A Comparative Analysis of Implants Presenting Different Diameters: Extra-Narrow, Narrow and Conventional

 ,
,  , and
, and
Abstract
1. Introduction
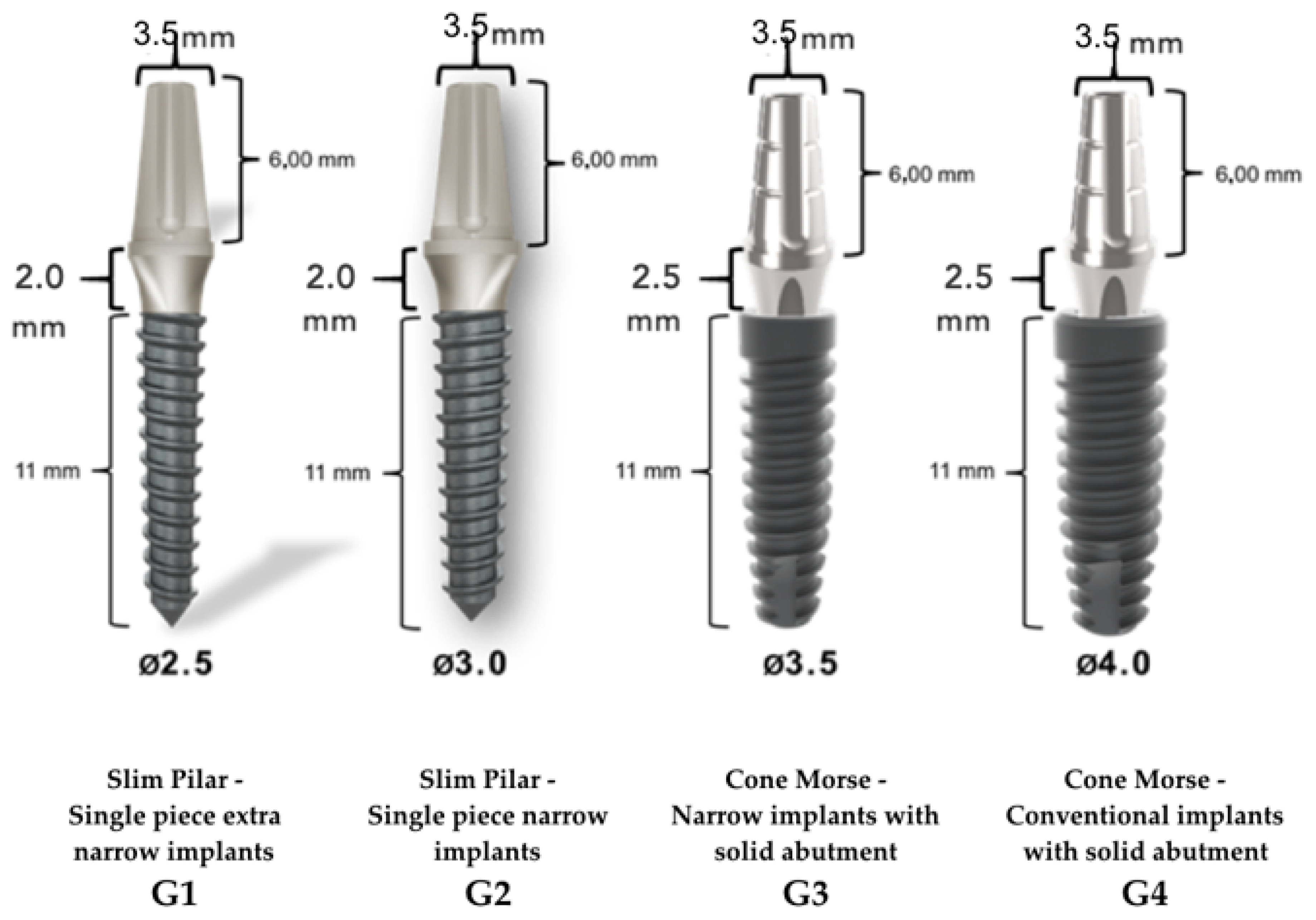
2. Materials and Methods
3. Results
3.1. Descriptive Statistics and Data Analysis
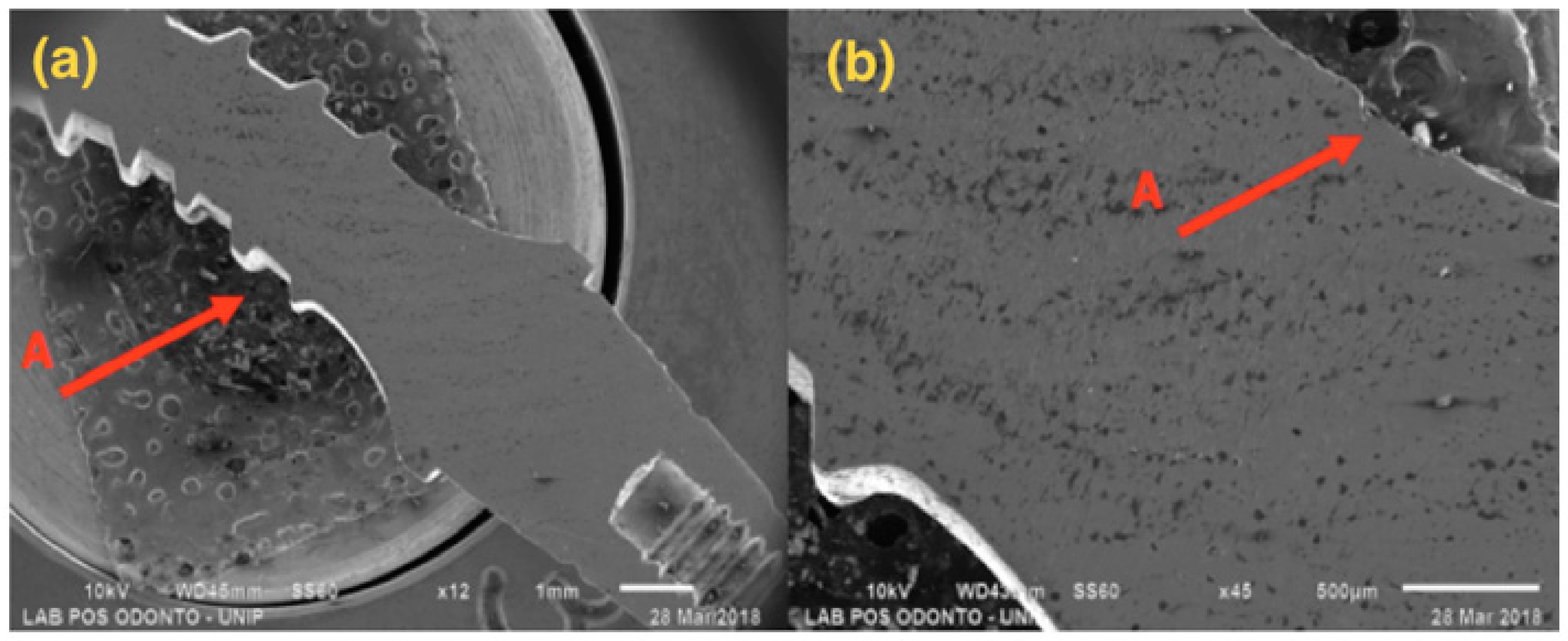
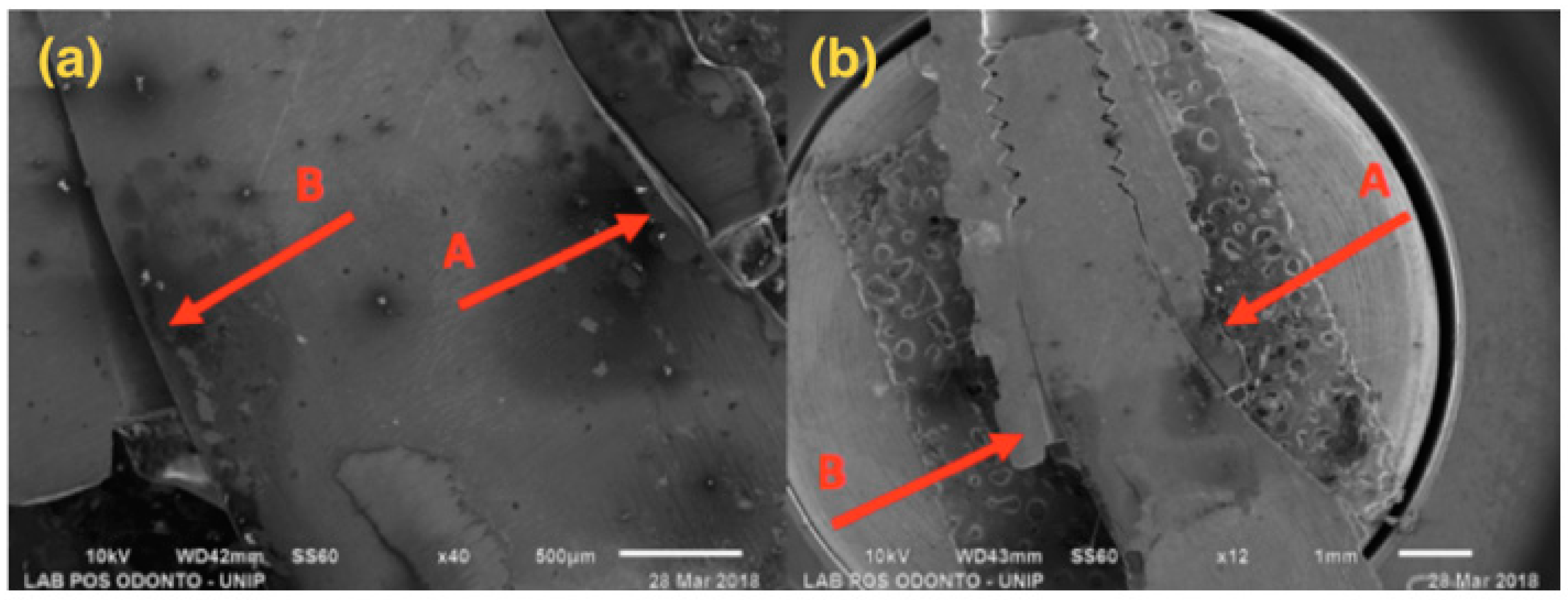
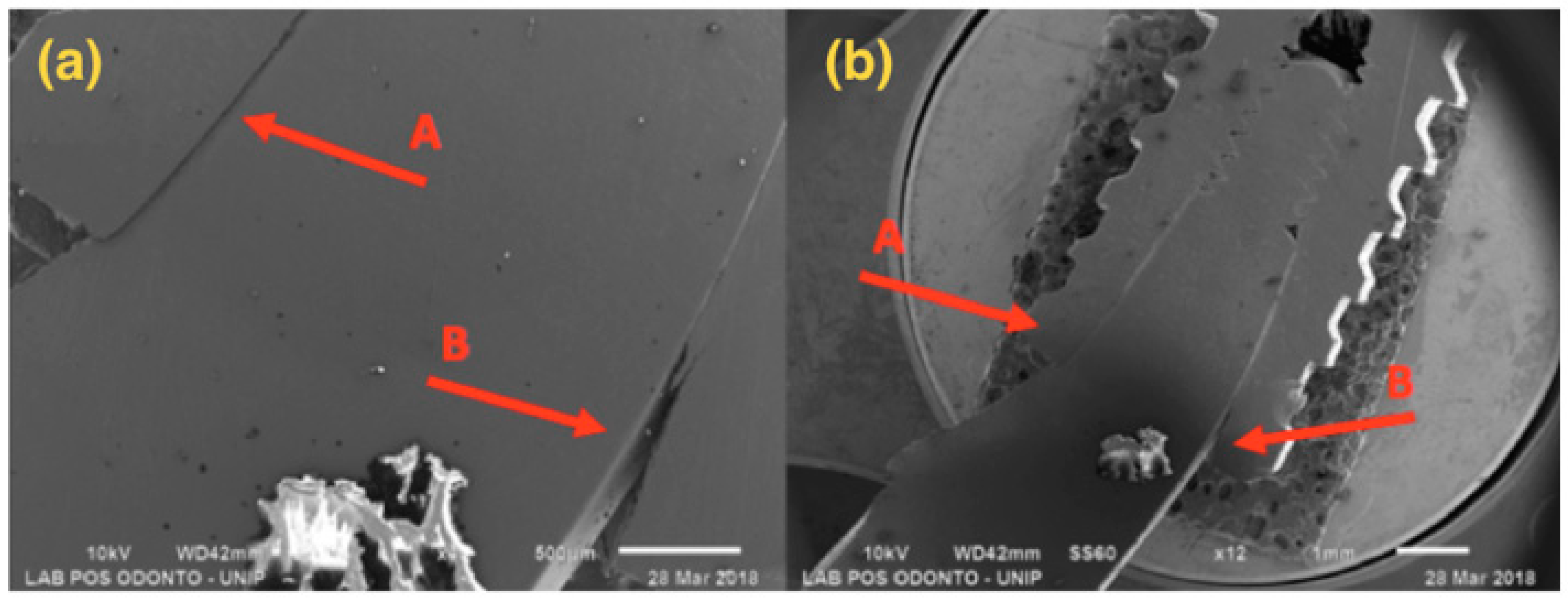
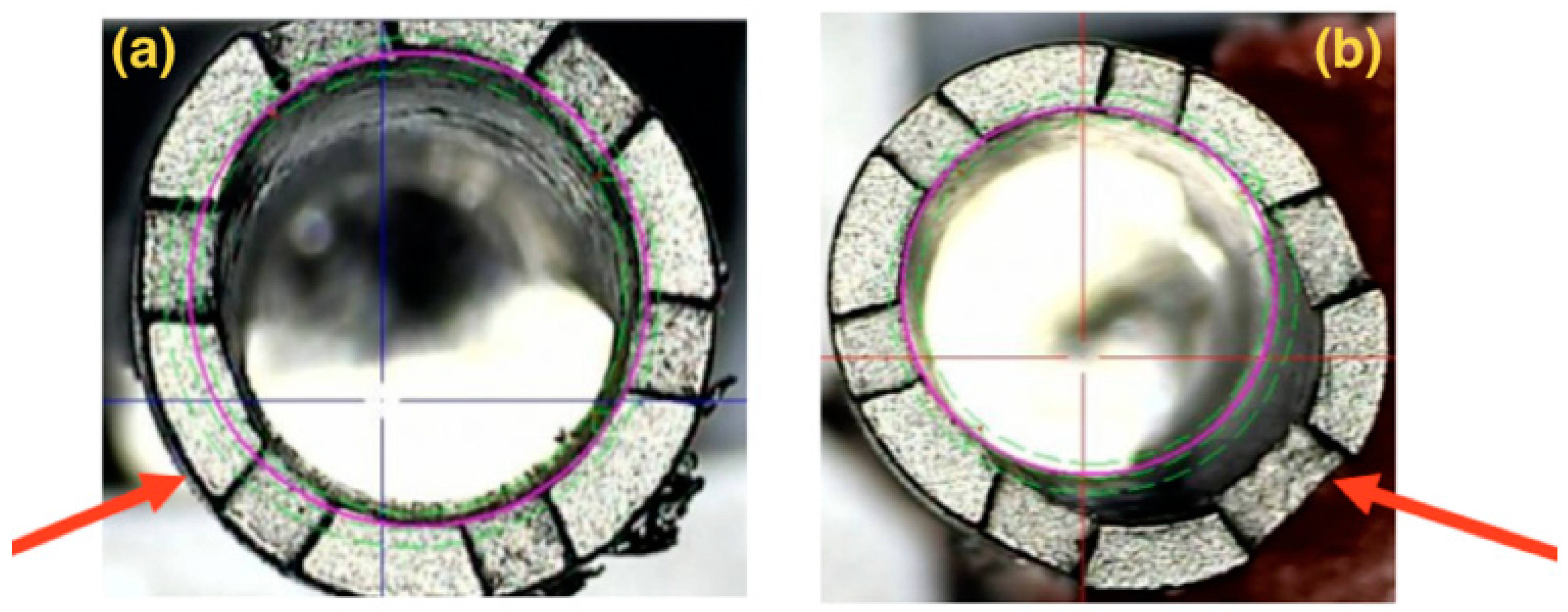
3.2. Scanning Electron Microscopy (SEM)
3.3. Profilometer
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bourauel, C.; Aitlahrach, M.; Heinemann, F.; Hasan, I. Biomechanical finite element analysis of small diameter and short dental implants: Extensive study of commercial implants. Biomed. Tech. 2012, 57, 21–32. [Google Scholar]
- Toyoshima, Y.; Wakabayashi, N. Load limit of mini-implants with reduced abutment height based on fatigue fracture resistance: Experimental and finite element study. Int. J. Oral Maxillofac. Implants 2015, 30, e10–e16. [Google Scholar] [PubMed]
- Pieri, F.; Siroli, L.; Forlivesi, C.; Corinaldesi, G. Clinical, esthetic, and radiographic evaluation of small-diameter (3.0-mm) implants supporting single crowns in the anterior region: A 3-year prospective study. Int. J. Periodontics Restor. Dent. 2014, 34, 825–832. [Google Scholar]
- Klein, M.O.; Schiegnitz, E.; Al-Nawas, B. Systematic review on success of narrow-diameter dental implants. Int. J. Oral Maxillofac. Implants 2014, 29, 43–54. [Google Scholar]
- Andersen, E.; Saxegaard, E.; Knutsen, B.M.; Haanæs, H.R. A prospective clinical study evaluating the safety and effectiveness of narrow-diameter threaded implants in the anterior region of the maxilla. Int. J. Oral Maxillofac. Implants 2001, 16, 217–224. [Google Scholar]
- Zinsli, B.; Sagesser, T.; Mericske, E.; Mericske-Stern, R. Clinical evaluation of small-diameter ITI implants: A prospective study. Int. J. Oral Maxillofac. Implants 2004, 19, 92–99. [Google Scholar]
- Al-Johany, S.S.; Al Amri, M.D.; Alsaeed, S.; Alalola, B. Dental Implant Length and Diameter: A Proposed Classification Scheme. J. Prosthodont. 2017, 26, 252–260. [Google Scholar]
- Allum, S.R.; Tomlinson, R.A.; Joshi, R. The impact of loads on standard diameter, small diameter and mini implants: A comparative laboratory study. Clin. Oral Implants Res. 2008, 19, 553–559. [Google Scholar]
- Gealh, W.C.; Mazzo, V.; Barbi, F.; Camarini, E.T. Osseointegrated implant fracture: Causes and treatment. J. Oral Implantol. 2011, 37, 499–503. [Google Scholar]
- Berglundh, T.; Persson, L.; Klinge, B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J. Clin. Periodontol. 2002, 29 (Suppl. 3), 197–212. [Google Scholar]
- Eckert, S.E.; Meraw, S.J.; Cal, E.; Ow, R.K. Analysis of incidence and associated factors with fractured implants: A retrospective study. Int. J. Oral Maxillofac. Implants 2000, 15, 662–667. [Google Scholar] [PubMed]
- Renouard, F.; Rangert, B. Risk Factors in Implant Dentistry: Simplified Clinical Analysis for Predictable Treatment; Quintessence Publishing Company: New Malden, UK, 1999. [Google Scholar]
- Polizzi, G.; Fabbro, S.; Furri, M.; Herrmann, I.; Squarzoni, S. Clinical application of narrow Brånemark System implants for single-tooth restorations. Int. J. Oral Maxillofac. Implants 1999, 14, 496–503. [Google Scholar] [PubMed]
- Rangert, B.; Krogh, P.H.; Langer, B.; Van Roekel, N. Bending overload and implant fracture: A retrospective clinical analysis. Int. J. Oral Maxillofac. Implants 1995, 10, 326–334. [Google Scholar] [PubMed]
- Anitua, E.; Saracho, J.; Begoña, L.; Alkhraisat, M.H. Long-term follow-up of 2.5-mm narrow-diameter implants supporting a fixed prostheses. Clin. Implant Dent. Relat. Res. 2016, 18, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Dentistry-Implants, Dynamic Fatigue Test for Endosseous Dental Implants. Available online: https://www.iso.org/standard/41034.html (accessed on 11 February 2019).
- Alexandre Gehrke, S.; Delgado-Ruiz, R.A.; Prados Frutos, J.C.; Prados-Privado, M.; Anina Dedavid, B.; Granero Marín, J.M.; Calvo Guirado, J.L. Misfit of Three Different Implant-Abutment Connections Before and After Cyclic Load Application: An In vitro Study. Int. J. Oral Maxillofac. Implants 2017, 32, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Shemtov-Yona, K.; Rittel, D.; Levin, L.; Machtei, E.E. The effect of oral-like environment on dental implants’ fatigue performance. Clin. Oral Implants Res. 2014, 25, e166–e170. [Google Scholar] [CrossRef]
- Almeida, E.O.; Freitas, A.C., Jr.; Bonfante, E.A.; Marotta, L.; Silva, N.R.; Coelho, P.G. Mechanical testing of implant-supported anterior crowns with different implant/abutment connections. Int. J. Oral. Maxillofac. Implant 2013, 28, 103–108. [Google Scholar] [CrossRef]
- Bonfante, E.A.; Almeida, E.O.; Lorenzoni, F.C.; Coelho, P.G. Effects of implant diameter and prosthesis retention system on the reliability of single crowns. Int. J. Oral. Maxillofac. Implant 2015, 30, 95–101. [Google Scholar] [CrossRef]
- Freitas-Júnior, A.C.; Rocha, E.P.; Bonfante, E.A.; Almeida, E.O.; Anchieta, R.B.; Martini, A.P.; Coelho, P.G. Biomechanical evaluation of internal and external hexagon platform switched implant-abutment connections: An in vitro laboratory and three-dimensional finite element analysis. Dent. Mater. 2012, 28, e218–e228. [Google Scholar] [CrossRef]
- Machado, L.S.; Bonfante, E.A.; Anchieta, R.B.; Yamaguchi, S.; Coelho, P.G. Implant-abutment connection designs for anterior crowns: Reliability and failure modes. Implant Dent. 2013, 22, 540–545. [Google Scholar] [CrossRef]
- Galindo-Moreno, P.; Nilsson, P.; King, P.; Worsaae, N.; Schramm, A.; Padial-Molina, M.; Maiorana, C. Clinical and radiographic evaluation of early loaded narrow-diameter implants: 5-year follow-up of a multicenter prospective clinical study. Clin. Oral Implants Res. 2017, 12, 1584–1591. [Google Scholar] [CrossRef] [PubMed]
- Regalo, S.C.H.; Santos, C.M.; Vitti, M.; Regalo, C.A.; de Vasconcelos, P.B.; Mestriner Jr, W.; Siéssere, S. Evaluation of molar and incisor bite force in indigenous compared with white population in Brazil. Arch. Oral Biol. 2008, 53, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Sadrimanesh, R.; Siadat, H.; Sadr-Eshkevari, P.; Monzavi, A.; Maurer, P.; Rashad, A. Alveolar bone stress around implants with different abutment angulation: An FE-analysis of anterior maxilla. Implant Dent. 2012, 21, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.D.B.; Pfeifer, A.B.; Silva, M.R.P.; Sendyk, C.L.; Sendyk, W.R. Fracture of abutment screw supporting a cemented implant-retained prosthesis with external hexagon connection: A case report with sem evaluation. J. Appl. Oral Sci. 2007, 15, 148–151. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Freitas, G.P.; Hirata, R.; Bonfante, E.A.; Tovar, N.; Coelho, P.G. Survival Probability of Narrow and Standard-Diameter Implants with Different Implant-Abutment Connection Designs. Int. J. Prosthodont. 2016, 29, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Binon, P.P. Evaluation of machining accuracy and consistency of selected implants, standard abutments, and laboratory analogs. Int. J. Prosthodont. 1995, 8, 162–178. [Google Scholar]
- Bordin, D.; Witek, L.; Fardin, V.P.; Bonfante, E.A.; Coelho, P.G. Fatigue failure of narrow implants with different implant-abutment connection designs. J. Prosthodont. 2018, 27, 659–664. [Google Scholar] [CrossRef]
- Prados-Privado, M.; Bea, J.A.; Rojo, R.; Gehrke, S.A.; Calvo-Guirado, J.L.; Prados-Frutos, J.C. New Model to Study Fatigue in Dental Implants Based on Probabilistic Finite Elements and Cumulative Damage Model. Appl Bionics Biomech. 2017, 2017, 5. [Google Scholar] [CrossRef]
- Gherlone, E.F.; Capparé, P.; Pasciuta, R.; Grusovin, M.G.; Mancini, N.; Burioni, R. Evaluation of resistance against bacterial microleakage of a new conical implant-abutment connection versus conventional connections: An in vitro study. New Microbiol. 2016, 39, 49–56. [Google Scholar]
- Gastaldi, G.; Vinci, R.; Ferrini, F.; Giorgio, G.; Capparé, P. Immediate versus delayed loading of a new conical connection implant in the esthetic zone: A randomized study with 2-year follow-up. J Osseointegr. 2017, 9, 271–275. [Google Scholar]
- Bordin, D.; Bergamo, E.T.; Fardin, V.P.; Coelho, P.G.; Bonfante, E.A. Fracture strength and probability of survival of narrow and extra-narrow dental implants after fatigue testing: In vitro and in silico analysis. J. Mech. Behav. Biomed. Mater. 2017, 71, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Hirata, R.; Bonfante, E.A.; Anchieta, R.B.; Machado, L.S.; Freitas, G.; Fardin, V.P.; Coelho, P.G. Reliability and failure modes of narrow implant systems. Clin. Oral Investig. 2015, 20, 1505–1513. [Google Scholar] [CrossRef] [PubMed]
- Assaf, A.; Saad, M.; Daas, M.; Abdallah, J.; Abdallah, R. Use of Narrow-Diameter Implants in the Posterior Jaw. Implant Dent. 2015, 24, 294–306. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maximum (N) | Tensile Strength (MPa) | Maximum Bending Moment (Nmm) | |
|---|---|---|---|
| Group 1 | 134.29 (10.27) a | 22.38 (1.71) a | 1316.02 (100.6) a |
| Group 2 | 300.61 ( 24.26) b | 50.1 (4.04) b | 2945.97 ( 237.7) b |
| Group 3 | 360.24 (23.34) c | 60.04(3.89) c | 3530.38 (228.75) c |
| Group 4 | 419.1 (18.87) d | 69.85(3.14) d | 4096.7 (182.73) d |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuzzolo Neto, H.; Tuzita, A.S.; Gehrke, S.A.; de Vasconcellos Moura, R.; Zaffalon Casati, M.; Mikail Melo Mesquita, A. A Comparative Analysis of Implants Presenting Different Diameters: Extra-Narrow, Narrow and Conventional. Materials 2020, 13, 1888. https://doi.org/10.3390/ma13081888
Tuzzolo Neto H, Tuzita AS, Gehrke SA, de Vasconcellos Moura R, Zaffalon Casati M, Mikail Melo Mesquita A. A Comparative Analysis of Implants Presenting Different Diameters: Extra-Narrow, Narrow and Conventional. Materials. 2020; 13(8):1888. https://doi.org/10.3390/ma13081888
Chicago/Turabian StyleTuzzolo Neto, Henrique, Alessandra Sayuri Tuzita, Sérgio Alexandre Gehrke, Renata de Vasconcellos Moura, Márcio Zaffalon Casati, and Alfredo Mikail Melo Mesquita. 2020. "A Comparative Analysis of Implants Presenting Different Diameters: Extra-Narrow, Narrow and Conventional" Materials 13, no. 8: 1888. https://doi.org/10.3390/ma13081888
APA StyleTuzzolo Neto, H., Tuzita, A. S., Gehrke, S. A., de Vasconcellos Moura, R., Zaffalon Casati, M., & Mikail Melo Mesquita, A. (2020). A Comparative Analysis of Implants Presenting Different Diameters: Extra-Narrow, Narrow and Conventional. Materials, 13(8), 1888. https://doi.org/10.3390/ma13081888