
Accuracy of the Intra- and Extra-Oral Scanning Technique for Transferring the Intaglio Surface of a Pontic of Provisional Restorations to Definitive Restorations


Abstract
:1. Introduction
2. Materials and Methods
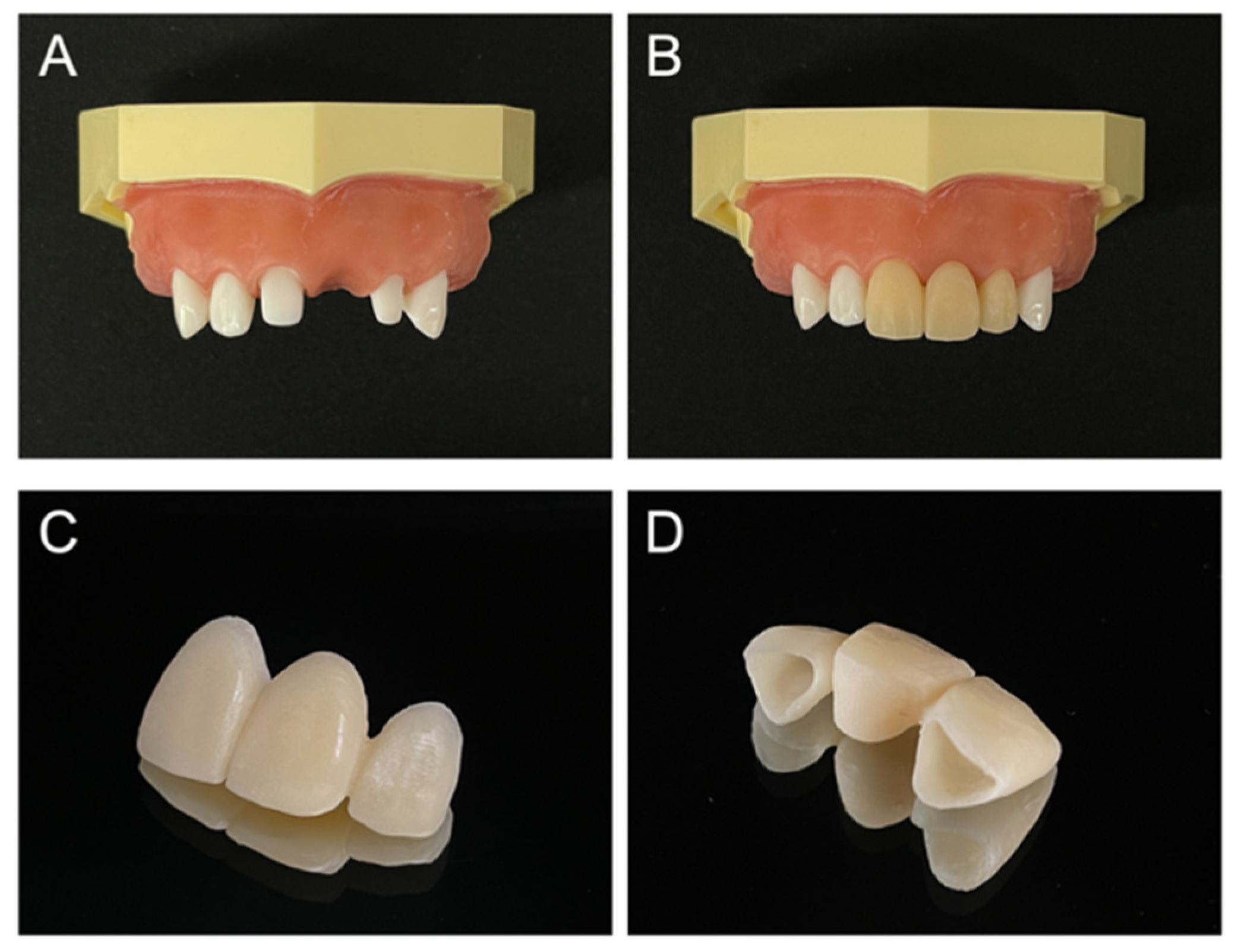
2.1. Conventional Impression Method
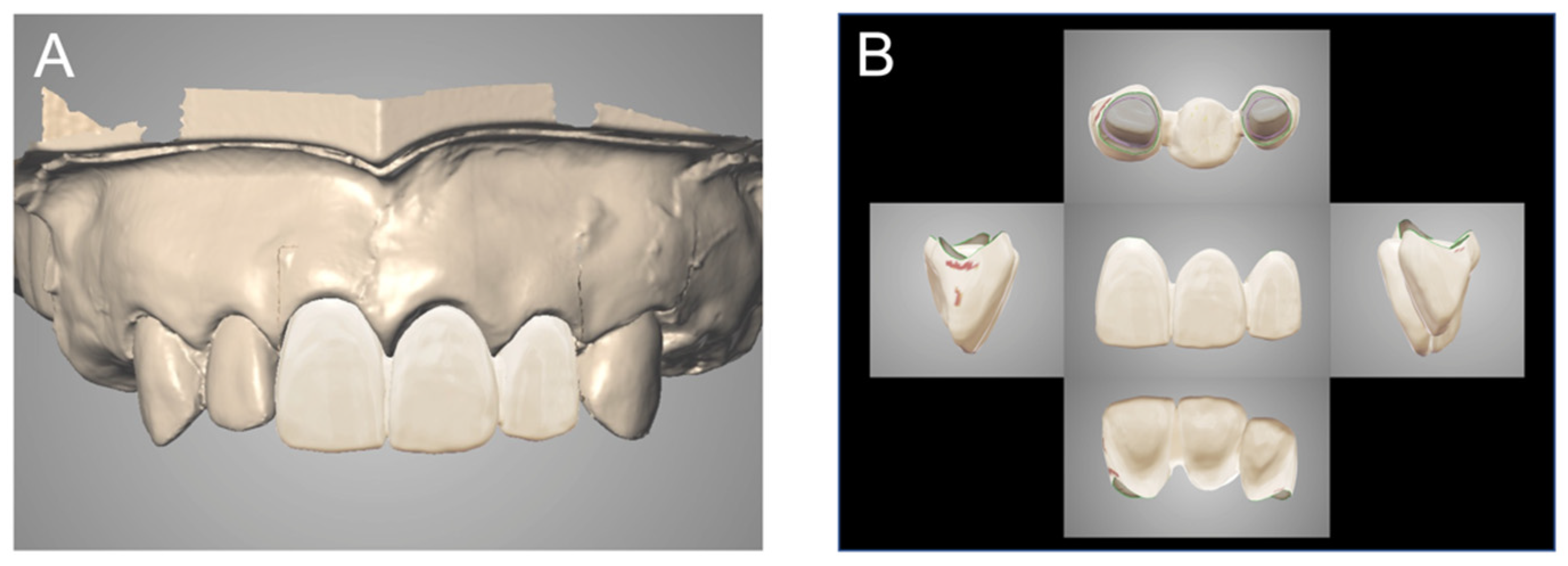
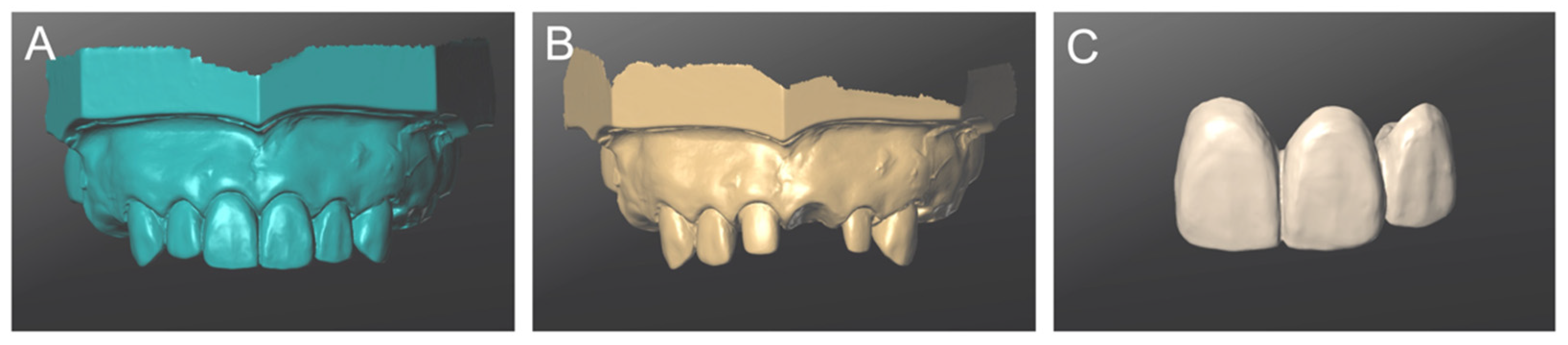
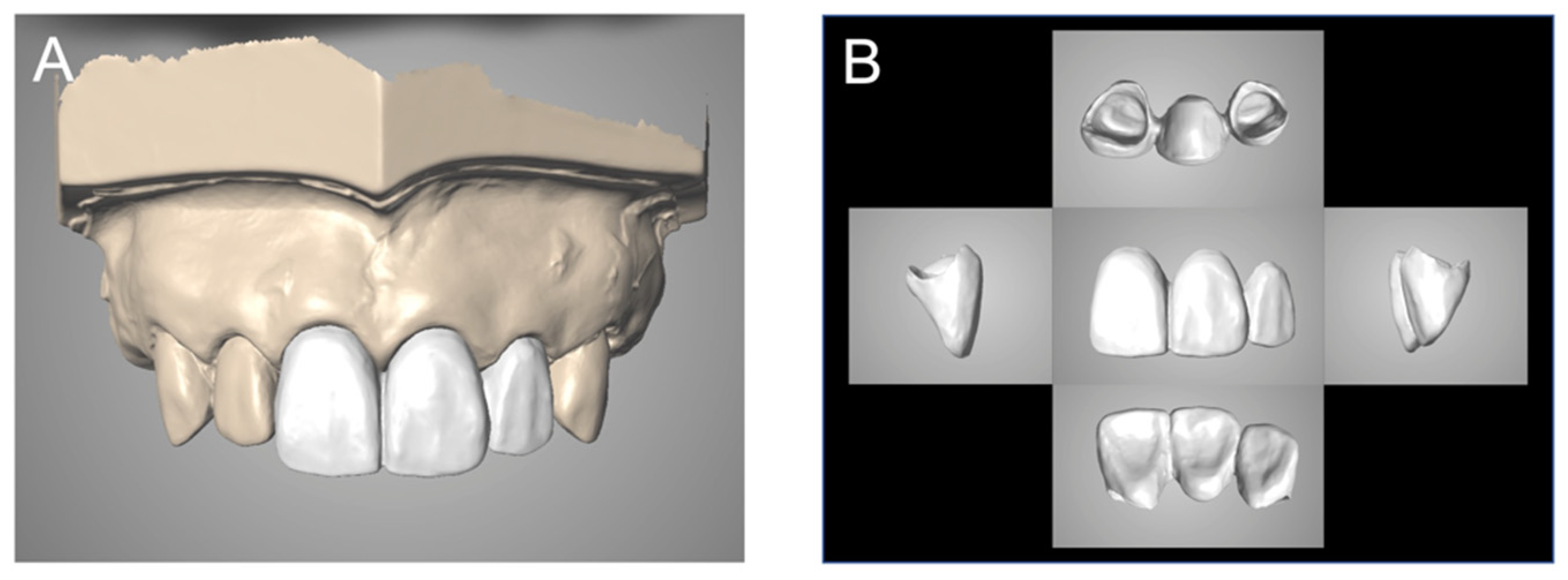
2.2. The IEOS Technique
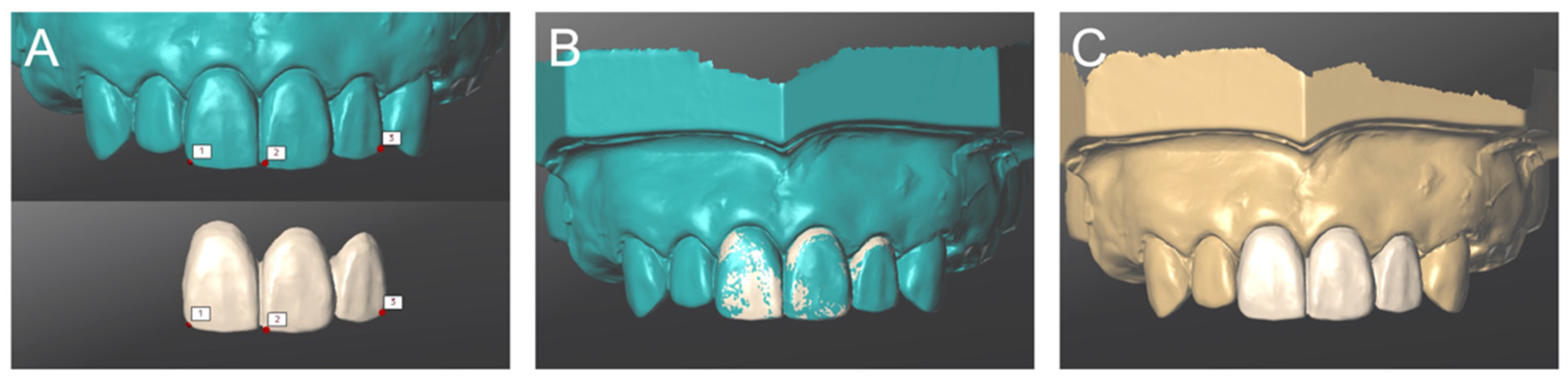
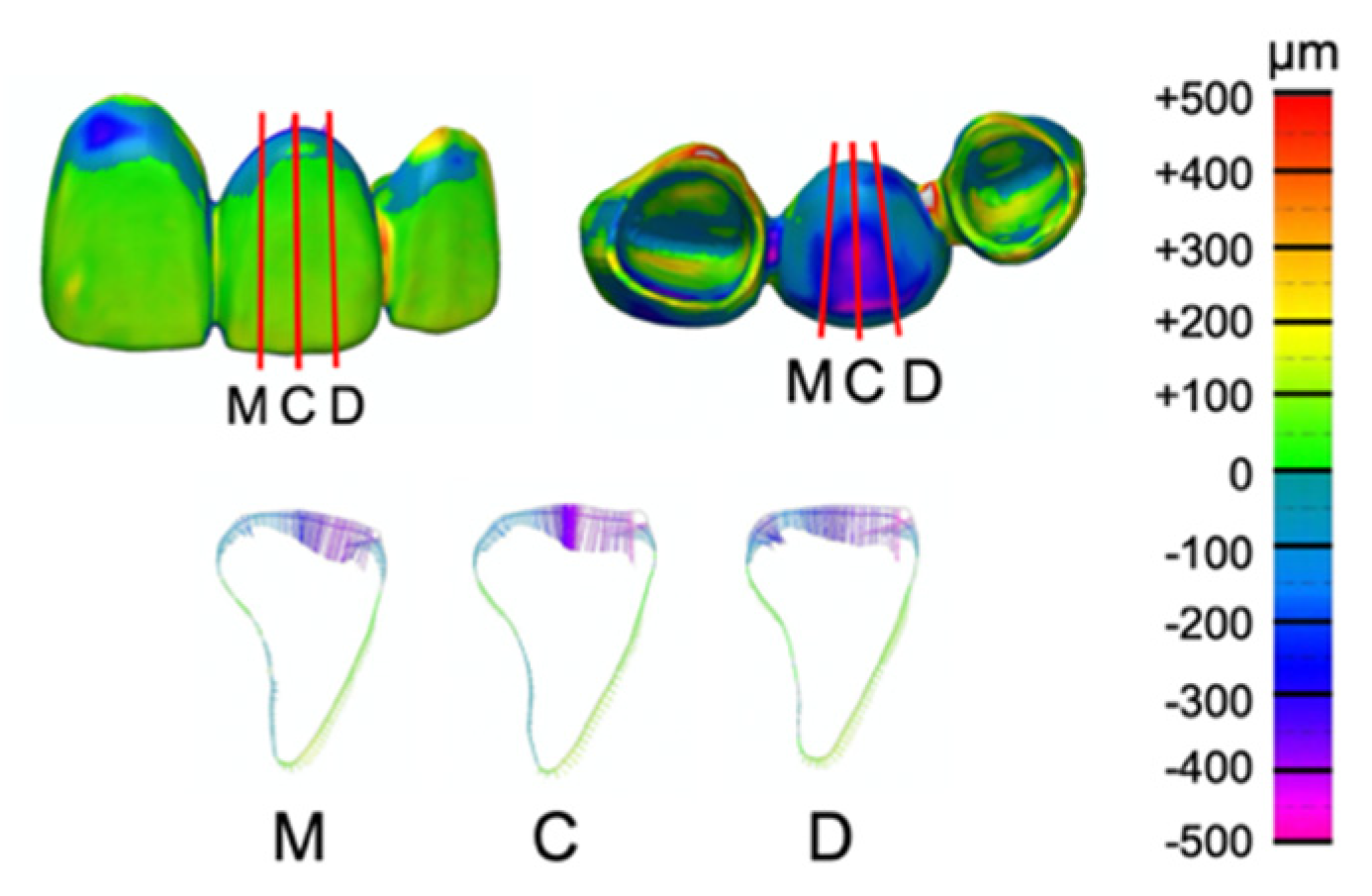
2.3. Measurement
2.4. Statistical Analysis
3. Results
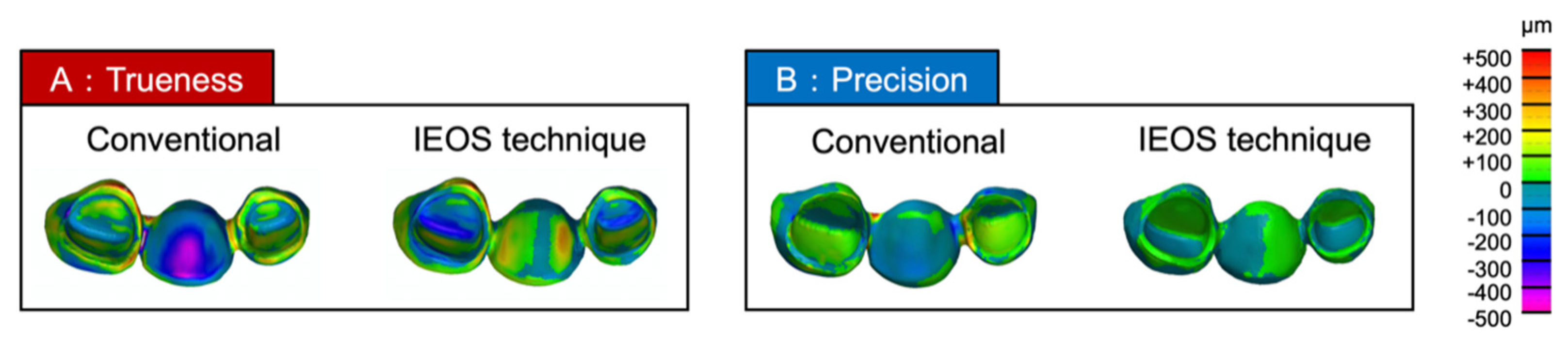
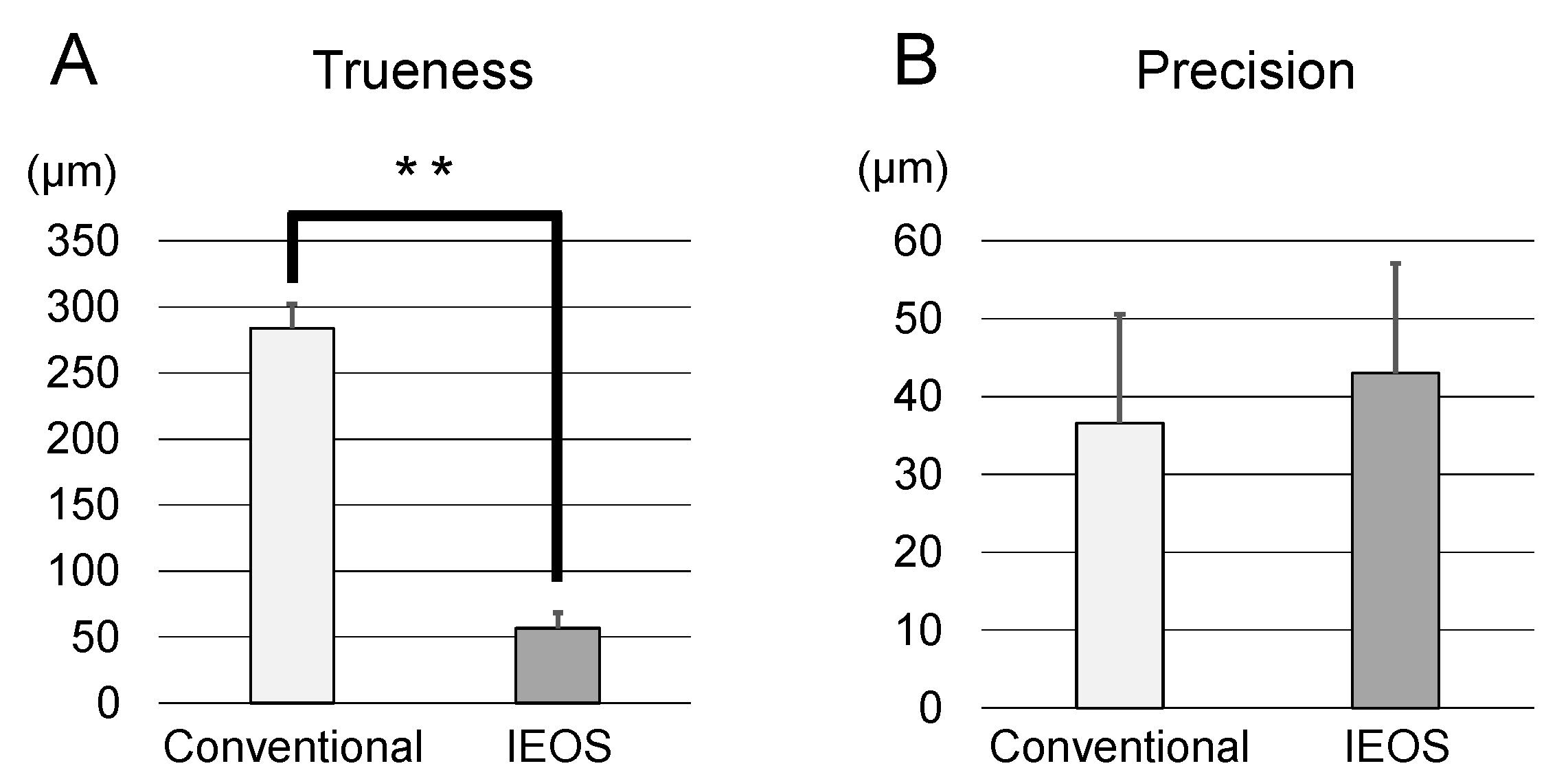
3.1. Trueness
3.2. Precision
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef] [Green Version]
- Koulivand, S.; Ghodsi, S.; Siadat, H.; Alikhasi, M. A clinical comparison of digital and conventional impression techniques regarding finish line locations and impression time. J. Esthet. Restor. Dent. 2020, 32, 236–243. [Google Scholar] [CrossRef]
- Del Corso, M.; Abà, G.; Vazquez, L.; Dargaud, J.; Ehrenfest, D.M.D. Optical three-dimensional scanning acquisition of the position of osseointegrated implants: An in vitro study to determine method accuracy and operational feasibility. Clin. Implant Dent. Relat. Res. 2009, 11, 214–221. [Google Scholar] [CrossRef]
- Ahlholm, P.; Sipilä, K.; Vallittu, P.; Jakonen, M.; Kotiranta, U. Digital versus conventional impressions in fixed prosthodontics: A review. J Prosthodont. 2018, 27, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Schepke, U.; Meijer, H.J.A.; Kerdijk, W.; Cune, M.S. Digital versus analog complete-arch impressions for single-unit premolar implant crowns: Operating time and patient preference. J. Prosthet. Dent. 2015, 114, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Flügge, T.V.; Schlager, S.; Nelson, K.; Nahles, S.; Metzger, M.C. Precision of intraoral digital dental impressions with iTero and extraoral digitization with the iTero and a model scanner. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, K.; Sachdeva, A.U.; Saitoh, S.; Lee, S.-P.; Kubota, T.; Mizoguchi, I. Assessment of the accuracy and reliability of new 3-dimensional scanning devices. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Anh, J.-W.; Park, J.-M.; Chun, Y.-S.; Kim, M.; Kim, M. A comparison of the precision of three-dimensional images acquired by 2 digital intraoral scanners: Effects of tooth irregularity and scanning direction. Korean J. Orthod. 2016, 46, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Wiranto, M.G.; Engelbrecht, W.P.; Tutein Nolthenius, H.E.; van der Meer, W.J.; Ren, Y. Validity, reliability, and reproduci-bility of linear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressions. Am. J. Orthod. Dentofacial. Orthop. 2013, 143, 140–147. [Google Scholar] [CrossRef]
- Ender, A.; Zimmermann, M.; Mehl, A. Accuracy of complete- and partial-arch impressions of actual intraoral scanning systems in vitro. Int. J. Comput. Dent. 2019, 22, 11–19. [Google Scholar] [PubMed]
- Kamimura, E.; Tanaka, S.; Takaba, M.; Tachi, K.; Baba, K. In vivo evaluation of inter-operator reproducibility of digital dental and conventional impression techniques. PLoS ONE 2017, 12, e0179188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, G.K.; Leary, J.M. Pontic design and localized ridge augmentation in fixed partial denture design. Dent. Clin. N. Am. 1992, 36, 591–605. [Google Scholar]
- Orsini, G.; Murmura, G.; Artese, L.; Piattelli, A.; Piccirilli, M.; Caputi, S. Tissue healing under provisional restorations with ovate pontics: A pilot human histological study. J. Prosthet. Dent. 2006, 96, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Su, T.-S.; Sun, J. Comparison of marginal and internal fit of 3-unit ceramic fixed dental prostheses made with either a conventional or digital impression. J. Prosthet. Dent. 2016, 116, 362–367. [Google Scholar] [CrossRef]
- Sasada, Y.; Huynh-Ba, G.; Funakoshi, E. Transferring subgingival contours around implants and the intaglio surface of the pontic to definitive digital casts by using an intraoral scanner: A technique. J. Prosthet. Dent. 2019, 123, 210–214. [Google Scholar] [CrossRef]
- Miyoshi, K.; Tanaka, S.; Yokoyama, S.; Sanda, M.; Baba, K. Effects of different types of intraoral scanners and scanning ranges on the precision of digital implant impressions in edentulous maxilla: An in vitro study. Clin. Oral Implant. Res. 2020, 31, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Son, K.; Lee, K.-B. Displacement of scan body during screw tightening: A comparative in vitro study. J. Adv. Prosthodont. 2020, 12, 307–315. [Google Scholar] [CrossRef]
- Lim, J.-H.; Park, J.-M.; Kim, M.; Heo, S.-J.; Myung, J.-Y. Comparison of digital intraoral scanner reproducibility and image trueness considering repetitive experience. J. Prosthet. Dent. 2018, 119, 225–232. [Google Scholar] [CrossRef]
- Güth, J.-F.; Keul, C.; Stimmelmayr, M.; Beuer, F.; Edelhoff, D. Accuracy of digital models obtained by direct and indirect data capturing. Clin. Oral Investig. 2013, 17, 1201–1208. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; Watzek, G. Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score. Clin. Oral Implant. Res. 2005, 16, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Belser, U.C.; Grütter, L.; Vailati, F.; Bornstein, M.M.; Weber, H.-P.; Buser, D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: A cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores. J. Periodontol. 2009, 80, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Khoury, F.; Happe, A.; Hoppe, A. Soft tissue management in oral implantology: A review of surgical techniques for shaping an esthetic and functional peri-implant soft tissue structure. Quintessence Int. 2001, 31, 483–499. [Google Scholar]
- Chee, W. Provisional restorations in soft tissue management around dental implants. Periodontol. 2000 2001, 27, 139–147. [Google Scholar] [CrossRef]
- Chen, S.; Liang, W.; Chen, F. Factors affecting the accuracy of elastometric impression materials. J. Dent. 2004, 32, 603–609. [Google Scholar] [CrossRef]
- Millstein, P. Determining the accuracy of gypsum casts made from type IV dental stone. J. Oral Rehabil. 1992, 19, 239–243. [Google Scholar] [CrossRef]
- Camardella, L.T.; Breuning, H.; Vilella, O. Accuracy and reproducibility of measurements on plaster models and digital models created using an intraoral scanner. J. Orofac. Orthop. Fortschr. Kieferorthopädie 2017, 78, 211–220. [Google Scholar] [CrossRef]
- Tomita, Y.; Uechi, J.; Konno, M.; Sasamoto, S.; Iijima, M.; Mizoguchi, I. Accuracy of digital models generated by conventional impression/plaster-model methods and intraoral scanning. Dent. Mater. J. 2018, 37, 628–633. [Google Scholar] [CrossRef] [Green Version]
- Seelbach, P.; Brueckel, C.; Wöstmann, B. Accuracy of digital and conventional impression techniques and workflow. Clin. Oral Investig. 2013, 17, 1759–1764. [Google Scholar] [CrossRef] [PubMed]
- Kaihara, Y.; Kihara, T.; Kakayama, A.; Amano, H.; Nikawa, H.; Kozai, K. Accuracy of a non-contact 3D measuring system for dental model analysis. Pediatr. Dent. J. 2013, 23, 71–78. [Google Scholar] [CrossRef]
- Bell, A.; Ayoub, A.F.; Siebert, P. Assessment of the accuracy of a three-dimensional imaging system for archiving dental study models. J. Orthod. 2003, 30, 219–223. [Google Scholar] [CrossRef]
- Nawafleh, N.A.; Mack, F.; Evans, J.L.; Mackay, J.; Hatamleh, M.M. Accuracy and reliability of methods to measure marginal adaptation of crowns and FDPs: A literature review. J. Prosthodont. 2013, 22, 419–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, P.; Ender, A.; Joda, T.; Katsoulis, J. Impact of digital intraoral scan strategies on the impression accuracy using the TRIOS Pod scanner. Quintessence Int. 2016, 47, 343–349. [Google Scholar] [PubMed]
- Arakida, T.; Kanazawa, M.; Iwaki, M.; Suzuki, T.; Minakuchi, S. Evaluating the influence of ambient light on scanning trueness, precision, and time of intra oral scanner. J. Prosthodont. Res. 2018, 62, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Ting-Shu, S.; Jian, S. Intraoral digital impression technique: A review. J. Prosthodont. 2015, 24, 313–321. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Accuracy | Mean ± SD | p-Value | |
|---|---|---|---|
| Conventional Method | IEOS Technique | ||
| Trueness | 283.9 ± 19 μm | 56.6 ± 12 μm | <0.001 ** |
| Precision | 36.6 ± 14 μm | 43.0 ± 14 μm | 0.32 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanda, K.; Yasunami, N.; Okada, M.; Furuhashi, A.; Ayukawa, Y. Accuracy of the Intra- and Extra-Oral Scanning Technique for Transferring the Intaglio Surface of a Pontic of Provisional Restorations to Definitive Restorations. Materials 2021, 14, 6489. https://doi.org/10.3390/ma14216489
Sanda K, Yasunami N, Okada M, Furuhashi A, Ayukawa Y. Accuracy of the Intra- and Extra-Oral Scanning Technique for Transferring the Intaglio Surface of a Pontic of Provisional Restorations to Definitive Restorations. Materials. 2021; 14(21):6489. https://doi.org/10.3390/ma14216489
Chicago/Turabian StyleSanda, Koma, Noriyuki Yasunami, Maki Okada, Akihiro Furuhashi, and Yasunori Ayukawa. 2021. "Accuracy of the Intra- and Extra-Oral Scanning Technique for Transferring the Intaglio Surface of a Pontic of Provisional Restorations to Definitive Restorations" Materials 14, no. 21: 6489. https://doi.org/10.3390/ma14216489
APA StyleSanda, K., Yasunami, N., Okada, M., Furuhashi, A., & Ayukawa, Y. (2021). Accuracy of the Intra- and Extra-Oral Scanning Technique for Transferring the Intaglio Surface of a Pontic of Provisional Restorations to Definitive Restorations. Materials, 14(21), 6489. https://doi.org/10.3390/ma14216489