
The Potential of Stereolithography for 3D Printing of Synthetic Trabecular Bone Structures



Abstract
:1. Introduction
- To acquire data on the suitability of SLA technology for the intended application.
- To evaluate replicability in trabecular spacing, thickness and total porosity, with micro-computed tomography (micro-CT) analysis.
- To evaluate mechanical properties with compression testing and screw pull-out tests.
2. Materials and Methods
2.1. SLA Printing
2.2. Mechanical Testing
2.2.1. Compression Tests
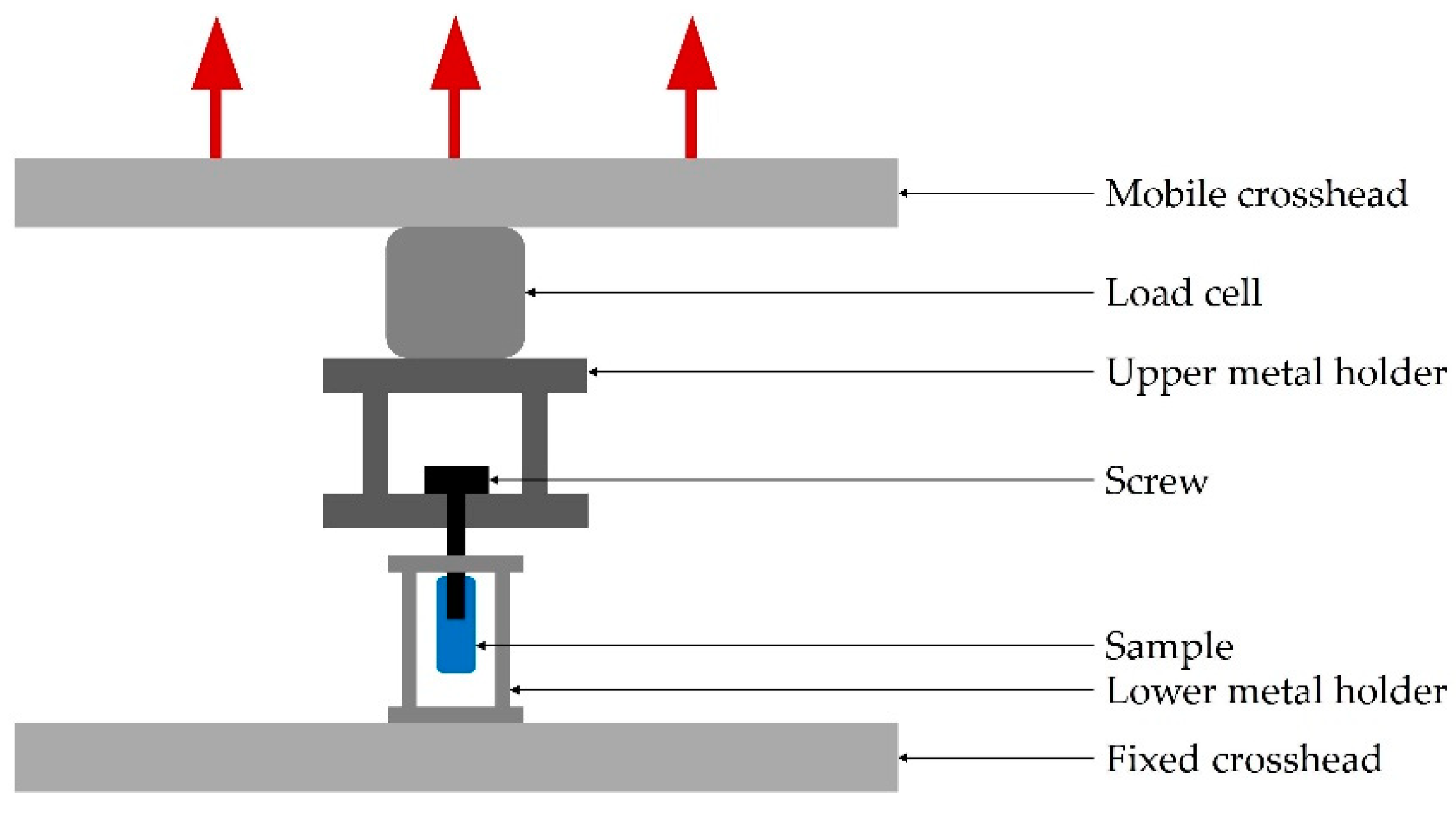
2.2.2. Pull-Out Tests
2.2.3. Statistical Analysis
2.3. Morphological Evaluation by Micro-CT
3. Results and Discussion
3.1. Mechanical Testing
3.1.1. Compression Tests
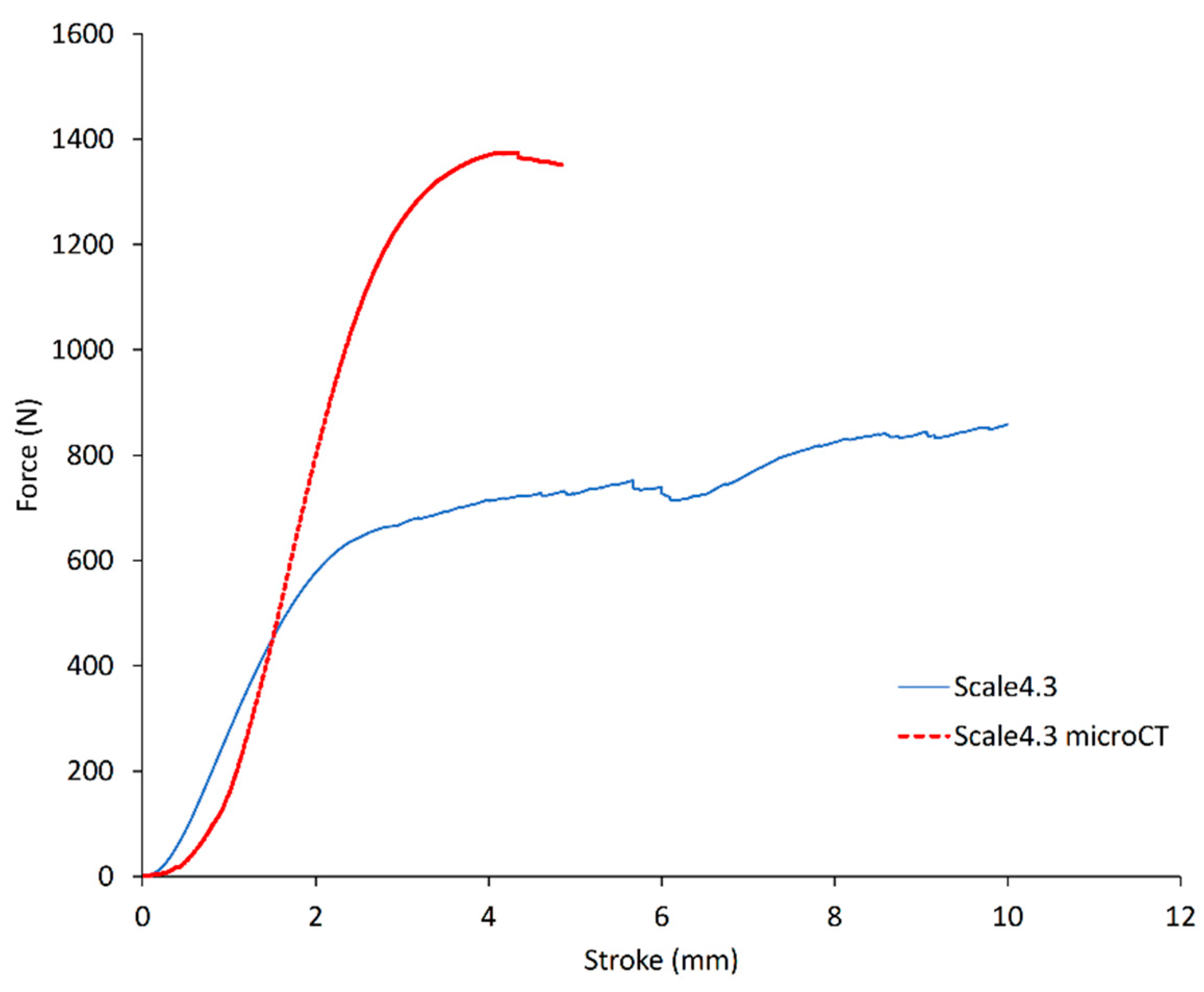
3.1.2. Pull-out Tests
3.2. Morphological Evaluation by Micro-CT
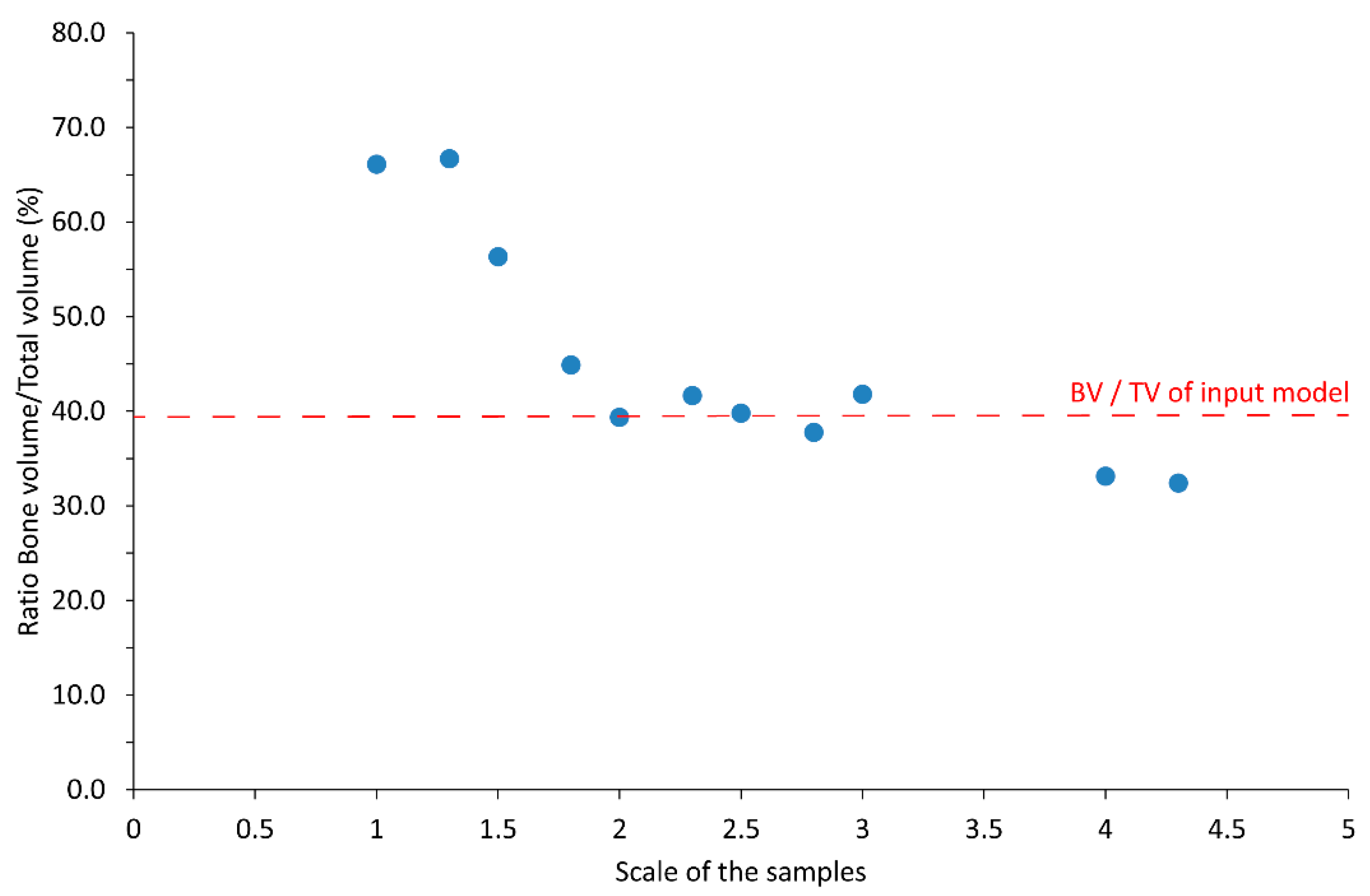
3.2.1. Bone Fraction Measured with Micro-CT
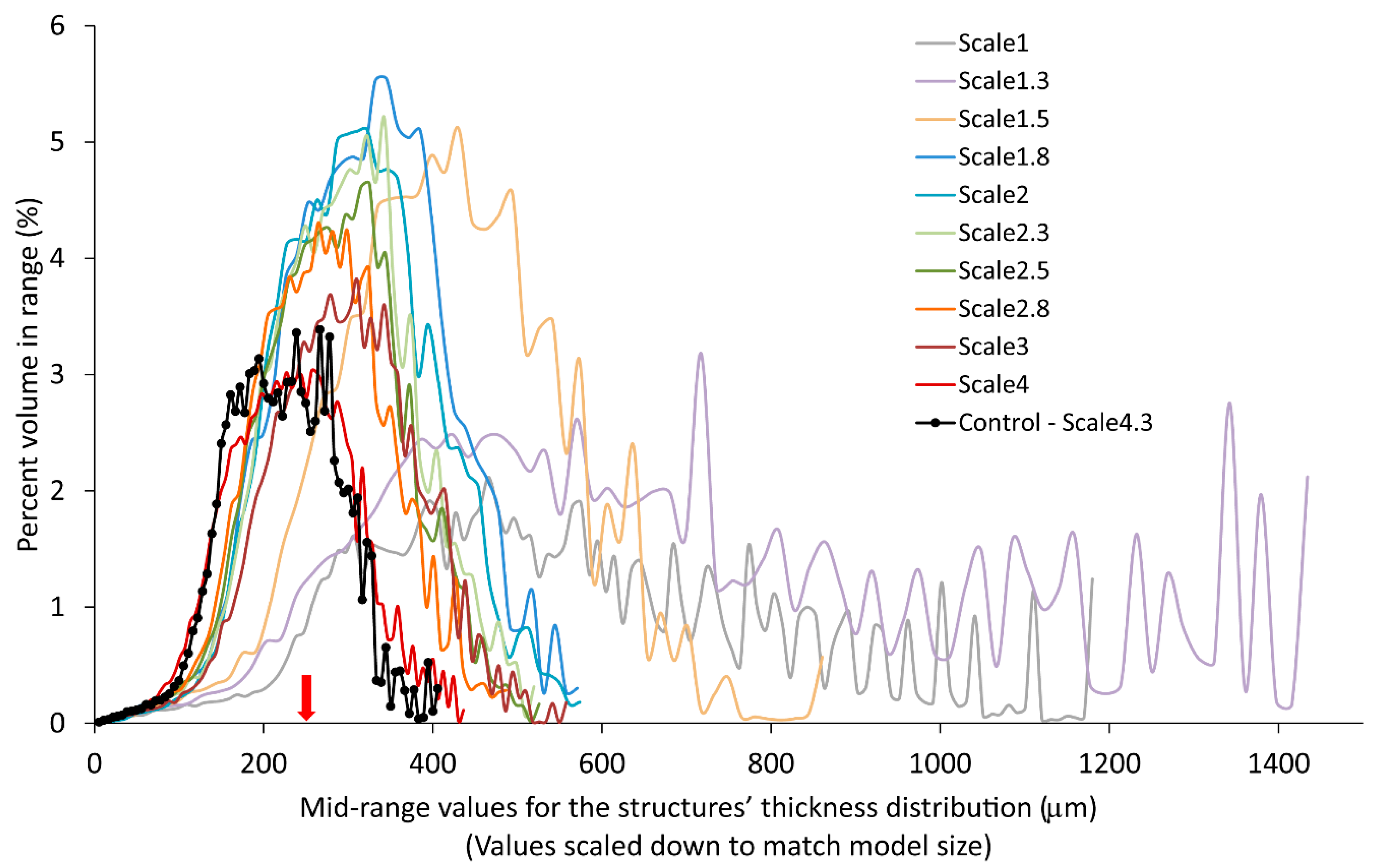
3.2.2. Trabecular Thickness Distribution
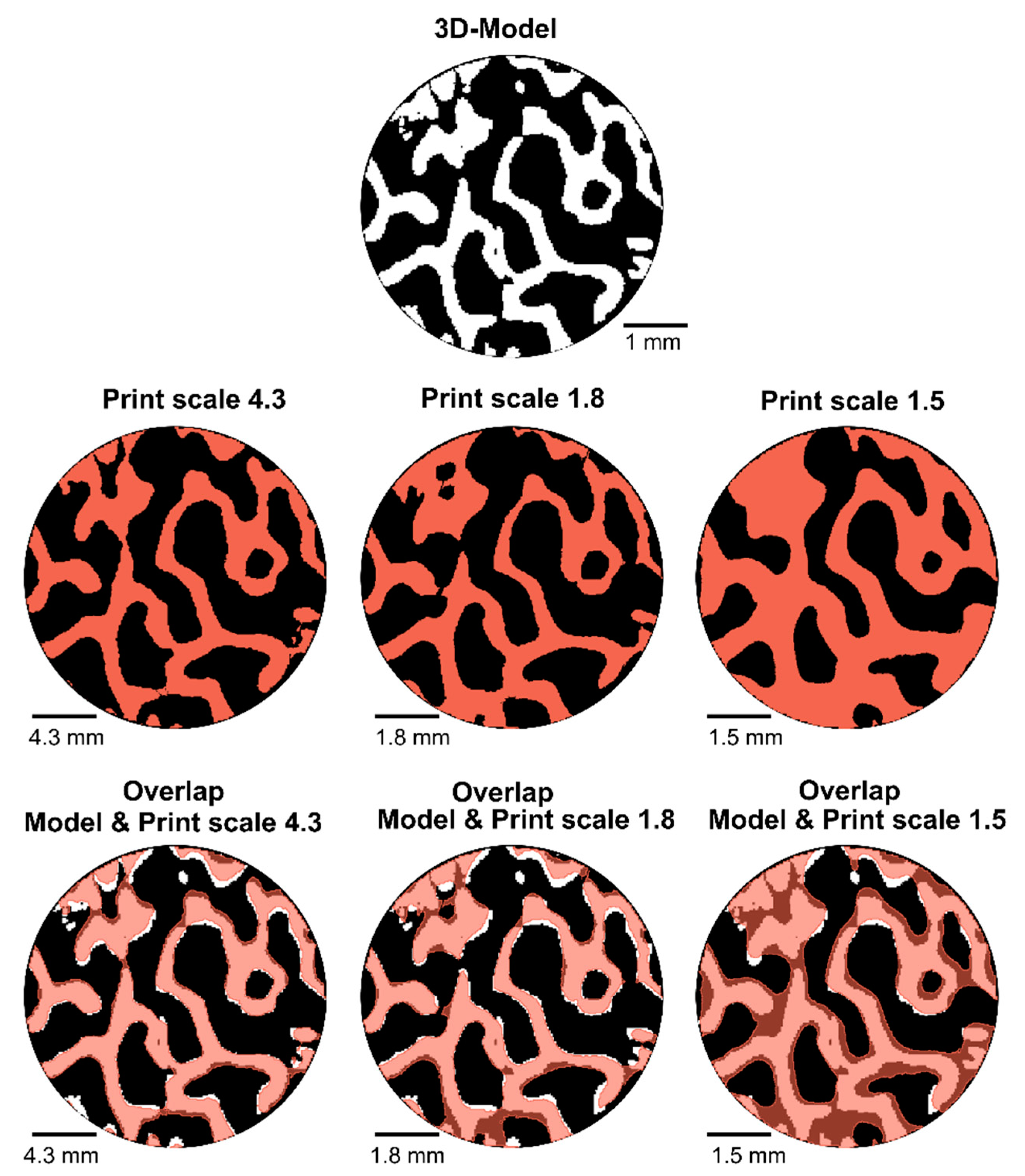
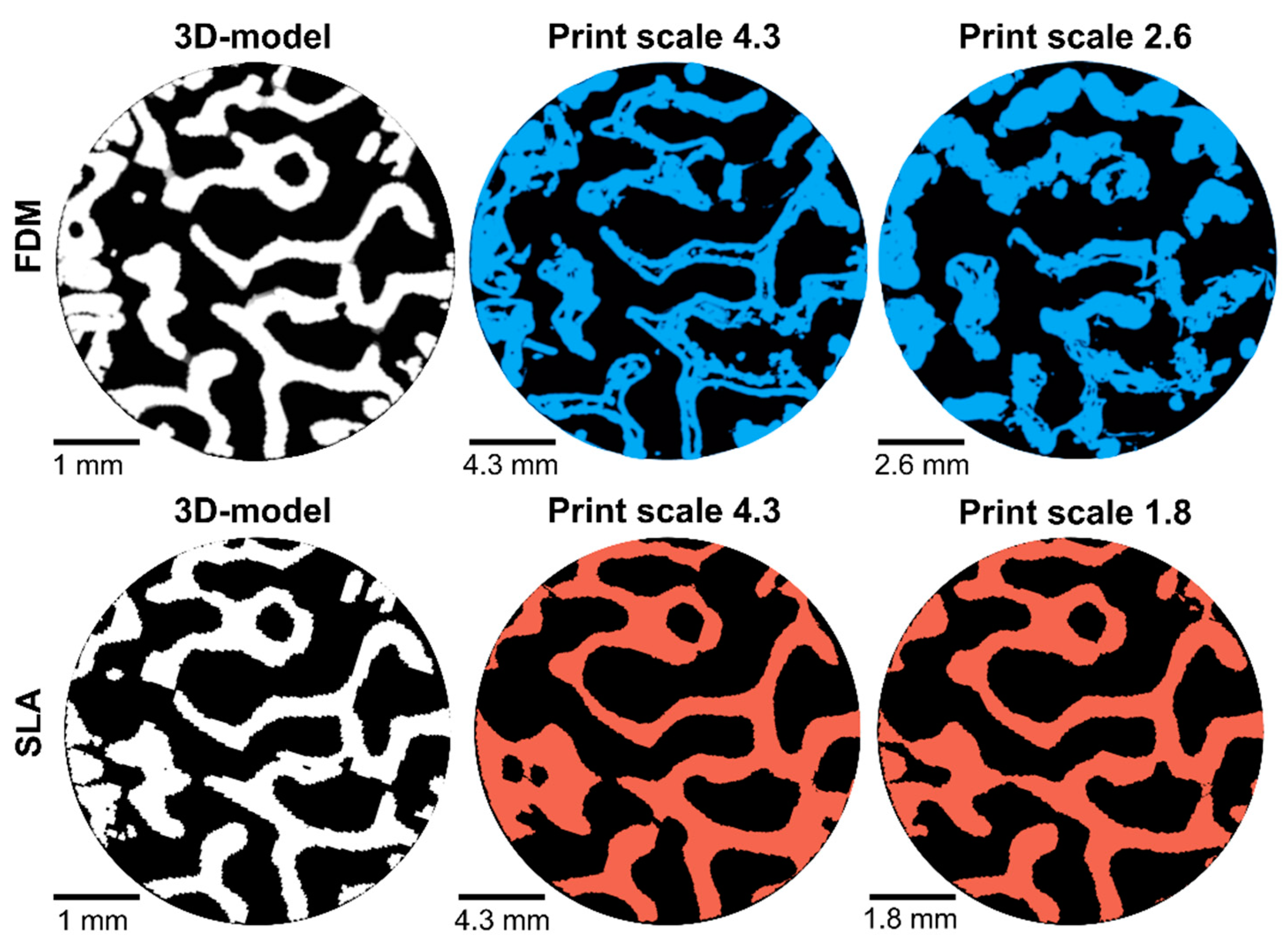
3.2.3. Volumetric Comparison
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Facts and Figures. 2005. Available online: https://hcup-us.ahrq.gov/reports/factsandfigures/facts_figures_2005.jsp#ex3_6c (accessed on 5 April 2021).
- Burkhard, M.; Fürnstahl, P.; Farshad, M. Three-dimensionally printed vertebrae with different bone densities for surgical training. Eur. Spine J. 2019, 28, 798–806. [Google Scholar] [CrossRef]
- Gilbody, J.; Prasthofer, A.; Ho, K.; Costa, M. The use and effectiveness of cadaveric workshops in higher surgical training: A systematic review. Ann. R. Coll. Surg. Engl. 2011, 93, 347–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burr, D.B. Chapter 1—Bone Morphology and Organization. In Basic and Applied Bone Biology, 2nd ed.; Burr, D.B., Allen, M.R., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 3–26. ISBN 978-0-12-813259-3. [Google Scholar]
- Cristofolini, L.; Viceconti, M. Mechanical validation of whole bone composite tibia models. J. Biomech. 2000, 33, 279–288. [Google Scholar] [CrossRef]
- Patel, P.S.; Shepherd, D.E.; Hukins, D.W. Compressive properties of commercially available polyurethane foams as mechanical models for osteoporotic human cancellous bone. BMC Musculoskelet. Disord. 2008, 9, 137. [Google Scholar] [CrossRef] [Green Version]
- Ferdowsian, H.R.; Beck, N. Ethical and Scientific Considerations Regarding Animal Testing and Research. PLoS ONE 2011, 6, e24059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poukalova, M.; Yakacki, C.M.; Guldberg, R.E.; Lin, A.; Saing, M.; Gillogly, S.D.; Gall, K. Pullout Strength of Suture Anchors: Effect of Mechanical Properties of Trabecular Bone. J. Biomech. 2010, 43, 1138–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bose, S.; Vahabzadeh, S.; Bandyopadhyay, A. Bone tissue engineering using 3D printing. Mater. Today 2013, 16, 496–504. [Google Scholar] [CrossRef]
- Ng, W.L.; Chua, C.K.; Shen, Y.-F. Print Me An Organ! Why We Are Not There Yet. Prog. Polym. Sci. 2019, 97, 101145. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, G.; Liang, H.; Gao, C.; Peng, S.; Shen, L.; Shuai, C. Additive manufacturing of bone scaffolds. Int. J. Bioprinting 2018, 5, 148. [Google Scholar] [CrossRef]
- Alsheghri, A.; Reznikov, N.; Piché, N.; McKee, M.D.; Tamimi, F.; Song, J. Optimization of 3D network topology for bioinspired design of stiff and lightweight bone-like structures. Mater. Sci. Eng. C 2021, 123, 112010. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Spanou, A.; Diez-Escudero, A.; Persson, C. 3D-printed PLA/HA composite structures as synthetic trabecular bone: A feasibility study using fused deposition modeling. J. Mech. Behav. Biomed. Mater. 2020, 103, 103608. [Google Scholar] [CrossRef]
- Szymczyk-Ziółkowska, P.; Łabowska, M.B.; Detyna, J.; Michalak, I.; Gruber, P. A review of fabrication polymer scaffolds for biomedical applications using additive manufacturing techniques. Biocybern. Biomed. Eng. 2020, 40, 624–638. [Google Scholar] [CrossRef]
- Ng, W.L.; Lee, J.M.; Zhou, M.; Chen, Y.-W.; Lee, K.-X.A.; Yeong, W.Y.; Shen, Y.-F. Vat polymerization-based bioprinting—process, materials, applications and regulatory challenges. Biofabrication 2020, 12, 022001. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Mille, L.S.; Robledo, J.A.; Uribe, T.; Huerta, V.; Zhang, Y.S. Recent Advances in Formulating and Processing Biomaterial Inks for Vat Polymerization-Based 3D Printing. Adv. Healthc. Mater. 2020, 9, 2000156. [Google Scholar] [CrossRef]
- Chartrain, N.A.; Williams, C.B.; Whittington, A.R. A review on fabricating tissue scaffolds using vat photopolymerization. Acta Biomater. 2018, 74, 90–111. [Google Scholar] [CrossRef] [PubMed]
- Mézière, F.; Juskova, P.; Woittequand, J.; Muller, M.; Bossy, E.; Boistel, R.; Malaquin, L.; Derode, A. Experimental observation of ultrasound fast and slow waves through three-dimensional printed trabecular bone phantoms. J. Acoust. Soc. Am. 2016, 139, EL13–EL18. [Google Scholar] [CrossRef] [Green Version]
- Barak, M.M.; Black, M.A. A novel use of 3D printing model demonstrates the effects of deteriorated trabecular bone structure on bone stiffness and strength. J. Mech. Behav. Biomed. Mater. 2018, 78, 455–464. [Google Scholar] [CrossRef]
- Fernández-Cervantes, I.; Morales, M.A.; Agustín-Serrano, R.; Cardenas-García, M.; Pérez-Luna, P.V.; Arroyo-Reyes, B.L.; Maldonado-García, A. Polylactic acid/sodium alginate/hydroxyapatite composite scaffolds with trabecular tissue morphology designed by a bone remodeling model using 3D printing. J. Mater. Sci. 2019, 54, 9478–9496. [Google Scholar] [CrossRef]
- Milazzo, M.; Contessi Negrini, N.; Scialla, S.; Marelli, B.; Farè, S.; Danti, S.; Buehler, M.J. Additive Manufacturing Approaches for Hydroxyapatite-Reinforced Composites. Adv. Funct. Mater. 2019, 29, 1903055. [Google Scholar] [CrossRef] [Green Version]
- Black_Resin_SDS_EU.pdf. Available online: https://archive-media.formlabs.com/upload/Black_Resin_SDS_EU.pdf (accessed on 14 June 2020).
- Materials-Technical-Library FORMLABS.pdf. Available online: https://formlabs-media.formlabs.com/filer_public/ac/89/ac8963db-f54a-4cac-8fe9-fb740a7b06f1/formlabs-materials-library.pdf (accessed on 14 June 2020).
- SLA 3D Printing Materials Compared. Available online: https://www.3dhubs.com/knowledge-base/sla-3d-printing-materials-compared/ (accessed on 31 May 2020).
- ISO 5833:2002(en), Implants for Surgery—Acrylic Resin Cements. Available online: https://www.iso.org/obp/ui/#iso:std:iso:5833:ed-2:v1:en (accessed on 31 May 2021).
- Ridler, T.W.; Calvard, S. Picture Thresholding Using an Iterative Slection Method. IEEE Trans. Syst. Man Cybern. 1978, SMC-8, 630–632. [Google Scholar]
- Hildebrand, T.; Rüegsegger, P. A new method for the model-independent assessment of thickness in three-dimensional images. J. Microsc. 1997, 185, 67–75. [Google Scholar] [CrossRef]
- 3D Slicer. Available online: https://www.slicer.org/ (accessed on 26 September 2020).
- Coffey, T.; Urquhart, S.G.; Ade, H. Characterization of the effects of soft X-ray irradiation on polymers. J. Electron Spectrosc. Relat. Phenom. 2002, 122, 65–78. [Google Scholar] [CrossRef]
- Alexander, P.; Fox, M. The degradation of polymethacrylic acid by X-rays. Trans. Faraday Soc. 1954, 50, 605–612. [Google Scholar] [CrossRef]
- Chapman, J.R.; Harrington, R.M.; Lee, K.M.; Anderson, P.A.; Tencer, A.F.; Kowalski, D. Factors Affecting the Pullout Strength of Cancellous Bone Screws. J. Biomech. Eng. 1996, 118, 391–398. [Google Scholar] [CrossRef]
- Shea, T.M.; Doulgeris, J.J.; Gonzalez-Blohm, S.A.; Lee, W.E.; Aghayev, K.; Vrionis, F.D. Balancing Rigidity and Safety of Pedicle Screw Fixation via a Novel Expansion Mechanism in a Severely Osteoporotic Model. BioMed Res. Int. 2015, 2015, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Mueller, T.L.; Basler, S.E.; Müller, R.; van Lenthe, G.H. Time-lapsed imaging of implant fixation failure in human femoral heads. Med. Eng. Phys. 2013, 35, 636–643. [Google Scholar] [CrossRef]
- Wu, D.; Pujari-Palmer, M.; Bojan, A.; Palmquist, A.; Procter, P.; Öhman-Mägi, C.; Ferguson, S.J.; Isaksson, P.; Persson, C. The effect of two types of resorbable augmentation materials—A cement and an adhesive—On the screw pullout pullout resistance in human trabecular bone. J. Mech. Behav. Biomed. Mater. 2020, 110, 103897. [Google Scholar] [CrossRef] [PubMed]
- Pujari-Palmer, M.; Robo, C.; Persson, C.; Procter, P.; Engqvist, H. Influence of cement compressive strength and porosity on augmentation performance in a model of orthopedic screw pull-out. J. Mech. Behav. Biomed. Mater. 2018, 77, 624–633. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bone Type | Porosity (%) | Compressive Strength (MPa) | Elastic Modulus (GPa) |
|---|---|---|---|
| Fernandez-Cervantes et al. [20] | Milazzo et al. [21] | Milazzo et al. [21] | |
| Cortical | <10 | 130–180 | 12–18 |
| Trabecular | 50–90 | 4–12 | 0.1–0.5 |
| Formlabs Resin | Elastic Modulus for “Green” Parts (GPa) | Elastic Modulus for “Cured” Parts (GPa) |
|---|---|---|
| Black | 1.6 | 2.8 |
| GreyPro | 1.4 | 2.6 |
| Durable | 0.45 | 1.26 |
| Resin | Recommended Cure Time (min) | Recommended Cure Temperature (°C) |
|---|---|---|
| Black | 30 | 60 |
| GreyPro | 15 | 80 |
| Durable | 60 | 60 |
| Resin | Scale Factor | Number of Specimens Scanned |
|---|---|---|
| Black | 1 | 1 |
| 1.3 | 2 | |
| 1.5 | 2 | |
| 1.8 | 2 | |
| 2 | 1 | |
| 2.3 | 1 | |
| 2.5 | 1 | |
| 2.8 | 1 | |
| 3 | 1 | |
| 4 | 1 horizontally printed 1 vertically printed | |
| 4.3 | 4 |
| Study | Samples | Stiffness (N/mm) | Pull-Out Strength (N) |
|---|---|---|---|
| Present study Printed by SLA | Black resin | 819.3 ± 127.8 | 755.6 ± 146.8 |
| Wu et al. [13] Printed by FDM | Pure poly(lactic acid) (PLA) | 931.1 ± 82.3 | 1369.7 ± 32.9 |
| PLA + 5% hydroxyapatite (HA) | 1295.2 ± 283.3 | 1657 ± 446.9 | |
| PLA + 10% HA | 1374.7 ± 140.1 | 1891.3 ± 223.8 | |
| PLA + 15% HA | 1374.6 ± 514.8 | 1555 ± 613.3 |
| Study | Material | Insertion Depth (mm) | Screw Diameter (mm) | Pull-out Strength (N) | Scaled Pull-Out Strength (N) |
|---|---|---|---|---|---|
| Present study | SLA-printed resin | 20 | 6.7 | 755.6 ± 146.8 | 755.6 ± 146.8 |
| Shea et al., 2015 [32] | Sawbones ™, density 0.08 g/cm³ | 45 | 6.5 | 393 ± 9 | 147 ± 4 |
| Mueller et al., 2013 [33] | Sawbones ™, density 0.16–0.32 g/cm³ | 22 | 12.5 | 700–2500 | 305–1127 |
| Mueller et al., 2013 [33] | Human femoral head (screw pushed inwards in the specimen) | 22 | 12.5 | 2489–4347 | 1176–2055 |
| Wu et al., 2020 [34] | Human femoral head | 9 | 4 | 314–635 | 1134–2293 |
| Wu et al., 2020 [13] | 3D-printed PLA/HA | 20 | 6.5 | 1400–1900 | 1400–1900 |
| Sample | Difference to Model in Total Volume (%) |
|---|---|
| Scale 4.3 | 6.1% |
| Scale 1.8 | 8.9% |
| Scale 1.5 | 53.6% |
| Sample | Underfilling (%) Volume Percentage of the Model that Was Not Printed | Overfilling (%) Volume Percentage of the Printed Part that Was Not in the Original Model (Extra Volume) |
|---|---|---|
| Scale 4.3 | 11 | 15 |
| Scale 1.8 | 23 | 22 |
| Scale 1.5 | 5 | 59 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grzeszczak, A.; Lewin, S.; Eriksson, O.; Kreuger, J.; Persson, C. The Potential of Stereolithography for 3D Printing of Synthetic Trabecular Bone Structures. Materials 2021, 14, 3712. https://doi.org/10.3390/ma14133712
Grzeszczak A, Lewin S, Eriksson O, Kreuger J, Persson C. The Potential of Stereolithography for 3D Printing of Synthetic Trabecular Bone Structures. Materials. 2021; 14(13):3712. https://doi.org/10.3390/ma14133712
Chicago/Turabian StyleGrzeszczak, Ana, Susanne Lewin, Olle Eriksson, Johan Kreuger, and Cecilia Persson. 2021. "The Potential of Stereolithography for 3D Printing of Synthetic Trabecular Bone Structures" Materials 14, no. 13: 3712. https://doi.org/10.3390/ma14133712
APA StyleGrzeszczak, A., Lewin, S., Eriksson, O., Kreuger, J., & Persson, C. (2021). The Potential of Stereolithography for 3D Printing of Synthetic Trabecular Bone Structures. Materials, 14(13), 3712. https://doi.org/10.3390/ma14133712