
Performance of a Piezoelectric Energy Harvesting System for an Energy-Autonomous Instrumented Total Hip Replacement: Experimental and Numerical Evaluation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Finite Elemente Analysis
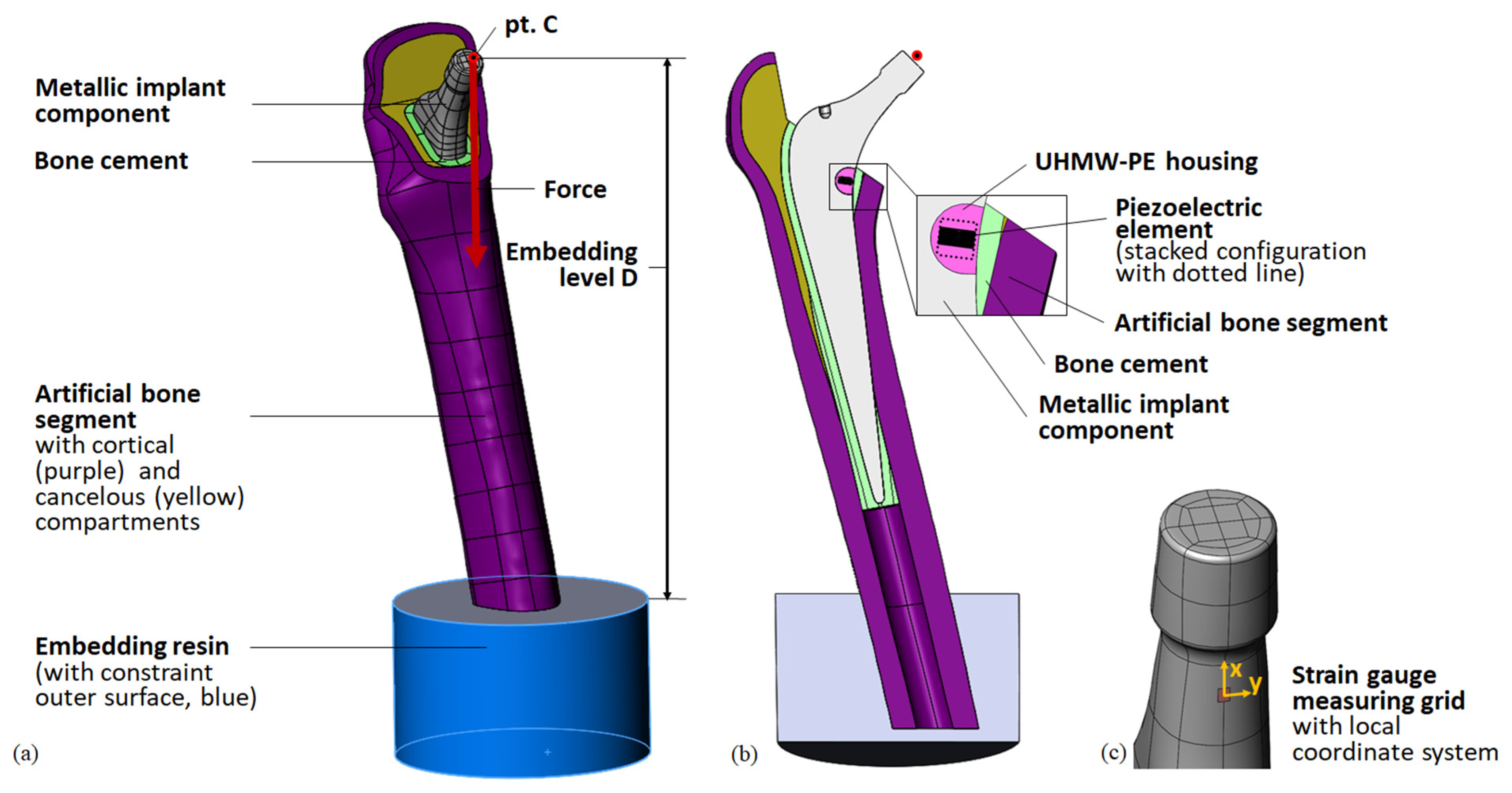
2.1.1. Geometry
2.1.2. Loads and Boundary Conditions
2.1.3. Meshing
2.1.4. Material Properties
2.1.5. Analysis Settings and Hardware
2.1.6. Post-Processing and Output Parameters
- maximum von Mises stress in the implant cavity σimp,
- maximum von Mises stress in the piezoelectric element’s midplane cross-section σpiez (i.e., for the stacked configuration, the higher stress value of the two midplanes of the two single elements),
- contact force F33 acting on the piezoelectric element’s end faces in the direction of its cylinder axis,
- generated open-circuit voltage VOC, and
- total displacement of point C .
2.1.7. FEA Studies
Iterative Study for the Reproduction of Previous Results in the New Setup
Sensitivity Analysis
- geometrical changes
- ○
- resection level of the bone (distance to energy harvesting system); –1, +1, +2 mm
- ○
- thickness of the bone cement layer; ±1 mm
- ○
- embedding level D; ±3 mm
- ○
- alignment of the femoral bone segment; ±5° rotation in the implants’ medio-lateral plane and antero-posterior plane
- scaled material properties (±10% Young’s moduli for artificial bone, bone cement, housing and metallic total hip stem).
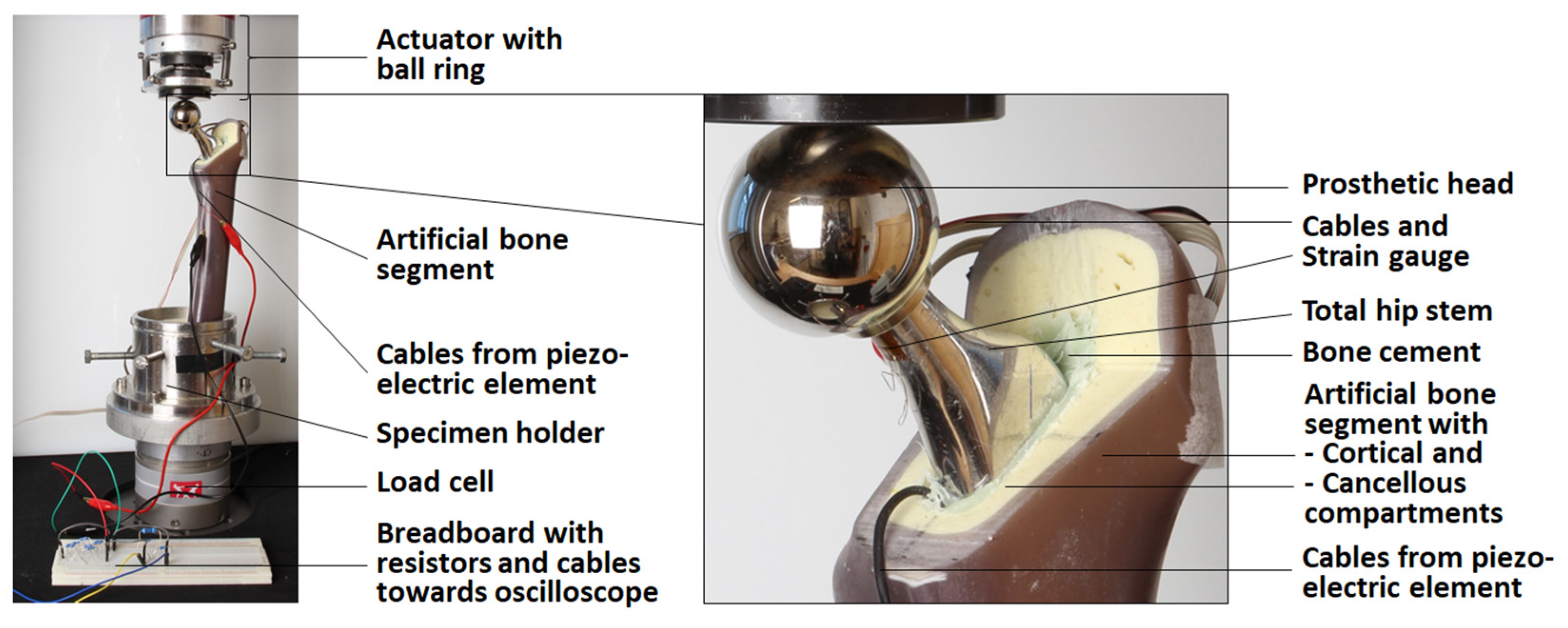
2.2. Experimental Testing
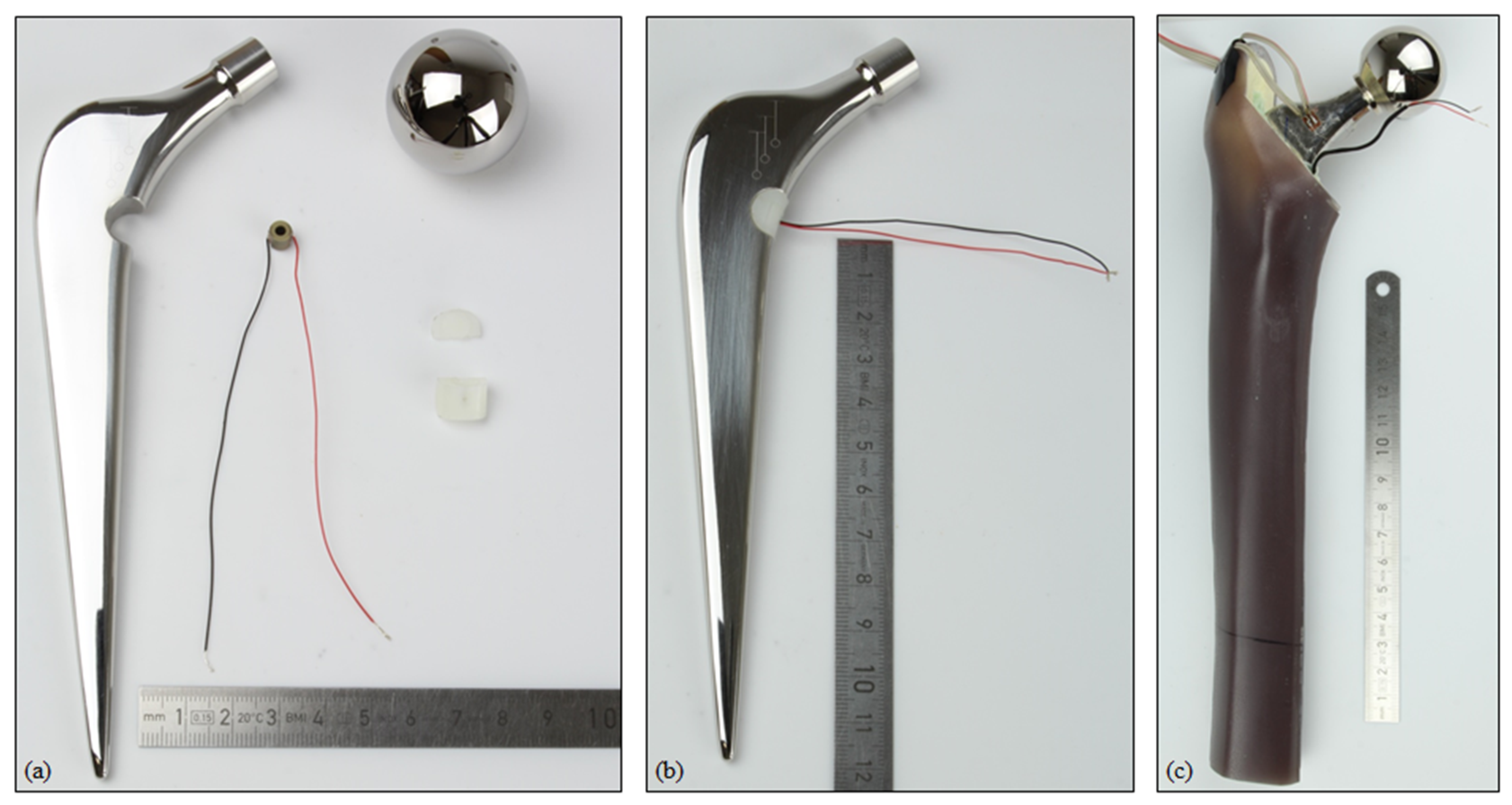
2.2.1. Sample Preparation
2.2.2. Quasi-Static Testing for Model Validation
2.2.3. Mechanical Testing
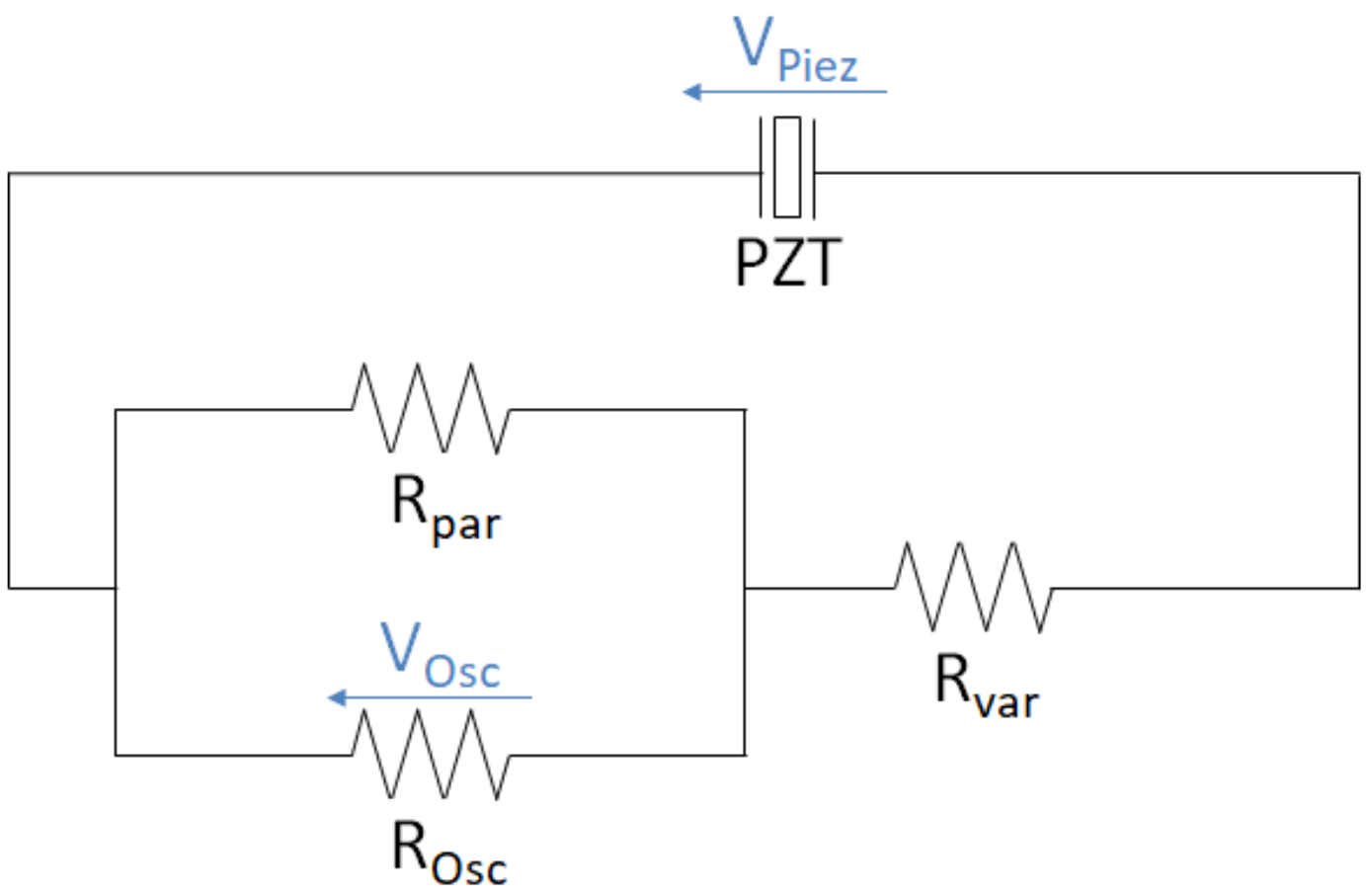
2.2.4. Testing of the Piezoelectric Element
3. Results
3.1. Results of Finite Element Analysis: Deformation, Loading, and Sensitivity
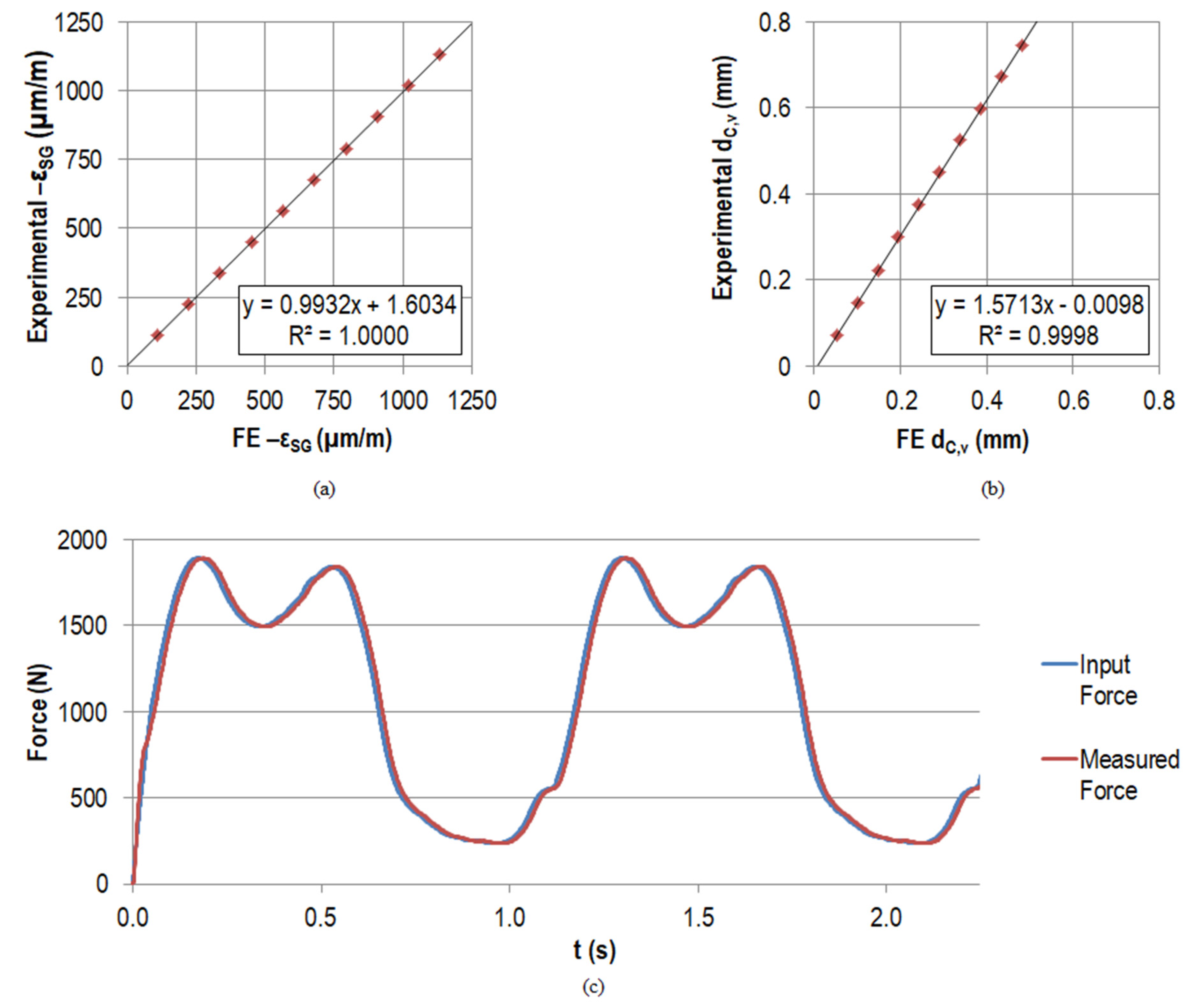
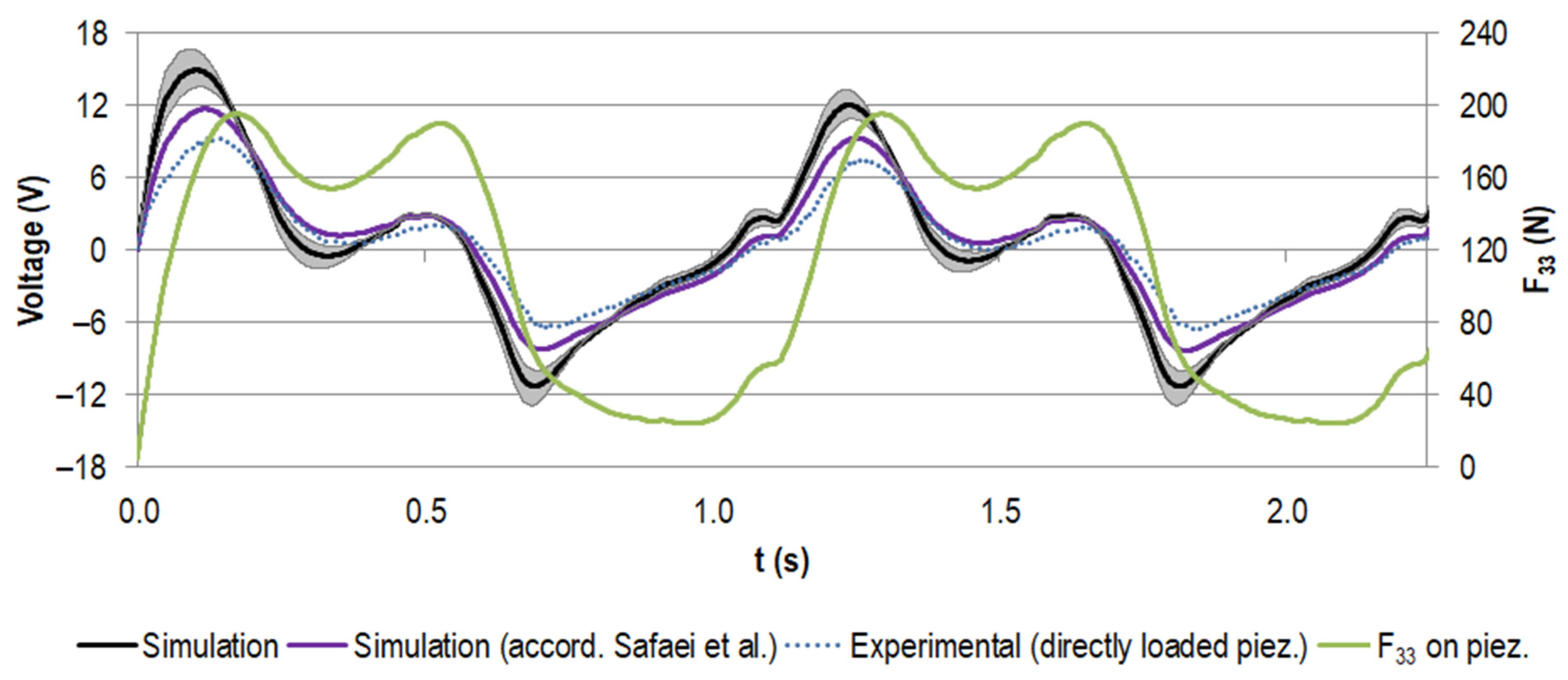
3.2. Experimental Results and Validation
4. Discussion
4.1. Finite Element Analysis: Deformation, Loading, and Sensitivity
4.1.1. Reproduction of Results for New Test Setup
4.1.2. Sensitivity Analysis
4.2. Experimental Testing and Comparison to Numerical Data
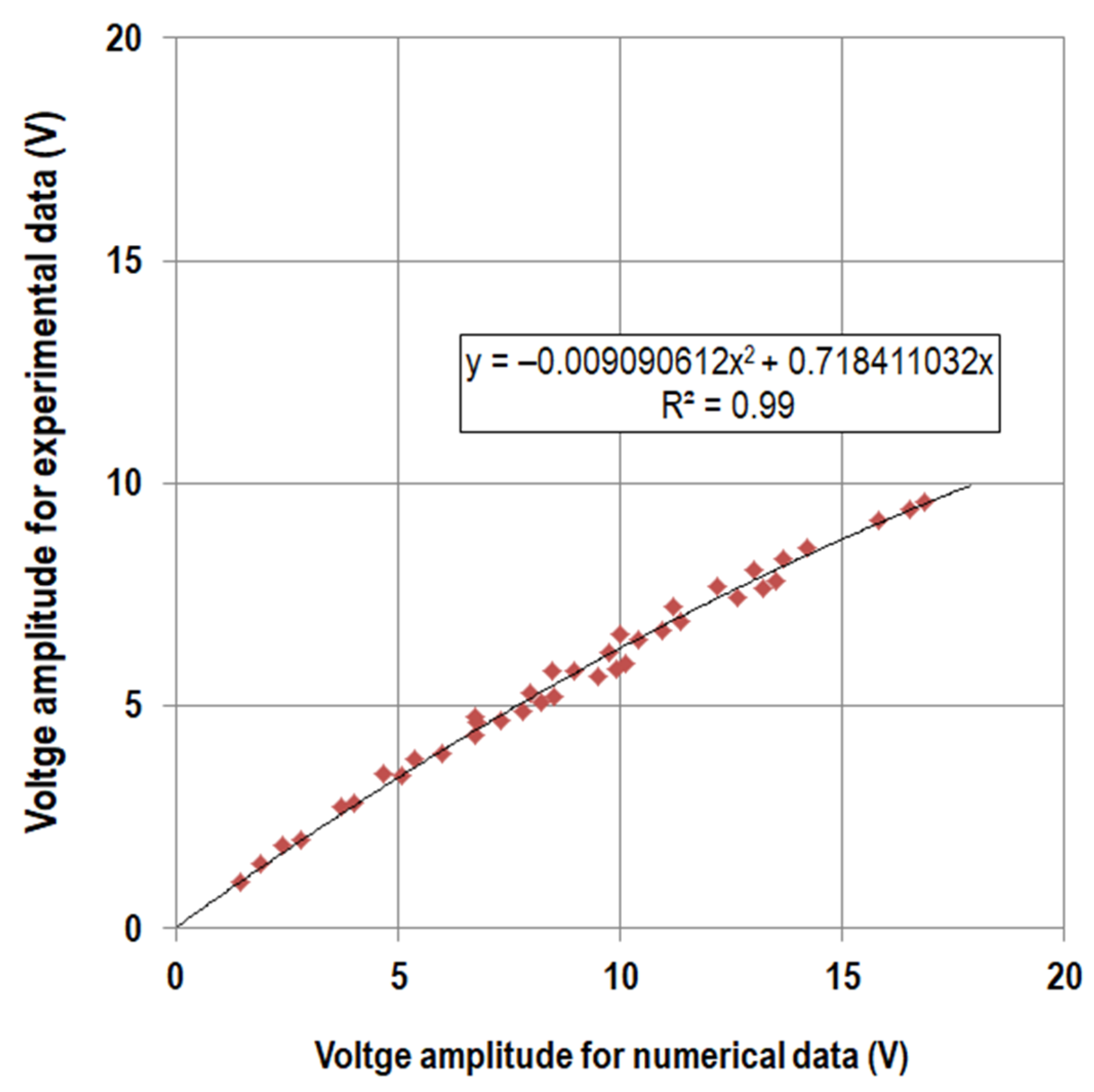
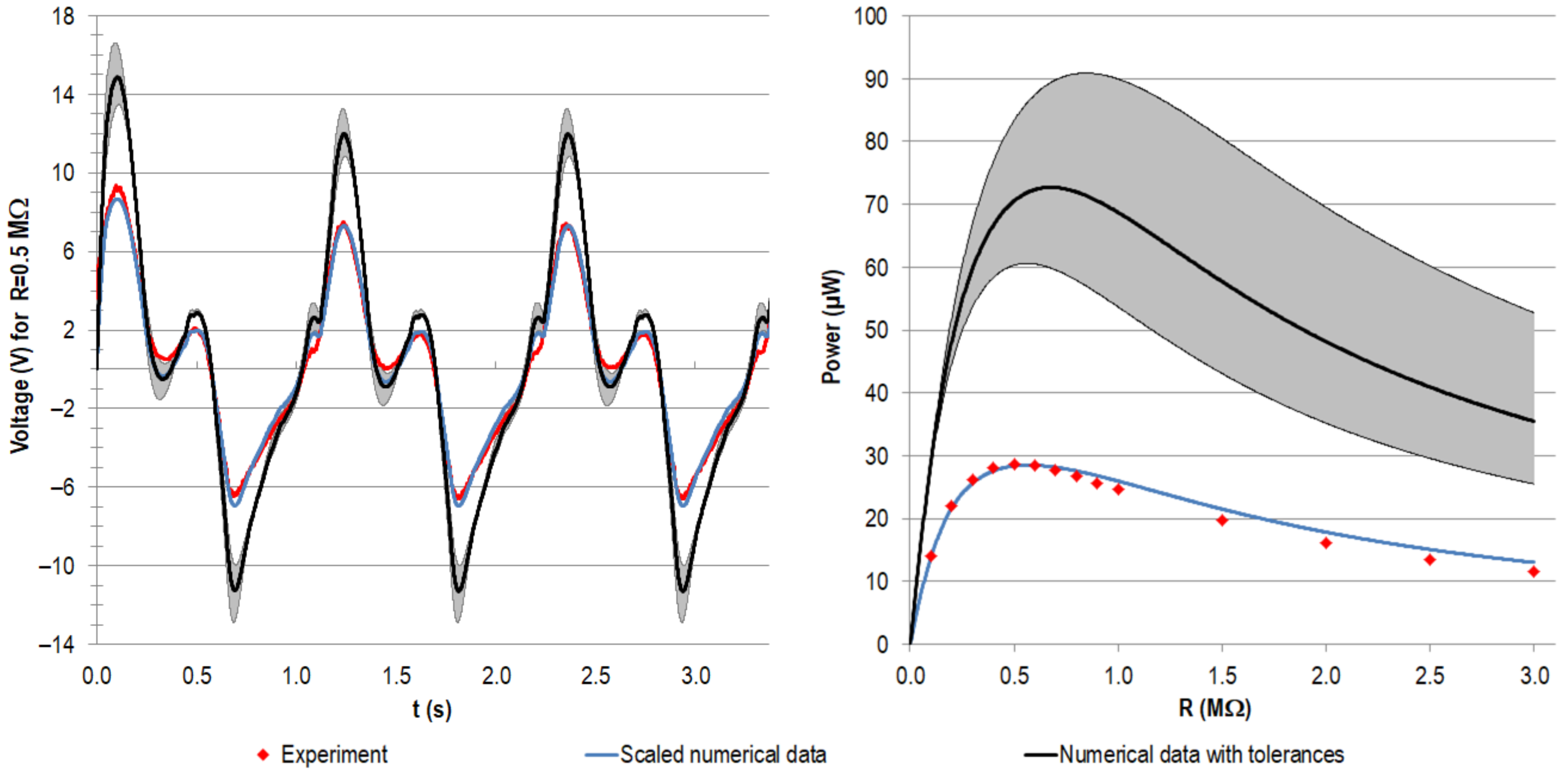
4.2.1. Model Validation
4.2.2. Interpretation of Experimental Data
4.2.3. Interpretation of Numerical Model and Relation with Experiments
4.2.4. Discussion of Power Output
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Sensitvity Analysis

Appendix A.2. Model Calibration
References
- Lespasio, M.J.; Sultan, A.A.; Piuzzi, N.S.; Khlopas, A.; Husni, M.E.; Muschler, G.F.; Mont, M.A. Hip Osteoarthritis: A Primer. Perm. J. 2018, 22, 17–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, R.J.; Palmer, A.; Taylor, A.; Porter, M.L.; Malchau, H.; Glyn-Jones, S. Hip replacement. Lancet 2018, 392, 1662–1671. [Google Scholar] [CrossRef]
- Murray, C.J.L. (Ed.) The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020; Harvard School of Public Health: Cambridge, UK, 1996; ISBN 0965546608. [Google Scholar]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef]
- OECD. Hip and Knee replacement. In Health at a Glance 2017: OECD Indicators; OECD Publishing: Paris, France, 2017; ISBN 9789264280397. [Google Scholar]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of Primary and Revision Hip and Knee Arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg.-Am. Vol. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Pabinger, C.; Lothaller, H.; Portner, N.; Geissler, A. Projections of hip arthroplasty in OECD countries up to 2050. HIP Int. 2018, 28, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.; Garbuz, D.S.; Greidanus, N.V.; Masri, B.; Duncan, C.P. Quality of Life Outcomes in Revision vs Primary Total Hip Arthroplasty: A Prospective Cohort Study. J. Arthroplast. 2008, 23, 550–553. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.L.; Lau, E.; Suggs, J.; Kurtz, S.M.; Manley, M.T. Risk of Subsequent Revision after Primary and Revision Total Joint Arthroplasty. Clin. Orthop. Relat. Res. 2010, 468, 3070–3076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bitton, R. The economic burden of osteoarthritis. Am. J. Manag. Care 2009, 15, 230–235. [Google Scholar]
- Ong, K.L.; Mowat, F.S.; Chan, N.; Lau, E.; Halpern, M.T.; Kurtz, S.M. Economic Burden of Revision Hip and Knee Arthroplasty in Medicare Enrollees. Clin. Orthop. Relat. Res. 2006, 446, 22–28. [Google Scholar] [CrossRef]
- Pabinger, C.; Geissler, A. Utilization rates of hip arthroplasty in OECD countries. Osteoarthr. Cartil. 2014, 22, 734–741. [Google Scholar] [CrossRef] [Green Version]
- Kurtz, S.M.; Ong, K.L.; Lau, E.; Bozic, K.J. Impact of the Economic Downturn on Total Joint Replacement Demand in the United States: Updated projections to 2021. J. Bone Jt. Surg.-Am. Vol. 2014, 96, 624–630. [Google Scholar] [CrossRef]
- Ledet, E.H.; Liddle, B.; Kradinova, K.; Harper, S. Smart implants in orthopedic surgery, improving patient outcomes: A review. Innov. Entrep. Health 2018, 5, 41–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, C.; Zimmermann, U.; Van Rienen, U. Modeling of an Optimized Electrostimulative Hip Revision System Under Consideration of Uncertainty in the Conductivity of Bone Tissue. IEEE J. Biomed. Health Inform. 2015, 19, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, U.; Ebner, C.; Su, Y.; Bender, T.; Bansod, Y.; Mittelmeier, W.; Bader, R.; van Rienen, U. Numerical Simulation of Electric Field Distribution around an Instrumented Total Hip Stem. Appl. Sci. 2021, 11, 6677. [Google Scholar] [CrossRef]
- Raben, H.; Kämmerer, P.W.; Bader, R.; Van Rienen, U. Establishment of a Numerical Model to Design an Electro-Stimulating System for a Porcine Mandibular Critical Size Defect. Appl. Sci. 2019, 9, 2160. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, T.A.C.; Marote, A.; Santos, T.; Torrão, J.; Ramos, A.; Simões, J.A.O.; Silva, O.A.B.D.C.E.; Furlani, E.P.; Vieira, S.I.; Ferreira, J.A.F. New cosurface capacitive stimulators for the development of active osseointegrative implantable devices. Sci. Rep. 2016, 6, 30231. [Google Scholar] [CrossRef]
- Mittelmeier, W.; Lehner, S.; Kraus, W.; Matter, H.P.; Gerdesmeyer, L.; Steinhauser, E. BISS: Concept and biomechanical investigations of a new screw system for electromagnetically induced internal osteostimulation. Arch. Orthop. Trauma Surg. 2004, 124, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Rydell, N.W. Forces Acting on the Femoral Head-Prosthesis: A Study on Strain Gauge Supplied Prostheses in Living Persons. Acta Orthop. Scand. 1966, 37 (Suppl. S88), 1–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waugh, T.R. Intravital Measurements During Instrumental Correction of Idiopathic Scoliosis. Acta Orthop. Scand. 1966, 37, 1–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergmann, G.; Graichen, F.; Siraky, J.; Jendrzynski, H.; Rohlmann, A. Multichannel strain gauge telemetry for orthopaedic implants. J. Biomech. 1988, 21, 169–176. [Google Scholar] [CrossRef]
- Carlson, C.E.; Mann, R.W.; Harris, W.H. A Radio Telemetry Device for Monitoring Cartilage Surface Pressures in the Human Hip. IEEE Trans. Biomed. Eng. 1974, 21, 257–264. [Google Scholar] [CrossRef]
- Damm, P.; Graichen, F.; Rohlmann, A.; Bender, A.; Bergmann, G. Total hip joint prosthesis for in vivo measurement of forces and moments. Med. Eng. Phys. 2010, 32, 95–100. [Google Scholar] [CrossRef] [PubMed]
- D’Lima, D.; Townsend, C.P.; Arms, S.W.; Morris, B.A.; Colwell, C.W. An implantable telemetry device to measure intra-articular tibial forces. J. Biomech. 2005, 38, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Windisch, C.; Kolb, W.; Röhner, E.; Wagner, M.; Roth, A.; Matziolis, G.; Wägner, A. Invasive Electromagnetic Field Treatment in Osteonecrosis of the Femoral Head: A Prospective Cohort Study. Open Orthop. J. 2014, 8, 125–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platt, S.R.; Farritor, S.; Garvin, K.; Haider, H. The Use of Piezoelectric Ceramics for Electric Power Generation within Orthopedic Implants. IEEE/ASME Trans. Mechatron. 2005, 10, 455–461. [Google Scholar] [CrossRef]
- Almouahed, S.; Gouriou, M.; Hamitouche, C.; Stindel, E.; Roux, C. Self-powered instrumented knee implant for early detection of postoperative complications. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Buenos Aires, Argentina, 31 August–4 September 2010; Volume 2010, pp. 5121–5124. [Google Scholar] [CrossRef]
- Almouahed, S.; Hamitouche, C.; Poignet, P.; Stindel, E. Battery-free force sensor for instrumented knee implant. In Proceedings of the 2017 IEEE Healthcare Innovations and Point of Care Technologies (HI-POCT), Bethesda, MD, USA, 6–8 November 2017. [Google Scholar] [CrossRef]
- Almouahed, S.; Hamitouche, C.; Stindel, E. Optimized Prototype of Instrumented Knee Implant: Experimental Validation. IRBM 2017, 38, 250–255. [Google Scholar] [CrossRef]
- Wilson, B.E.; Anton, S.R.; Meneghini, R. Development of Biomechanical Knee Force Model for Evaluation of Piezoelectric Sensors for In-Vivo Monitoring. In ASME 2014 Conference on Smart Materials, Adaptive Structures and Intelligent Systems, Proceedings of the ASME Conference on Smart Materials, Adaptive Structures and Intelligent Systems, 8–10 September 2014; Zagrai, A., Ed.; ASME: Newport, RI, USA, 2014; p. V002T02A018. ISBN 978-0-7918-4615-5. [Google Scholar]
- Wilson, B.E. Modeling and Experimentation for Evaluation of Piezoelectric Sensors for In-Vivo Monitoring. Master’s Thesis, Tennessee Technological University, Cookeville, TN, USA, 2015. [Google Scholar]
- Safaei, M.; Meneghini, R.M.; Anton, S.R. Parametric analysis of electromechanical and fatigue performance of total knee replacement bearing with embedded piezoelectric transducers. Smart Mater. Struct. 2017, 26, 094002. [Google Scholar] [CrossRef] [PubMed]
- Safaei, M.; Meneghini, R.M.; Anton, S.R. Force detection, center of pressure tracking, and energy harvesting from a piezoelectric knee implant. Smart Mater. Struct. 2018, 27, 114007. [Google Scholar] [CrossRef] [PubMed]
- Safaei, M.; Dupre, S.; Hoummadi, E.; Anton, S.R. Design, analysis, and fabrication of a piezoelectric force tray for total knee replacements. J. Intell. Mater. Syst. Struct. 2019, 93, 1045389X1988000. [Google Scholar] [CrossRef] [PubMed]
- Holmberg, J.; Alexander, L.; Rajamani, R.; Bechtold, J.E. Battery-Less Wireless Instrumented Knee Implant. J. Med. Devices 2013, 7, 011006. [Google Scholar] [CrossRef]
- Luciano, V.; Sardini, E.; Serpelloni, M.; Baronio, G. An energy harvesting converter to power sensorized total human knee prosthesis. Meas. Sci. Technol. 2014, 25, 25702. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.; Jain, M.; Salman, E.; Willing, R.; Towfighian, S. A smart knee implant using triboelectric energy harvesters. Smart Mater. Struct. 2019, 28, 025040. [Google Scholar] [CrossRef] [PubMed]
- Morais, R.; Silva, N.; Santos, P.; Frias, C.; Ferreira, J.A.F.; Ramos, A.; Simõesd, J.; Baptista, J.; Reis, M.J.C.D.S. Permanent magnet vibration power generator as an embedded mechanism for smart hip prosthesis. Procedia Eng. 2010, 5, 766–769. [Google Scholar] [CrossRef]
- Silva, N.; Santos, P.; Ferreira, J.; Santos, M.; Reis, M.J.C.D.S.; Morais, R. Multi-purpose and Multi-source Energy Management System for Biomedical Implants. Procedia Eng. 2012, 47, 722–725. [Google Scholar] [CrossRef] [Green Version]
- Lange, H.-E.; Hohlfeld, D.; Bader, R.; Kluess, D. A piezoelectric energy harvesting concept for an energy-autonomous instrumented total hip replacement. Smart Mater. Struct. 2020, 29, 115051. [Google Scholar] [CrossRef]
- Lange, H.-E.; Bader, R.; Kluess, D. Endurance testing and finite element simulation of a modified hip stem for integration of an energy harvesting system. Proc. Inst. Mech. Eng. Part. H J. Eng. Med. 2021, 22, 9544119211021675. [Google Scholar] [CrossRef]
- International Organization for Standardization. Implants for Surgery Components—Partial and Total Hip Joint Prostheses—Part 4: Determination of Endurance Properties and Performance of Stemmed Femoral; International Organization for Standardization: Geneva, Switzerland, 2015; ISO 7206-4:2010. [Google Scholar]
- Kluess, D.; Lange, H.-E.; Heyer, H.; Sander, M.; Mittelmeier, W.; Bader, R. Supplementary finite element analysis in experimental testing of total hip stems. Mater. Test. 2018, 60, 489–494. [Google Scholar] [CrossRef]
- Bergmann, G.; Bender, A.; Dymke, J.; Duda, G.; Damm, P. Standardized Loads Acting in Hip Implants. PLoS ONE 2016, 11, e0155612. [Google Scholar] [CrossRef]
- Wieding, J.; Souffrant, R.; Fritsche, A.; Mittelmeier, W.; Bader, R. Finite Element Analysis of Osteosynthesis Screw Fixation in the Bone Stock: An Appropriate Method for Automatic Screw Modelling. PLoS ONE 2012, 7, e33776. [Google Scholar] [CrossRef]
- Nuño, N.; Groppetti, R.; Senin, N. Static coefficient of friction between stainless steel and PMMA used in cemented hip and knee implants. Clin. Biomech. 2006, 21, 956–962. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yin, Z.; Li, H.; Gao, G.; Zhang, X. Friction and wear characteristics of ultrahigh molecular weight polyethylene (UHMWPE) composites containing glass fibers and carbon fibers under dry and water-lubricated conditions. Wear 2017, 380–381, 42–51. [Google Scholar] [CrossRef]
- Leung, K.-S.; Taglang, G.; Schnettler, R.; Alt, V.; Haarman, H.J.T.M.; Seidel, H.; Kempf, I. Practice of Intramedullary Locked Nails; Springer: Berlin/Heidelberg, Germany, 2006; ISBN 978-3-540-25349-5. [Google Scholar]
- Kurtz, S.M. UHMWPE biomaterials handbook. In Ultra High Molecular Weight Polyethylene in Total Joint Replacement and Medical Devices, 2nd ed.; Academic Press: London, UK, 2009; ISBN 9780123747211. [Google Scholar]
- PI Ceramic GmbH. Material Coefficients PIC255, v4.3; PI Ceramic GmbH: Lederhose, Germany, 2017. [Google Scholar]
- Saha, S.; Pal, S. Mechanical properties of bone cement: A review. J. Biomed. Mater. Res. 1984, 18, 435–462. [Google Scholar] [CrossRef] [PubMed]
- Pacific Research Laboratories Inc. Biomechanical Materials for Precise, Repeatable Testing: Materials Guide. Available online: https://www.sawbones.com/biomechanical-product-info (accessed on 23 July 2019).
- Huntsman Advanced Materials. Data sheet: RenCast® FC 52/53 Isocyanate / FC 53 Polyol. In Casting Resin Quick Setting Polyurethane System; Huntsman Advanced Materials (Swizerland) GmbH: Basel, Switzerland, 2014. [Google Scholar]
- Berlincourt, D.A.; Curran, D.R.; Jaffe, H. Piezoelectric and Piezomagnetic Materials and Their Function in Transducers. In Physical Acoustics: Principles and Methods; Mason, W., Ed.; Academic Press: New York, NY, USA; London, UK, 1964; pp. 169–270. ISBN 9781483228570. [Google Scholar]
- Safaei, M. A piezoelectric instrumented total knee replacement for sensing and energy harvesting. In Dissertation; Tennessee Technological University: Cookeville, TN, USA, 2019. [Google Scholar]
- Safaei, M.; Anton, S.R. Experimental Evaluation of Sensing and Energy Harvesting Behavior of Implanted Piezoelectric Transducers in Total Knee Replacement. In Volume 1: Development and Characterization of Multifunctional Materials; Mechanics and Behavior of Active Materials; Bioinspired Smart Materials and Systems; Energy Harvesting; Emerging Technologies, Proceedings of the ASME 2017 Conference on Smart Materials, Adaptive Structures and Intelligent Systems, Snowbird, UT, USA, 18–20 September 2017; ASME: New York, NY, USA, 2017; p. V001T07A011. ISBN 978-0-7918-5825-7. [Google Scholar]
- PI Ceramic GmbH. Data sheet Round PICMA® Chip Actuators: Miniature Multilayer Piezo Actuators with and without Inner Hole. Available online: https://static.piceramic.com/fileadmin/user_upload/physik_instrumente/files/datasheets/PD0xx-Datasheet.pdf (accessed on 15 January 2019).
- Speirs, A.; Heller, M.; Duda, G.N.; Taylor, W.R. Physiologically based boundary conditions in finite element modelling. J. Biomech. 2007, 40, 2318–2323. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Cooper, T.A.; Lin, H.-T.; Wereszczak, A. Fatigue responses of lead zirconate titanate stacks under semibipolar electric cycling with mechanical preload. J. Appl. Phys. 2010, 108, 084107. [Google Scholar] [CrossRef]
- Heller, M.; Bergmann, G.; Kassi, J.-P.; Claes, L.; Haas, N.; Duda, G. Determination of muscle loading at the hip joint for use in pre-clinical testing. J. Biomech. 2005, 38, 1155–1163. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, Y. Comparison of Fatigue Properties and Fatigue Crack Growth Rates of Various Implantable Metals. Materials 2012, 5, 2981–3005. [Google Scholar] [CrossRef] [Green Version]
- Kluess, D.; Soodmand, E.; Lorenz, A.; Pahr, D.; Schwarze, M.; Cichon, R.; Varady, P.A.; Herrmann, S.; Buchmeier, B.; Schröder, C.; et al. A round-robin finite element analysis of human femur mechanics between seven participating laboratories with experimental validation. Comput. Methods Biomech. Biomed. Eng. 2019, 22, 1020–1031. [Google Scholar] [CrossRef] [PubMed]
- Lange, H.-E.; Bader, R.; Kluess, D. Design Study on Customised Piezoelectric Elements for Energy Harvesting in Total Hip Replacements. Energies 2021, 14, 3480. [Google Scholar] [CrossRef]
- Lange, H.-E.; Arbeiter, N.; Bader, R.; Kluess, D. Experimental Study of an Energy Harvesting System for Energy-Autonomous Instrumented Total Hip Replacements. In Proceedings of the 26th Congress of the European Society of Biomechanics, Milan, Italy, 11–14 July 2021. [Google Scholar]
- Santos, M.; Ferreira, J.; Ramos, A.; Pascoal, R.; Morais, R.; Silva, N.; Simoes, J.; Reis, M.J.C.S.; Boeri, C.N.; Festas, A.; et al. Multi-Source Energy Harvesting Power Generators for Instrumented Implants—Towards the Development of a Smart Hip Prosthesis. In Biodevices 2012, Proceedings of the International Conference on Biomedical Electronics and Devices; Vilamoura, Algarve, Portugal, 1–4 February 2012; Integrated in BIOSTEC (International Joint Conference on Biomedical Engineering Systems and Technologies); International Conference on Biomedical Electronics and Devices; Gabriel, J., Ed.; SciTePress: Setubal, Portugal, 2012; Volume l, pp. 71–81. ISBN 978-989-8425-91-1. [Google Scholar]
- Safaei, M.; Meneghini, R.M.; Anton, S.R. Energy Harvesting and Sensing with Embedded Piezoelectric Ceramics in Knee Implants. IEEE/ASME Trans. Mechatron. 2018, 23, 864–874. [Google Scholar] [CrossRef]
- Morais, R.; Silva, N.; Santos, P.M.; Frias, C.M.; Ferreira, J.A.F.; Ramos, A.; Simões, J.A.; Baptista, J.; Reis, M.J.C.D.S. Double permanent magnet vibration power generator for smart hip prosthesis. Sens. Actuators A Phys. 2011, 172, 259–268. [Google Scholar] [CrossRef]
- Chen, H.; Liu, M.; Hao, W.; Chen, Y.; Jia, C.; Zhang, C.; Wang, Z. Low-Power Circuits for the Bidirectional Wireless Monitoring System of the Orthopedic Implants. IEEE Trans. Biomed. Circuits Syst. 2009, 3, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Dauben, T.J.; Ziebart, J.; Bender, T.; Zaatreh, S.; Kreikemeyer, B.; Bader, R. A Novel In Vitro System for Comparative Analyses of Bone Cells and Bacteria under Electrical Stimulation. BioMed Res. Int. 2016, 2016, 5178640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plocksties, F.; Niemann, C.; Bader, R.; Mows, F.; Seitz, H.; Kammerer, P.W.; Dau, M.; Kamp, V.; Heller, J.; Timmermann, D. Requirements and Design of an Implant for Electrical Stimulation for Bone Regeneration in Animals. In Proceedings of the 2020 IEEE 2nd Global Conference on Life Sciences and Technologies (LifeTech), Kyoto, Japan, 10–12 March 2020; pp. 157–160. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FX (N) | FY (N) | FZ (N) | Ftotal (N) |
|---|---|---|---|
| 396.97 | –167.82 | –1843.27 | 1892.99 |
| Component (Material) | Young’s Modulus (GPa) | Poisson’s Ratio |
|---|---|---|
| Implant | ||
| Metallic total hip stem (high-nitrogen stainless steel) | 195 [49] | 0.3 1 |
| Housing (UHMW-PE) | 0.83 [50] | 0.46 [50] |
| Piezoelectric element (PZT) | 52.4 [51] | 0.35 [51] |
| Bone cement (polymethylmethacrylate) | 2.3 [52] | 0.3 1 |
| Artificial bone | ||
| Cortical bone (short fibre-filled epoxy) | 16 [53] | 0.26 [53] |
| Cancellous bone (polyurethane foam) | 0.155 [53] | 0.3 1 |
| Embedding resin (casting resin with filler) | 2.4 [54] | 0.3 1 |
| Parameter (Unit) | Value |
|---|---|
| (-) | 936 |
| (-) | 759 |
| (-) | 1751 |
| d33 (m/V) | 3.996 × 10–10 |
| e31 (N/Vm) | –6.730 |
| e33 (N/Vm) | 15.680 |
| e15 (N/Vm) | 13.140 |
| Configuration | Capacity acc. Manufacturer (nF) | Calculated Capacity (nF) | ||
|---|---|---|---|---|
| Ref. Value | Low | High | ||
| Single element | 110 | 88 | 132 | 168.9 |
| Stacked element | 220 | 176 | 264 | 337.7 |
| dc,total (mm) | σimp (MPa) | σpiez (MPa) | F33 (N) | VOC (V) | |||
|---|---|---|---|---|---|---|---|
| Single Element | After iterative study | 1.64 | 273.5 | 16.6 | 138.7 | 11.6 | |
| Previous model [41] | 1.65 | 269.4 | 14.1 | 141.6 | 11.9 | ||
| Difference | relative | –0.6% | 1.5% | 17.7% | –2.0% | –2.5% | |
| absolute | –0.01 | 4.1 | 2.5 | –2.9 | –0.3 | ||
| Stacked Element | After iterative study | 1.65 | 269.6 | 18.1 | 194.9 | 16.8 | |
| Previous model [41] | 1.65 | 267.2 | 16.9 | 196.3 | 16.9 | ||
| Difference | relative | 0.0% | 0.9% | 7.1% | –0.7% | –0.6% | |
| absolute | 0.0 | 2.4 | 1.2 | –1.4 | –0.1 | ||
| FX (N) | FY (N) | FZ (N) | Ftotal (N) | ||
| Bergmann et al. [45] | 535.72 | –342.48 | –1747.18 | 1859.28 | |
| Scaled after iterative study | 396.97 | –167.82 | –1843.27 | 1892.99 | |
| Difference | relative | –25.9% | –51.0% | 5.5% | 1.80% |
| absolute | –138.75 | 174.67 | –96.09 | 33.71 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lange, H.-E.; Arbeiter, N.; Bader, R.; Kluess, D. Performance of a Piezoelectric Energy Harvesting System for an Energy-Autonomous Instrumented Total Hip Replacement: Experimental and Numerical Evaluation. Materials 2021, 14, 5151. https://doi.org/10.3390/ma14185151
Lange H-E, Arbeiter N, Bader R, Kluess D. Performance of a Piezoelectric Energy Harvesting System for an Energy-Autonomous Instrumented Total Hip Replacement: Experimental and Numerical Evaluation. Materials. 2021; 14(18):5151. https://doi.org/10.3390/ma14185151
Chicago/Turabian StyleLange, Hans-E., Nils Arbeiter, Rainer Bader, and Daniel Kluess. 2021. "Performance of a Piezoelectric Energy Harvesting System for an Energy-Autonomous Instrumented Total Hip Replacement: Experimental and Numerical Evaluation" Materials 14, no. 18: 5151. https://doi.org/10.3390/ma14185151
APA StyleLange, H.-E., Arbeiter, N., Bader, R., & Kluess, D. (2021). Performance of a Piezoelectric Energy Harvesting System for an Energy-Autonomous Instrumented Total Hip Replacement: Experimental and Numerical Evaluation. Materials, 14(18), 5151. https://doi.org/10.3390/ma14185151