
Influence of Digital Manufacturing and Abutment Design on Full-Arch Implant Prostheses—An In Vitro Study


Abstract
1. Introduction
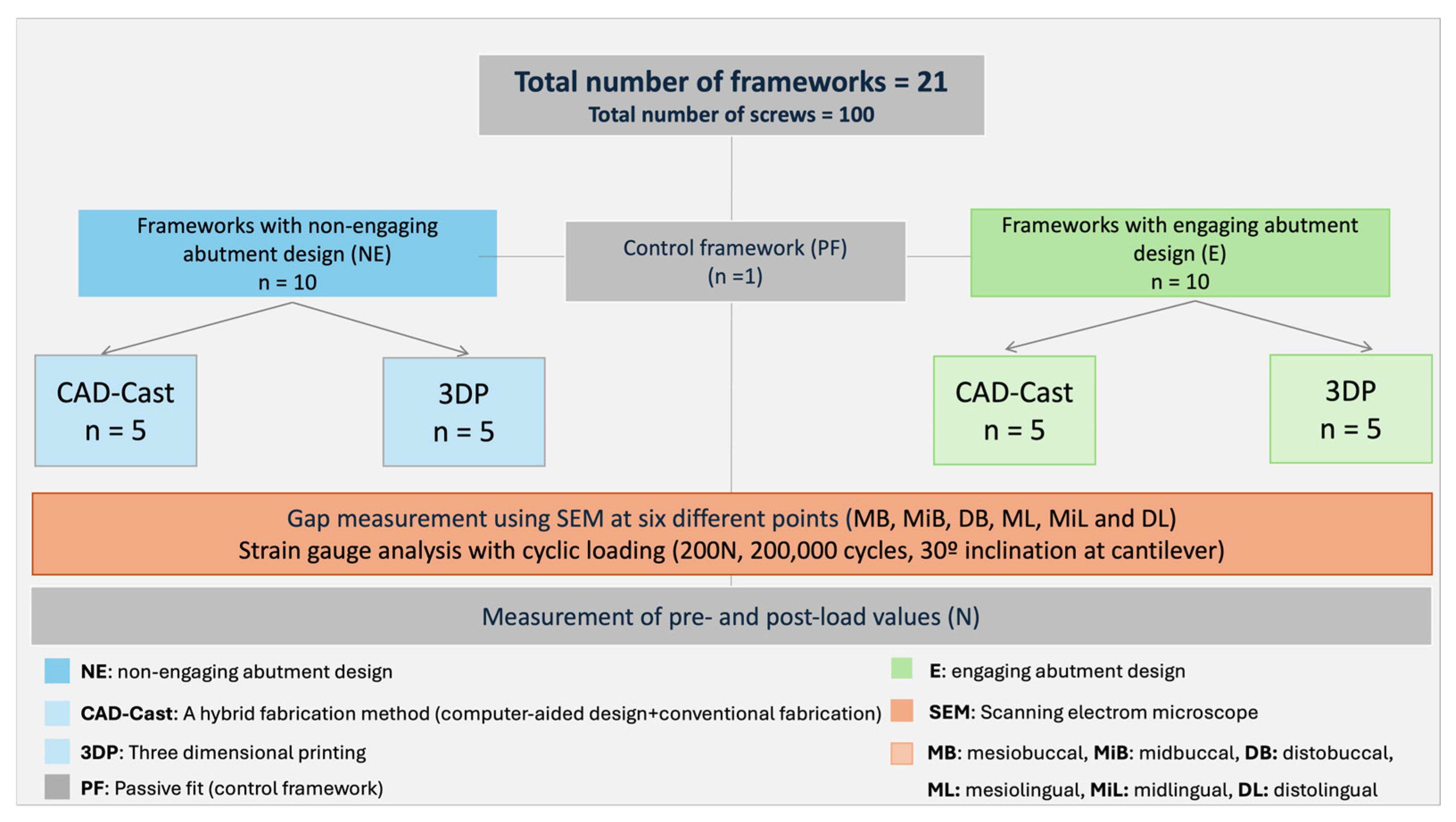
2. Materials and Methods
2.1. Control Framework Fabrication (PF Group)
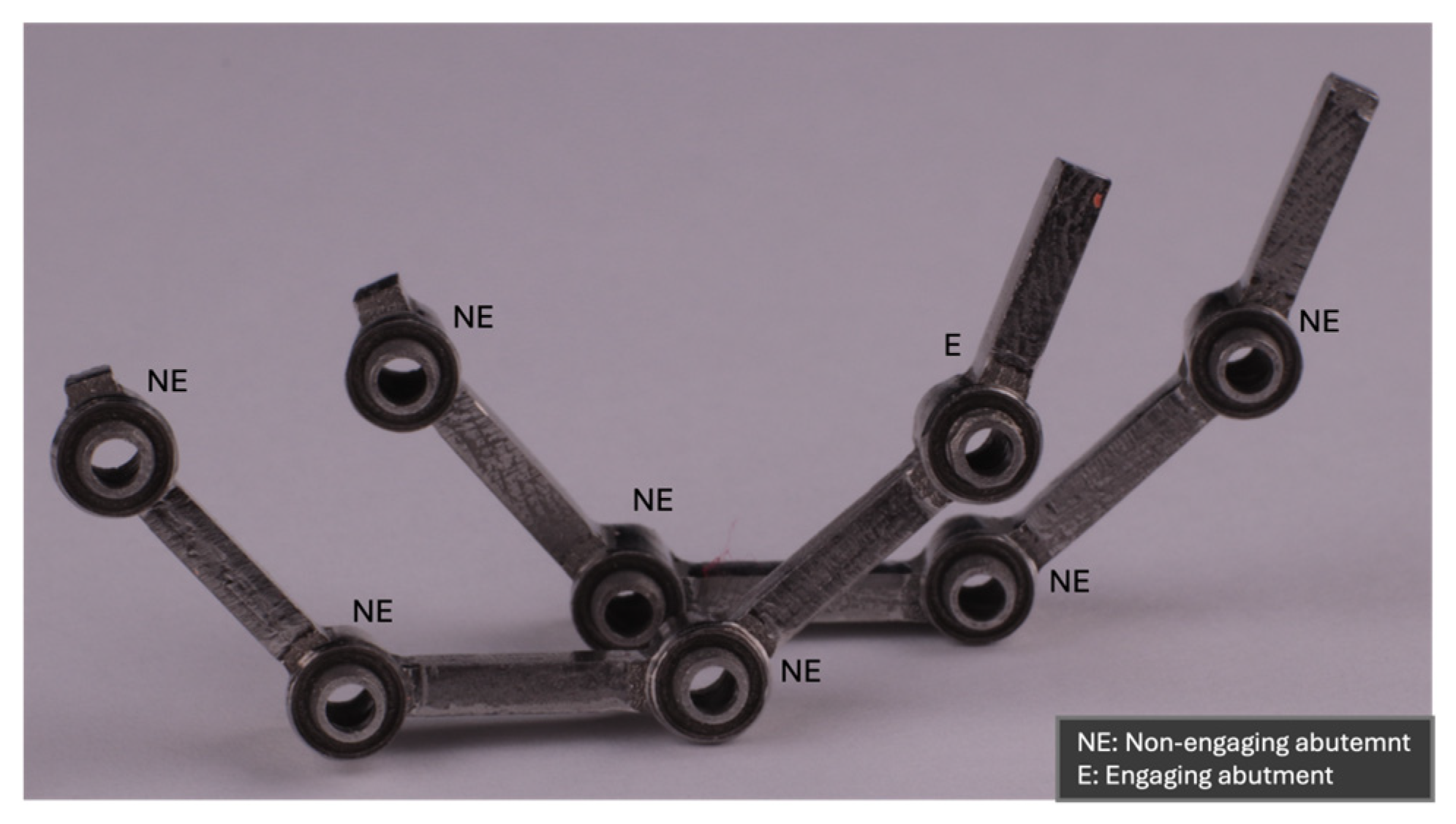
2.2. Test Framework Fabrication
2.3. Strain Gauge Placement and Calibration
2.4. Preload Measurements and Cyclic Loading
2.5. Statistical Analysis
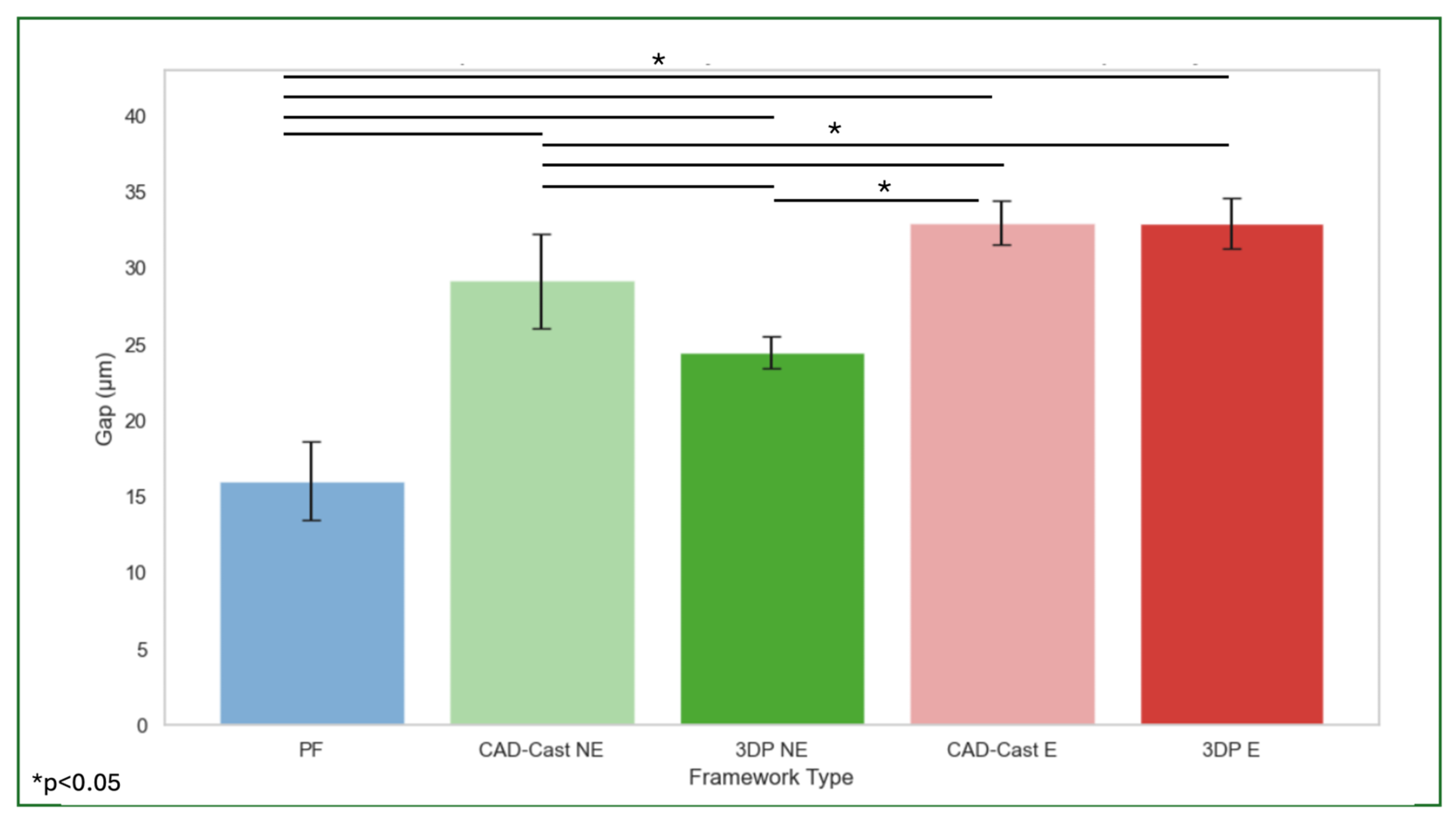
3. Results
4. Discussion
5. Conclusions
- ⚬
- 3DP technique produces prostheses with better implant–abutment fit than the CAD-cast.
- ⚬
- Using a single engaging terminal abutment results in an implant–abutment misfit that remains within acceptable limits.
- ⚬
- Different manufacturing techniques produce approximate preload values at the implant–abutment connection screw when the prosthesis is loaded.
- ⚬
- Using only non-engaging abutments results in higher preload values with the CAD-cast manufacturing technique.
- ⚬
- Using a single engaging terminal abutment results in higher preload values with the 3DP manufacturing technique.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CAD | Computer-aided design |
| CAD/CAM | Computer-aided design/computer-aided manufacturing |
| E | Engaging abutment |
| ICFDP | Implant-supported cantilever fixed dental prostheses |
| NE | Non-engaging abutment |
| PF | Passive fit |
| SEM | Scanning electron microscope |
| 3DP | Three-dimensional printing |
References
- Asvanund, P. A Strain Gauge Analysis Comparing External and Internal Implant Abutment Connections. Implant. Dent. 2014, 23, 206–211. [Google Scholar] [CrossRef]
- Epprecht, A.; Zeltner, M.; Benic, G.; Özcan, M. A strain gauge analysis comparing 4-unit veneered zirconium dioxide implant-borne fixed dental prosthesis on engaging and non-engaging abutments before and after torque application. Clin. Exp. Dent. Res. 2018, 4, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Storelli, S.; Del Fabbro, M.; Scanferla, M.; Palandrani, G.; Romeo, E. Implant-supported cantilevered fixed dental rehabilitations in fully edentulous patients: Systematic review of the literature. Part II. Clin. Oral Implants Res. 2018, 29 (Suppl. 18), 275–294. [Google Scholar] [CrossRef] [PubMed]
- Schmid, E.; Morandini, M.; Roccuzzo, A.; Ramseier, C.A.; Sculean, A.; Salvi, G.E. Clinical and radiographic outcomes of implant-supported fixed dental prostheses with cantilever extension. A retrospective cohort study with a follow-up of at least 10 years. Clin. Oral Implants Res. 2020, 31, 1243–1252. [Google Scholar] [CrossRef]
- Purcell, B.; McGlumphy, E.; Yilmaz, B.; Holloway, J.; Beck, F. Anteroposterior Spread and Cantilever Length in Mandibular Metal-Resin Implant-Fixed Complete Dental Prostheses: A 7- to 9-Year Analysis. Int. J. Prosthodont. 2015, 28, 512–518. [Google Scholar] [CrossRef]
- Nishioka, R.S.; Nishioka, L.N.B.d.M.; Abreu, C.W.; de Vasconcellos, L.G.O.; Balducci, I. Machined and plastic copings in three-element prostheses with different types of implant-abutment joints: A strain gauge comparative analysis. J. Appl. Oral Sci. 2010, 18, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Catapano, S.; Ferrari, M.; Mobilio, N.; Montanari, M.; Corsalini, M.; Grande, F. Comparative analysis of the stability of prosthetic screws under cyclic loading in implant prosthodontics: An in vitro study. Appl. Sci. 2021, 11, 622. [Google Scholar] [CrossRef]
- Eliasson, A.; Eriksson, T.; Johansson, A.; Wennerberg, A. Fixed partial prostheses supported by 2 or 3 implants: A retrospective study up to 18 years. Int. J. Oral Maxillofac. Implants 2006, 21, 567–574. [Google Scholar] [PubMed]
- Romeo, E.; Storelli, S. Systematic review of the survival rate and the biological, technical, and aesthetic complications of fixed dental prostheses with cantilevers on implants reported in longitudinal studies with a mean of 5 years follow-up. Clin. Oral Implants Res. 2012, 23 (Suppl. 6), 39–49. [Google Scholar] [CrossRef]
- Schoenbaum, T.R.; Stevenson, R.G.; Balinghasay, E. The hemi-engaging fixed dental implant prosthesis: A technique for improved stability and handling. J. Prosthet. Dent. 2017, 120, 17–19. [Google Scholar] [CrossRef]
- Presotto, A.G.C.; Barão, V.A.R.; Bhering, C.L.B.; Mesquita, M.F. Dimensional precision of implant-supported frameworks fabricated by 3D printing. J. Prosthet. Dent. 2019, 122, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Sadeghpour, M.; Özcan, M. A Review of the Applications of Additive Manufacturing Technologies Used to Fabricate Metals in Implant Dentistry. J. Prosthodont. 2020, 29, 579–593. [Google Scholar] [CrossRef]
- Rutkunas, V.; Gedrimiene, A.; Jacobs, R.; Malinauskas, M. Comparison of conventional and digital workflows for implant-supported screw-retained zirconia FPD bars: Fit and cement gap evaluation using SEM analysis. Int. J. Oral Implantol. 2021, 14, 199–210. [Google Scholar]
- Rekow, E.D. Digital dentistry: The new state of the art—Is it disruptive or destructive? Dent. Mater. 2020, 36, 9–24. [Google Scholar] [CrossRef]
- Ramalho, I.; Witek, L.; Coelho, P.; Bergamo, E.; Pegoraro, L.; Bonfante, E. Influence of Abutment Fabrication Method on 3D Fit at the Implant-Abutment Connection. Int. J. Prosthodont. 2020, 33, 641–647. [Google Scholar] [CrossRef]
- Bohner, L.; Hanisch, M.; De Luca Canto, G.; Mukai, E.; Sesma, N.; Tortamano Neto, P. Accuracy of casts fabricated by digital and conventional implant impressions. J. Oral Implantol. 2019, 45, 94–99. [Google Scholar] [CrossRef]
- Bae, S.; Hong, M.H.; Lee, H.; Lee, C.H.; Hong, M.; Lee, J.; Lee, D.-H. Reliability of metal 3D printing with respect to the marginal fit of fixed dental prostheses: A systematic review and meta-analysis. Materials 2020, 13, 4781. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Chen, Y.-W.; Alshawaf, B.; Kang, K.; Finkelman, M.; Chronopoulos, V.; Weber, H.-P. Digital workflow: In vitro accuracy of 3D printed casts generated from complete-arch digital implant scans. J. Prosthet. Dent. 2020, 124, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Kourtis, S.; Damanaki, M.; Kaitatzidou, S.; Kaitatzidou, A.; Roussou, V. Loosening of the fixing screw in single implant crowns: Predisposing factors, prevention and treatment options. J. Esthet. Restor. Dent. 2017, 29, 233–246. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Wang, J. Mechanism of and factors associated with the loosening of the implant abutment screw: A review. J. Esthet. Restor. Dent. 2019, 31, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Dogus, S.M.; Kurtz, K.S.; Watanabe, I.; Griggs, J.A. Effect of engaging abutment position in implant-borne, screw-retained three-unit fixed cantilevered prostheses. J. Prosthodont. 2011, 20, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Merz, B.R.; Hunenbart, S.; Belser, U.C. Mechanics of the implant-abutment connection: An 8-degree taper compared to a butt joint connection. Int. J. Oral Maxillofac. Implants 2000, 15, 519–526. [Google Scholar]
- Gracis, S.; Michalakis, K.; Vigolo, P.; Vult von Steyern, P.; Zwahlen, M.; Sailer, I. Internal vs. external connections for abutments/reconstructions: A systematic review. Clin. Oral Implants Res. 2012, 23 (Suppl. 6), 202–216. [Google Scholar] [CrossRef] [PubMed]
- Kwan, J.C.; Kwan, N. The effects of a vertical compressive cyclic load on abutment screws and the stability of the prosthesis in nonengaging and partially engaging abutments in a screw-retained splinted fixed dental prosthesis. Int. J. Oral Maxillofac. Implants 2022, 37, 571–578. [Google Scholar] [CrossRef]
- Siripru, J.; Puengpaiboon, U.; Sukjamsri, C.; Mahardawi, B.; Aimjirakul, N. Impact of type and position of abutment connection on microstrain distribution: An in vitro study. J. Adv. Prosthodont. 2024, 16, 290. [Google Scholar] [CrossRef]
- Vetromilla, B.M.; Brondani, L.P.; Pereira-Cenci, T.; Bergoli, C.D. Influence of different implant-abutment connection designs on the mechanical and biological behavior of single-tooth implants in the maxillary esthetic zone: A systematic review. J. Prosthet. Dent. 2019, 121, 398–403.e3. [Google Scholar] [CrossRef]
- Savignano, R.; Soltanzadeh, P.; Suprono, M.S. Computational biomechanical analysis of engaging and nonengaging abutments for implant screw-retained fixed dental prostheses. J. Prosthodont. 2020, 30, 604–609. [Google Scholar] [CrossRef]
- Altuwaijri, S.M.; Alotaibi, H.N.; Alnassar, T.M. The effect of the digital manufacturing technique of cantilevered implant-supported frameworks on abutment screw preload. J. Adv. Prosthodont. 2022, 14, 22–31. [Google Scholar] [CrossRef]
- El-Sheikh, M.A.Y.; Mostafa, T.M.N.; El-Sheikh, M.M. Effect of different angulations and collar lengths of conical hybrid implant abutment on screw loosening after dynamic cyclic loading. Int. J. Implant. Dent. 2018, 4, 39. [Google Scholar] [CrossRef] [PubMed]
- Hecker, D.M.; Eckert, S.E.; Choi, Y.G. Cyclic loading of implant-supported prostheses: Comparison of gaps at the prosthetic-abutment interface when cycled abutments are replaced with as-manufactured abutments. J. Prosthet. Dent. 2006, 95, 26–32. [Google Scholar] [CrossRef]
- Benjaboonyazit, K.; Chaijareenont, P.; Khongkhunthian, P. Removal torque pattern of a combined cone and octalobule index implant-abutment connection at different cyclic loading: An in vitro experimental study. Int. J. Implant. Dent. 2019, 5, 1. [Google Scholar] [CrossRef]
- Ramalho, I.S.; Bergamo, E.T.P.; Witek, L.; Coelho, P.G.; Lopes, A.C.O.; Bonfante, E.A. Implant-abutment fit influences the mechanical performance of single-crown prostheses. J. Mech. Behav. Biomed. Mater. 2020, 102, 103506. [Google Scholar] [CrossRef]
- Katsoulis, J.; Takeichi, T.; Gaviria, A.S.; Peter, L.; Katsoulis, K. Misfit of implant prostheses and its impact on clinical outcomes. Definition, assessment and a systematic review of the literature. Eur. J. Oral Implantol. 2017, 10, 121–138. [Google Scholar]
- Abduo, J.; Bennani, V.; Waddell, N.; Lyons, K.; Swain, M. Assessing the fit of implant fixed prostheses: A critical review. Int. J. Oral Maxillofac. Implants 2010, 25, 506–515. [Google Scholar]
- Papaspyridakos, P.; Chen, C.J.; Chuang, S.K.; Weber, H.P.; Gallucci, G.O. A systematic review of biologic and technical complications with fixed implant rehabilitations for edentulous patients. Int. J. Oral Maxillofac. Implants 2012, 27, 102–110. [Google Scholar] [PubMed]
- Karl, M.; Graef, F.; Wichmann, M.; Krafft, T. Passivity of fit of CAD/CAM and copy-milled frameworks, veneered frameworks, and anatomically contoured zirconia ceramic implant-supported fixed prostheses. J. Prosthet. Dent. 2012, 107, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Jemt, T.; Book, K. Prosthesis misfit and marginal bone loss in edentulous implant patients. Int. J. Oral Maxillofac. Implants 1997, 11, 620–625. [Google Scholar]
- Gonzalo, E.; Vizoso, B.; Lopez-Suarez, C.; Diaz, P.; Pelaez, J.; Suarez, M.J. Evaluation of milled titanium versus laser sintered Co-Cr abutments on the marginal misfit in internal implant-abutment connection. Materials 2020, 13, 4873. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Tsoi, J.K.H.; Lam, W.Y.H.; Pow, E.H.N. Implant framework misfit: A systematic review on assessment methods and clinical complications. Clin. Implant. Dent. Relat. Res. 2021, 23, 244–258. [Google Scholar] [CrossRef]
- Katsoulis, J.; Müller, P.; Mericske-Stern, R.; Blatz, M.B. CAD/CAM fabrication accuracy of long- vs. short-span implant-supported FDPs. Clin. Oral Implants Res. 2015, 26, 245–249. [Google Scholar] [CrossRef]
- Bhering, C.L.B.; Marques, I.D.S.V.; Takahashi, J.M.F.K.; Barão, V.A.R.; Consani, R.L.X.; Mesquita, M.F. The effect of casting and masticatory simulation on strain and misfit of implant-supported metal frameworks. Mater. Sci. Eng. C 2016, 62, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Duyck, J.; Naert, I. Influence of prosthesis fit and the effect of a luting system on the prosthetic connection preload: An in vitro study. Int. J. Prosthodont. 2002, 15, 123–129. [Google Scholar]
- Hegde, R.; Lemons, J.E.; Broome, J.C.; McCracken, M.S. Validation of strain gauges as a method of measuring precision of fit of implant bars. Implant. Dent. 2009, 18, 151–161. [Google Scholar] [CrossRef]
- Fan, X.; Chen, L.; Chen, Q.; Wang, F.; Wu, Y.; Sun, Y. Influence of a mesial cantilever on stress, strain, and axial force in fixed partial dentures with a distally tilted implant in the atrophic posterior maxilla. J. Prosthodont. Res. 2024, 68, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Taşın, S.; Turp, I.; Bozdağ, E.; Sünbüloğlu, E.; Üşümez, A. Evaluation of strain distribution on an edentulous mandible generated by cobalt-chromium metal alloy fixed complete dentures fabricated with different techniques: An in vitro study. J. Prosthet. Dent. 2019, 122, 47–53. [Google Scholar] [CrossRef]
- Revilla-Leon, M.; Özcan, M. Additive manufacturing technologies used for processing polymers: Current status and potential application in prosthetic dentistry. J. Prosthodont. 2019, 28, 146–158. [Google Scholar] [CrossRef]
- Revilla Leon, M.; Klemm, I.; Garcia-Arranz, J.; Özcan, M. 3D metal printing—Additive manufacturing technologies for frameworks of implant-borne fixed dental prosthesis. Eur. J. Prosthodont. Restor. Dent. 2017, 25, 143–147. [Google Scholar]
- Yıldırım, Ö.; Yeşil, Z.; Hatipoğlu, Ö. Effect of different 3D-printing systems on the flexural strength of provisional fixed dental prostheses: A systematic review and network meta-analysis of in vitro studies. BMC Oral Health 2025, 25, 82. [Google Scholar] [CrossRef]
- Alageel, O. Three-dimensional printing technologies for dental prosthesis: A review. Rapid Prototyp. J. 2022, 28, 1764–1778. [Google Scholar] [CrossRef]
- ISO 14801:2017; Dentistry—Implants—Dynamic Loading Test for Endosseous Dental Implants. ISO: Geneva, Switzerland, 2017.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PF | CAD-cast_NE | 3DP_NE | CAD-cast_E | 3DP_E | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean (BP) | Mean (LP) | Mean (BP) | Mean (LP) | Mean (BP) | Mean (LP) | Mean (BP) | Mean (LP) | Mean (BP) | Mean (LP) | |
| Implant No. 1 | 12.00 | 16.33 | 26.10 | 25.70 | 24.67 | 24.57 | 30.53 | 34.53 | 34.00 | 35.33 |
| Implant No. 2 | 12.00 | 16.33 | 30.50 | 28.90 | 24.00 | 24.00 | 33.93 | 33.73 | 32.00 | 31.33 |
| Implant No. 3 | 17.33 | 17.33 | 32.80 | 31.60 | 22.67 | 22.67 | 31.93 | 32.07 | 32.00 | 31.67 |
| Implant No. 4 | 18.00 | 19.00 | 27.40 | 30.80 | 24.00 | 24.00 | 34.53 | 32.60 | 35.33 | 32.00 |
| Mean ± SD | 16.04 ± 2.60 | 29.20 ± 3.10 | 24.05 ± 1.05 | 32.98 ± 1.43 | 32.96 ± 1.67 | |||||
| Framework Manufacturing Technique | Abutment Connection Design | Mean ± SD (N) | F | Df | Mean Difference | Sig |
|---|---|---|---|---|---|---|
| CAD-cast | NE | 293.2 ± 266.5 | 2.2 | 8 | 152.4 | 0.25 |
| CAD-cast | E | 140.8 ± 87.4 | 2.2 | 8 | 152.4 | 0.25 |
| 3DP | NE | 330 ± 25 | 46 | 8 | 30 | 0.79 |
| 3DP | E | 360 ± 25 | 46 | 8 | 30 | 0.79 |
| Framework Manufacturing Technique | Mean ± SD (Preload in Ncm) | p |
|---|---|---|
| PF | 173.4 ± 79.5 | 0.5 |
| CAD-cast | 293.2 ± 266.5 | 0.5 |
| 3DP | 330 ± 253.2 | 0.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Altwaijri, S.; Alotaibi, H.; Alnassar, T.M.; Aldegheishem, A. Influence of Digital Manufacturing and Abutment Design on Full-Arch Implant Prostheses—An In Vitro Study. Materials 2025, 18, 3543. https://doi.org/10.3390/ma18153543
Altwaijri S, Alotaibi H, Alnassar TM, Aldegheishem A. Influence of Digital Manufacturing and Abutment Design on Full-Arch Implant Prostheses—An In Vitro Study. Materials. 2025; 18(15):3543. https://doi.org/10.3390/ma18153543
Chicago/Turabian StyleAltwaijri, Shahad, Hanan Alotaibi, Talal M. Alnassar, and Alhanoof Aldegheishem. 2025. "Influence of Digital Manufacturing and Abutment Design on Full-Arch Implant Prostheses—An In Vitro Study" Materials 18, no. 15: 3543. https://doi.org/10.3390/ma18153543
APA StyleAltwaijri, S., Alotaibi, H., Alnassar, T. M., & Aldegheishem, A. (2025). Influence of Digital Manufacturing and Abutment Design on Full-Arch Implant Prostheses—An In Vitro Study. Materials, 18(15), 3543. https://doi.org/10.3390/ma18153543