
Effect of Restorative Material on Mechanical Response of Provisional Endocrowns: A 3D—FEA Study

 ,
, 

Abstract
1. Introduction
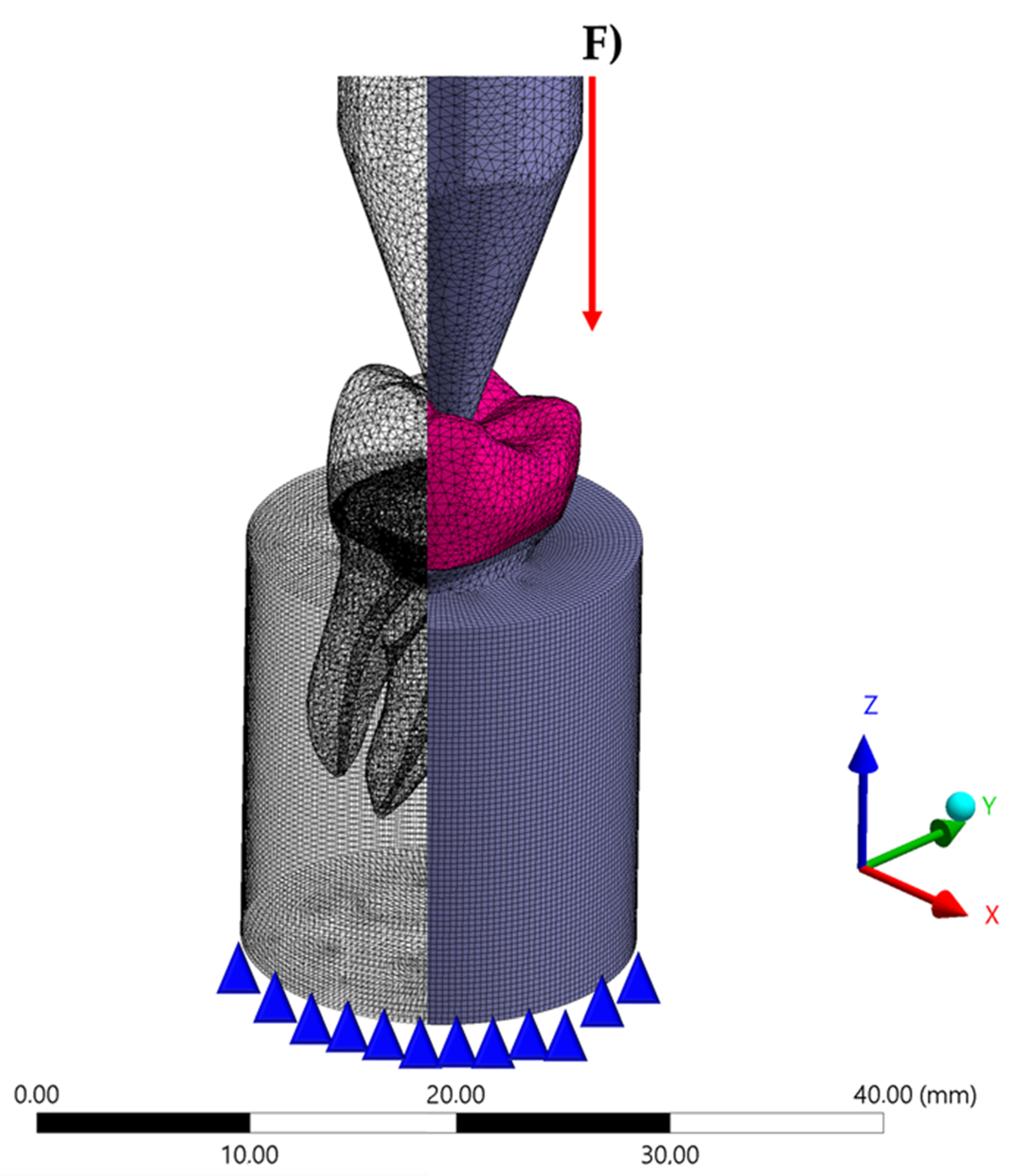
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Balkenhol, M.; Mautner, M.C.; Ferger, P.; Wöstmann, B. Mechanical properties of provisional crown and bridge materials: Chemical-curing versus dual-curing systems. J. Dent. 2008, 36, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Keys, W.F.; Keirby, N.; Ricketts, D.N.J. Provisional Restorations—A Permanent Problem? Dent. Update 2016, 43, 908–912. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.R.; Kim, S.H.; Lee, J.B.; Han, J.S. Improving shear bond strength of temporary crown and fixed dental prosthesis resins by surface treatments. J. Mater. Sci. 2016, 51, 1463–1475. [Google Scholar] [CrossRef]
- Revilla-León, M.; Meyers, M.J.; Zandinejad, A.; Özcan, M. A review on chemical composition, mechanical properties, and manufacturing work flow of additively manufactured current polymers for interim dental restorations. J. Esthet. Restor. Dent. 2019, 31, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Shibasaki, S.; Takamizawa, T.; Suzuki, T.; Nojiri, K.; Tsujimoto, A.; Barkmeier, W.W.; Latta, M.A.; Miyazaki, M. Influence of Different Curing Modes on Polymerization Behavior and Mechanical Properties of Dual-Cured Provisional Resins. Oper. Dent. 2017, 42, 526–536. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dal Piva, A.M.O.; de Jager, N.; Bottino, M.A.; de Kok, P.; Kleverlaan, C.J. Full-Crown Versus Endocrown Approach: A 3D-Analysis of Both Restorations and the Effect of Ferrule and Restoration Material. J. Prosthodont. 2020, 28. [Google Scholar] [CrossRef]
- Ghoul, W.E.; Özcan, M.; Tribst, J.P.M.; Salameh, Z. Fracture resistance, failure mode and stress concentration in a modified endocrown design. Biomater. Investig. Dent. 2020, 7, 110–119. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dal Piva, A.M.O.; Madruga, C.F.L.; Valera, M.C.; Borges, A.L.S.; Bresciani, E.; de Melo, R.M. Endocrown restorations: Influence of dental remnant and restorative material on stress distribution. Dent. Mater. 2018, 34, 1466–1473. [Google Scholar] [CrossRef]
- Da Fonseca, G.F.; Dal Piva, A.M.; Tribst, J.P.; Borges, A.L. Influence of Restoration Height and Masticatory Load Orientation on Ceramic Endocrowns. J. Contemp. Dent. Pract. 2018, 19, 1052–1057. [Google Scholar] [CrossRef]
- Da Fonseca, G.F.; de Andrade, G.S.; Dal Piva, A.M.O.; Tribst, J.P.M.; Borges, A.L.S. Computer-aided design finite element modeling of different approaches to rehabilitate endodontically treated teeth. J. Indian Prosthodont. Soc. 2018, 18, 329–335. [Google Scholar] [CrossRef]
- El Ghoul, W.A.; Özcan, M.; Ounsi, H.; Tohme, H.; Salameh, Z.J. Effect of different CAD-CAM materials on the marginal and internal adaptation of endocrown restorations: An in vitro study. J. Prosthet. Dent. 2020, 123, 128–134. [Google Scholar] [CrossRef] [PubMed]
- El Ghoul, W.; Özcan, M.; Silwadi, M.; Salameh, Z. Fracture resistance and failure modes of endocrowns manufactured with different CAD/CAM materials under axial and lateral loading. J. Esthet. Restor. Dent. 2019, 31, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Gresnigt, M.M.; Özcan, M.; van den Houten, M.L.; Schipper, L.; Cune, M.S. Fracture strength, failure type and Weibull characteristics of lithium disilicate and multiphase resin composite endocrowns under axial and lateral forces. Dent. Mater. 2016, 32, 607–614. [Google Scholar] [CrossRef]
- Tribst, J.P.; Dal Piva, A.O.; Madruga, C.F.; Valera, M.C.; Bresciani, E.; Bottino, M.A.; de Melo, R.M. The impact of restorative material and ceramic thickness on CAD\CAM endocrowns. J. Clin. Exp. Dent. 2019, 11, 969–977. [Google Scholar] [CrossRef] [PubMed]
- Dogui, H.; Abdelmalek, F.; Amor, A.; Douki, N. Endocrown: An Alternative Approach for Restoring Endodontically Treated Molars with Large Coronal Destruction. Case. Rep. Dent. 2018, 1581952. [Google Scholar] [CrossRef]
- Irmaleny, Z.; Sholeh, A.; Mardiyah, A.; Agustin, D. Endocrown Restoration on Postendodontics Treatment on Lower First Molar. J. Int. Soc. Prev. Community Dent. 2019, 9, 303–310. [Google Scholar]
- Taha, D.; Abu-Elfadl, A.; Morsi, T. Minimally invasive prosthodontic correction of pseudo class III malocclusion by implementing a systematic digital workflow: A clinical report. J. Prosthet. Dent. 2021, 125, 8–14. [Google Scholar] [CrossRef]
- Dejak, B.; Młotkowski, A. A comparison of mvM stress of inlays, onlays and endocrowns made from various materials and their bonding with molars in a computer simulation of mastication—FEA. Dent. Mater. 2020, 36, 854–864. [Google Scholar] [CrossRef]
- Helal, M.A.; Wang, Z. Biomechanical Assessment of Restored Mandibular Molar by Endocrown in Comparison to a Glass Fiber Post-Retained Conventional Crown: 3D Finite Element Analysis. J. Prosthodont. 2019, 28, 988–996. [Google Scholar] [CrossRef] [PubMed]
- Dureja, I.; Yadav, B.; Malhotra, P.; Dabas, N.; Bhargava, A.; Pahwa, R. A comparative evaluation of vertical marginal fit of provisional crowns fabricated by computer-aided design/computer-aided manufacturing technique and direct (intraoral technique) and flexural strength of the materials: An in vitro study. J. Indian Prosthodont. Soc. 2018, 18, 314–320. [Google Scholar] [CrossRef]
- Li, X.; Kang, T.; Zhan, D.; Xie, J.; Guo, L. Biomechanical behavior of endocrowns vs fiber post-core-crown vs cast post-core-crown for the restoration of maxillary central incisors with 1 mm and 2 mm ferrule height: A 3D static linear finite element analysis. Medicine (Baltimore). 2020, 99, e22648. [Google Scholar] [CrossRef] [PubMed]
- Ausiello, P.; Ciaramella, S.; De Benedictis, A.; Lanzotti, A.; Tribst, J.P.M.; Watts, D.C. The use of different adhesive filling material and mass combinations to restore class II cavities under loading and shrinkage effects: A 3D-FEA. Comput. Methods Biomech. Biomed. Eng. 2020, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, B.; Devi, N.N.; Gupta, N.; Singh, R. Comparative Evaluation of Various Temperature Changes on Stress Distribution in Class II Mesial-occlusal-distal Preparation restored with Different Restorative Materials: A Finite Element Analysis. Int. J. Clin. Pediatr. Dent. 2018, 11, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.M.; Kelly, A.; Tagiyeva, N.; Kanagasingam, S. Comparing endocrown restorations on permanent molars and premolars: A systematic review and meta-analysis. Br. Dent. J. 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Belleflamme, M.M.; Geerts, S.O.; Louwette, M.M.; Grenade, C.F.; Vanheusden, A.J.; Mainjot, A.K. No post-no core approach to restore severely damaged posterior teeth: An up to 10-year retrospective study of documented endocrown cases. J. Dent. 2017, 63, 1–7. [Google Scholar] [CrossRef]
- Hollanders, A.C.C.; Kuper, N.K.; Huysmans, M.C.D.N.J.M.; Versluis, A. The effect of occlusal loading on cervical gap deformation: A 3D finite element analysis. Dent. Mater. 2020, 36, 681–686. [Google Scholar] [CrossRef]
- Naqash, T.A.; Alfarsi, M.; Hussain, M.W. Marginal accuracy of provisional crowns using three material systems and two techniques: A scanning electron microscope study. Pak. J. Med. Sci. 2019, 35, 55–60. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhao, Y.P. Adhesive Contact of Nanowire in Three-Point Bending Test. J. Adhes. Sci. Technol. 2011, 10, 1107–1129. [Google Scholar] [CrossRef]
- Haralur, S.B.; Alamrey, A.A.; Alshehri, S.A.; Alzahrani, D.S.; Alfarsi, M. Effect of different preparation designs and all ceramic materials on fracture strength of molar endocrowns. J. Appl. Biomater. Funct. Mater. 2020, 18. [Google Scholar] [CrossRef]
- Lin, J.; Lin, Z.; Zheng, Z. Effect of different restorative crown design and materials on stress distribution in endodontically treated molars: A finite element analysis study. BMC. Oral. Health 2020, 18, 226. [Google Scholar] [CrossRef]
- Govare, N.; Contrepois, M. Endocrowns: A systematic review. J. Prosthet. Dent. 2020, 123, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Wang, D.; Rong, Q.; Qian, J.; Wang, X. Effect of central retainer shape and abduction angle during preparation of teeth on dentin and cement layer stress distributions in endocrown-restored mandibular molars. Dent. Mater. J. 2020, 5, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Eskitaşçioğlu, M.; Küçük, O.; Eskitaşçioğlu, G.; Eraslan, O.; Belli, S. The Effect of Different Materials and Techniques on Stress Distribution in CAD/CAM Endocrowns. Strength Mater. 2020, 52, 812–819. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Kani, R.; Kawakami, K.; Tsuji, M.; Inoue, S.; Lee, C.; Kiba, W.; Imazato, S. Fatigue behavior and crack initiation of CAD/CAM resin composite molar crowns. Dent. Mater. 2018, 34, 1578–1584. [Google Scholar] [CrossRef] [PubMed]
- Penteado, M.M.; Tribst, J.P.M.; Dal Piva, A.M.; Ausiello, P.; Zarone, F.; Garcia-Godoy, F.; Borges, A.L. Mechanical behavior of conceptual posterior dental crowns with functional elasticity gradient. Am. J. Dent. 2019, 32, 165–168. [Google Scholar]
- Zimmermann, M.; Valcanaia, A.; Neiva, G.; Mehl, A.; Fasbinder, D. Three-Dimensional Digital Evaluation of the Fit of Endocrowns Fabricated from Different CAD/CAM Materials. J. Prosthodont. 2019, 28, 504–509. [Google Scholar] [CrossRef]
- Zheng, Z.; He, Y.; Ruan, W.; Ling, Z.; Zheng, C.; Gai, Y.; Yan, W. Biomechanical behavior of endocrown restorations with different CAD-CAM materials: A 3D finite element and in vitro analysis. J. Prosthet. Dent. 2020, 26. [Google Scholar] [CrossRef]
- Al-Dabbagh, R.A. Survival and success of endocrowns: A systematic review and meta-analysis. J. Prosthet. Dent. 2020, 17. [Google Scholar] [CrossRef]
- Biacchi, G.R.; Mello, B.; Basting, R.T. The endocrown: An alternative approach for restoring extensively damaged molars. J. Esthet. Restor. Dent. 2013, 25, 383–390. [Google Scholar] [CrossRef]
- Madhavan, S.; Jude, S.M.; Achammada, S.; Ullattuthodi, S.; Kuriachan, T.; Jacob, J. Comparison of Marginal Accuracy of Interim Restoration Fabricated from Self-cure Composite and Autopolymerizing Acrylic Resin: An In Vitro Study. J. Pharm. Bioallied Sci. 2020, 12, S361–S366. [Google Scholar] [CrossRef]
- Miura, S.; Fujisawa, M.; Komine, F.; Maseki, T.; Ogawa, T.; Takebe, J.; Nara, Y. Importance of interim restorations in the molar region. J. Oral Sci. 2019, 18, 195–199. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material/Structure | Composition | Elastic Modulus (GPa) * | Poisson Ratio | Reference |
|---|---|---|---|---|
| Enamel | - | 80 | 0.30 | [22] |
| Dentin | - | 18 | 0.23 | [22] |
| Fixation cylinder | Polyurethane resin | 3.6 | 0.30 | [5] |
| Temporary cement | Zinc oxide-based cement | 1.35 | 0.30 | [23] |
| Acrylic resin | Polymethyl methacrylate, diethyl phthalate, benzoyl peroxide, titanium dioxide. | 2.2 | 0.30 | [5] |
| Bis-acrylic resin | UDMA, bis-GMA, benzoyl peroxide, Amine and fillers. | 2.9 | 0.30 | [5] |
| Resin composite | UDMA, bis-GMA, bis-EMA, TEGDMA, Silica and fillers. | 8.0 | 0.25 | [22] |
| Acrylic Resin | Bis-Acrylic Resin | Resin Composite | |
|---|---|---|---|
| Tensile stress in the endocrown | 9.6 | 9.7 | 10.1 |
| Shear stress in the endocrown | 4.2 | 4.3 | 4.7 |
| Tensile stress in the cement layer | 8.9 | 8.8 | 3.4 |
| Shear stress in the cement layer | 9.2 | 9.0 | 7.5 |
| Tensile stress in the enamel tissue | 16.5 | 16.1 | 13.4 |
| Tensile stress in the dentin tissue | 15.9 | 15.2 | 9.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tribst, J.P.M.; Borges, A.L.S.; Silva-Concílio, L.R.; Bottino, M.A.; Özcan, M. Effect of Restorative Material on Mechanical Response of Provisional Endocrowns: A 3D—FEA Study. Materials 2021, 14, 649. https://doi.org/10.3390/ma14030649
Tribst JPM, Borges ALS, Silva-Concílio LR, Bottino MA, Özcan M. Effect of Restorative Material on Mechanical Response of Provisional Endocrowns: A 3D—FEA Study. Materials. 2021; 14(3):649. https://doi.org/10.3390/ma14030649
Chicago/Turabian StyleTribst, João Paulo Mendes, Alexandre Luiz Souto Borges, Laís Regiane Silva-Concílio, Marco Antonio Bottino, and Mutlu Özcan. 2021. "Effect of Restorative Material on Mechanical Response of Provisional Endocrowns: A 3D—FEA Study" Materials 14, no. 3: 649. https://doi.org/10.3390/ma14030649
APA StyleTribst, J. P. M., Borges, A. L. S., Silva-Concílio, L. R., Bottino, M. A., & Özcan, M. (2021). Effect of Restorative Material on Mechanical Response of Provisional Endocrowns: A 3D—FEA Study. Materials, 14(3), 649. https://doi.org/10.3390/ma14030649