
Dentin Exposure after Tooth Preparation for Laminate Veneers: A Microscopical Analysis to Evaluate the Influence of Operators’ Expertise

 ,
,  ,
, 

Abstract
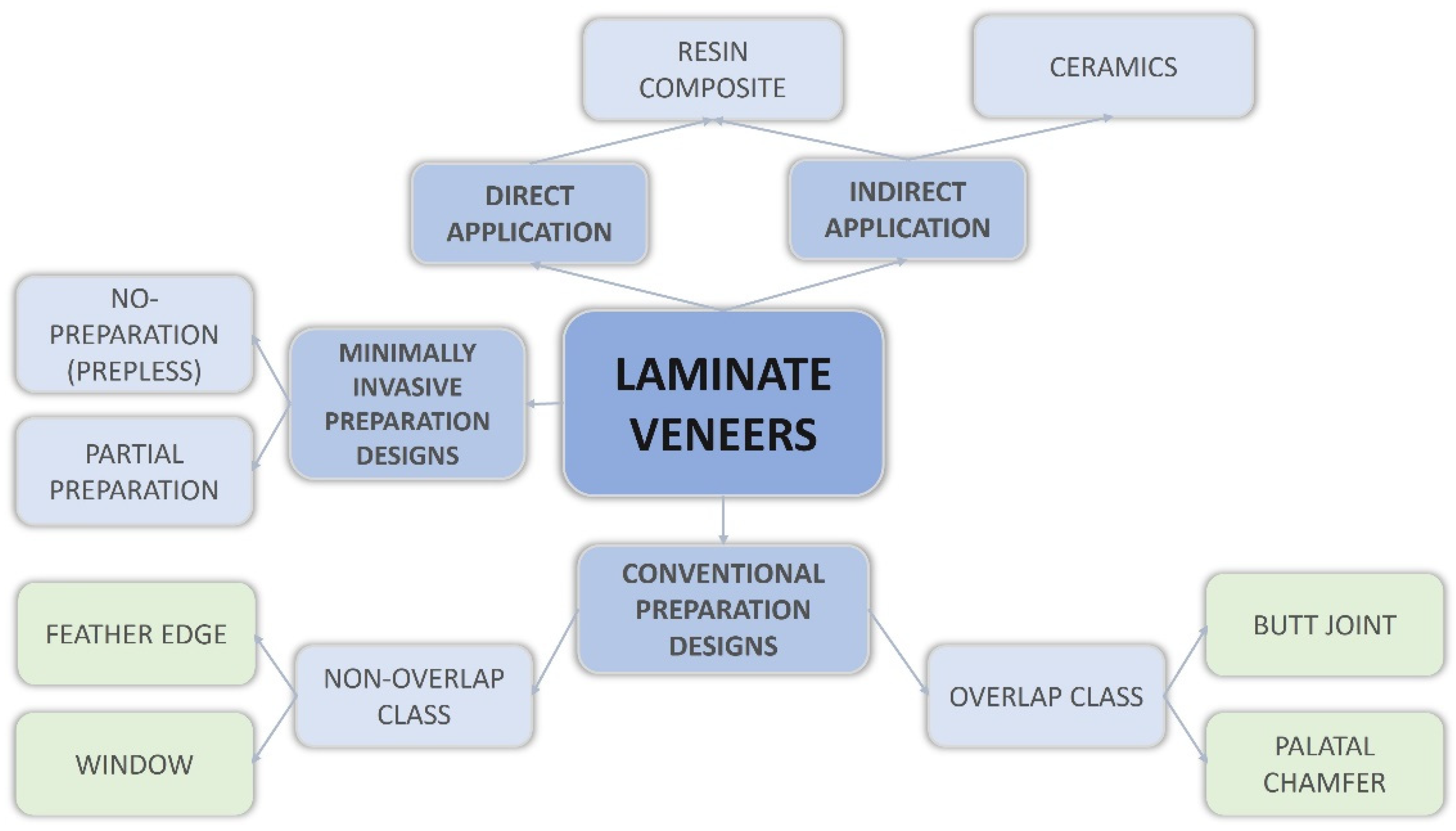
:1. Introduction
- there is no association among different designs of tooth preparation for LVs and the amount of dentin exposure;
- there is no difference both intra- and inter-individual in the discrimination under magnification between prepared enamel and dentin for operators with different clinical expertise.
2. Materials and Methods
2.1. Specimen Selection
- crown length: 10–10.5 mm;
- root length: 12–13 mm;
- mesiodistal diameter of crown: 8.5–9 mm;
- mesiodistal diameter of crown at cervix: 6.3–7 mm;
- buccopalatal diameter of crown: 7 mm;
- buccopalatal diameter of crown at cervix: 6 mm [25].
2.2. Tooth Preparation
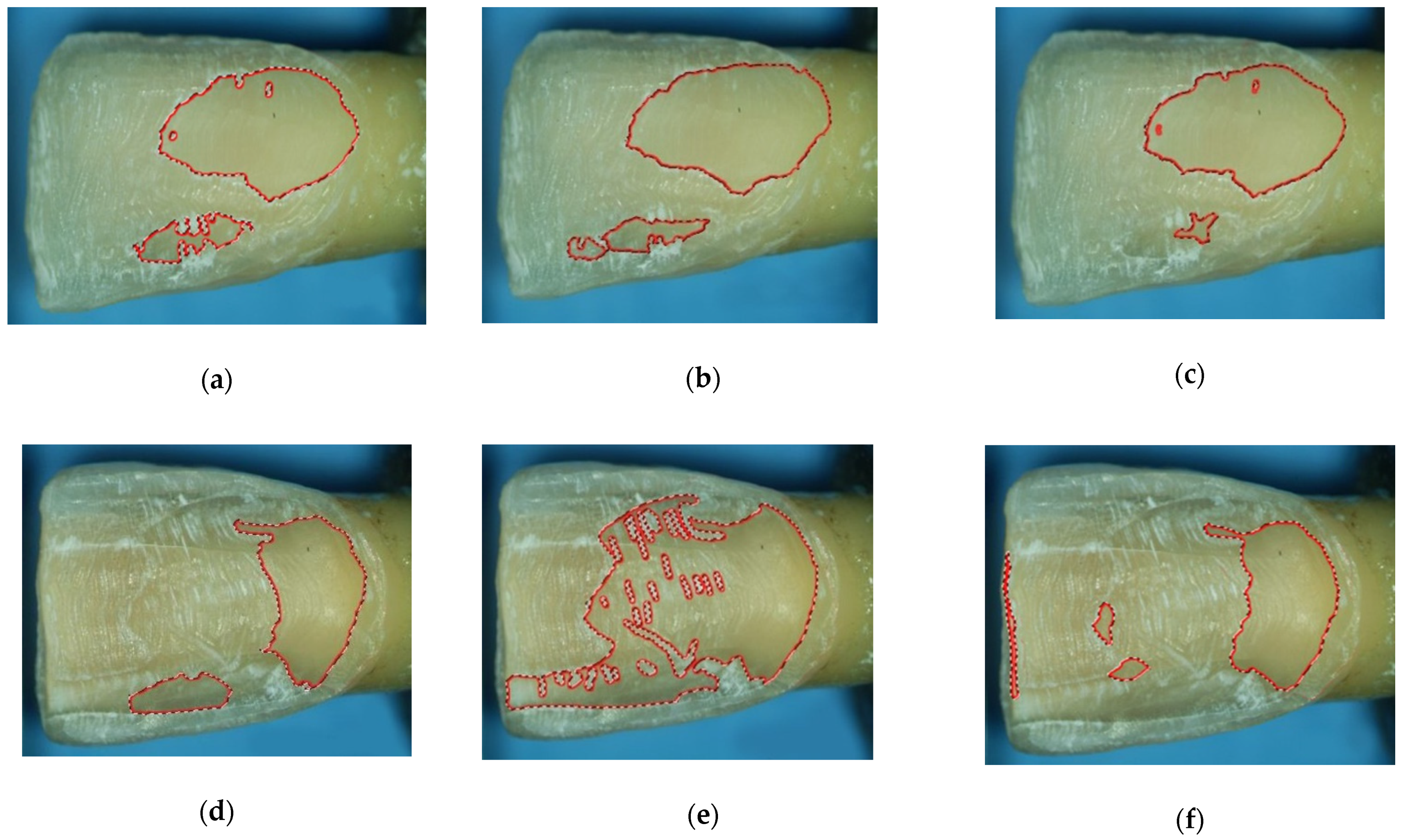
2.3. Analysis of Prepared Surfaces
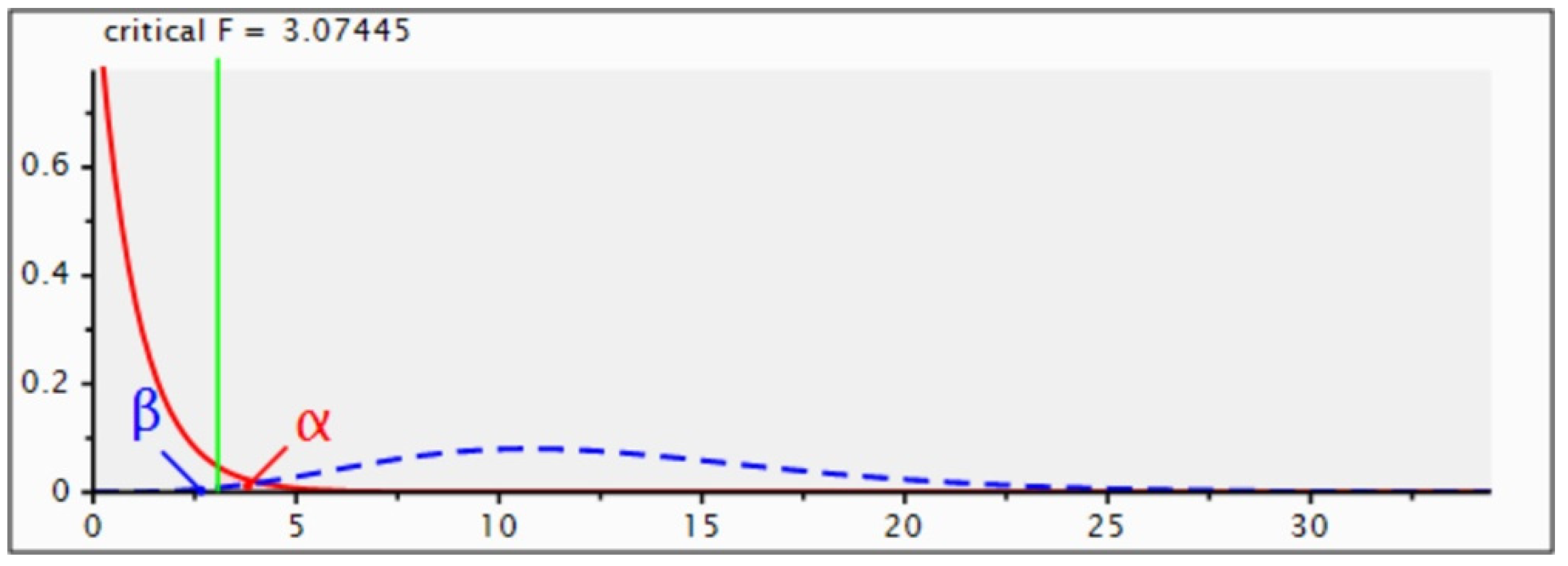
2.4. Statistical Analysis
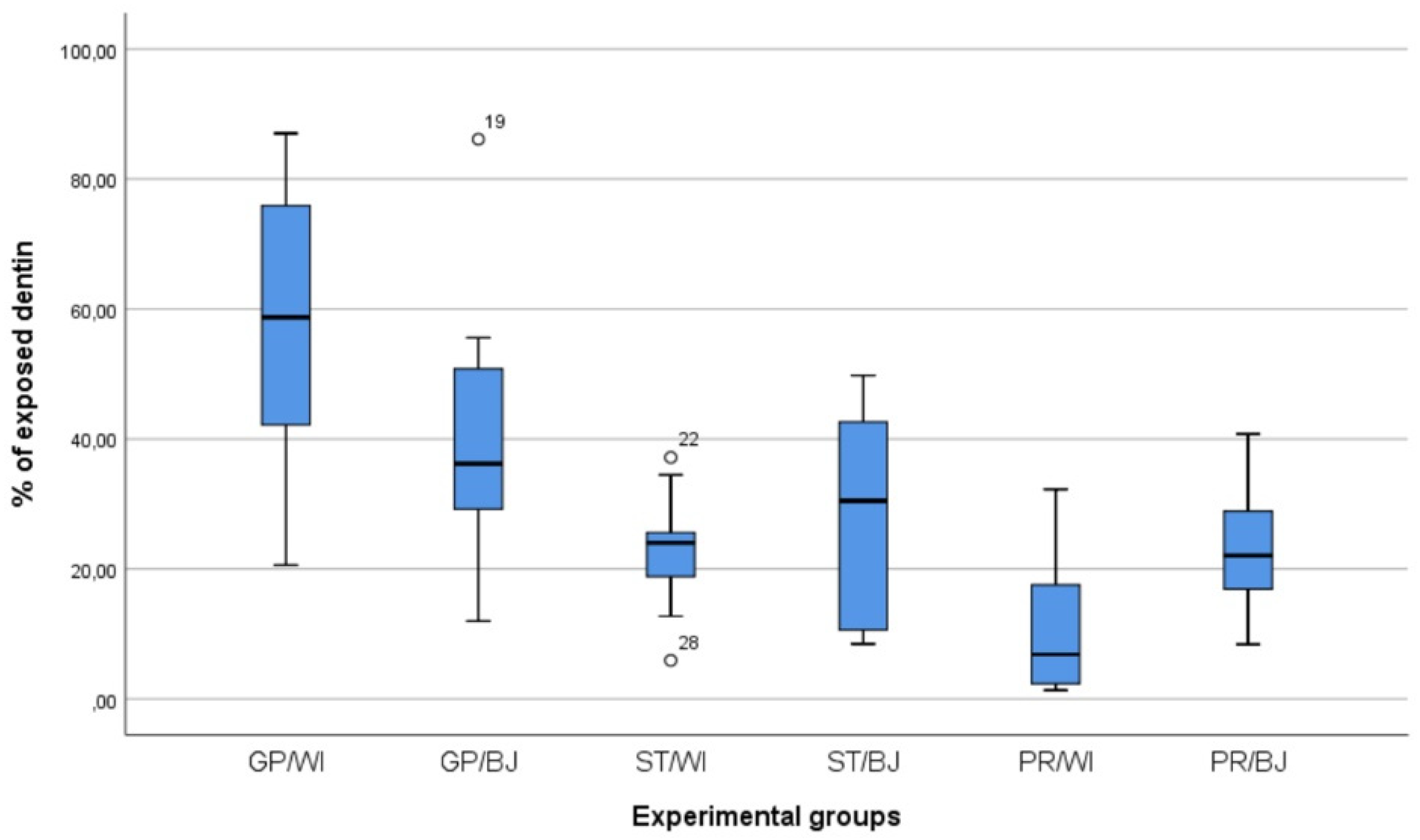
3. Results
4. Discussion
5. Conclusions
- the quantity of exposed dentin is not associated with the two considered preparation designs, namely window and butt joint;
- the expertise of clinical operators represents a discriminating factor in identifying prepared hard dental tissues, as both an undergraduate student and an expert prosthodontist showed statistically different values from a general practitioner as to the window preparation;
- in the butt joint preparation, no differences were found between the different operators;
- variability was found in the inter-individual evaluation of exposed dentin following different preparation designs for LVs;
- no intra-operator variability was detected both in window and butt joint preparations;
- magnification tools were useful to discriminate between prepared enamel and dentin.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blunck, U.; Fischer, S.; Hajtó, J.; Frei, S.; Frankenberger, R. Ceramic laminate veneers: Effect of preparation design and ceramic thickness on fracture resistance and marginal quality in vitro. Clin. Oral Investig. 2020, 24, 2745–2754. [Google Scholar] [CrossRef] [PubMed]
- Alothman, Y.; Bamasoud, M.S. The success of dental veneers according to preparation design and material type. Open Access Maced. J. Med. Sci. 2018, 12, 2402–2408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.; Gai, K.; Chen, J.; Jiang, L. Comparison of failure and complication risks of porcelain laminate and indirect resin veneer restorations: A meta-analysis. Int. J. Prosthodont. 2019, 32, 59–65. [Google Scholar] [CrossRef] [PubMed]
- The Academy of Prosthodontics. The Glossary of Prosthodontic Terms: Ninth Edition. J. Prosthet. Dent. 2017, 117, e1–e105. [Google Scholar] [CrossRef] [Green Version]
- Zarone, F.; Di Mauro, M.I.; Ausiello, P.; Ruggiero, G.; Sorrentino, R. Current status on lithium disilicate and zirconia: A narrative review. BMC Oral Health 2019, 19, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saker, S.; Özcan, M. Marginal discrepancy and load to fracture of monolithic zirconia laminate veneers: The effect of preparation design and sintering protocol. Dent. Mater. J. 2021, 40, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Zarone, F.; Ruggiero, G.; Leone, R.; Breschi, L.; Leuci, S.; Sorrentino, R. Zirconia-reinforced lithium silicate (ZLS) mechanical and biological properties: A literature review. J. Dent. 2021, 109, 103661. [Google Scholar] [CrossRef] [PubMed]
- Lo Muzio, L.; Bucci, P.; Carile, F.; Riccitiello, F.; Scotti, C.; Coccia, E.; Rappelli, G. Prosthetic rehabilitation of a child affected from anhydrotic ectodermal dysplasia: A case report. J. Contemp. Dent. Pract. 2005, 6, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Zarone, F.; Leone, R.; Di Mauro, M.I.; Ferrari, M.; Sorrentino, R. No-preparation ceramic veneers: A systematic review. J. Osseointegr. 2018, 10, 17–22. [Google Scholar] [CrossRef]
- Malcmacher, L. No-preparation porcelain veneers-back to the future! Dent. Today 2005, 24, 86–91. [Google Scholar]
- Strassler, H.E. Minimally invasive porcelain veneers: Indications for a conservative esthetic dentistry treatment modality. Gen. Dent. 2007, 55, 68694. [Google Scholar]
- Cherukara, G.P.; Davis, G.R.; Seymour, K.G.; Zou, L.; Samarawickrama, D.Y. Dentin exposure in tooth preparations for porcelain veneers: A pilot study. J. Prosthet. Dent. 2005, 94, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Peumans, M.; Van Meerbeek, B.; Lambrechts, P.; Vanherle, G. Porcelain veneers: A review of the literature. J. Dent. 2000, 28, 163–177. [Google Scholar] [CrossRef]
- Burke, F.J. Survival rates for porcelain laminate veneers with special reference to the effect of preparation in dentin: A literature review. J. Esthet. Restor. Dent. 2012, 24, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Shetty, A.; Kaiwar, A.; Shubhashini, N.; Ashwini, P.; Naveen, D.; Adarsha, M.; Shetty, M.; Meena, N. Survival rates of porcelain laminate restoration based on different incisal preparation designs: An analysis. J. Conserv. Dent. 2011, 14, 10–15. [Google Scholar] [CrossRef] [Green Version]
- Chai, S.Y.; Bennani, V.; Aarts, J.M.; Lyons, K. Incisal preparation design for ceramic veneers: A critical review. J. Am. Dent. Assoc. 2018, 149, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Albanesi, R.B.; Pigozzo, M.N.; Sesma, N.; Laganá, D.C.; Morimoto, S. Incisal coverage or not in ceramic laminate veneers: A systematic review and meta-analysis. J. Dent. 2016, 52, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hong, N.; Yang, H.; Li, J.; Wu, S.; Li, Y. Effect of preparation designs on the prognosis of porcelain laminate veneers: A systematic review and meta-analysis. Oper. Dent. 2017, 42, E197–E213. [Google Scholar] [CrossRef] [PubMed]
- da Costa, D.C.; Coutinho, M.; de Sousa, A.S.; Ennes, J.P. A meta-analysis of the most indicated preparation design for porcelain laminate veneers. J. Adhes. Dent. 2013, 15, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Zarone, F.; Epifania, E.; Leone, G.; Sorrentino, R.; Ferrari, M. Dynamometric assessment of the mechanical resistance of porcelain veneers related to tooth preparation: A comparison between two techniques. J. Prosthet. Dent. 2006, 95, 354–363. [Google Scholar] [CrossRef]
- Ferrari, M.; Patroni, S.; Balleri, P. Measurement of enamel thickness in relation to reduction for etched laminate veneers. Int. J. Periodontics Restor. Dent. 1992, 12, 407–413. [Google Scholar]
- Gresnigt, M.M.M.; Cune, M.S.; Schuitemaker, J.; van der Made, S.A.M.; Meisberger, E.W.; Magne, P.; Özcan, M. Performance of ceramic laminate veneers with immediate dentine sealing: An 11 year prospective clinical trial. Dent. Mater. 2019, 35, 1042–1052. [Google Scholar] [CrossRef] [PubMed]
- Gurel, G.; Morimoto, S.; Calamita, M.A.; Coachman, C.; Sesma, N. Clinical performance of porcelain laminate veneers: Outcomes of the aesthetic pre-evaluative temporary (APT) technique. Int. J. Periodontics Restor. Dent. 2012, 32, 625–635. [Google Scholar]
- Hegde, R.; Hegde, V. Magnification-enhanced contemporary dentistry: Getting started. J. Interdiscip. Dent. 2016, 6, 91–100. [Google Scholar] [CrossRef]
- Nelson, S.; Ash, M.M. Wheeler’s Dental Anatomy, Physiology, and Occlusion, 9th ed.; Saunders Elsevier: St. Luis, MO, USA, 2009; p. 13. [Google Scholar]
- Schneider, H.; Park, K.J.; Häfer, M.; Rüger, C.; Schmalz, G.; Krause, F.; Schmidt, J.; Ziebolz, D.; Haak, R. Dental applications of optical coherence tomography (OCT) in cariology. Appl. Sci. 2017, 7, 472. [Google Scholar] [CrossRef] [Green Version]
- Wilmers, J.; Bargmann, S. Nature’s design solutions in dental enamel: Uniting high strength and extreme damage resistance. Acta Biomater. 2020, 107, 1–24. [Google Scholar] [CrossRef]
- Ohazama, A. Histological analysis of the embryonic and adult tooth. Methods Mol. Biol. 2012, 887, 1–13. [Google Scholar]
- Hoffmann, L.; Feraric, M.; Hoster, E.; Litzenburger, F.; Kunzelmann, K.H. Investigations of the optical properties of enamel and dentin for early caries detection. Clin. Oral Investig. 2021, 25, 1281–1289. [Google Scholar] [CrossRef] [PubMed]
- Shillingburg, H.T.J.; Sather, D.A.; Wilson, E.L.J.; Cain, J.R.; Mitchell, D.L.; Blanco, L.J.; Kessler, J.C. Fundamentals of Fixed Prosthodontics, 4th ed.; Quintessence Publishing: Hanover Park, IL, USA, 2014; p. 422. [Google Scholar]
- Morimoto, S.; Albanesi, R.B.; Sesma, N.; Agra, C.M.; Braga, M.M. Main of feldspathic porcelain and glass-ceramic laminate veneers: A systematic review and meta-analysis of survival and complication rates. Int. J. Prosthodont. 2016, 29, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Beier, U.S.; Kapferer, I.; Burtscher, D.; Dumfahrt, H. Clinical performance of porcelain laminate veneers for up to 20 years. Int. J. Prosthodont. 2012, 25, 79–85. [Google Scholar] [PubMed]
- Petridis, H.P.; Zekeridou, A.; Malliari, M.; Tortopidis, D.; Koidis, P. Survival of ceramic veneers made of different materials after a minimum follow-up period of five years: A systematic review and meta-analysis. Eur. J. Esthet. Dent. 2012, 7, 138–152. [Google Scholar] [PubMed]
- Layton, D.M.; Walton, T.R. The up to 21-year clinical outcome and survival of feldspathic porcelain veneers: Accounting for clustering. Int. J. Prosthodont. 2012, 25, 604–612. [Google Scholar] [PubMed]
- Perillo, L.; Sorrentino, R.; Apicella, D.; Quaranta, A.; Gherlone, E.; Zarone, F.; Ferrari, M.; Aversa, R.; Apicella, A. Nonlinear visco-elastic finite element analysis of porcelain veneers: A submodelling approach to strain and stress distributions in adhesive and resin cement. J. Adhes. Dent. 2010, 12, 403–413. [Google Scholar] [PubMed]
- Sorrentino, R.; Apicella, D.; Riccio, C.; Gherlone, E.; Zarone, F.; Aversa, R.; Garcia Godoy, F.; Ferrari, M.; Apicella, A. Nonlinear visco-elastic finite element analysis of different porcelain veneers configuration. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 91, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Layton, D.; Walton, T. An up to 16-year prospective study of 304 porcelain veneers. Int. J. Prosthodont. 2007, 20, 389–396. [Google Scholar] [PubMed]
- Zhu, J.; Gao, J.; Jia, L.; Tan, X.; Xie, C.; Yu, H. Shear bond strength of ceramic laminate veneers to finishing surfaces with different percentages of preserved enamel under a digital guided method. BMC Oral Health 2022, 22, 3. [Google Scholar] [CrossRef] [PubMed]
- Gresnigt, M.M.M.; Braeckmans, A.; van der Made, S.A.M.; Naves, L.Z. Partial anterior indirect restorations in cases with dentin exposure. Int. J. Esthet. Dent. 2021, 16, 554–569. [Google Scholar] [PubMed]
- Bud, M.; Jitaru, S.; Lucaciu, O.; Korkut, B.; Dumitrascu-Timis, L.; Ionescu, C.; Cimpean, S.; Delean, A. The advantages of the dental operative microscope in restorative dentistry. Med. Pharm. Rep. 2021, 94, 22–27. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Operators | Mean (%) | Standard Deviation | Lower-Upper Bound |
|---|---|---|---|
| ST/WI | 22.82 | 9.23 | 16.21–29.42 |
| ST/BJ | 28.99 | 15.45 | 17.93–40.04 |
| GP/WI | 58.05 | 21.58 | 42.61–73.49 |
| GP/BJ | 40.56 | 21.25 | 25.35–55.76 |
| PR/WI | 10.55 | 10.16 | 3.27–17.82 |
| PR/BJ | 23.42 | 9.56 | 16.58–30.26 |
| Operators | Mean (mm2) | Standard Deviation | Lower-Upper Bound |
|---|---|---|---|
| ST/WI | 16.44 | 7.19 | 11.29–21.58 |
| ST/BJ | 20.83 | 11.94 | 12.29–29.38 |
| GP/WI | 40.64 | 12.91 | 31.41–49.88 |
| GP/BJ | 28.32 | 14.78 | 17.74–38.89 |
| PR/WI | 7.63 | 7.86 | 2.01–13.25 |
| PR/BJ | 16.75 | 7.45 | 11.42–22.09 |
| Source | SS | df | MS | F | p |
|---|---|---|---|---|---|
| Corrected Model | 13,694.17 | 5 | 2738.83 | 11.43 | <0.001 |
| Intercept | 56,675.34 | 1 | 56,675.34 | 236.67 | <0.001 |
| Operator | 11,144.83 | 2 | 5572.41 | 23.27 | <0.001 |
| Preparation | 3.97 | 1 | 3.97 | 0.01 | 0.898 |
| Operator × Preparation | 2545.36 | 2 | 1272.68 | 5.31 | 0.008 |
| Error | 12,931.04 | 54 | 239.46 | ||
| Total | 83,300.56 | 60 | |||
| Corrected Total | 26,625.22 | 59 |
| Comparison | p |
|---|---|
| ST/WI-ST/BJ | 0.880 |
| GP/WI-GP/BJ | 0.475 |
| PR/WI-PR/BJ | 0.083 |
| ST/WI-GP/WI | 0.005 * |
| ST/WI-PR/WI | 0.099 |
| GP/WI-PR/WI | <0.001 * |
| ST/BJ-GP/BJ | 0.731 |
| ST/BJ-PR/BJ | 0.921 |
| GP/BJ-PR/BJ | 0.254 |
| ST-GP | <0.001 * |
| ST-PR | 0.277 |
| GP-PR | <0.001 * |
| Preparation Design | Advantages | Disadvantages |
|---|---|---|
| Window |
| |
| Butt joint |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorrentino, R.; Ruggiero, G.; Borelli, B.; Barlattani, A.; Zarone, F. Dentin Exposure after Tooth Preparation for Laminate Veneers: A Microscopical Analysis to Evaluate the Influence of Operators’ Expertise. Materials 2022, 15, 1763. https://doi.org/10.3390/ma15051763
Sorrentino R, Ruggiero G, Borelli B, Barlattani A, Zarone F. Dentin Exposure after Tooth Preparation for Laminate Veneers: A Microscopical Analysis to Evaluate the Influence of Operators’ Expertise. Materials. 2022; 15(5):1763. https://doi.org/10.3390/ma15051763
Chicago/Turabian StyleSorrentino, Roberto, Gennaro Ruggiero, Bruna Borelli, Alberta Barlattani, and Fernando Zarone. 2022. "Dentin Exposure after Tooth Preparation for Laminate Veneers: A Microscopical Analysis to Evaluate the Influence of Operators’ Expertise" Materials 15, no. 5: 1763. https://doi.org/10.3390/ma15051763
APA StyleSorrentino, R., Ruggiero, G., Borelli, B., Barlattani, A., & Zarone, F. (2022). Dentin Exposure after Tooth Preparation for Laminate Veneers: A Microscopical Analysis to Evaluate the Influence of Operators’ Expertise. Materials, 15(5), 1763. https://doi.org/10.3390/ma15051763