |
| DB7 | 0.765 (0.342) | 0.423 (0.142) | −0.533 (−0.0548) |
| Maternal age | −0.961 (−0.596) | - | −0.869 (−0.0758) |
| Constant | 27.64 *** (7.938) | 26.18 *** (6.859) | 29.33 *** (2.884) |
| Number of observations | 2119 | 853 | 321 |
| R Squared | 0.442 | 0.461 | 0.474 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alderighi, S.; Landa, P.; Tànfani, E.; Testi, A. Assessing the Impact of Patient Characteristics on Genetic Clinical Pathways: A Regression Approach. Algorithms 2024, 17, 75. https://doi.org/10.3390/a17020075
Alderighi S, Landa P, Tànfani E, Testi A. Assessing the Impact of Patient Characteristics on Genetic Clinical Pathways: A Regression Approach. Algorithms. 2024; 17(2):75. https://doi.org/10.3390/a17020075
Chicago/Turabian StyleAlderighi, Stefano, Paolo Landa, Elena Tànfani, and Angela Testi. 2024. "Assessing the Impact of Patient Characteristics on Genetic Clinical Pathways: A Regression Approach" Algorithms 17, no. 2: 75. https://doi.org/10.3390/a17020075
APA StyleAlderighi, S., Landa, P., Tànfani, E., & Testi, A. (2024). Assessing the Impact of Patient Characteristics on Genetic Clinical Pathways: A Regression Approach. Algorithms, 17(2), 75. https://doi.org/10.3390/a17020075