

Using Explainable AI (XAI) for the Prediction of Falls in the Older Population


Abstract
1. Introduction
2. Materials and Methods
2.1. Dataset
2.2. Input Features
2.3. Future Falls
2.4. Random Forests and Feature Relevance
2.5. Classification Performance Measures
2.6. Workflow Summary
- Extraction of data from the TILDA database.
- Data processing and cleaning (removing data with missing values, removing duplicate data, and encoding binary variables).
- Building random forest prediction models (all falls and syncope model; simple falls model; complex falls model; syncope model).
- Python 3 programming language was used on the Anaconda platform.
- GridSearchCV package was implemented for tuning of hyperparameters.
- Assessing the model’s performance by calculating the precision, recall and F1 scores.
- Feature relevance: SHAP and random forest feature importances were derived from the four models.
2.7. Detailed Code
- All falls and syncope: https://www.kaggle.com/code/tang1628/3rffallssyncope-rebalance (accessed on 20 August 2022).
- Simple falls: https://www.kaggle.com/code/tang1628/3rfsimplefallspred-rebalance (accessed on 20 August 2022).
- Complex falls: https://www.kaggle.com/code/tang1628/3rfcomplexfalls-rebalance (accessed on 20 August 2022).
- Syncope: https://www.kaggle.com/code/tang1628/3rfsyncope-rebalance (accessed on 20 August 2022).
3. Results
3.1. Dataset
3.2. Prediction Performance
3.3. Feature Importance
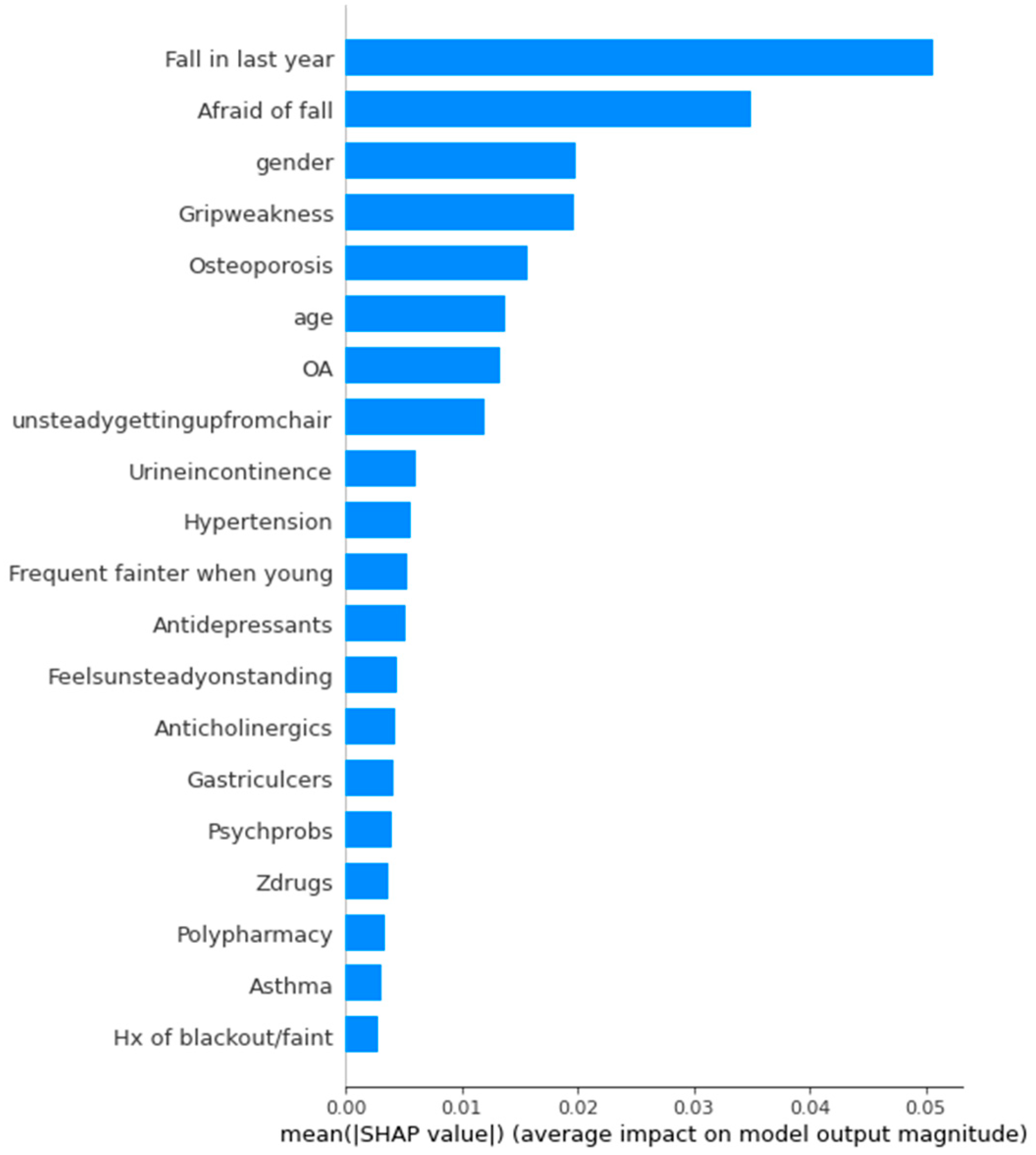
3.4. SHAP Values
4. Discussion
4.1. Accuracy of Prediction
4.2. All Falls and Syncope
4.3. Simple Falls
4.4. Complex Falls
4.5. Syncope
4.6. Limitations
4.6.1. Self-Report Limitation
4.6.2. Low Granularity in Certain Features
4.6.3. Other Dataset Limitations
4.6.4. Technical Limitations and Alternative Algorithms
4.6.5. Alternative Algorithms and Explainability Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stel, V.S.; Smit, J.H.; Pluijm, S.M.; Lips, P. Consequences of falling in older men and women and risk factors for health service use and functional decline. Age Ageing 2004, 33, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Gannon, B.; O’Shea, E.; Hudson, E. The Economic Cost of Falls and Fractures in People aged 65 and over in Ireland: Technical Report to NCAOP/HSE/DOHC. 2007. Available online: https://www.hse.ie/eng/services/publications/olderpeople/the-economic-costs-of-falls-and-fractures-in-people-aged-65-and-over-in-ireland.pdf (accessed on 24 September 2022).
- HSE; NCAOP; DOHC. Strategy to Prevent Falls and Fractures in Ireland’s Ageing Population: Report of the National Steering Group on the Prevention of Falls in Older People and the Prevention and Management of Osteoporosis throughout Life. 2008. Available online: https://www.hse.ie/eng/services/publications/olderpeople/strategy-to-prevent-falls-and-fractures-in-irelands-ageing-population---full-report.pdf (accessed on 24 September 2022).
- NICE. Falls in Older People: Assessing Risk and Prevention: Clinical Guideline [CG161]. 2013. Available online: https://www.nice.org.uk/guidance/cg161 (accessed on 24 September 2022).
- Tan, M.P.; Kenny, R.A. Cardiovascular assessment of falls in older people. Clin. Interv. Aging 2006, 1, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, N.; Romero-Ortuno, R. The Syncope-Falls Index: A tool for predicting risk of syncope and complex falls in the older adult based on cumulative health deficits. QJM 2022, 115, 367–373. [Google Scholar] [CrossRef]
- Usmani, S.; Saboor, A.; Haris, M.; Khan, M.A.; Park, H. Latest Research Trends in Fall Detection and Prevention Using Machine Learning: A Systematic Review. Sensors 2021, 21, 5134. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.R.C.; Knight, S.P.; Donoghue, O.A.; Hernández, B.; Rizzo, R.; Kenny, R.A.; Romero-Ortuno, R. Comparison of Gait Speed Reserve, Usual Gait Speed, and Maximum Gait Speed of Adults Aged 50+ in Ireland Using Explainable Machine Learning. Front. Netw. Physiol. 2021, 1. [Google Scholar] [CrossRef]
- Kumar, S.; Du, C.; Graham, S.; Nguyen, T. Using Machine Learning to Predict Frailty from Cognitive Assessments. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 2021, 1648–1652. [Google Scholar]
- Moguilner, S.; Knight, S.P.; Davis, J.R.C.; O’Halloran, A.M.; Kenny, R.A.; Romero-Ortuno, R. The Importance of Age in the Prediction of Mortality by a Frailty Index: A Machine Learning Approach in the Irish Longitudinal Study on Ageing. Geriatrics 2021, 6, 84. [Google Scholar] [CrossRef]
- Nowak, A.; Hubbard, R.E. Falls and frailty: Lessons from complex systems. J. R. Soc. Med. 2009, 102, 98–102. [Google Scholar] [CrossRef]
- Arrieta, A.B.; Díaz-Rodríguez, N.; Ser, J.D.; Bennetot, A.; Tabik, S.; Barbado, A.; Garcia, S.; Gil-Lopez, S.; Molina, D.; Benjamins, R.; et al. Explainable Artificial Intelligence (XAI): Concepts, taxonomies, opportunities and challenges toward responsible AI. Inf. Fusion 2020, 58, 82–115. [Google Scholar] [CrossRef]
- Loyola-González, O. Black-Box vs. White-Box: Understanding Their Advantages and Weaknesses From a Practical Point of View. IEEE Access 2019, 7, 154096–154113. [Google Scholar] [CrossRef]
- Adadi, A.; Berrada, M. Peeking Inside the Black-Box: A Survey on Explainable Artificial Intelligence (XAI). IEEE Access 2018, 6, 52138–52160. [Google Scholar] [CrossRef]
- Pawar, U.; O’Shea, D.; Rea, S.; O’Reilly, R. Incorporating explainable artificial intelligence (XAI) to aid the understanding of machine learning in the healthcare domain. In Proceedings of the 8th Irish Conference on Artificial Intelligence and Cognitive Science 2020, Dublin, Ireland, 7–8 December 2020; pp. 1–12. [Google Scholar]
- Chico, V. The impact of the General Data Protection Regulation on health research. Br. Med. Bull. 2018, 128, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Kearney, P.M.; Cronin, H.; O’Regan, C.; Kamiya, Y.; Savva, G.M.; Whelan, B.; Kenny, R. Cohort profile: The Irish Longitudinal Study on Ageing. Int. J. Epidemiol. 2011, 40, 877–884. [Google Scholar] [CrossRef]
- Brignole, M.; Moya, A.; de Lange, F.J.; Deharo, J.-C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martín, A.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.Z.; Rahman, M.S.; Rahman, M.S. A Random Forest based predictor for medical data classification using feature ranking. Inform. Med. Unlocked 2019, 15, 100180. [Google Scholar] [CrossRef]
- Saenz-Cogollo, J.F.; Agelli, M. Investigating Feature Selection and Random Forests for Inter-Patient Heartbeat Classification. Algorithms 2020, 13, 75. [Google Scholar] [CrossRef]
- Louppe, G.; Wehenkel, L.; Sutera, A.; Geurts, P. Understanding variable importances in forests of randomized trees. In Proceedings of the 26th International Conference on Neural Information Processing Systems—Volume 1, Lake Tahoe, NV, USA, 5–10 December 2013; Curran Associates Inc.: Lake Tahoe, NV, USA, 2013; pp. 431–439. [Google Scholar]
- Podgorelec, V.; Kokol, P.; Stiglic, B.; Rozman, I. Decision Trees: An Overview and Their Use in Medicine. J. Med. Syst. 2002, 26, 445–463. [Google Scholar] [CrossRef]
- Lundberg, S.M.; Lee, S.-I. A unified approach to interpreting model predictions. In Proceedings of the 31st International Conference on Neural Information Processing Systems, Long Beach, CA, USA, 4–9 December 2017; Curran Associates Inc.: Long Beach, CA, USA, 2017; pp. 4768–4777. [Google Scholar]
- Bhuiya, M.M.R.; Hasan, M.M.U.; Keellings, D.J.; Mohiuddin, H. Application of Machine Learning Classifiers for Mode Choice Modeling for Movement-Challenged Persons. Future Transp. 2022, 2, 328–346. [Google Scholar] [CrossRef]
- Donoghue, O.A.; Hernandez, B.; O’Connell, M.D.L.; Kenny, R.A. Using conditional inference forests to examine predictive ability for future falls and syncope in older adults: Results from The Irish Longitudinal Study on Ageing. J. Gerontol. Ser. A 2022, glac156. [Google Scholar] [CrossRef]
- Gade, G.V.; Jorgensen, M.G.; Ryg, J.; Riis, J.; Thomsen, K.; Masud, T.; Andersen, S. Predicting falls in community-dwelling older adults: A systematic review of prognostic models. BMJ Open 2021, 11, e044170. [Google Scholar] [CrossRef]
- Lindberg, D.S.; Prosperi, M.; Bjarnadottir, R.I.; Thomas, J.; Crane, M.; Chen, Z.; Shear, K.; Solberg, L.M.; Snigurska, U.A.; Wu, Y.; et al. Identification of important factors in an inpatient fall risk prediction model to improve the quality of care using EHR and electronic administrative data: A machine-learning approach. Int. J. Med. Inform. 2020, 143, 104272. [Google Scholar] [CrossRef]
- Fuller, G.F. Falls in the elderly. Am. Fam. Physician 2000, 61, 2159–2168. [Google Scholar]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef]
- Chang, V.C.; Do, M.T. Risk factors for falls among seniors: Implications of gender. Am. J. Epidemiol. 2015, 181, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.; Tham, Y.C.; Chee, M.L.; Tan, N.Y.Q.; Wong, K.H.; Majithia, S.; Sabanayagam, C.; Lamoureux, E.; Wong, T.Y.; Cheng, C.Y. Falls and Recurrent Falls among Adults in A Multi-ethnic Asian Population: The Singapore Epidemiology of Eye Diseases Study. Sci. Rep. 2018, 8, 7575. [Google Scholar] [CrossRef] [PubMed]
- Treves, N.; Perlman, A.; Kolenberg Geron, L.; Asaly, A.; Matok, I. Z-drugs and risk for falls and fractures in older adults—A systematic review and meta-analysis. Age Ageing 2018, 47, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Young, W.R.; Mark Williams, A. How fear of falling can increase fall-risk in older adults: Applying psychological theory to practical observations. Gait Posture 2015, 41, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Yeung, S.S.Y.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef]
- Gold, T.; Williams, S.A.; Weiss, R.J.; Wang, Y.; Watkins, C.; Carroll, J.; Middleton, C.; Silverman, S. Impact of fractures on quality of life in patients with osteoporosis: A US cross-sectional survey. J. Drug Assess. 2019, 8, 175–183. [Google Scholar] [CrossRef]
- Borgstrom, F.; Karlsson, L.; Ortsater, G.; Norton, N.; Halbout, P.; Cooper, C.; Lorentzon, M.; McCloskey, E.V.; Harvey, N.C.; Javaid, M.K.; et al. International Osteoporosis, F. Fragility fractures in Europe: Burden, management and opportunities. Arch. Osteoporos. 2020, 15, 59. [Google Scholar] [CrossRef]
- Rivasi, G.; Rafanelli, M.; Mossello, E.; Brignole, M.; Ungar, A. Drug-Related Orthostatic Hypotension: Beyond Anti-Hypertensive Medications. Drugs Aging 2020, 37, 725–738. [Google Scholar] [CrossRef] [PubMed]
- de Jong, M.R.; Van der Elst, M.; Hartholt, K.A. Drug-related falls in older patients: Implicated drugs, consequences, and possible prevention strategies. Ther Adv Drug Saf 2013, 4, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Sink, K.M.; Evans, G.W.; Shorr, R.I.; Bates, J.T.; Berlowitz, D.; Conroy, M.B.; Felton, D.M.; Gure, T.; Johnson, K.C.; Kitzman, D.; et al. Syncope, Hypotension, and Falls in the Treatment of Hypertension: Results from the Randomized Clinical Systolic Blood Pressure Intervention Trial. J. Am. Geriatr. Soc. 2018, 66, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Sexton, D.J.; Canney, M.; O’Connell, M.D.L.; Moore, P.; Little, M.A.; O’Seaghdha, C.M.; Kenny, R.A. Injurious Falls and Syncope in Older Community-Dwelling Adults Meeting Inclusion Criteria for SPRINT. JAMA Intern. Med. 2017, 177, 1385–1387. [Google Scholar] [CrossRef]
- O’Donoghue, P.; O’Halloran, A.; Kenny, R.; Romero-Ortuno, R. Older adults identified as frail by Frailty Index and FRAIL scale who were intensively treated for hypertension were at increased risk of 2-year adverse health outcomes in The Irish Longitudinal Study on Ageing (TILDA) [version 2; peer review: 1 approved with reservations, 1 not approved]. HRB Open Research 2022, 5, 45. [Google Scholar]
- Mcintosh, S.; Costa, D.D.; Kenny, R.A. Outcome of an Integrated Approach to the Investigation of Dizziness, Falls and Syncope, in Elderly Patients Referred to a ‘Syncope’ Clinic. Age Ageing 1993, 22, 53–58. [Google Scholar] [CrossRef]
- Freiberger, E.; de Vreede, P. Falls recall—Limitations of the most used inclusion criteria. Eur. Rev. Aging Phys. Act. 2011, 8, 105–108. [Google Scholar] [CrossRef]
- Delbaere, K.; Close, J.C.; Kochan, N.A.; Sachdev, P.S.; Lord, S.R. Good memory as a predictor of falls: Fact or artefact. Age Ageing 2012, 41, 404–408. [Google Scholar] [CrossRef]
- O’Dwyer, C.; Bennett, K.; Langan, Y.; Fan, C.W.; Kenny, R.A. Amnesia for loss of consciousness is common in vasovagal syncope. Europace 2011, 13, 1040–1045. [Google Scholar] [CrossRef]
- Hsiao, W.-C.; Shih, Y.-S. Splitting variable selection for multivariate regression trees. Stat. Probab. Lett. 2007, 77, 265–271. [Google Scholar] [CrossRef]
- Dey, A. Machine Learning Algorithms: A Review. Int. J. Comput. Sci. Inf. Technol. 2016, 7, 1174–1179. [Google Scholar]
- Price, W.N. Big data and black-box medical algorithms. Sci. Transl. Med. 2018, 10, 471. [Google Scholar] [CrossRef] [PubMed]
- Mazurowski, M.A.; Habas, P.A.; Zurada, J.M.; Lo, J.Y.; Baker, J.A.; Tourassi, G.D. Training neural network classifiers for medical decision making: The effects of imbalanced datasets on classification performance. Neural Netw. 2008, 21, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Shaikhina, T.; Khovanova, N.A. Handling limited datasets with neural networks in medical applications: A small-data approach. Artif. Intell. Med. 2017, 75, 51–63. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | Type of Variable (Continuous, Binary) | Feature Value |
|---|---|---|
| Polypharmacy | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Continuous | 65–80 |
| Binary | 0 = Male, 1 = Female |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Binary | 0 = Absent, 1 = Present |
| Model | Number of Events in the Original Dataset | Number or Events in the Training Dataset after Rebalance |
|---|---|---|
| All Falls and Syncope | 0: 1549 1: 1351 | 0: 1098 1: 1070 |
| Simple Falls | 0: 2683 1: 217 | 0: 1888 1: 1868 |
| Complex Falls | 0: 1823 1: 1077 | 0: 1302 1: 1250 |
| Syncope | 0: 2715 1: 185 | 0: 1899 1: 1902 |
| Model (Class) | Precision | Recall | F1-Score |
|---|---|---|---|
| Falls and Syncope (0) | 0.58 | 0.65 | 0.61 |
| Falls and Syncope (1) | 0.63 | 0.56 | 0.59 |
| Simple Falls (0) | 0.90 | 0.63 | 0.75 |
| Simple Falls (1) | 0.72 | 0.93 | 0.82 |
| Complex Falls (0) | 0.57 | 0.69 | 0.62 |
| Complex Falls (1) | 0.65 | 0.52 | 0.58 |
| Syncope (0) | 0.81 | 0.88 | 0.84 |
| Syncope (1) | 0.87 | 0.79 | 0.83 |
| All Falls and Syncope Model | Feature Importance Coefficient |
|---|---|
| Fall in last year | 0.140 |
| Age | 0.108 |
| Afraid of fall | 0.070 |
| Sex | 0.060 |
| Osteoarthritis | 0.046 |
| Osteoporosis | 0.040 |
| Hypertension | 0.036 |
| Urine incontinence | 0.031 |
| Frequent fainter when young | 0.030 |
| Polypharmacy | 0.029 |
| Grip weakness | 0.026 |
| History of blackout/faint | 0.025 |
| Abnormal heart rhythm | 0.024 |
| Antihypertensives | 0.024 |
| Unsteady getting up from chair | 0.022 |
| Z-drugs | 0.020 |
| Anticholinergics | 0.020 |
| Angina | 0.020 |
| Asthma | 0.019 |
| Antidepressants | 0.017 |
| Simple Falls Model | Feature Importance Coefficient |
|---|---|
| Age | 0.138 |
| Sex | 0.041 |
| Weight loss | 0.039 |
| Hypertension | 0.035 |
| Fall in last year | 0.034 |
| Myocardial infarction | 0.034 |
| Polypharmacy | 0.033 |
| Urine incontinence | 0.030 |
| Afraid of fall | 0.030 |
| Unsteady on standing | 0.028 |
| Unsteady getting up from chair | 0.027 |
| MMSE less than 24 | 0.027 |
| COPD | 0.027 |
| Asthma | 0.026 |
| Grip weakness | 0.026 |
| Frequent fainter when young | 0.025 |
| Osteoarthritis | 0.024 |
| Abnormal heart rhythm | 0.024 |
| Angina | 0.023 |
| History of blackout/faint | 0.021 |
| Complex Falls Top Features | Feature Importance |
|---|---|
| Fall in last year | 0.135 |
| Age | 0.110 |
| Afraid of fall | 0.081 |
| Osteoporosis | 0.045 |
| Sex | 0.042 |
| Grip weakness | 0.039 |
| Osteoarthritis | 0.034 |
| Unsteady getting up from chair | 0.034 |
| Urine incontinence | 0.028 |
| Frequent fainter when young | 0.028 |
| Hypertension | 0.023 |
| Polypharmacy | 0.023 |
| Feels unsteady on standing | 0.022 |
| Antidepressants | 0.021 |
| Antihypertensives | 0.020 |
| Anticholinergics | 0.019 |
| Psychiatric problems | 0.019 |
| Abnormal heart rhythm | 0.017 |
| History of blackout/faint | 0.016 |
| Diabetes | 0.016 |
| Syncope Model | Feature Importance |
|---|---|
| Age | 0.118 |
| Frequent fainter when young | 0.043 |
| Polypharmacy | 0.041 |
| Fall in last year | 0.040 |
| MI | 0.039 |
| Unsteady getting up from chair | 0.038 |
| Sex | 0.033 |
| Osteoporosis | 0.031 |
| Angina | 0.030 |
| Grip weakness | 0.029 |
| Abnormal heart rhythm | 0.029 |
| Antihypertensives | 0.029 |
| Varicose ulcers | 0.027 |
| Cancer | 0.027 |
| Osteoarthritis | 0.026 |
| Afraid of fall | 0.025 |
| Hypertension | 0.024 |
| Urine incontinence | 0.023 |
| Poor smell | 0.022 |
| History of blackout/faint | 0.021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, Y.T.; Romero-Ortuno, R. Using Explainable AI (XAI) for the Prediction of Falls in the Older Population. Algorithms 2022, 15, 353. https://doi.org/10.3390/a15100353
Tang YT, Romero-Ortuno R. Using Explainable AI (XAI) for the Prediction of Falls in the Older Population. Algorithms. 2022; 15(10):353. https://doi.org/10.3390/a15100353
Chicago/Turabian StyleTang, Yue Ting, and Roman Romero-Ortuno. 2022. "Using Explainable AI (XAI) for the Prediction of Falls in the Older Population" Algorithms 15, no. 10: 353. https://doi.org/10.3390/a15100353
APA StyleTang, Y. T., & Romero-Ortuno, R. (2022). Using Explainable AI (XAI) for the Prediction of Falls in the Older Population. Algorithms, 15(10), 353. https://doi.org/10.3390/a15100353