
Accuracy of Dental Implant Placement by a Novel In-House Model-Free and Zero-Setup Fully Guided Surgical Template Made of a Light-Cured Composite Resin (VARO Guide®): A Comparative In Vitro Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Group Allocation
- Expert group (n = 10): experience of implant surgery >100 cases
- Beginner group (n = 10): experience of implant surgery < 10cases
2.2. Experimental Materials
2.2.1. Surgical Guides
- VARO Guide® (Neobiotech, Seoul, Korea): a novel type of in-house, model-free and zero-setup surgical templates, which is fabricated by milling the light-cured preguide filled with composite resin composed of dimethacrylate and diurethane (Figure 1a)
- Navi Guide® (Neobiotech): a polymethylmethacrylate (PMMA)-based surgical template with a metal sleeve, which is 3D-printed based on the virtual design (Figure 1b).
- VG group: fully guided implant surgery using VARO Guide® (VG);
- NG group: fully guided implant surgery using Navi Guide® (NG).
2.2.2. Dentiform Model and Implant Fixture
2.3. Treatment Protocol
2.3.1. Presurgical Virtual Implant Placement and Surgical Guide Fabrication for the VG Group
2.3.2. Presurgical Virtual Implant Placement and Surgical Guide Fabrication for the NG Group
2.3.3. Fully Guided Implant Surgery
2.4. Outcome Variables and Measurements
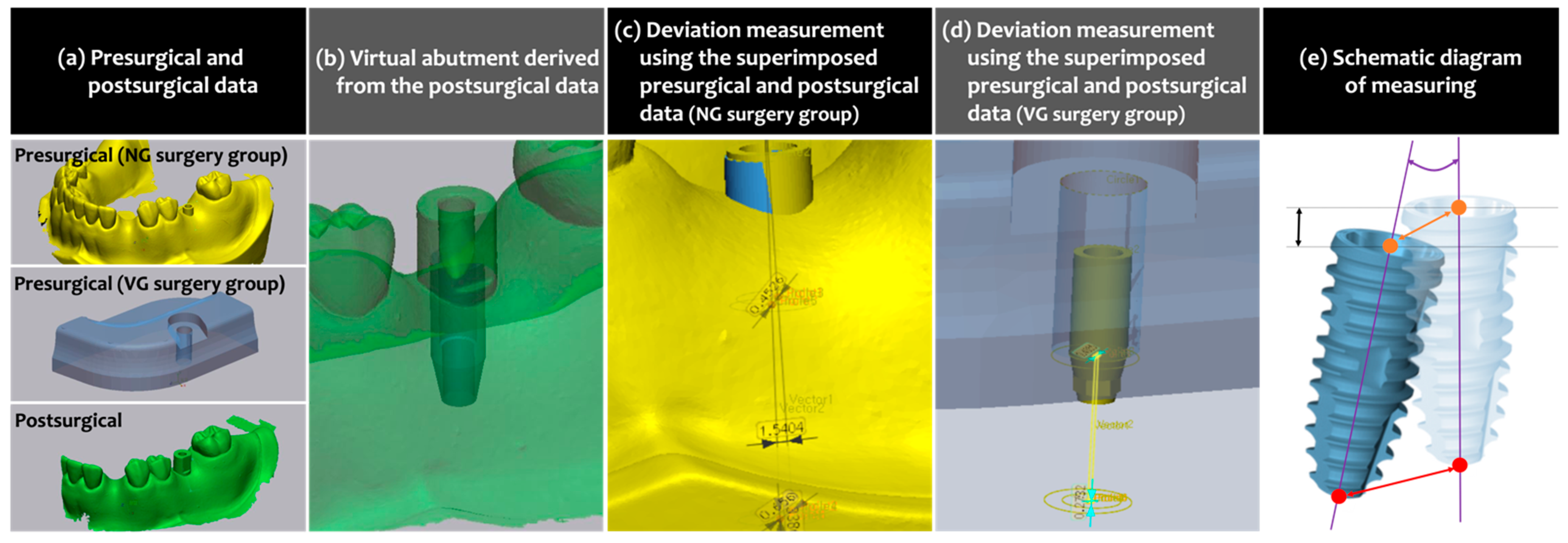
2.4.1. Accuracy of Implant Placement
- Vertical deviation (mm): the linear deviation measured in the aspect of vertical height of the implant fixture platform.
- Angular deviation (°): the angle measured between the virtually planned axis and the actually placed axis of the implant.
- Platform deviation (mm): the linear deviation measured in the horizontal aspect at the implant fixture platform level.
- Apex deviation (mm): the linear deviation measured in the horizontal aspect at the implant fixture apex level.
2.4.2. Procedure Time
- Total procedure time: the time spent from the beginning of the presurgical preparation to the end of the implant surgery.
- Presurgical preparation time: the time spent on the virtual implant planning and surgical guide fabrication estimated in detail as follows:
- -
- Curing/scanning time: time spent on preguide curing (VG group only) or optical scanning (NG group only);
- -
- Virtual planning time: time spent on virtual planning with the corresponding computer software of each surgery group;
- -
- Guide fabrication and delivery time: time spent from the start of milling (VG group only) or 3D printing (NG group only) to the delivery of the surgical guide to the surgeon.
- Surgery time: the time spent on the fully guided implant placement only (from the start of the surgical guide sitting onto the dentiform model to the final installation of the implant fixture).
2.5. Statistical Analysis
- VG group versus NG group, in terms of implant placement accuracy and procedure time.
- VG group versus NG group within the expert group, in terms of implant placement accuracy and procedure time.
- VG group versus NG group within the beginner group, in terms of implant placement accuracy and procedure time.
- Expert group versus beginner group within the VG group, in terms of implant placement accuracy and procedure time.
- Expert group versus beginner group within the NG group, in terms of implant placement accuracy and procedure time.
3. Results
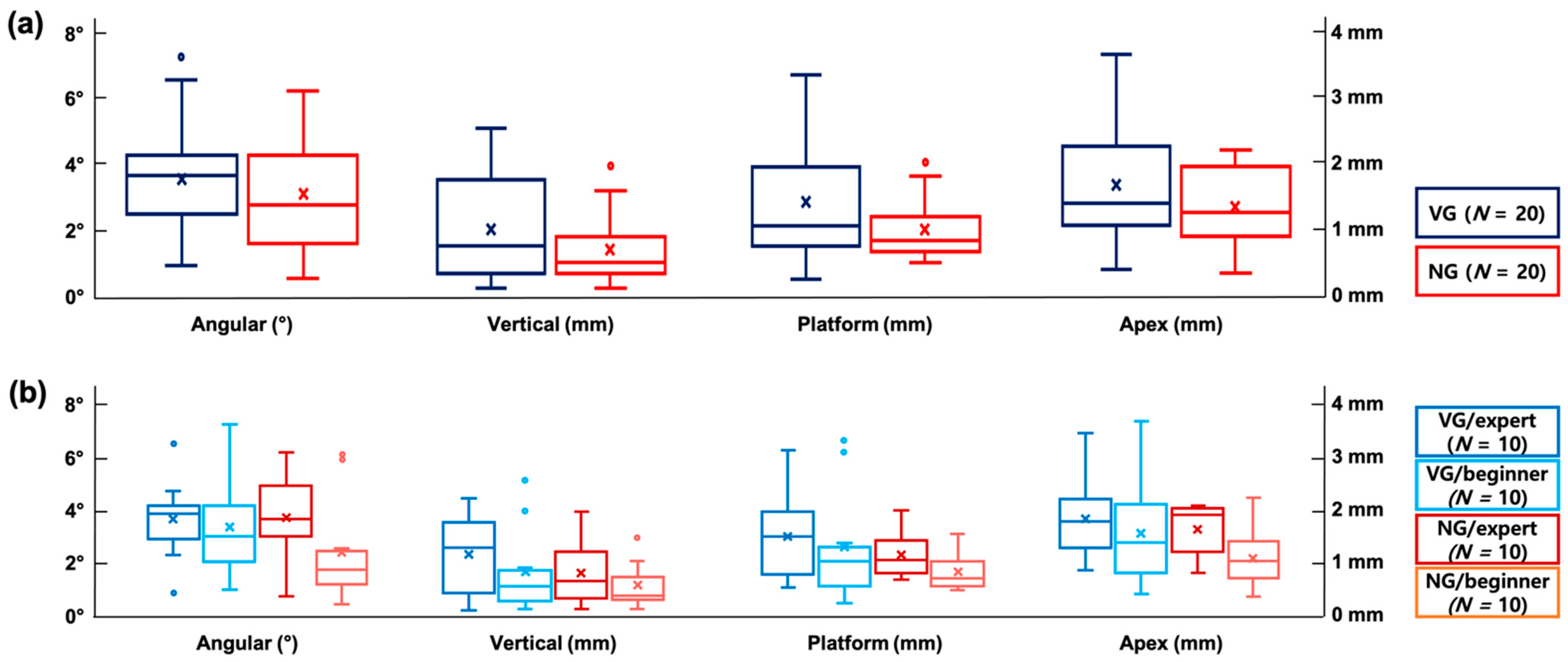
3.1. Accuracy of Implant Placement
3.1.1. VG versus NG Surgery
3.1.2. VG versus NG Surgery within the Expert and Beginner Groups
3.1.3. Expert Group versus Beginner Group within the VG and NG Surgery
3.2. Procedure Time
3.2.1. VG versus NG Surgery
3.2.2. VG versus NG Surgery within the Expert and Beginner Groups
3.2.3. Expert Group versus Beginner Group within the VG and NG Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- van Velzen, F.J.; Ofec, R.; Schulten, E.A.; Ten Bruggenkate, C.M. 10-year survival rate and the incidence of peri-implant disease of 374 titanium dental implants with a SLA surface: A prospective cohort study in 177 fully and partially edentulous patients. Clin. Oral Implants Res. 2015, 26, 1121–1128. [Google Scholar] [CrossRef]
- Shen, P.; Zhao, J.; Fan, L.; Qiu, H.; Xu, W.; Wang, Y.; Zhang, S.; Kim, Y.J. Corrigendum to “Accuracy evaluation of computer-designed surgical guide template in oral implantology”. J. Craniomaxillofac. Surg. 2016, 44, 758. [Google Scholar] [CrossRef]
- Chen, S.; Ou, Q.; Lin, X.; Wang, Y. Comparison Between a Computer-Aided Surgical Template and the Free-Hand Method: A Systematic Review and Meta-Analysis. Implant Dent. 2019, 28, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Schnitman, P.A.; Hayashi, C.; Han, R.K. Why guided when freehand is easier, quicker, and less costly? J. Oral Implantol. 2014, 40, 670–678. [Google Scholar] [CrossRef] [PubMed]
- Schulz, M.C.; Rittmann, L.; Range, U.; Lauer, G.; Haim, D. The Use of Orientation Templates and Free-Hand Implant Insertion in Artificial Mandibles-An Experimental Laboratory Examination in Fifth-Year Dental Students. Dent. J. (Basel) 2018, 6, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.E.; Park, J.H.; Moon, H.S.; Shim, J.S. Simplified digital workflow for dental implant restoration on a stock abutment using an intraoral scanner: A dental technique. J. Prosthet. Dent. 2017, 118, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Zhang, L.; Cai, Z.; Shan, X. Dental Implant Rehabilitation After Jaw Reconstruction Assisted by Virtual Surgical Planning. Int. J. Oral Maxillofac. Implants 2019, 34, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- D’Haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontology 2017, 73, 121–133. [Google Scholar] [CrossRef]
- Sancho-Puchades, M.; Alfaro, F.H.; Naenni, N.; Jung, R.; Hammerle, C.; Schneider, D. A Randomized Controlled Clinical Trial Comparing Conventional and Computer-Assisted Implant Planning and Placement in Partially Edentulous Patients. Part 2: Patient Related Outcome Measures. Int. J. Periodontics Restor. Dent. 2019, 39, e99–e110. [Google Scholar] [CrossRef]
- Schneider, D.; Sancho-Puchades, M.; Schober, F.; Thoma, D.; Hammerle, C.; Jung, R. A Randomized Controlled Clinical Trial Comparing Conventional and Computer-Assisted Implant Planning and Placement in Partially Edentulous Patients. Part 3: Time and Cost Analyses. Int. J. Periodontics Restor. Dent. 2019, 39, e71–e82. [Google Scholar] [CrossRef]
- Schneider, D.; Sancho-Puchades, M.; Benic, G.I.; Hammerle, C.H.; Jung, R.E. A Randomized Controlled Clinical Trial Comparing Conventional and Computer-Assisted Implant Planning and Placement in Partially Edentulous Patients. Part 1: Clinician-Related Outcome Measures. Int. J. Periodontics Restor. Dent. 2018, 38, s49–s57. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Park, J.M.; Kim, S.M.; Kim, M.J.; Lee, J.H.; Kim, M.J. An assessment of template-guided implant surgery in terms of accuracy and related factors. J. Adv. Prosthodont. 2013, 5, 440–447. [Google Scholar] [CrossRef] [Green Version]
- Schnutenhaus, S.; Edelmann, C.; Rudolph, H.; Dreyhaupt, J.; Luthardt, R.G. 3D accuracy of implant positions in template-guided implant placement as a function of the remaining teeth and the surgical procedure: A retrospective study. Clin. Oral Investig. 2018, 22, 2363–2372. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Song, Y.W.; Park, S.H.; Kim, J.H.; Park, J.M.; Lee, J.S. Clinical factors influencing implant positioning by guided surgery using a nonmetal sleeve template in the partially edentulous ridge: Multiple regression analysis of a prospective cohort. Clin. Oral Implants Res. 2020, 31, 1187–1198. [Google Scholar] [CrossRef]
- Hoffmann, J.; Westendorff, C.; Gomez-Roman, G.; Reinert, S. Accuracy of navigation-guided socket drilling before implant installation compared to the conventional free-hand method in a synthetic edentulous lower jaw model. Clin. Oral Implants Res. 2005, 16, 609–614. [Google Scholar] [CrossRef]
- Ozan, O.; Turkyilmaz, I.; Ersoy, A.E.; McGlumphy, E.A.; Rosenstiel, S.F. Clinical accuracy of 3 different types of computed tomography-derived stereolithographic surgical guides in implant placement. J. Oral Maxillofac Surg. 2009, 67, 394–401. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29 (Suppl. 16), 416–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo-Oyagüe, R.; Lynch, C.D.; Turrión, A.S.; López-Lozano, J.F.; Torres-Lagares, D.; Suárez-García, M.J. Misfit and microleakage of implant-supported crown copings obtained by laser sintering and casting techniques, luted with glass-ionomer, resin cements and acrylic/urethane-based agents. J. Dent. 2013, 41, 90–96. [Google Scholar] [CrossRef]
- Pereira, L.M.S.; Sordi, M.B.; Magini, R.S.; Calazans Duarte, A.R.; Souza, J.C.M. Abutment misfit in implant-supported prostheses manufactured by casting technique: An integrative review. Eur. J. Dent. 2017, 11, 553–558. [Google Scholar] [CrossRef]
- Castillo-de-Oyagüe, R.; Sánchez-Turrión, A.; López-Lozano, J.F.; Albaladejo, A.; Torres-Lagares, D.; Montero, J.; Suárez-García, M.J. Vertical misfit of laser-sintered and vacuum-cast implant-supported crown copings luted with definitive and temporary luting agents. Med. Oral Patol. Oral Cir. Bucal 2012, 17, e610–e617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eshraghi, T.; McAllister, N.; McAllister, B. Clinical applications of digital 2-D and 3-D radiography for the periodontist. J. Evid. Based Dent. Pract. 2012, 12, 36–45. [Google Scholar] [CrossRef]
- Jung, R.E.; Schneider, D.; Ganeles, J.; Wismeijer, D.; Zwahlen, M.; Hämmerle, C.H.; Tahmaseb, A. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2009, 24, 92–109. [Google Scholar]
- Park, J.M.; Yi, T.K.; Koak, J.Y.; Kim, S.K.; Park, E.J.; Heo, S.J. Comparison of five-axis milling and rapid prototyping for implant surgical templates. Int. J. Oral Maxillofac. Implant. 2014, 29, 374–383. [Google Scholar] [CrossRef] [Green Version]
- Hur, B.; Oh, K.C.; Shim, J.S.; Park, J.M. Use of Model-Free and Zero-Setup Computer-Guided Implant Surgical Template for Partial Edentulous Cases. Implantology 2019, 23, 220–228. [Google Scholar] [CrossRef]
- Sun, T.M.; Lan, T.H.; Pan, C.Y.; Lee, H.E. Dental implant navigation system guide the surgery future. Kaohsiung J. Med. Sci. 2018, 34, 56–64. [Google Scholar] [CrossRef]
- Neugebauer, J.; Stachulla, G.; Ritter, L.; Dreiseidler, T.; Mischkowski, R.A.; Keeve, E.; Zöller, J.E. Computer-aided manufacturing technologies for guided implant placement. Expert Rev. Med. Devices 2010, 7, 113–129. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (Experts + Beginners) | Expert Group | Beginner Group | |
|---|---|---|---|
| Number of participants | 20 | 10 | 10 |
| Age (mean ± standard deviation, years) | 29.55 ± 3.44 | 31.2 ± 3.29 | 27.9 ± 3.07 |
| Period of dental implant surgeon career (mean ± standard deviation, years) | 3.10 ± 2.29 | 4.80 ± 2.10 | 1.40 ± 0.52 |
| Groups | Vertical Deviation (mm) | Angular Deviation (°) | Platform Deviation (mm) | Apex Deviation (mm) | |
|---|---|---|---|---|---|
| VG surgery group | Overall (experts + beginners) | 0.95, 0.71 (−0.60, 1.30) | 3.49, 3.62 (2.73, 4.25) | 1.37, 1.01 (0.95, 1.79) | 1.68, 1.41 (1.28, 2.08) |
| Expert group (N = 10) | 1.12, 1.24 (0.64, 1.60) | 3.64, 3.86 (2.70, 4.58) | 1.48, 1.47 (0.96, 2.01) | 1.81, 1.77 (1.34, 2.29) | |
| Beginner group (N = 10) | 0.78, 0.51 (0.27, 1.29) | 3.34, 2.97 (2.11, 4.58) | 1.25, 0.98 (0.58, 1.93) | 1.54, 1.36 (0.89, 2.20) | |
| NG surgery group | Overall (experts + beginners) | 0.64, 0.44 (0.40, 0.88) | 3.04, 2.69 (2.19, 3.90) | 0.95, 0.78 (0.75, 1.14) | 1.34, 1.25 (1.08, 1.60) |
| Expert group (N = 10) | 0.75, 0.62 (0.36, 1.15) | 3.72, 3.64 (2.66, 4.78) | 1.12, 1.01 (0.83, 1.42) | 1.62, 1.92 (1.30, 1.93) | |
| Beginner group (N = 10) | 0.52, 0.33 (0.26, 0.79) | 2.37, 1.71 (1.12, 3.62) | 0.78, 0.66 (0.55, 1.00) | 1.07, 1.02 (0.72, 1.42) |
| Groups | Total Time (min) | Presurgical Preparation Time (min) | Surgery Time (min) | |
|---|---|---|---|---|
| VG surgery group | Overall (experts + beginners) | 26.33, 28.58 (23.57, 29.10) | 19.63, 20.93 (17.52, 21.75) | 6.70, 7.07 (5.70, 7.68) |
| Expert group (N = 10) | 28.30, 29.37 (24.27, 32.33) | 21.68, 22.80 (19.00, 24.35) | 6.62, 7.40 (5.10, 8.15) | |
| Beginner group (N = 10) | 24.37, 25.55 (20.82, 27.92) | 17.06, 16.75 (14.72, 20.48) + | 6.77, 6.13 (5.42, 8.12) | |
| NG surgery group | Overall (experts + beginners) | 378.83, 379.35 (376.57, 381.10) * | 372.93, 372.95 (371.07, 374.78) * | 5.90, 5.88 (4.97, 6.83) |
| Expert group (N = 10) | 376.68, 377.00 (373.85, 379.52) * | 371.88, 371.72 (369.40, 374.37) * | 4.80, 4.92 (3.68, 5.92) | |
| Beginner group (N = 10) | 380.98, 380.93 (377.88, 384.08) * | 373.97, 374.92 (371.25, 376.70) * | 7.02, 6.57 (5.83, 8.18) + |
| Groups | Curing/Scanning Time (min) | Virtual Planning Time (min) | Guide Fabrication and Delivery Time (min) | |
|---|---|---|---|---|
| VG surgery group | Overall (experts + beginners) | 3.22, 3.40 (2.83, 3.58) | 5.68, 5.73 (4.53, 6.82) | 10.75, 12.07 (9.63, 11.87) |
| Expert group (N = 10) | 2.97, 3.30 (2.47, 3.45) | 7.58, 7.88 (6.33, 8.83) | 11.13, 12.10 (9.66, 12.60) | |
| Beginner group (N = 10) | 3.47, 3.40 (2.93, 4.00) | 3.78, 3.28 (2.85, 4.72) + | 10.37, 10.87 (8.63, 12.08) | |
| NG surgery group | Overall (experts + beginners) | 3.42, 3.10 (2.97, 3.87) | 9.52, 8.30 (7.68, 11.35) * | 360.00, 360.00 (360.00, 360.00) a,* |
| Expert group (N = 10) | 3.75, 3.68 (2.95, 4.55) | 8.13, 7.66 (5.75, 10.52) | ||
| Beginner group (N = 10) | 3.08, 3.10 (2.73, 3.42) | 10.90, 11.73 (8.27, 13.53) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Y.W.; Kim, J.; Kim, J.-H.; Park, J.-M.; Jung, U.-W.; Cha, J.-K. Accuracy of Dental Implant Placement by a Novel In-House Model-Free and Zero-Setup Fully Guided Surgical Template Made of a Light-Cured Composite Resin (VARO Guide®): A Comparative In Vitro Study. Materials 2021, 14, 4023. https://doi.org/10.3390/ma14144023
Song YW, Kim J, Kim J-H, Park J-M, Jung U-W, Cha J-K. Accuracy of Dental Implant Placement by a Novel In-House Model-Free and Zero-Setup Fully Guided Surgical Template Made of a Light-Cured Composite Resin (VARO Guide®): A Comparative In Vitro Study. Materials. 2021; 14(14):4023. https://doi.org/10.3390/ma14144023
Chicago/Turabian StyleSong, Young Woo, Jongseung Kim, Jang-Hyun Kim, Ji-Man Park, Ui-Won Jung, and Jae-Kook Cha. 2021. "Accuracy of Dental Implant Placement by a Novel In-House Model-Free and Zero-Setup Fully Guided Surgical Template Made of a Light-Cured Composite Resin (VARO Guide®): A Comparative In Vitro Study" Materials 14, no. 14: 4023. https://doi.org/10.3390/ma14144023
APA StyleSong, Y. W., Kim, J., Kim, J.-H., Park, J.-M., Jung, U.-W., & Cha, J.-K. (2021). Accuracy of Dental Implant Placement by a Novel In-House Model-Free and Zero-Setup Fully Guided Surgical Template Made of a Light-Cured Composite Resin (VARO Guide®): A Comparative In Vitro Study. Materials, 14(14), 4023. https://doi.org/10.3390/ma14144023