The Use of ESEM-EDX as an Innovative Tool to Analyze the Mineral Structure of Peri-Implant Human Bone


 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Histological Preparation
2.2. OM and ESEM-EDX Microanalysis
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Albrektsson, T.; Brånemark, P.I.; Hansson, H.A.; Lindström, J. Osseointegrated titanium implants. Requirements for ensuring a long-lasting, direct bone-to- implant anchorage in man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.E. Understanding peri-implant endosseous healing. J. Dent. Educ. 2003, 67, 932–949. [Google Scholar] [PubMed]
- Qian, J.; Wennerberg, A.; Albrektsson, T. Reasons for Marginal Bone Loss around Oral Implants. Clin. Implant Dent. Relat. Res. 2012, 14, 792–807. [Google Scholar] [CrossRef]
- Palmquist, A.; Lindberg, F.; Emanuelsson, L.; Branemark, R.; Engqvist, H.; Thomsen, P. Biomechanical, histological, and ultrastructural analyses of laser micro and nano-structured titanium alloy implants: A study in rabbit. J. Biomed. Mater. Res. A 2010, 92, 1476–1486. [Google Scholar] [CrossRef]
- Palmquist, A.; Lindberg, F.; Emanuelsson, L.; Branemark, R.; Engqvist, H.; Thomsen, P. Morphological studies on machined implants of commercially pure titanium and titanium alloy (Ti6Al4V) in the rabbit. J. Biomed. Mater. Res. B 2009, 91, 309–319. [Google Scholar] [CrossRef]
- Davies, J.E.; Mendes, V.C.; Ko, J.C.; Ajami, E. Topographic scale-range synergy at the functional bone/implant interface. Biomaterials 2014, 35, 25–35. [Google Scholar] [CrossRef]
- Shah, F.A.; Ruscsák, K.; Palmquist, A. 50 years of scanning electron microscopy of bone-a comprehensive overview of the important discoveries made and insights gained into bone material properties in health, disease, and taphonomy. Bone Res. 2019, 7, 1–15. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Iezzi, G.; Piattelli, A.; Prati, C.; Scarano, A. Osteoinductive potential and bone-bonding ability of ProRoot MTA, MTA Plus and Biodentine in rabbit intramedullary model: Microchemical characterization and histological analysis. Dent. Mater. 2017, 33, 33–238. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Zamparini, F.; Iezzi, G.; Degidi, M.; Botticelli, D.; Piattelli, A.; Prati, C. Microchemical and micromorphologic ESEM-EDX analysis of bone mineralization at the thread interface in human dental implants retrieved for mechanical complications after 2 months to 17 years. Int. J. Periodontics Restor. Dent. 2018, 38, 431–441. [Google Scholar] [CrossRef]
- Bigi, A.; Cojazzi, G.; Panzavolta, S.; Ripamonti, A.; Roveri, N.; Romanello, M.; Noris Suarez, K.; Moro, L. Chemical and structural Characterization of the Mineral Phase from Cortical and Trabecular Bone. J. Inorg. Biochem. 1997, 68, 45–51. [Google Scholar] [CrossRef]
- Akesson, K.; Grynpas, M.D.; Hancock, R.G.; Odselius, R.; Obrant, K.J. Energy-dispersive X-ray microanalysis of the bone mineral content in human trabecular bone: A comparison with ICPES and neutron activation analysis. Calcif. Tissue Int. 1994, 55, 236–239. [Google Scholar] [CrossRef] [PubMed]
- Eliades, G.; Mantzourani, M.; Labella, R.; Mutti, B.; Sharma, D. Interactions of dentine desensitisers with human dentine: Morphology and composition. J. Dent. 2013, 41, 28–39. [Google Scholar] [CrossRef]
- Shah, F.A.; Nilson, B.; Brånemark, R.; Thomsen, P.; Palmquist, A. The bone-implant interface nanoscale analysis of clinically retrieved dental implants. Nanomedicine 2014, 10, 1729–1737. [Google Scholar] [CrossRef] [PubMed]
- Shah, F.A.; Thomsen, P.; Palmquist, A. Osseointegration and current interpretations of the bone-implant interface. Acta Biomater. 2019, 84, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Yonezawa, D.; Piattelli, A.; Favero, R.; Ferri, M.; Iezzi, G.; Botticelli, D. Bone Healing at Functionally Loaded and Unloaded Screw-Shaped Implants Supporting Single Crowns: A Histomorphometric Study in Humans. Int. J. Oral Maxillofac. Implants 2018, 33, 181–187. [Google Scholar] [CrossRef]
- Prati, C.; Zamparini, F.; Pirani, C.; Montebugnoli, L.; Canullo, L.; Gandolfi, M.G. A Multilevel Analysis of Platform-Switching Flapless Implants Placed at Tissue Level: 4-year Prospective Cohort Study. Int. J. Oral Maxillofac. Implants 2020, 35, 330–341. [Google Scholar] [CrossRef]
- Tomasi, C.; Sanz, M.; Cecchinato, D.; Pjetursson, B.; Ferrus, J.; Lang, N.P.; Lindhe, J. Bone dimensional variations at implants placed in fresh extraction sockets: A multilevel multivariate analysis. Clin. Oral Implants Res. 2010, 21, 30–36. [Google Scholar] [CrossRef]
- Franchi, M.; Bacchelli, B.; Martini, D.; Pasquale, V.D.; Orsini, E.; Ottani, V.; Fini, M.; Giavaresi, G.; Giardino, R.; Ruggeri, A. Early detachment of titanium particles from various different surfaces of endosseous dental implants. Biomaterials 2004, 25, 2239–2246. [Google Scholar] [CrossRef]
- Franchi, M.; Fini, M.; Martini, D.; Orsini, E.; Leonardi, L.; Ruggeri, A.; Giavaresi, G.; Ottani, V. Biological fixation of endosseous implants. Micron 2005, 36, 665–671. [Google Scholar] [CrossRef]
- Coelho, P.G.; Marin, C.; Granato, R.; Suzuki, M. Histomorphologic analysis of 30 plateau root form implants retrieved after 8 to 13 years in function. A human retrieval study. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 91, 975–979. [Google Scholar] [CrossRef]
- Zhou, W.; Kuderer, S.; Liu, Z.; Ulm, C.; Rausch-Fan, X.; Tangl, S. Peri-implant bone remodeling at the interface of three different implant types: A histomorphometric study in mini-pigs. Clin. Oral Implant. Res. 2017, 28, 1443–1449. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, D.; Lang, N.P. Dynamics of osseointegration in various human and animal models—A comparative analysis. Clin. Oral Implant. Res. 2017, 28, 742–748. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
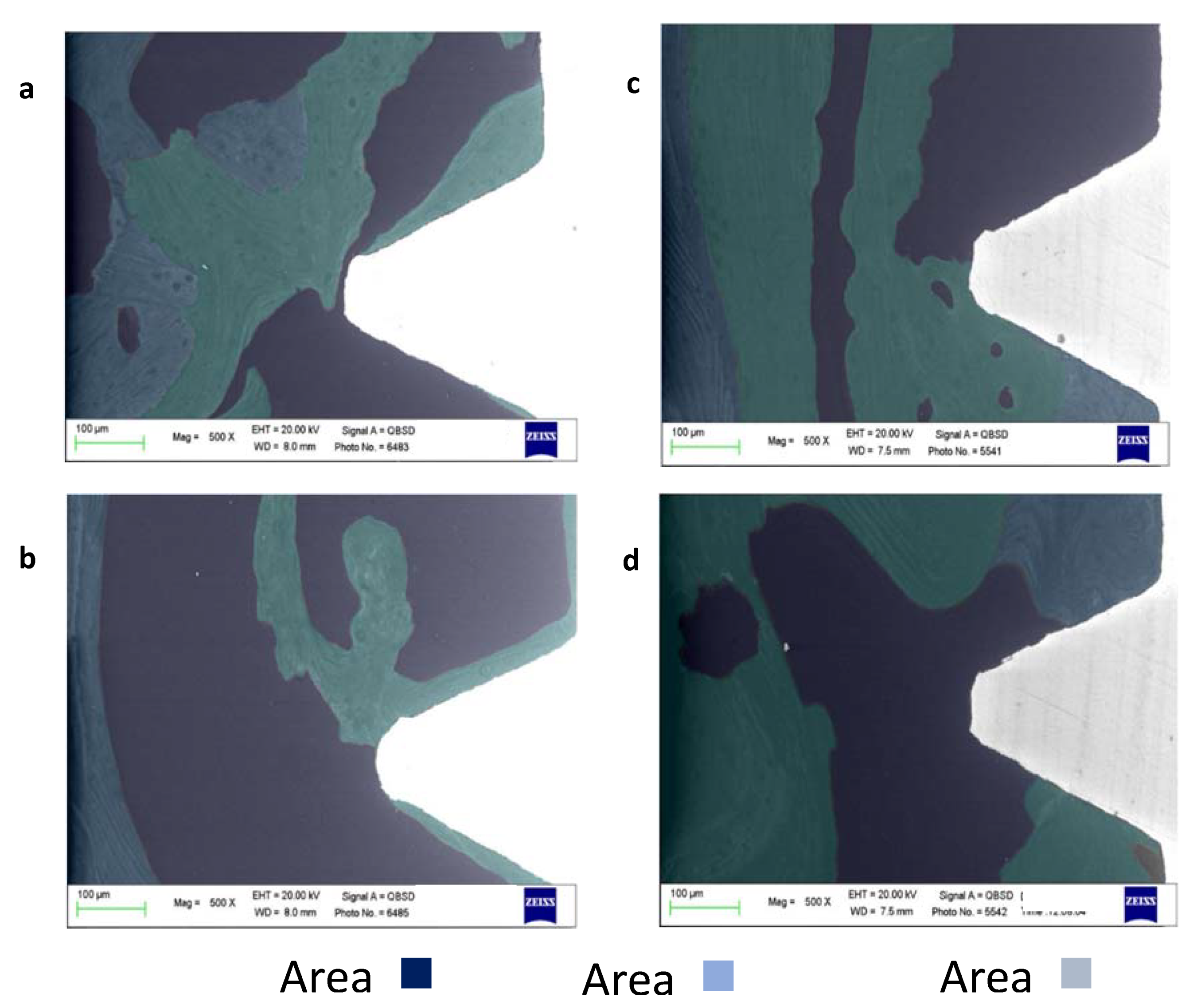
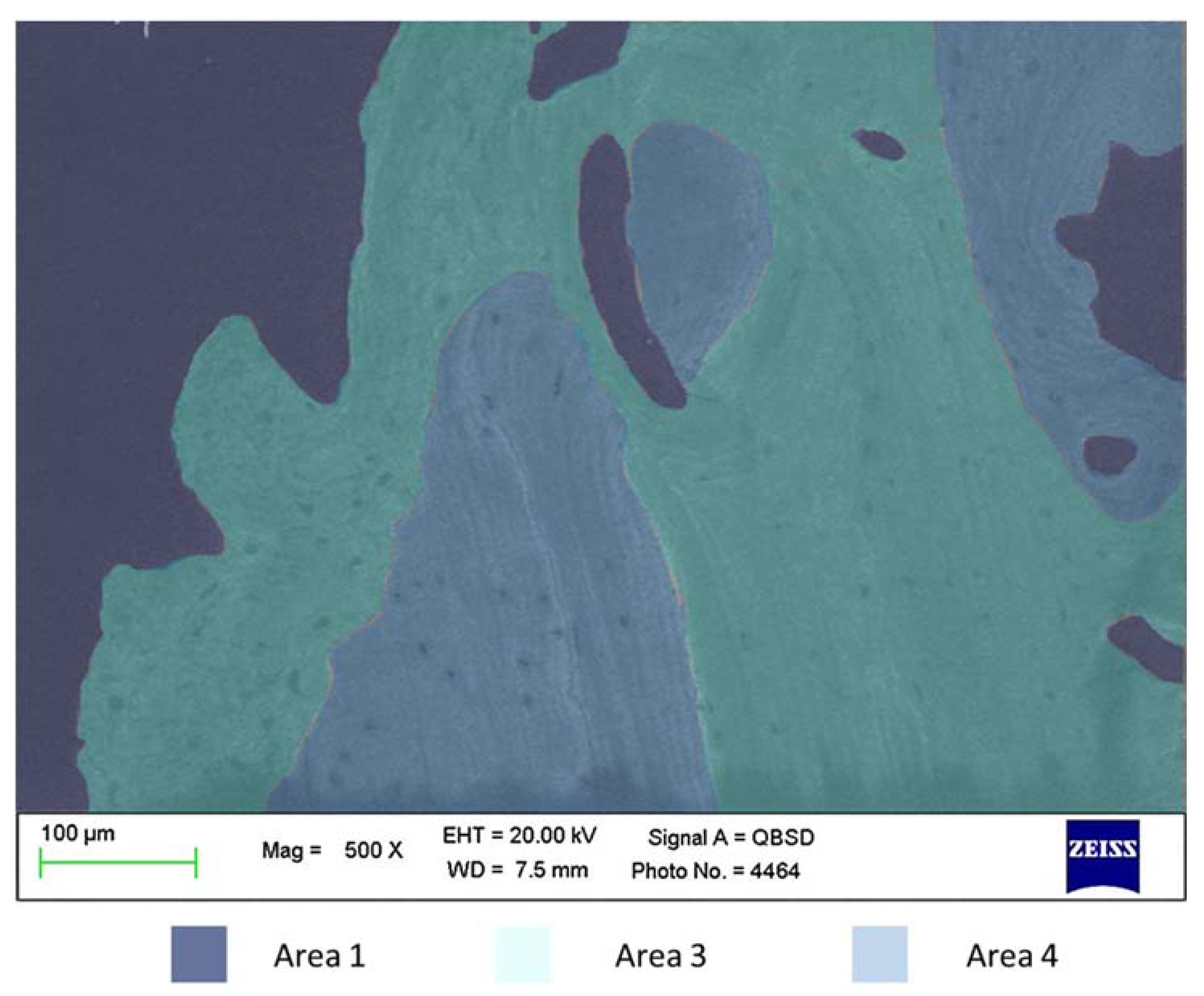
| Mineralization Areas | Ca | P | N |
|---|---|---|---|
| Bone Area 1 low mineralized bone (bone marrow) | Very low 0.7–1.20 | Very low 0.90–1.10 | High 13.0–15.0 |
| Bone Area 2 Medium mineralized bone (bone remodeling) | Moderate 1.25–1.75 | Moderate 1.10–1.50 | Moderate 11.0–12.0 |
| Bone Area 3 high mineralized area (mature old bone/bone chips) | High 1.75–3.00 | High 1.50–2.00 | Low 8.0–11.0 |
| Bone Area 4 high mineralized area (cortical bone) | Very High 2.75–5.00 | Very High 2.00–3.00 | Moderate 11.0–12.0 |
| Mineralization Areas | Ca/N | P/N | Ca/P |
|---|---|---|---|
| Bone Area 1 low mineralized bone (bone marrow) | Very low 0.01–0.08 | Very low 0.02–0.08 | Low 0.75–1.20 |
| Bone Area 2 Medium mineralized bone (bone remodeling) | Moderate 0.11–0.16 | Moderate 0.10–0.20 | Moderate 1.30–1.50 |
| Bone Area 3 high mineralized area (mature old bone /bone chips) | High 0.18–0.25 | High 0.15–0.25 | High 1.30–1.80 |
| Bone Area 4 high mineralized area (cortical bone) apatite | High 0.18–0.25 | High 0.15–0.20 | High 1.33–2.00 |
| ROI | Bone Area 1 low Mineralized Bone (Bone Marrow) | Bone Area 2 Medium Mineralized Bone (New Bone) | Bone Area 3 High Mineralized Area (Mature Old Bone/Bone Chips) |
|---|---|---|---|
| Coronal ROI | 34.9 ± 14.7 | 39.9 ± 12.1 | 26.5 ± 10.2 |
| Apical ROI | 43.2 ± 18.1 | 36.8 ± 12.9 | 19.8 ± 9.7 |
| Thread | Bone Area 1 Low Mineralized Bone (Bone Marrow) | Bone Area 2 Medium Mineralized Bone (Bone Remodeling) | Bone Area 3 Highly Mineralized Area (Mature Old Bone/Bone Chips) |
|---|---|---|---|
| Coronal | 34.2 ± 22.1 | 54.2 ± 19.1 | 13.2 ± 12.8 |
| Apical | 32.4 ± 20.1 | 50.2 ± 14.7 | 15.1 ± 12.1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prati, C.; Zamparini, F.; Botticelli, D.; Ferri, M.; Yonezawa, D.; Piattelli, A.; Gandolfi, M.G. The Use of ESEM-EDX as an Innovative Tool to Analyze the Mineral Structure of Peri-Implant Human Bone. Materials 2020, 13, 1671. https://doi.org/10.3390/ma13071671
Prati C, Zamparini F, Botticelli D, Ferri M, Yonezawa D, Piattelli A, Gandolfi MG. The Use of ESEM-EDX as an Innovative Tool to Analyze the Mineral Structure of Peri-Implant Human Bone. Materials. 2020; 13(7):1671. https://doi.org/10.3390/ma13071671
Chicago/Turabian StylePrati, Carlo, Fausto Zamparini, Daniele Botticelli, Mauro Ferri, Daichi Yonezawa, Adriano Piattelli, and Maria Giovanna Gandolfi. 2020. "The Use of ESEM-EDX as an Innovative Tool to Analyze the Mineral Structure of Peri-Implant Human Bone" Materials 13, no. 7: 1671. https://doi.org/10.3390/ma13071671
APA StylePrati, C., Zamparini, F., Botticelli, D., Ferri, M., Yonezawa, D., Piattelli, A., & Gandolfi, M. G. (2020). The Use of ESEM-EDX as an Innovative Tool to Analyze the Mineral Structure of Peri-Implant Human Bone. Materials, 13(7), 1671. https://doi.org/10.3390/ma13071671