

Evaluation of Near-Infrared Transparent Sealants for Occlusal Sealing: An In Vitro Study

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.3. Test Phase
2.4. Statistics
3. Results
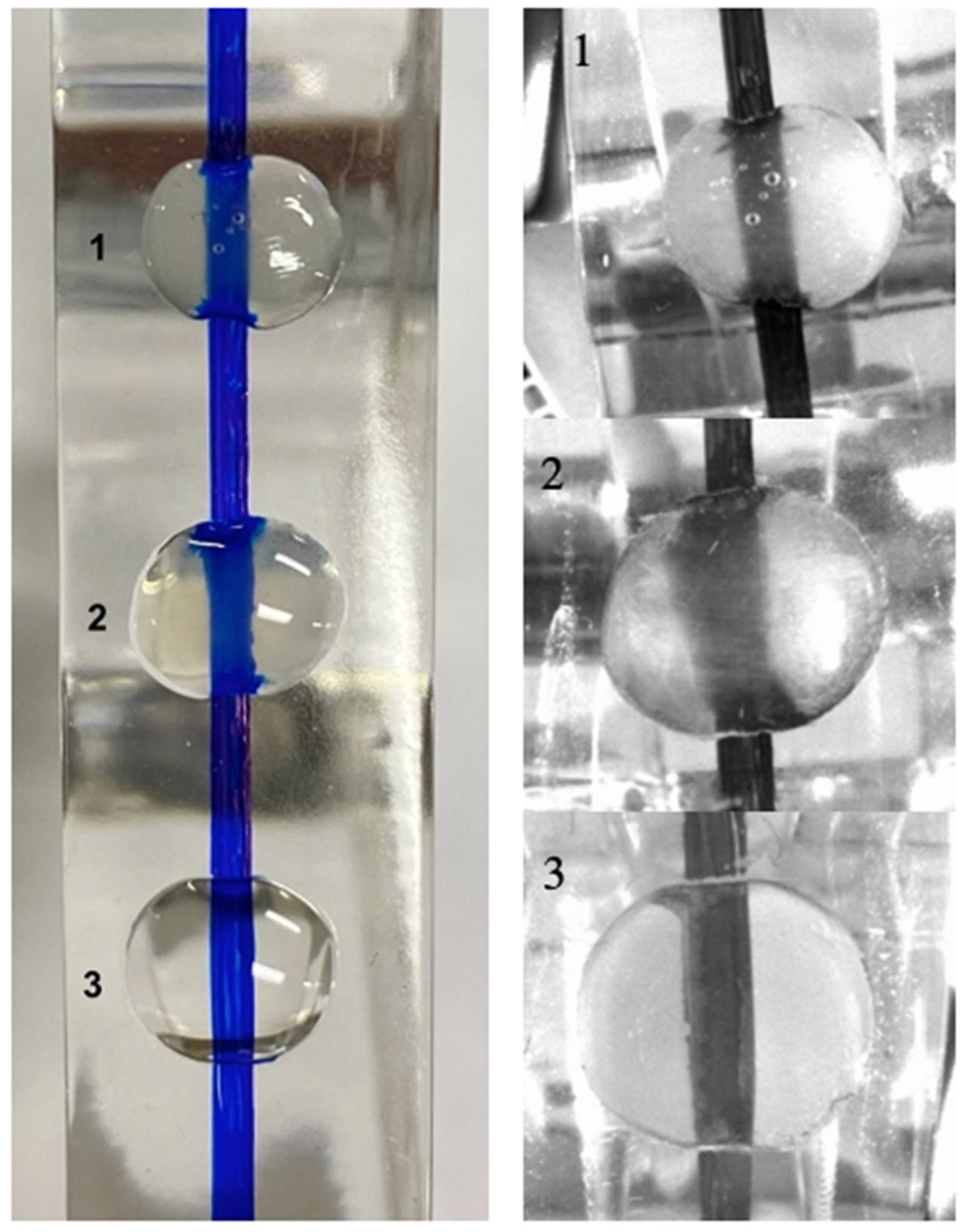
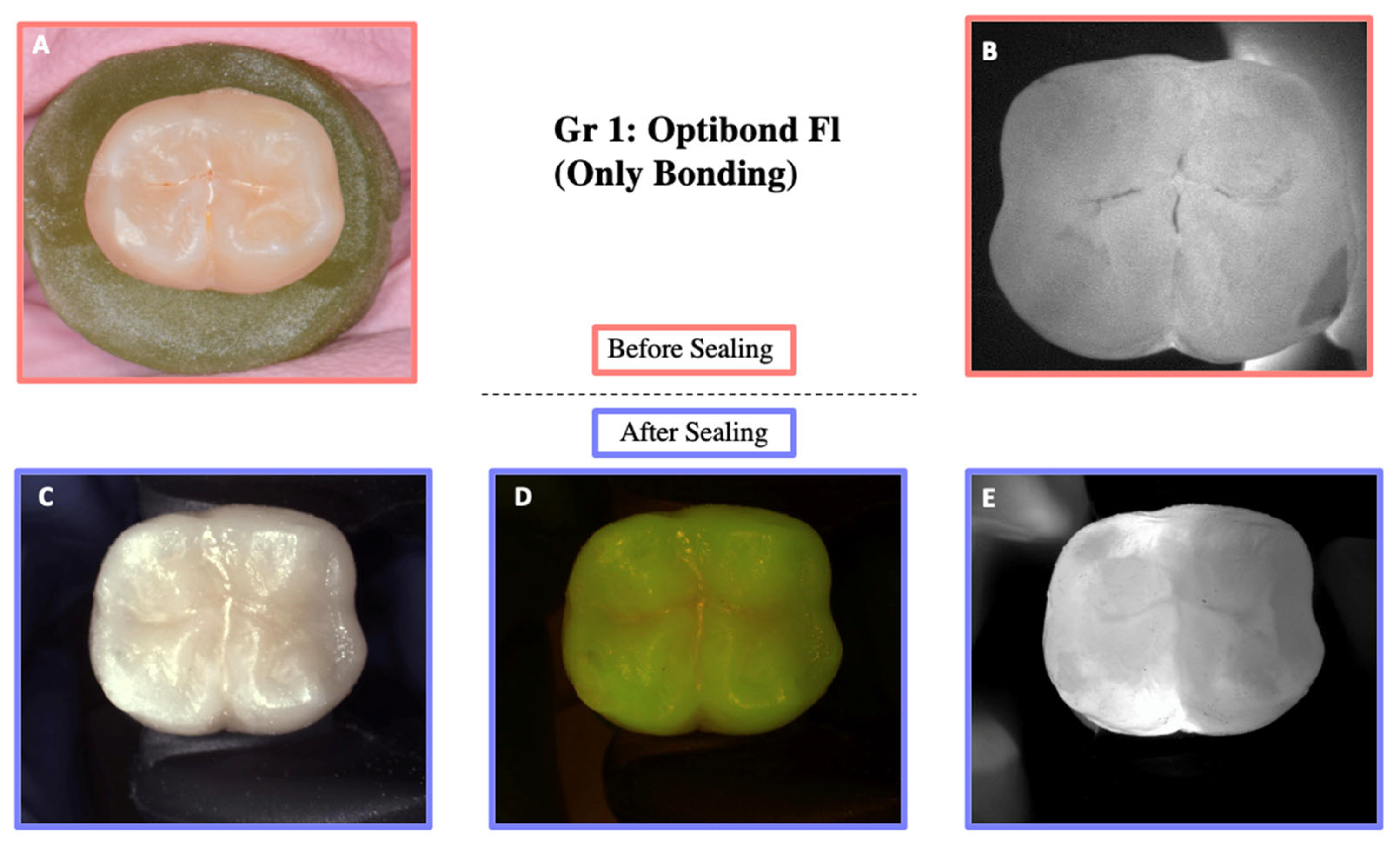
3.1. Near Infrared Translucency
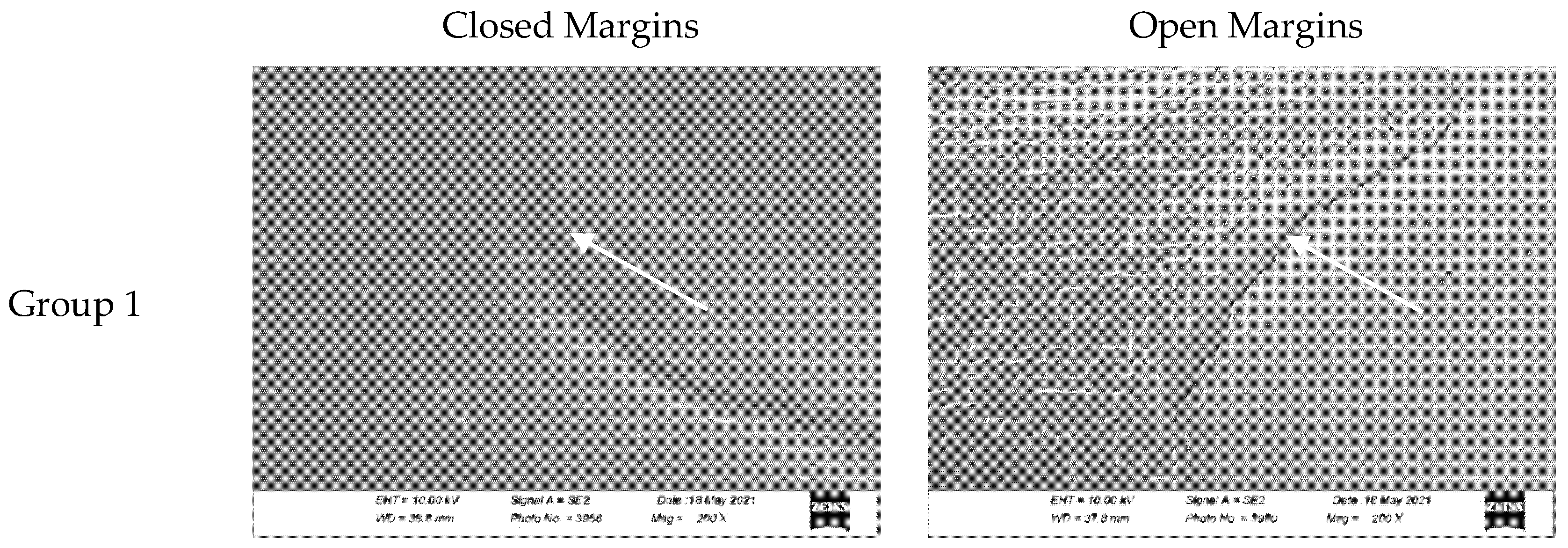
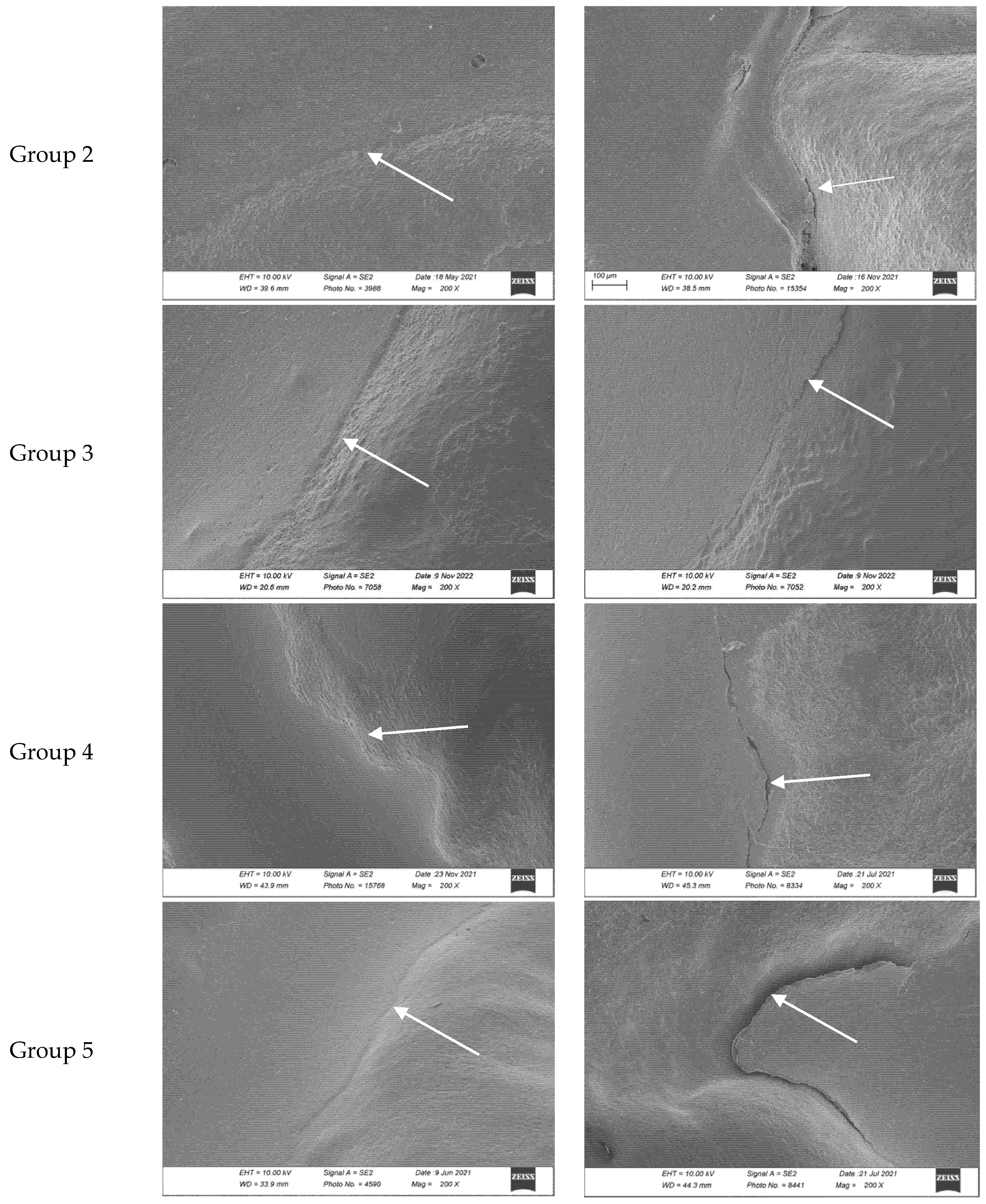
3.2. Marginal Adaptation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MDPI | Multidisciplinary Digital Publishing Institute |
| UDMA | Urethane dimethacrylate |
| Bis-GMA | Bisphenol A–glycidyl methacrylate |
| HEMA | Hydroxyethyl methacrylate |
| GPDM | Glycerol Phosphate Dimethacrylate |
| MMEP | Methacryloyloxyethyl Phosphate |
| MDP | Methacryloyloxydecyl Dihydrogen Phosphate |
| BHT | Butylated Hydroxytoluene |
| SBU | Scotchbond Universal |
| 4-MET | 4-Methacryloxyethyl Trimellitate Anhydride |
| MDTP | Methacryloyloxydecyl Dihydrogen Thiophosphate |
| NS | Non-significant |
References
- Marcenes, W.; Kassebaum, N.J.; Bernabe, E.; Flaxman, A.; Naghavi, M.; Lopez, A.; Murray, C.J. Global burden of oral conditions in 1990–2010: A systematic analysis. J. Dent. Res. 2013, 92, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Abdelaziz, M.; Krejci, I. Longitudinal Caries Detection and Monitoring with Near Infrared Transillumination; SPIE BiOS: San Francisco, CA, USA, 2019; Volume 10857. [Google Scholar]
- Abdelaziz, M.; Krejci, I. DIAGNOcam—A Near Infrared Digital Imaging Transillumination (NIDIT) technology. Int. J. Esthet. Dent. 2015, 10, 158–165. [Google Scholar] [PubMed]
- Sochtig, F.; Hickel, R.; Kuhnisch, J. Caries detection and diagnostics with near-infrared light transillumination: Clinical experiences. Quintessence Int. 2014, 45, 531–538. [Google Scholar] [PubMed]
- Amaechi, B.T. Emerging technologies for diagnosis of dental caries: The road so far. J. Appl. Phys. 2009, 105, 102047. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, D.; Lin, H. Infiltration and sealing for managing non-cavitated proximal lesions: A systematic review and meta-analysis. BMC Oral Health 2021, 21, 13. [Google Scholar] [CrossRef]
- Cvikl, B.; Moritz, A.; Bekes, K. Pit and Fissure Sealants-A Comprehensive Review. Dent. J. 2018, 6, 18. [Google Scholar] [CrossRef]
- Griffin, S.O.; Oong, E.; Kohn, W.; Vidakovic, B.; Gooch, B.F.; CDC Dental Sealant Systematic Review Work Group. The effectiveness of sealants in managing caries lesions. J. Dent. Res. 2008, 87, 169–174. [Google Scholar] [CrossRef]
- Fontana, M.; Platt, J.A.; Eckert, G.J.; Gonzalez-Cabezas, C.; Yoder, K.; Zero, D.T.; Ando, M.; Soto-Rojas, A.E.; Peters, M.C. Monitoring of sound and carious surfaces under sealants over 44 months. J. Dent. Res. 2014, 93, 1070–1075. [Google Scholar] [CrossRef]
- Beauchamp, J.; Caufield, P.W.; Crall, J.J.; Donly, K.; Feigal, R.; Gooch, B.; Ismail, A.; Kohn, W.; Siegal, M.; Simonsen, R.; et al. Evidence-based clinical recommendations for the use of pit-and-fissure sealants: A report of the American Dental Association Council on Scientific Affairs. J. Am. Dent. Assoc. 2008, 139, 257–268. [Google Scholar] [CrossRef]
- Da Silveira, A.D.; Borges, B.C.; de Almeida Varela, H.; de Lima, K.C.; Pinheiro, I.V. Progression of non-cavitated lesions in dentin through a nonsurgical approach: A preliminary 12-month clinical observation. Eur. J. Dent. 2012, 6, 34–42. [Google Scholar] [CrossRef]
- Ahovuo-Saloranta, A.; Forss, H.; Walsh, T.; Hiiri, A.; Nordblad, A.; Makela, M.; Worthington, H.V. Sealants for preventing dental decay in the permanent teeth. Cochrane Database Syst. Rev. 2013, 2013, CD001830. [Google Scholar]
- Feigal, R.J. The use of pit and fissure sealants. Pediatr. Dent. 2002, 24, 415–422. [Google Scholar]
- Pardi, V.; Pereira, A.C.; Mialhe, F.L.; Meneghim Mde, C.; Ambrosano, G.M. A 5-year evaluation of two glass-ionomer cements used as fissure sealants. Community Dent. Oral Epidemiol. 2003, 31, 386–391. [Google Scholar] [CrossRef]
- Mehrabkhani, M.; Mazhari, F.; Sadeghi, S.; Ebrahimi, M. Effects of sealant, viscosity, and bonding agents on microleakage of fissure sealants: An in vitro study. Eur. J. Dent. 2015, 9, 558–563. [Google Scholar] [CrossRef]
- Kantovitz, K.R.; Pascon, F.M.; Alonso, R.C.; Nobre-dos-Santos, M.; Rontani, R.M. Marginal adaptation of pit and fissure sealants after thermal and chemical stress. A SEM study. Am. J. Dent. 2008, 21, 377–382. [Google Scholar]
- Reddy, V.R.; Chowdhary, N.; Mukunda, K.S.; Kiran, N.K.; Kavyarani, B.S.; Pradeep, M.C. Retention of resin-based filled and unfilled pit and fissure sealants: A comparative clinical study. Contemp. Clin. Dent. 2015, 6, S18–S23. [Google Scholar] [CrossRef]
- Kumaran, P. Clinical evaluation of the retention of different pit and fissure sealants: A 1-year study. Int. J. Clin. Pediatr. Dent. 2013, 6, 183–187. [Google Scholar] [CrossRef]
- Rock, W.P.; Potts, A.J.; Marchment, M.D.; Clayton-Smith, A.J.; Galuszka, M.A. The visibility of clear and opaque fissure sealants. Br. Dent. J. 1989, 167, 395–396. [Google Scholar] [CrossRef]
- Abdelaziz, M.; Krejci, I.; Perneger, T.; Feilzer, A.; Vazquez, L. Near infrared transillumination compared with radiography to detect and monitor proximal caries: A clinical retrospective study. J. Dent. 2018, 70, 40–45. [Google Scholar] [CrossRef]
- Celiberti, P.; Carvalho, T.S.; Raggio, D.P.; Mendes, F.M. Influence of dental materials used for sealing caries lesions on laser fluorescence measurements. Lasers Med. Sci. 2012, 27, 287–295. [Google Scholar] [CrossRef]
- Rodriguez Tapia, M.T.; Ardu, S.; Daeniker, L.; Krejci, I. Evaluation of marginal adaptation, seal and resistance against fatigue cracks of different pit and fissure sealants under laboratory load. Am. J. Dent. 2011, 24, 367–371. [Google Scholar] [PubMed]
- Kersten, S.; Lutz, F.; Schupbach, P. Fissure sealing: Optimization of sealant penetration and sealing properties. Am. J. Dent. 2001, 14, 127–131. [Google Scholar]
- Stewart, C.W.; Morrow, B.R.; Garcia-Godoy, F. Evaluation of a novel instrument for placement of dental sealants. Am. J. Dent. 2020, 33, 69–73. [Google Scholar]
- Marigo, L.; Nocca, G.; Fiorenzano, G.; Calla, C.; Castagnola, R.; Cordaro, M.; Paolone, G.; Sauro, S. Influences of Different Air-Inhibition Coatings on Monomer Release, Microhardness, and Color Stability of Two Composite Materials. BioMed Res. Int. 2019, 2019, 4240264. [Google Scholar] [CrossRef]
- Krejci, I.; Reich, T.; Lutz, F.; Albertoni, M. An in vitro test procedure for evaluating dental restoration systems. 1. A computer-controlled mastication simulator. Schweiz. Monatsschr. Zahnmed. 1990, 100, 953–960. [Google Scholar]
- Mohamed Nur, M.I.M. Near Infrared Transillumination for the Detection and Monitoring of Occlusal Caries: A Retrospective Clinical Study; Université de Genève: Genève, Switzerland, 2020. [Google Scholar]
- Paolone, G.; Mandurino, M.; Scotti, N.; Cantatore, G.; Blatz, M.B. Color stability of bulk-fill compared to conventional resin-based composites: A scoping review. J. Esthet. Restor. Dent. 2023, 35, 657–676. [Google Scholar] [CrossRef]
- Peumans, M.; Kanumilli, P.; De Munck, J.; Van Landuyt, K.; Lambrechts, P.; Van Meerbeek, B. Clinical effectiveness of contemporary adhesives: A systematic review of current clinical trials. Dent. Mater. 2005, 21, 864–881. [Google Scholar] [CrossRef]
- Cehreli, Z.C.; Gungor, H.C. Quantitative microleakage evaluation of fissure sealants applied with or without a bonding agent: Results after four-year water storage in vitro. J. Adhes. Dent. 2008, 10, 379–384. [Google Scholar]
- Boksman, L.; McConnell, R.J.; Carson, B.; McCutcheon-Jones, E.F. A 2-year clinical evaluation of two pit and fissure sealants placed with and without the use of a bonding agent. Quintessence Int. 1993, 24, 131–133. [Google Scholar]
- Barreto, S.; Barbosa, I.; Pereira, G.; Dias, C.; Paulillo, L. Effects of primer excess on marginal adaptation, nanoleakage and bond strength of adhesive systems after aging. Braz. J. Oral Sci. 2019, 18, e191456. [Google Scholar] [CrossRef]
- Frankenberger, R.; Kramer, N.; Petschelt, A. Long-term effect of dentin primers on enamel bond strength and marginal adaptation. Oper. Dent. 2000, 25, 11–19. [Google Scholar] [PubMed]
- Symons, A.L.; Chu, C.Y.; Meyers, I.A. The effect of fissure morphology and pretreatment of the enamel surface on penetration and adhesion of fissure sealants. J. Oral Rehabil. 1996, 23, 791–798. [Google Scholar] [CrossRef]
- Burrow, M.F.; Burrow, J.F.; Makinson, O.F. Pits and fissures: Etch resistance in prismless enamel walls. Aust. Dent. J. 2001, 46, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Stavridakis, M.M.; Favez, V.; Campos, E.A.; Krejci, I. Marginal integrity of pit and fissure sealants. Qualitative and quantitative evaluation of the marginal adaptation before and after in vitro thermal and mechanical stressing. Oper. Dent. 2003, 28, 403–414. [Google Scholar]
- Courson, F.; Renda, A.M.; Attal, J.P.; Bouter, D.; Ruse, D.; Degrange, M. In vitro evaluation of different techniques of enamel preparation for pit and fissure sealing. J. Adhes. Dent. 2003, 5, 313–321. [Google Scholar]
- Gray, G.B.; Carey, G.P.; Jagger, D.C. An in vitro investigation of a comparison of bond strengths of composite to etched and air-abraded human enamel surfaces. J. Prosthodont. 2006, 15, 2–8. [Google Scholar] [CrossRef]
- Handelman, S.L.; Shey, Z. Michael Buonocore and the Eastman Dental Center: A historic perspective on sealants. J. Dent. Res. 1996, 75, 529–534. [Google Scholar] [CrossRef]
- Hannig, M.; Grafe, A.; Atalay, S.; Bott, B. Microleakage and SEM evaluation of fissure sealants placed by use of self-etching priming agents. J. Dent. 2004, 32, 75–81. [Google Scholar] [CrossRef]
- Celiberti, P.; Lussi, A. Use of a self-etching adhesive on previously etched intact enamel and its effect on sealant microleakage and tag formation. J. Dent. 2005, 33, 163–171. [Google Scholar] [CrossRef]
- Duangthip, D.; Lussi, A. Microleakage and penetration ability of resin sealant versus bonding system when applied following contamination. Pediatr. Dent. 2003, 25, 505–511. [Google Scholar]
- Duangthip, D.; Lussi, A. Variables contributing to the quality of fissure sealants used by general dental practitioners. Oper. Dent. 2003, 28, 756–764. [Google Scholar] [PubMed]
- Poggio, C.; Dagna, A.; Chiesa, M.; Colombo, M.; Scribante, A. Surface roughness of flowable resin composites eroded by acidic and alcoholic drinks. J. Conserv. Dent. 2012, 15, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Peker, O.; Bolgul, B. Evaluation of surface roughness and color changes of restorative materials used with different polishing procedures in pediatric dentistry. J. Clin. Pediatr. Dent. 2023, 47, 72–79. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Manufacturers | Batch No. | Composition | Protocol |
|---|---|---|---|---|
| MicroEtcher IIa | CD Dental | L1RLP | Aluminum oxide 27 microns | 5 s with a distance of 10 mm |
| Etching Ultra-Etch | Ultradent | BKGJD | 35% phosphoric acid | 60 s activated with the ultrasonic insert |
| Materials | Manufacturers | Batch No. | Composition |
|---|---|---|---|
| OptiBond FL | Kerr Dental | Primer: 9067698 Adhesive: 957693 | Primer: HEMA 1, GPDM 2, MMEP 3, ethanol, water, initiators Adhesive: Bis-GMA 4, HEMA, GPDM, barium-aluminum, borosilicate glass, disodium hexaflurosilicate, fumed silica (48% filler) |
| Scotchbond Universal | 3M | 11004A | 34% phosphoric acid, MDP 5, phosphate monomer, dimethacrylate Resins, HEMA modified, polyalkenoic acid, copolymer, filler, ethanol, water, initiators, silane |
| Fissurit | VoCo | 2031227 | Bis-GMA, UDMA 6, BHT 7, benzotriazolderiate, pyrogenic silicic acid |
| Helioseal Clear | Ivoclar Vivadent | W36096 | Bis-GMA, triethylene glycol, dimethacrylate (99% weight), catalysts, stabilizers, and pigments (1%) |
| Protocol |
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Group | Sealant Used |
|---|---|
| Group 1 | OptiBond FL (adhesive only) |
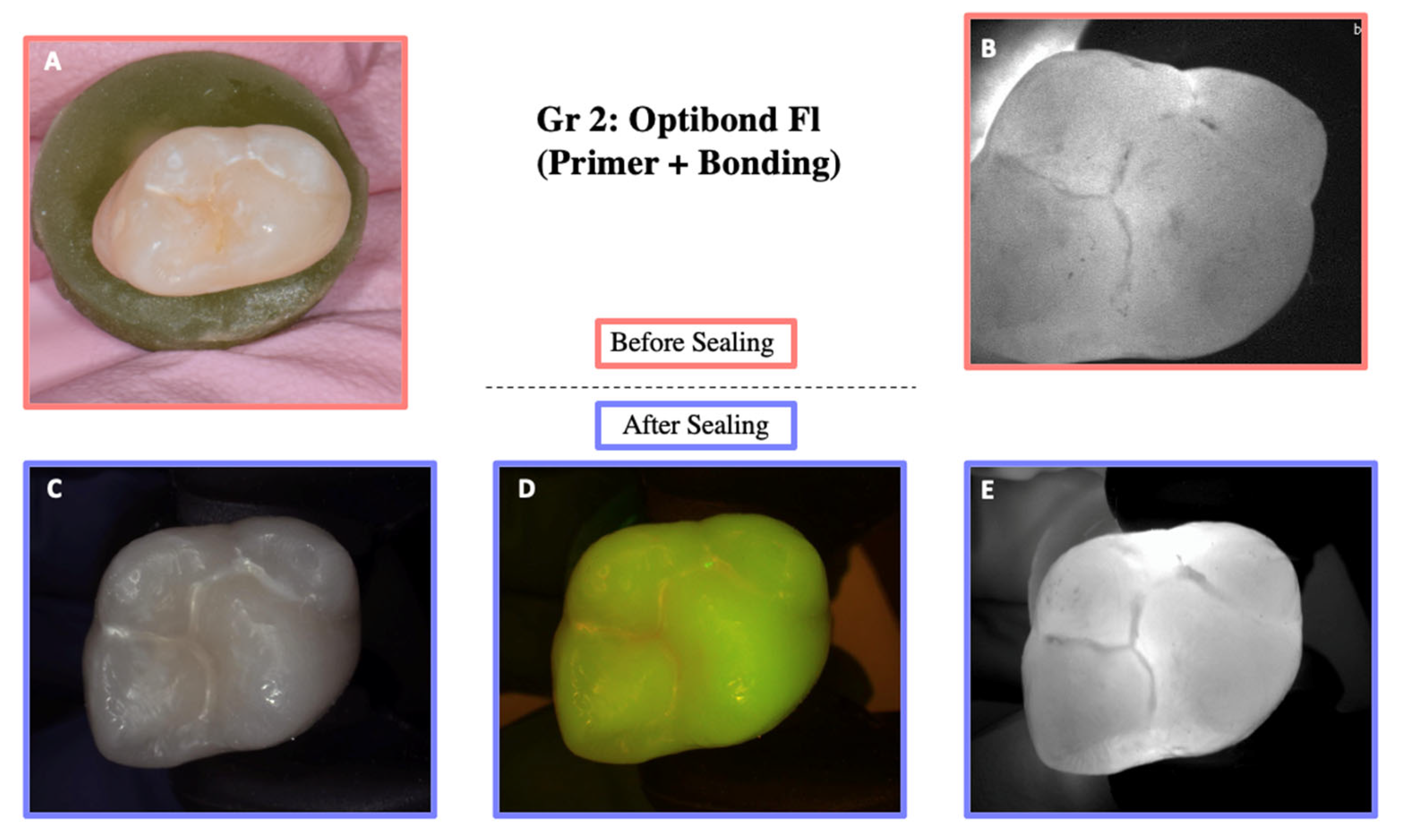
| Group 2 | OptiBond FL (primer and adhesive) |
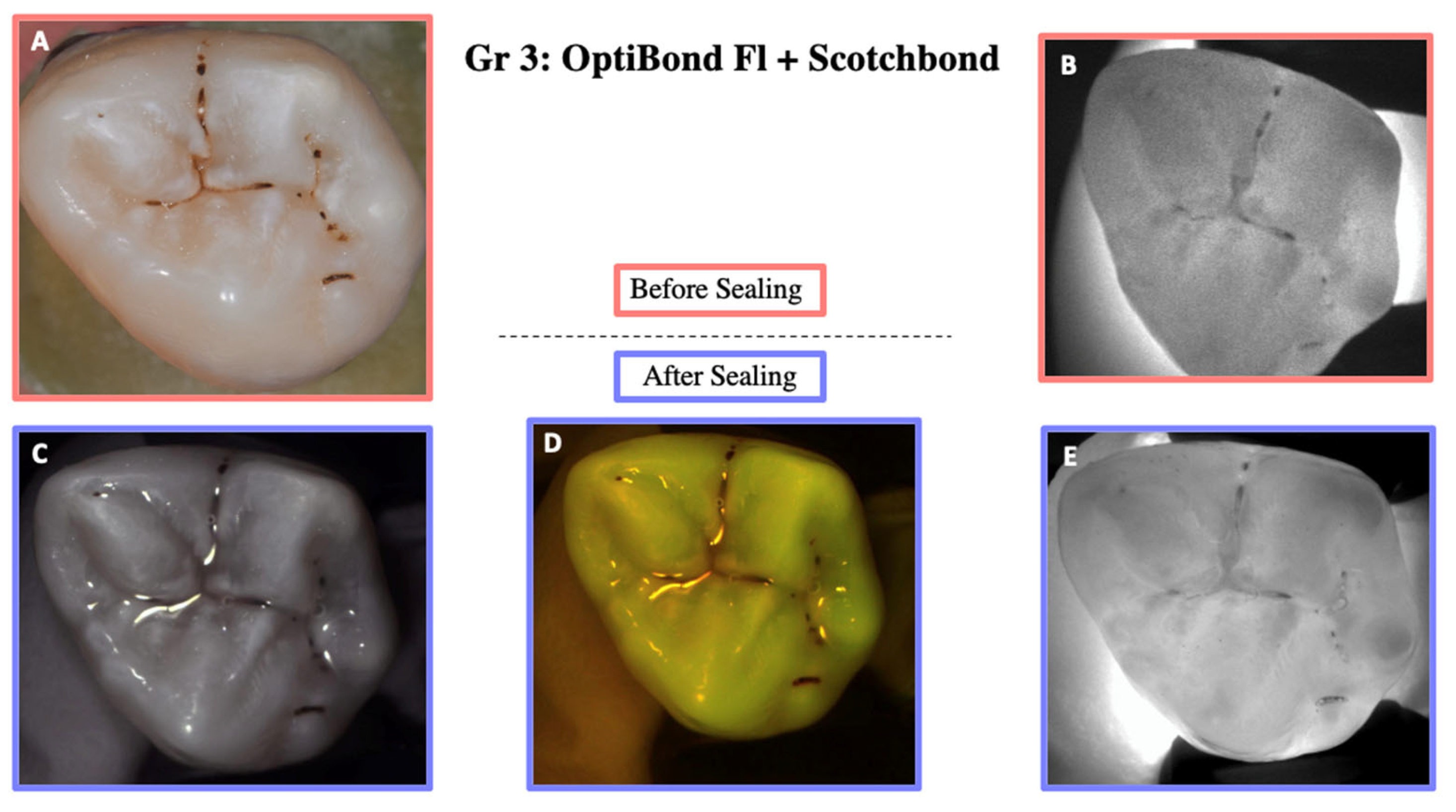
| Group 3 | Scotchbond Universal + OptiBond FL (adhesive) |
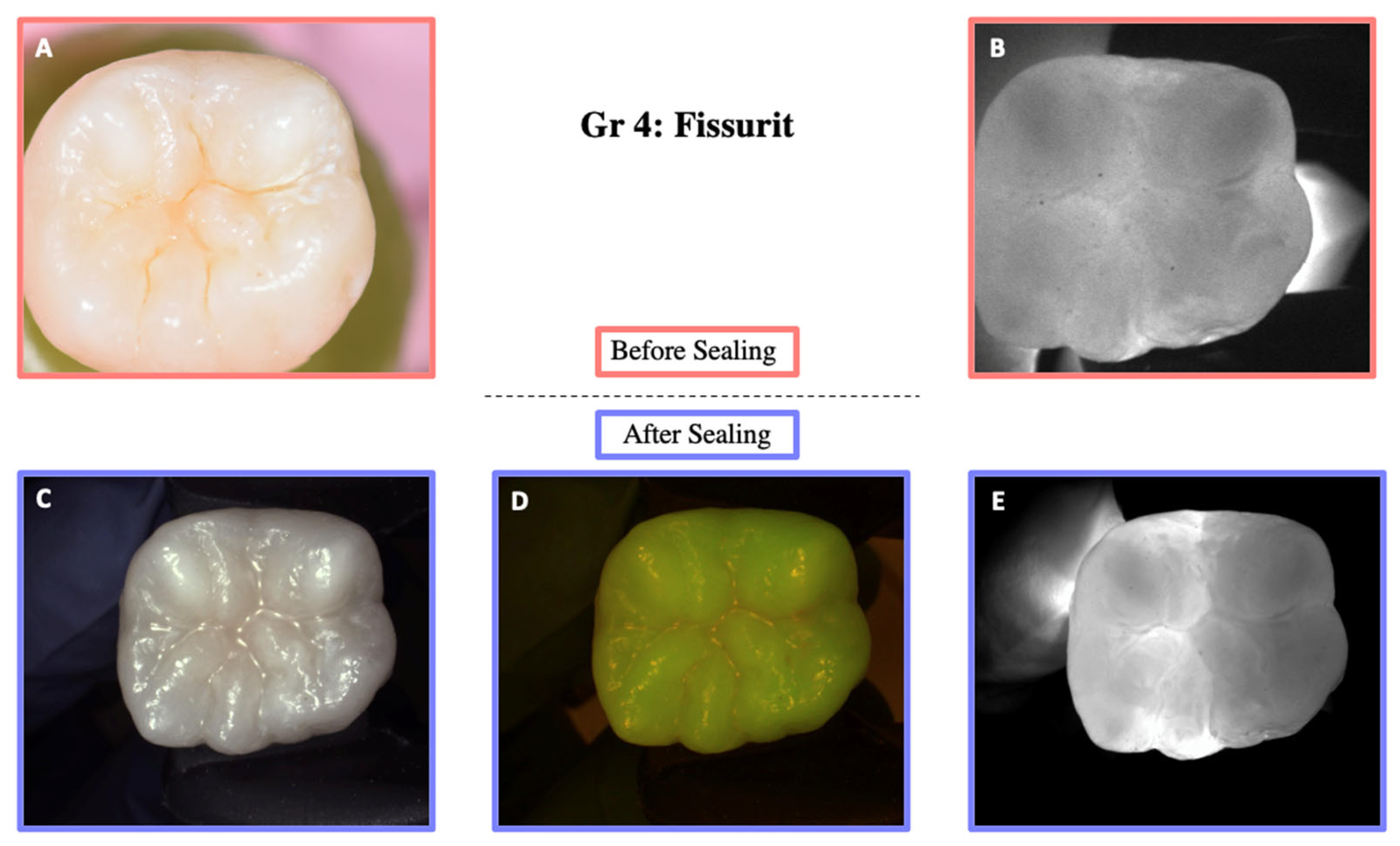
| Group 4 | Fissurit only |
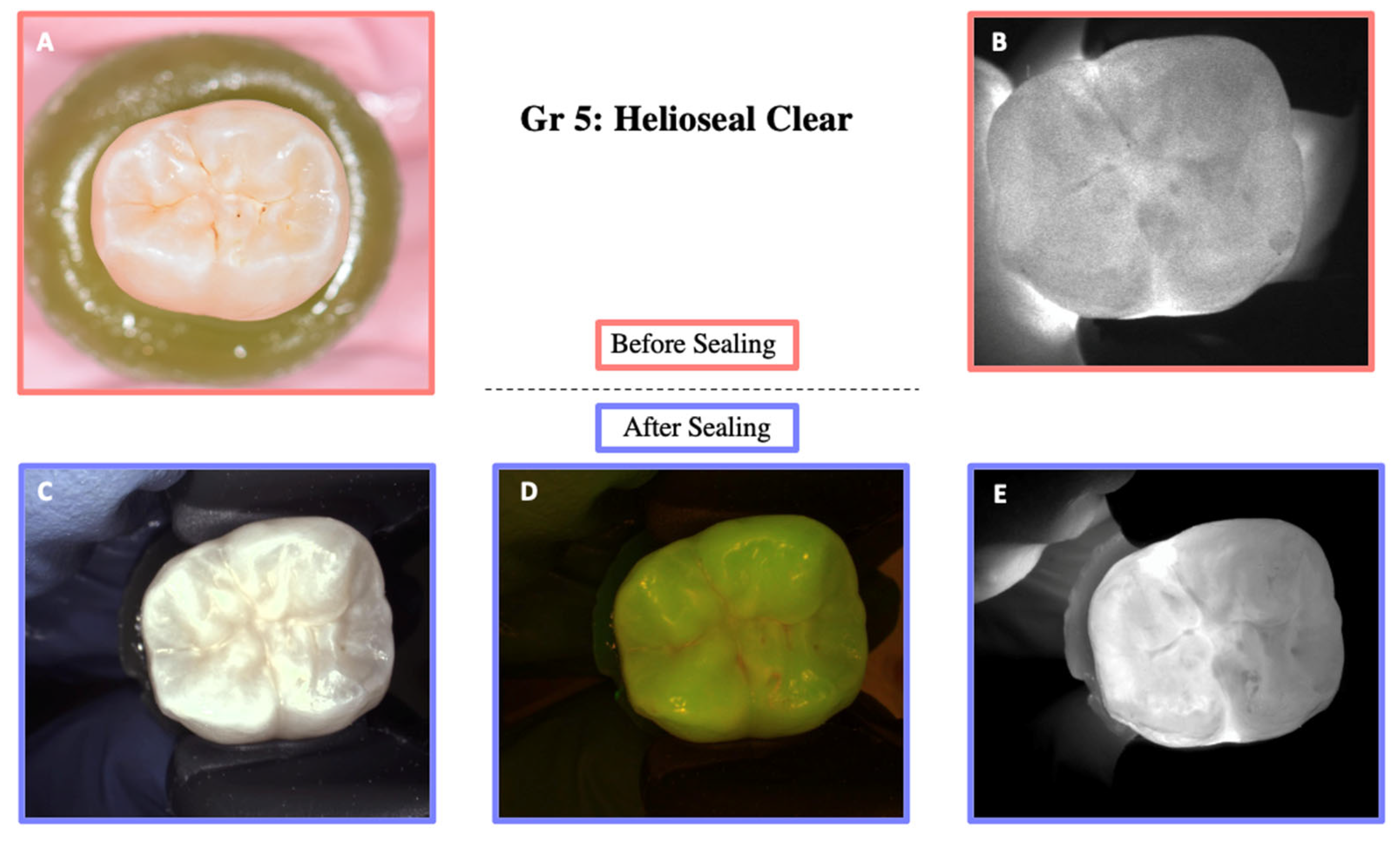
| Group 5 | Helioseal Clear only |
| Sealing Material | Transparent | Opaque |
|---|---|---|
| X | |
| X | |
| X | |
| X | |
| X |
| Group | Initial | Final |
|---|---|---|
| p = 0.3817 | p = 0.3712 |
| p = 0.2631 | p = 0.4088 |
| p = 0.9057 | p = 0.5090 |
| p = 0.3076 | p = 0.3972 |
| p = 0.0748 | p = 0.454 |
| OptiBond FL (Group 1) | Primer + Adhesive OptiBond FL (Group 2) | Scotchbond Universal + OptiBond FL (Adhesive) (Group 3) | Fissurit (Group 4) | Helioseal Clear (Group 5) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Initial | Final | Initial | Final | Initial | Final | Initial | Final | Initial | Final | |
| Mean | 96 | 92.28 | 74.42 | 69.39 | 90.62 | 89.24 | 95.2 | 89.22 | 93.25 | 88.52 |
| Median | 96.73 | 92.23 | 78.87 | 74.06 | 96.29 | 90.48 | 95.58 | 87.43 | 90.45 | 88.24 |
| Standard Deviation | 2.97 | 3.08 | 19.96 | 20.38 | 3.54 | 3.17 | 4.46 | 4.78 | 5.70 | 5.95 |
| Standard error of Mean | 1.05 | 1.09 | 7.06 | 7.21 | 1.25 | 1.12 | 1.58 | 1.69 | 2.02 | 2.10 |
| Minimum | 90.84 | 88.67 | 36.8 | 35.99 | 85.51 | 84.71 | 86.33 | 80.93 | 81.72 | 79.28 |
| Maximum | 99.17 | 96.59 | 94.36 | 91.00 | 96.10 | 94.20 | 99.17 | 94.25 | 97.87 | 95.73 |
| p-value | 0.12 | 0.001 | 0.329 | 0.001 | 0.002 | |||||
| Tukey’s Multiple Comparisons Test | Mean Diff. | 95.00% CI of Diff. | Summary | Adjusted p Value |
|---|---|---|---|---|
| OptiBond FL vs. Primer + OptiBond FL | 22.23 | 8.400–36.06 | ** | <0.001 |
| OptiBond FL vs. Fissurit | 1.928 | −11.90–15.76 | ns | 0.994 |
| OptiBond FL vs. Helioseal Clear | 3.255 | −10.58–17.08 | ns | 0.960 |
| OptiBond FL vs. SBU + OptiBond FL | 4.208 | −9.622–18.04 | ns | 0.904 |
| Primer + OptiBond FL vs. Fissurit | −20.30 | −34.13– −6.472 | ** | 0.001 |
| Primer + OptiBond FL vs. Helioseal Clear | −18.98 | −32.81– −5.146 | ** | 0.003 |
| Primer + OptiBond FL vs. SBU + OptiBond FL | −18.02 | −31.85– −4.192 | ** | 0.005 |
| Fissurit vs. Helioseal Clear | 1.327 | −12.50– 15.16 | ns | 0.999 |
| Fissurit vs. SBU + OptiBond FL | 2.281 | −11.55–16.11 | ns | 0.989 |
| Helioseal Clear vs. SBU + OptiBond FL | 0.9537 | −12.88–14.78 | ns | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Litzler, C.; Vazquez, L.; Anton Y Otero, C.I.; Krejci, I.; Rossier, I.; Abdelaziz, M. Evaluation of Near-Infrared Transparent Sealants for Occlusal Sealing: An In Vitro Study. Materials 2025, 18, 2421. https://doi.org/10.3390/ma18112421
Litzler C, Vazquez L, Anton Y Otero CI, Krejci I, Rossier I, Abdelaziz M. Evaluation of Near-Infrared Transparent Sealants for Occlusal Sealing: An In Vitro Study. Materials. 2025; 18(11):2421. https://doi.org/10.3390/ma18112421
Chicago/Turabian StyleLitzler, Camille, Lydia Vazquez, Clara Isabel Anton Y Otero, Ivo Krejci, Isaline Rossier, and Marwa Abdelaziz. 2025. "Evaluation of Near-Infrared Transparent Sealants for Occlusal Sealing: An In Vitro Study" Materials 18, no. 11: 2421. https://doi.org/10.3390/ma18112421
APA StyleLitzler, C., Vazquez, L., Anton Y Otero, C. I., Krejci, I., Rossier, I., & Abdelaziz, M. (2025). Evaluation of Near-Infrared Transparent Sealants for Occlusal Sealing: An In Vitro Study. Materials, 18(11), 2421. https://doi.org/10.3390/ma18112421