In Vitro Generation of Novel Functionalized Biomaterials for Use in Oral and Dental Regenerative Medicine Applications

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Generation of Acellular Fibrin–Agarose Scaffolds (AFAS)
2.2. Generation of Non-Functionalized Fibrin–Agarose Oral Mucosa Stroma Substitutes (n-FAOM)
2.3. Generation of Functionalized Fibrin–Agarose Oral Mucosa Stroma Substitutes (F-FAOM)
2.4. Histological Analyses
2.5. Analysis of ECM Components by Histochemistry
2.6. Immunohistochemical Analysis
2.7. Statistical Analyses
3. Results
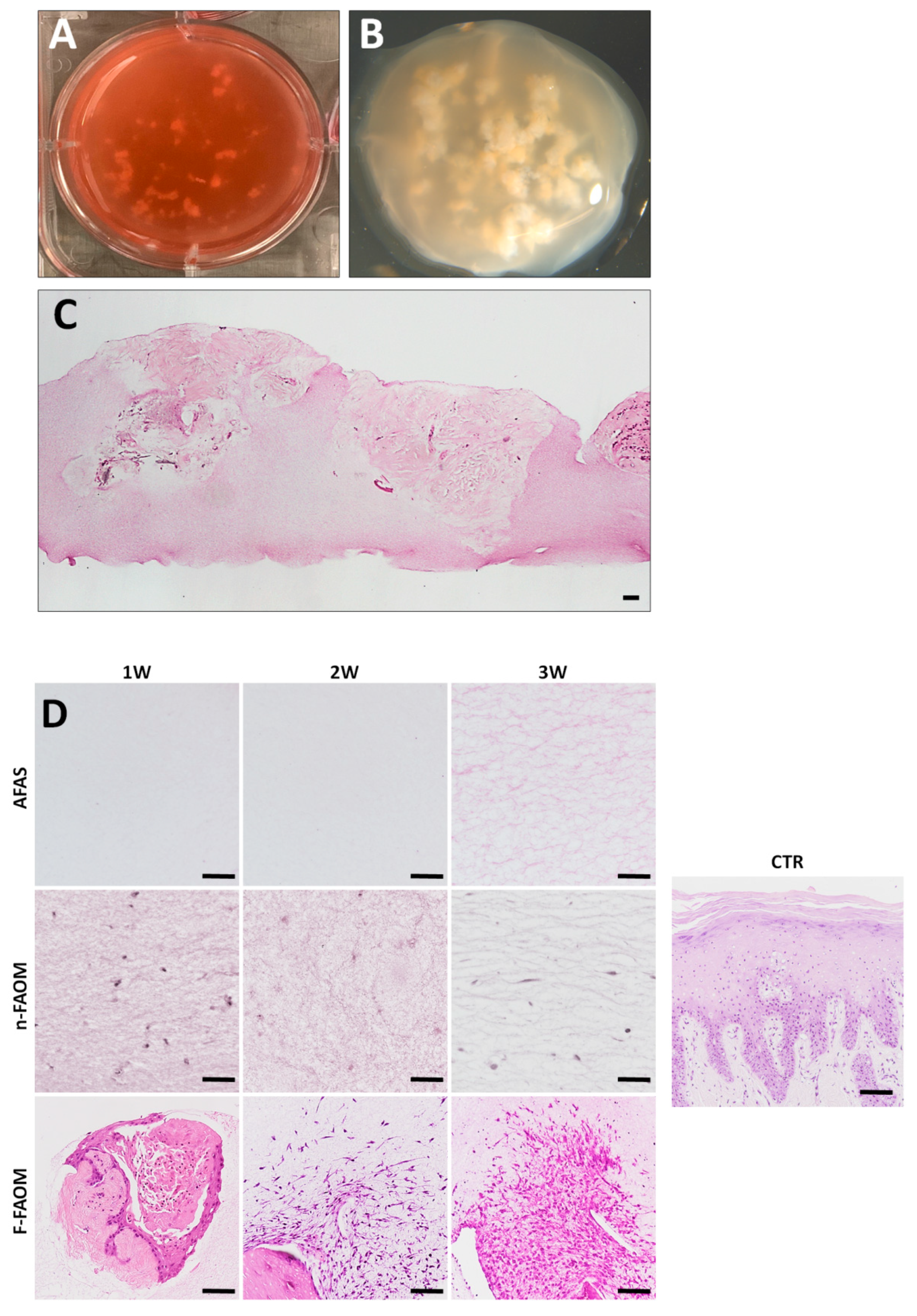
3.1. Histological Analysis of Functionalized and Non-Functionalized Fibrin–Agarose Oral Mucosa Stroma Substitutes
3.2. Cell Proliferation in the Fibrin–Agarose Biomaterial
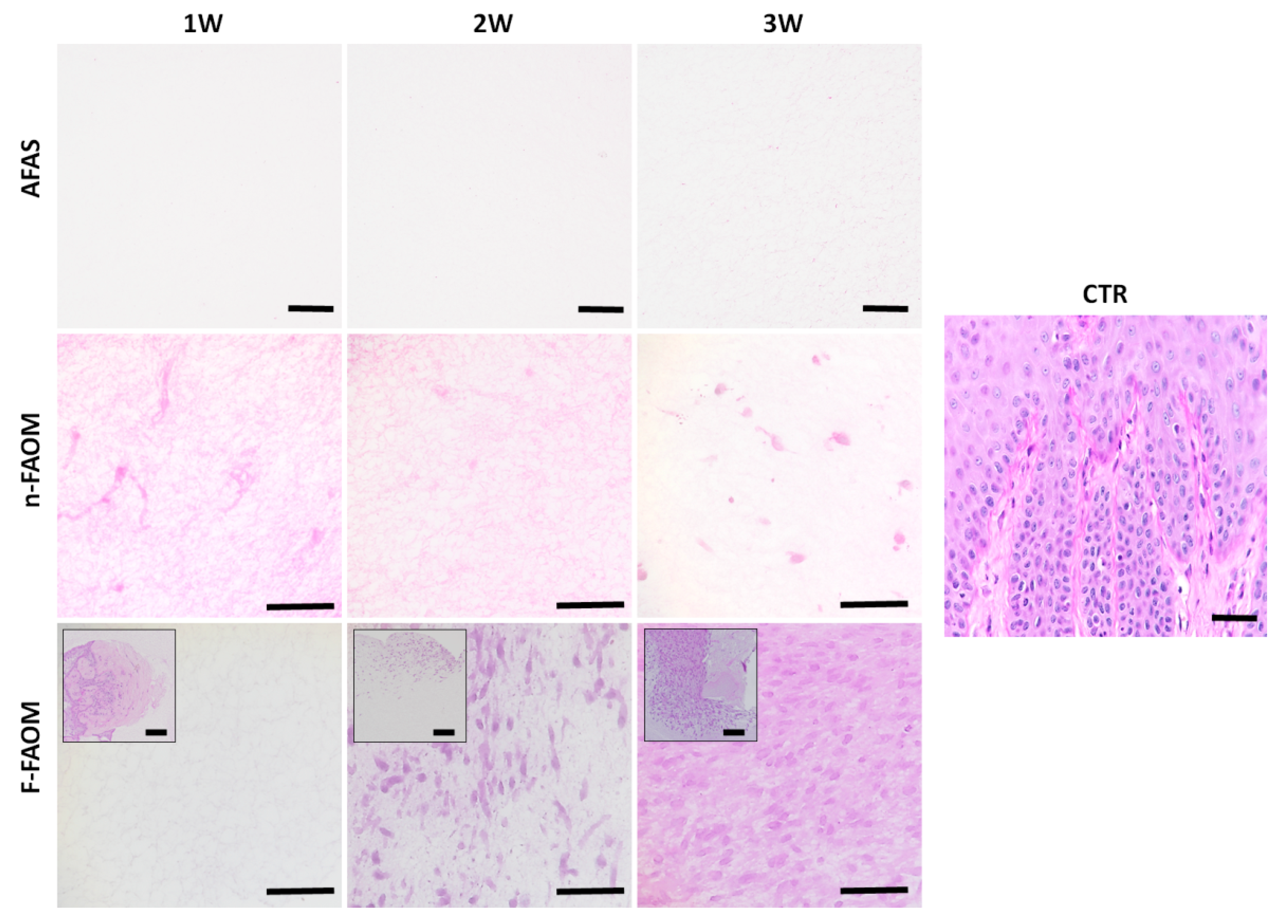
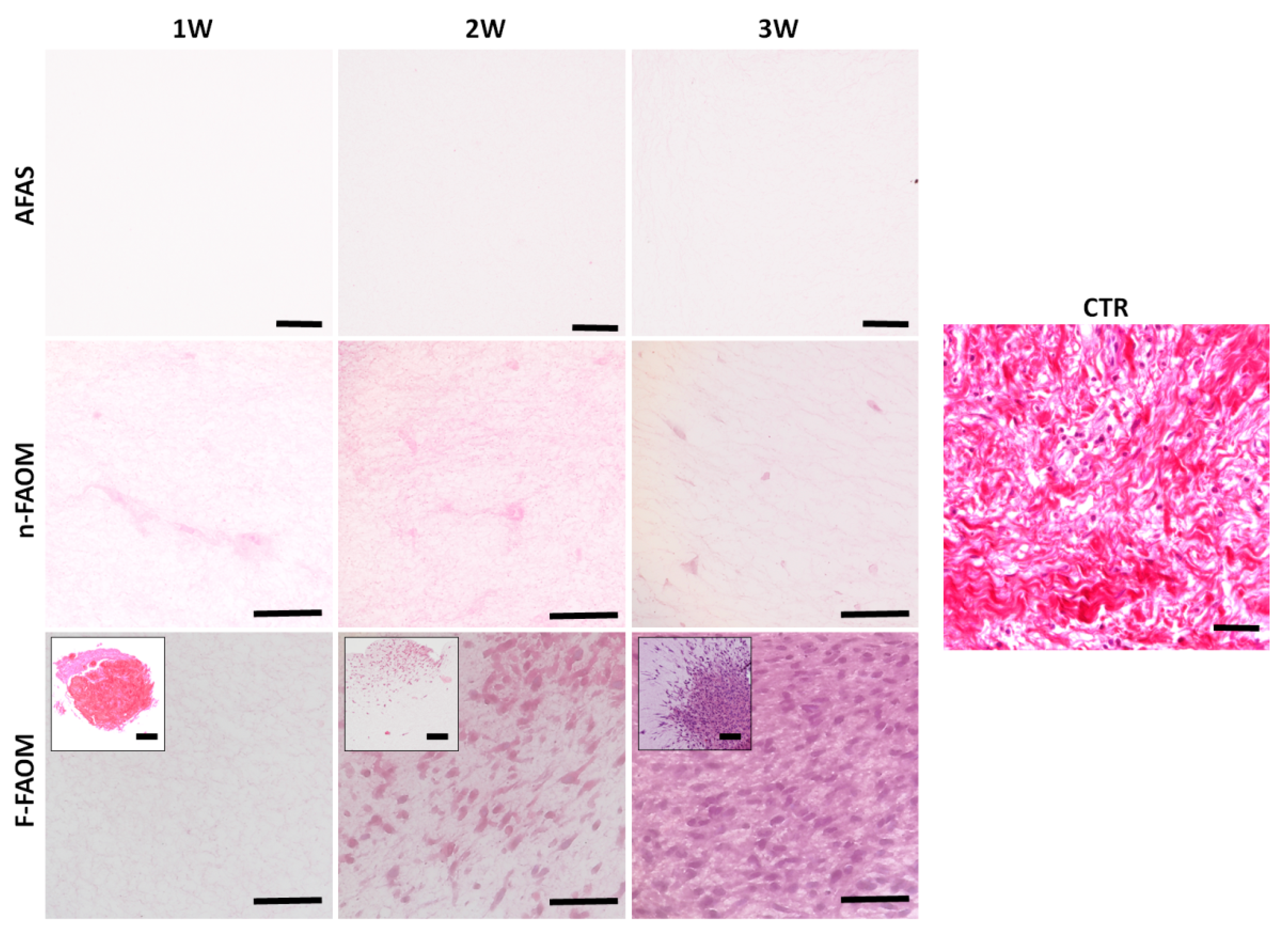
3.3. Development of Non-Fibrillar ECM Components in the Fibrin–Agarose Biomaterial
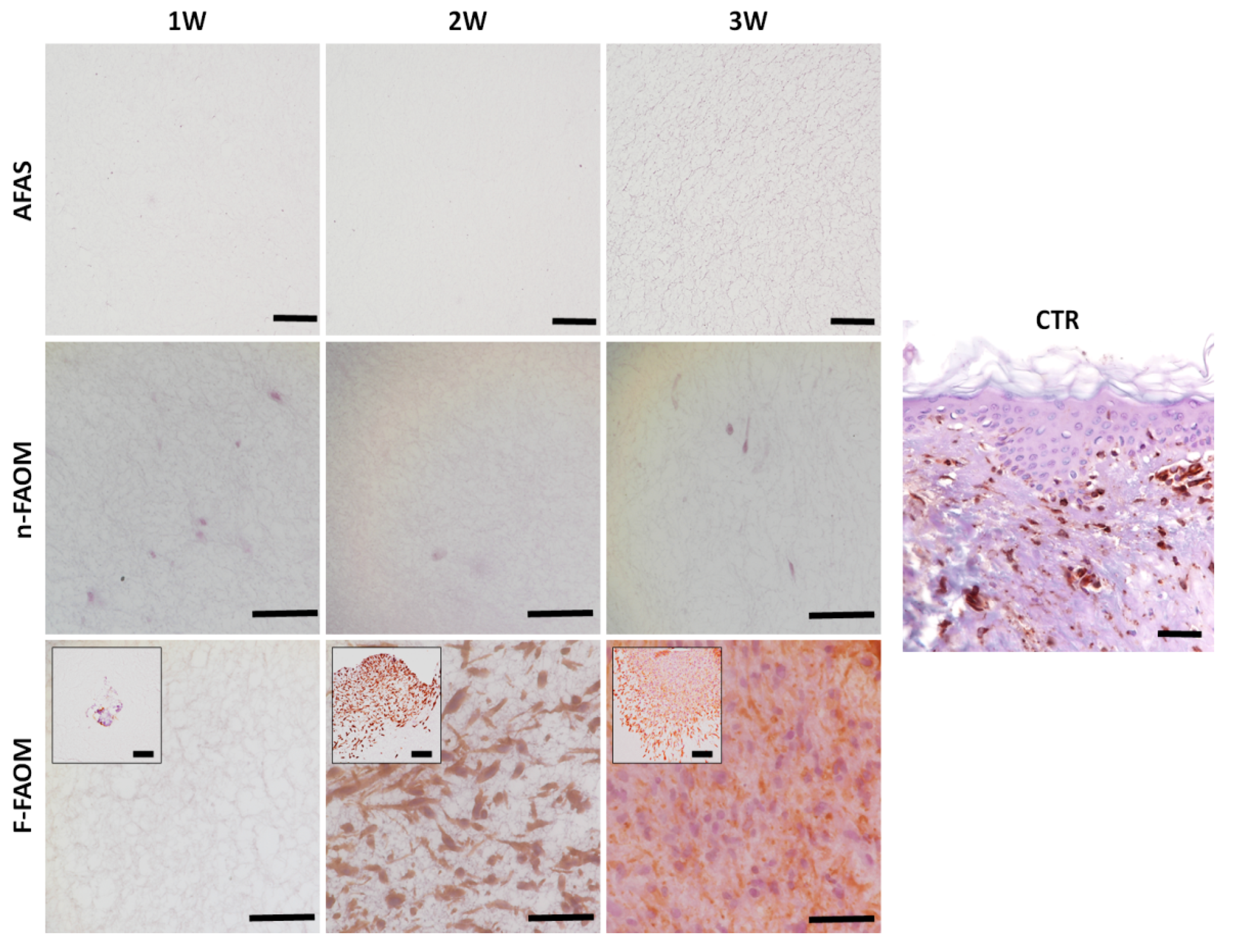
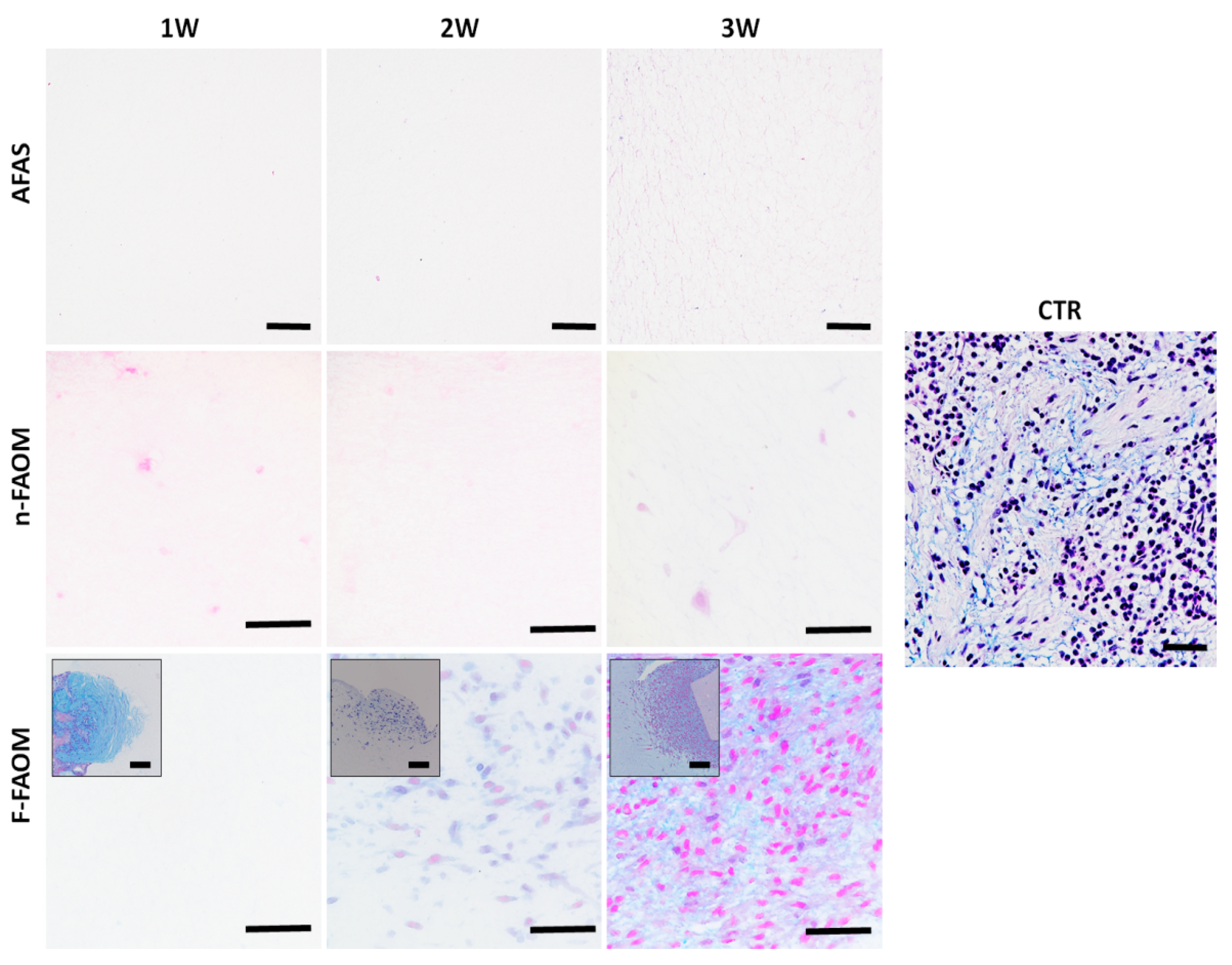
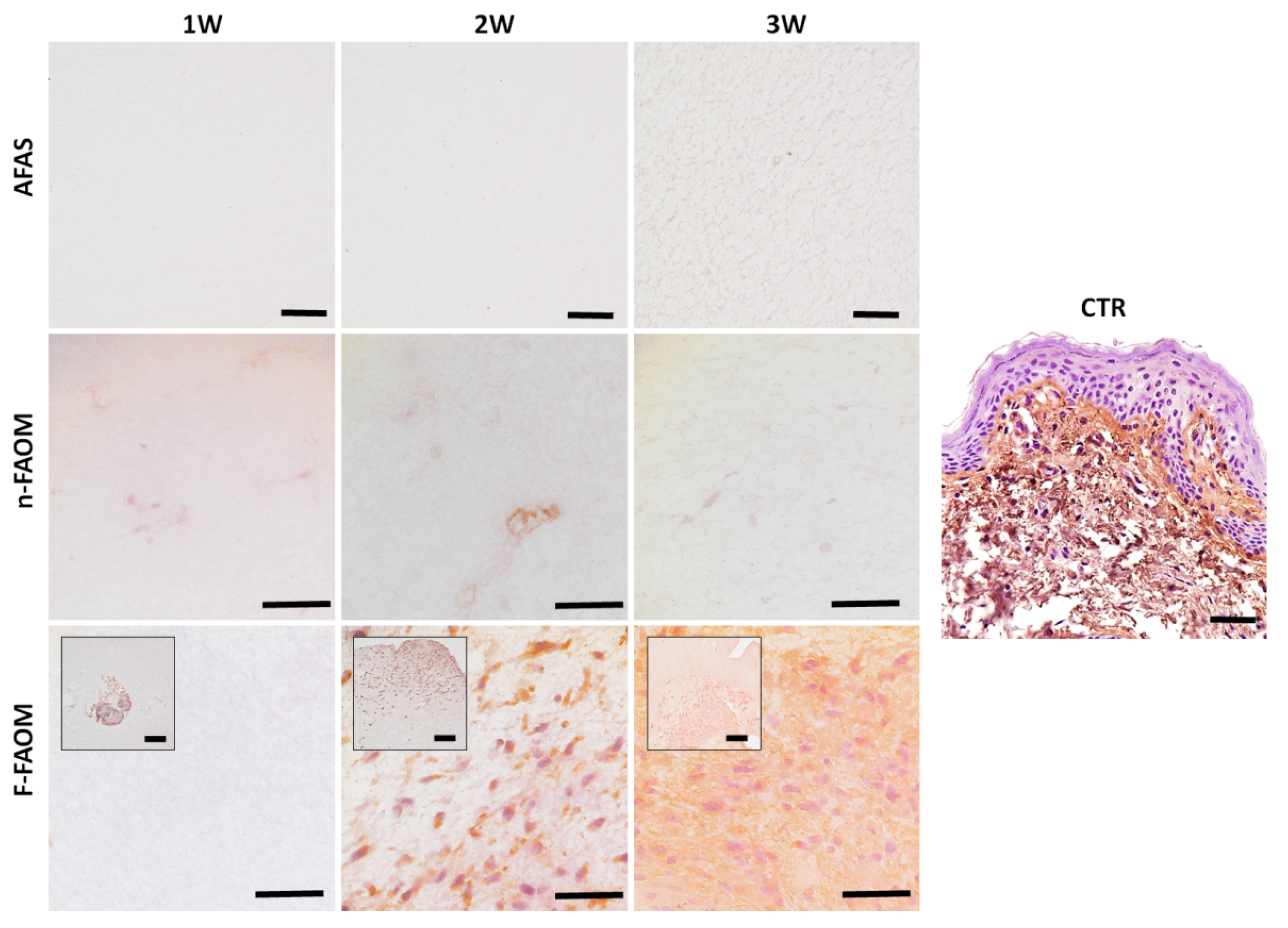
3.4. Development of Fibrillar ECM Components in the Fibrin–Agarose Biomaterial
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Witten, C.M.; McFarland, R.D.; Simek, S.L. Concise Review: The US Food and Drug Administration and Regenerative Medicine. Stem Cells Transl. Med. 2015, 4, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Fagogeni, I.; Metlerska, J.; Lipski, M.; Falgowski, T.; Maciej, G.; Nowicka, A. Materials used in regenerative endodontic procedures and their impact on tooth discoloration. J. Oral Sci. 2019, 61, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Larsson, L.; Decker, A.M.; Nibali, L.; Pilipchuk, S.P.; Berglundh, T.; Giannobile, W.V. Regenerative Medicine for Periodontal and Peri-implant Diseases. J. Dent. Res. 2016, 95, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Langer, R.; Vacanti, J.P. Tissue engineering. Science 1993, 260, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Garzon, I.; Sanchez-Quevedo, M.C.; Moreu, G.; Gonzalez-Jaranay, M.; Gonzalez-Andrades, M.; Montalvo, A.; Campos, A.; Alaminos, M. In vitro and in vivo cytokeratin patterns of expression in bioengineered human periodontal mucosa. J. Periodontal Res. 2009, 44, 588–597. [Google Scholar] [CrossRef]
- Rana, D.; Ramasamy, K.; Leena, M.; Pasricha, R.; Manivasagam, G.; Ramalingam, M. Surface functionalization of biomaterials. In Biology and Engineering of Stem Cell Niches; Vishwakarma, A., Karp, J.M., Eds.; Academic Press: Boston, MA, USA, 2017; pp. 331–343. [Google Scholar]
- Taraballi, F.; Zanini, S.; Lupo, C.; Panseri, S.; Cunha, C.; Riccardi, C.; Marcacci, M.; Campione, M.; Cipolla, L. Amino and carboxyl plasma functionalization of collagen films for tissue engineering applications. J. Colloid Interface Sci. 2013, 394, 590–597. [Google Scholar] [CrossRef]
- Stadlinger, B.; Hintze, V.; Bierbaum, S.; Moller, S.; Schulz, M.C.; Mai, R.; Kuhlisch, E.; Heinemann, S.; Scharnweber, D.; Schnabelrauch, M.; et al. Biological functionalization of dental implants with collagen and glycosaminoglycans-A comparative study. J. Biomed. Mater. Res. B Appl. Biomater. 2012, 100, 331–341. [Google Scholar] [CrossRef]
- Sapudom, J.; Rubner, S.; Martin, S.; Thoenes, S.; Anderegg, U.; Pompe, T. The interplay of fibronectin functionalization and TGF-beta1 presence on fibroblast proliferation, differentiation and migration in 3D matrices. Biomater. Sci. 2015, 3, 1291–1301. [Google Scholar] [CrossRef]
- Koh, H.S.; Yong, T.; Chan, C.K.; Ramakrishna, S. Enhancement of neurite outgrowth using nano-structured scaffolds coupled with laminin. Biomaterials 2008, 29, 3574–3582. [Google Scholar] [CrossRef]
- Rosellini, E.; Cristallini, C.; Guerra, G.D.; Barbani, N. Surface chemical immobilization of bioactive peptides on synthetic polymers for cardiac tissue engineering. J. Biomater. Sci. Polym. Ed. 2015, 26, 515–533. [Google Scholar] [CrossRef]
- Rana, D.; Ramasamy, K.; Leena, M.; Jimenez, C.; Campos, J.; Ibarra, P.; Haidar, Z.S.; Ramalingam, M. Surface functionalization of nanobiomaterials for application in stem cell culture, tissue engineering, and regenerative medicine. Biotechnol Prog 2016, 32, 554–567. [Google Scholar] [CrossRef] [PubMed]
- Martin-Piedra, M.A.; Alaminos, M.; Fernandez-Valades-Gamez, R.; Espana-Lopez, A.; Liceras-Liceras, E.; Sanchez-Montesinos, I.; Martinez-Plaza, A.; Sanchez-Quevedo, M.C.; Fernandez-Valades, R.; Garzon, I. Development of a multilayered palate substitute in rabbits: A histochemical ex vivo and in vivo analysis. Histochem. Cell Biol. 2017, 147, 377–388. [Google Scholar] [CrossRef]
- Garzon, I.; Miyake, J.; Gonzalez-Andrades, M.; Carmona, R.; Carda, C.; Sanchez-Quevedo Mdel, C.; Campos, A.; Alaminos, M. Wharton’s jelly stem cells: A novel cell source for oral mucosa and skin epithelia regeneration. Stem Cells Transl Med 2013, 2, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Garzon, I.; Martin-Piedra, M.A.; Alfonso-Rodriguez, C.; Gonzalez-Andrades, M.; Carriel, V.; Martinez-Gomez, C.; Campos, A.; Alaminos, M. Generation of a biomimetic human artificial cornea model using Wharton’s jelly mesenchymal stem cells. Investig. Ophthalmol. Vis. Sci. 2014, 55, 4073–4083. [Google Scholar] [CrossRef] [PubMed]
- Scionti, G.; Moral, M.; Toledano, M.; Osorio, R.; Duran, J.D.; Alaminos, M.; Campos, A.; Lopez-Lopez, M.T. Effect of the hydration on the biomechanical properties in a fibrin-agarose tissue-like model. J. Biomed. Mater. Res. A 2014, 102, 2573–2582. [Google Scholar] [CrossRef] [PubMed]
- Alfonso-Rodriguez, C.A.; Gonzalez-Andrades, E.; Jaimes-Parra, B.D.; Fernandez-Valades, R.; Campos, A.; Sanchez-Quevedo, M.C.; Alaminos, M.; Garzon, I. Ex vivo and in vivo modulatory effects of umbilical cord Wharton’s jelly stem cells on human oral mucosa stroma substitutes. Histol. Histopathol. 2015, 30, 1321–1332. [Google Scholar] [PubMed]
- Vinuela-Prieto, J.M.; Sanchez-Quevedo, M.C.; Alfonso-Rodriguez, C.A.; Oliveira, A.C.; Scionti, G.; Martin-Piedra, M.A.; Moreu, G.; Campos, A.; Alaminos, M.; Garzon, I. Sequential keratinocytic differentiation and maturation in a three-dimensional model of human artificial oral mucosa. J. Periodontal Res. 2015, 50, 658–665. [Google Scholar] [CrossRef]
- Oliveira, A.C.; Garzon, I.; Ionescu, A.M.; Carriel, V.; Cardona Jde, L.; Gonzalez-Andrades, M.; Perez Mdel, M.; Alaminos, M.; Campos, A. Evaluation of small intestine grafts decellularization methods for corneal tissue engineering. PLoS ONE 2013, 8, e66538. [Google Scholar] [CrossRef]
- Fernandez-Valades-Gamez, R.; Garzon, I.; Liceras-Liceras, E.; Espana-Lopez, A.; Carriel, V.; Martin-Piedra, M.A.; Munoz-Miguelsanz, M.A.; Sanchez-Quevedo, M.C.; Alaminos, M.; Fernandez-Valades, R. Usefulness of a bioengineered oral mucosa model for preventing palate bone alterations in rabbits with a mucoperiostial defect. Biomed. Mater. 2016, 11, 015015. [Google Scholar] [CrossRef]
- Martin-Piedra, M.A.; Garzon, I.; Gomez-Sotelo, A.; Garcia-Abril, E.; Jaimes-Parra, B.D.; Lopez-Cantarero, M.; Alaminos, M.; Campos, A. Generation and Evaluation of Novel Stromal Cell-Containing Tissue Engineered Artificial Stromas for the Surgical Repair of Abdominal Defects. Biotechnol. J. 2017, 12, 1700078. [Google Scholar] [CrossRef]
- Egea-Guerrero, J.J.; Carmona, G.; Correa, E.; Mata, R.; Arias-Santiago, S.; Alaminos, M.; Gacto, P.; Cuende, N. Transplant of Tissue-Engineered Artificial Autologous Human Skin in Andalusia: An Example of Coordination and Institutional Collaboration. Transpl. Proc. 2019, 51, 3047–3050. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Andrades, M.; Mata, R.; Gonzalez-Gallardo, M.D.C.; Medialdea, S.; Arias-Santiago, S.; Martinez-Atienza, J.; Ruiz-Garcia, A.; Perez-Fajardo, L.; Lizana-Moreno, A.; Garzon, I.; et al. A study protocol for a multicentre randomised clinical trial evaluating the safety and feasibility of a bioengineered human allogeneic nanostructured anterior cornea in patients with advanced corneal trophic ulcers refractory to conventional treatment. BMJ Open 2017, 7, e016487. [Google Scholar] [CrossRef] [PubMed]
- Moussa, D.G.; Aparicio, C. Present and future of tissue engineering scaffolds for dentin-pulp complex regeneration. J. Tissue Eng. Regen. Med. 2019, 13, 58–75. [Google Scholar] [CrossRef] [PubMed]
- Kasai, Y.; Takagi, R.; Kobayashi, S.; Owaki, T.; Yamaguchi, N.; Fukuda, H.; Sakai, Y.; Sumita, Y.; Kanai, N.; Isomoto, H.; et al. A stable protocol for the fabrication of transplantable human oral mucosal epithelial cell sheets for clinical application. Regen. Ther. 2020, 14, 87–94. [Google Scholar] [CrossRef]
- Heathman, T.R.; Glyn, V.A.; Picken, A.; Rafiq, Q.A.; Coopman, K.; Nienow, A.W.; Kara, B.; Hewitt, C.J. Expansion, harvest and cryopreservation of human mesenchymal stem cells in a serum-free microcarrier process. Biotechnol. Bioeng. 2015, 112, 1696–1707. [Google Scholar] [CrossRef]
- Costa, A.; Naranjo, J.D.; Londono, R.; Badylak, S.F. Biologic Scaffolds. Cold Spring Harb. Perspect. Med. 2017, 7, a025676. [Google Scholar] [CrossRef]
- Halper, J.; Kjaer, M. Basic components of connective tissues and extracellular matrix: Elastin, fibrillin, fibulins, fibrinogen, fibronectin, laminin, tenascins and thrombospondins. Adv. Exp. Med. Biol. 2014, 802, 31–47. [Google Scholar]
- Aviezer, D.; Levy, E.; Safran, M.; Svahn, C.; Buddecke, E.; Schmidt, A.; David, G.; Vlodavsky, I.; Yayon, A. Differential structural requirements of heparin and heparan sulfate proteoglycans that promote binding of basic fibroblast growth factor to its receptor. J. Biol. Chem. 1994, 269, 114–121. [Google Scholar]
- Browning, K.N. Extracellular matrix proteins in the gastrointestinal tract: More than a supporting role. J. Physiol. 2018, 596, 3831–3832. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Gardin, C.; Zamparini, F.; Ferroni, L.; Esposti, M.D.; Parchi, G.; Ercan, B.; Manzoli, L.; Fava, F.; Fabbri, P.; et al. Mineral-Doped Poly(L-lactide) Acid Scaffolds Enriched with Exosomes Improve Osteogenic Commitment of Human Adipose-Derived Mesenchymal Stem Cells. Nanomaterials 2020, 10, 432. [Google Scholar] [CrossRef]
- Kubo, K. Effects of static stretching on mechanical properties and collagen fiber orientation of the Achilles tendon in vivo. Clin. Biomech. 2018, 60, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Osorio, R.; Alfonso-Rodriguez, C.A.; Osorio, E.; Medina-Castillo, A.L.; Alaminos, M.; Toledano-Osorio, M.; Toledano, M. Novel potential scaffold for periodontal tissue engineering. Clin. Oral Investig. 2017, 21, 2695–2707. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Alcian Blue | PAS | Picrosirius Red | Type-I Collagen | |
|---|---|---|---|---|---|
| Control oral mucosa | CTR | 100 ± 26.01 | 100 ± 27.38 | 100 ± 42.28 | 100 ± 39.4 |
| Global groups | AFAS | 23 ± 1.35 | 16.34 ± 1.94 | 12.11 ± 6.04 | 22.05 ± 1.45 |
| n-FAOM | 21.22 ± 2.72 | 19.84 ± 10.42 | 19.66 ± 11.06 | 30.93 ± 5.85 | |
| F-FAOM | 41.79 ± 13.44 | 54.51 ± 23.97 | 55.79 ± 31.03 | 36.16 ± 17.33 | |
| Specific samples | AFAS-1W | 22.87 ± 1.1 | 15.61 ± 0.79 | 6.04 ± 0.71 | 22.03 ± 0.48 |
| AFAS-2W | 22.7 ± 1.14 | 16.71 ± 2 | 14.83 ± 2.76 | 22.11 ± 1.71 | |
| AFAS-3W | 23.4 ± 1.81 | 16.71 ± 2.63 | 15.47 ± 3.82 | 22.03 ± 1.89 | |
| n-FAOM-1W | 17.91 ± 1.2 | 21.1 ± 10.71 | 11.68 ± 8.1 | 28.64 ± 4.18 | |
| n-FAOM-2W | 18.97 ± 1.7 | 22.32 ± 5.21 | 20.95 ± 10.48 | 30.99 ± 4.19 | |
| n-FAOM-3W | 26.77 ± 1.73 | 16.1 ± 13.85 | 26.35 ± 5.54 | 33.17 ± 7.69 | |
| F-FAOM-1W | 17.55 ± 0.74 | 21.1 ± 10.04 | 29.81 ± 6.41 | 21.86 ± 4.23 | |
| F-FAOM-2W | 39.72 ± 4.4 | 55.61 ± 10.63 | 51.57 ± 9.26 | 34.17 ± 12.36 | |
| F-FAOM-3W | 68.09 ± 10.42 | 86.83 ± 4.64 | 85.98 ± 15.2 | 52.43 ± 6.9 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanco-Elices, C.; España-Guerrero, E.; Mateu-Sanz, M.; Sánchez-Porras, D.; García-García, Ó.D.; Sánchez-Quevedo, M.d.C.; Fernández-Valadés, R.; Alaminos, M.; Martín-Piedra, M.Á.; Garzón, I. In Vitro Generation of Novel Functionalized Biomaterials for Use in Oral and Dental Regenerative Medicine Applications. Materials 2020, 13, 1692. https://doi.org/10.3390/ma13071692
Blanco-Elices C, España-Guerrero E, Mateu-Sanz M, Sánchez-Porras D, García-García ÓD, Sánchez-Quevedo MdC, Fernández-Valadés R, Alaminos M, Martín-Piedra MÁ, Garzón I. In Vitro Generation of Novel Functionalized Biomaterials for Use in Oral and Dental Regenerative Medicine Applications. Materials. 2020; 13(7):1692. https://doi.org/10.3390/ma13071692
Chicago/Turabian StyleBlanco-Elices, Cristina, Enrique España-Guerrero, Miguel Mateu-Sanz, David Sánchez-Porras, Óscar Darío García-García, María del Carmen Sánchez-Quevedo, Ricardo Fernández-Valadés, Miguel Alaminos, Miguel Ángel Martín-Piedra, and Ingrid Garzón. 2020. "In Vitro Generation of Novel Functionalized Biomaterials for Use in Oral and Dental Regenerative Medicine Applications" Materials 13, no. 7: 1692. https://doi.org/10.3390/ma13071692
APA StyleBlanco-Elices, C., España-Guerrero, E., Mateu-Sanz, M., Sánchez-Porras, D., García-García, Ó. D., Sánchez-Quevedo, M. d. C., Fernández-Valadés, R., Alaminos, M., Martín-Piedra, M. Á., & Garzón, I. (2020). In Vitro Generation of Novel Functionalized Biomaterials for Use in Oral and Dental Regenerative Medicine Applications. Materials, 13(7), 1692. https://doi.org/10.3390/ma13071692