Development of 3D Printed Networks in Self-Healing Concrete


Abstract
1. Introduction
2. MVN Design and Materials
2.1. Design Concept and Considerations
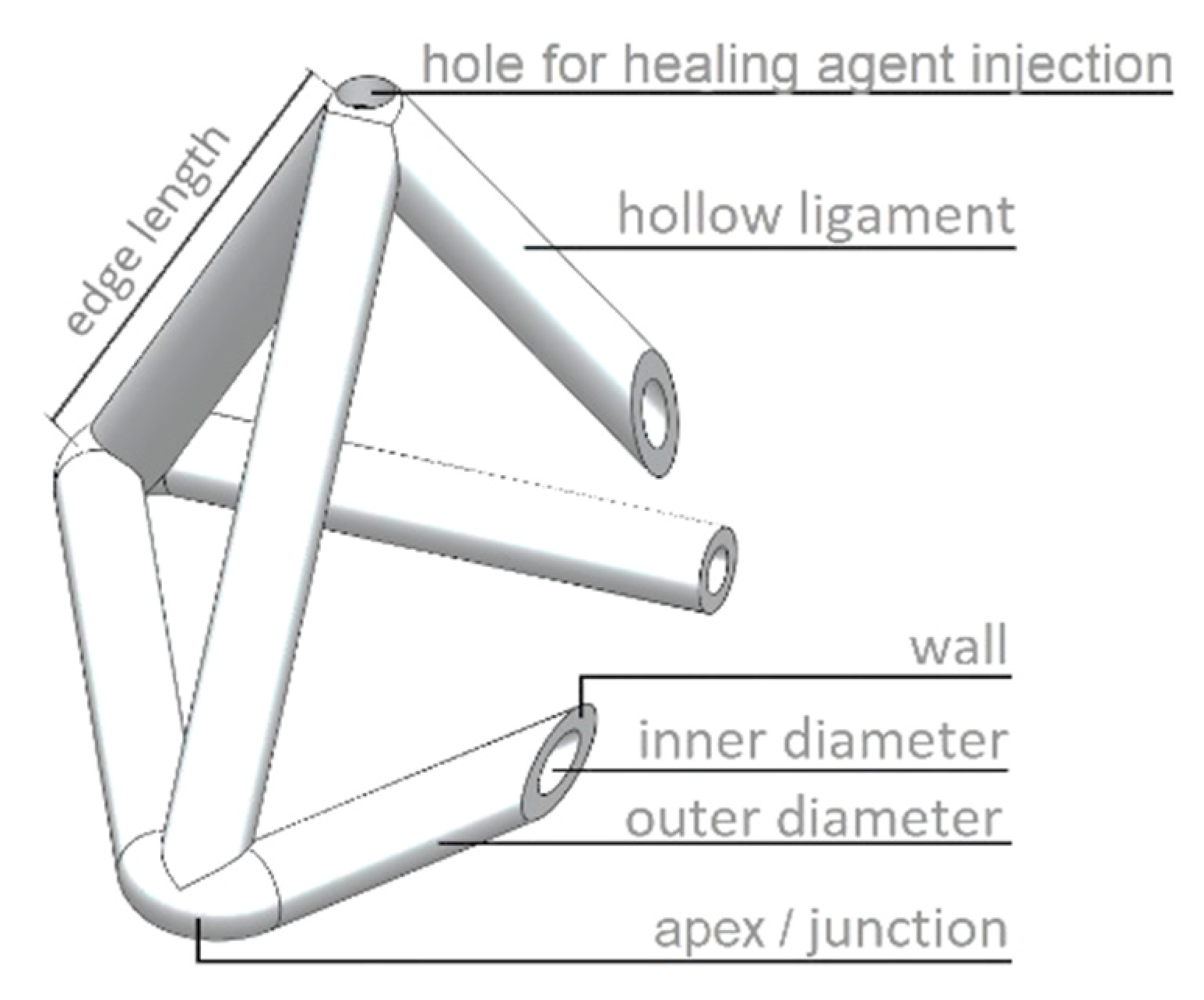
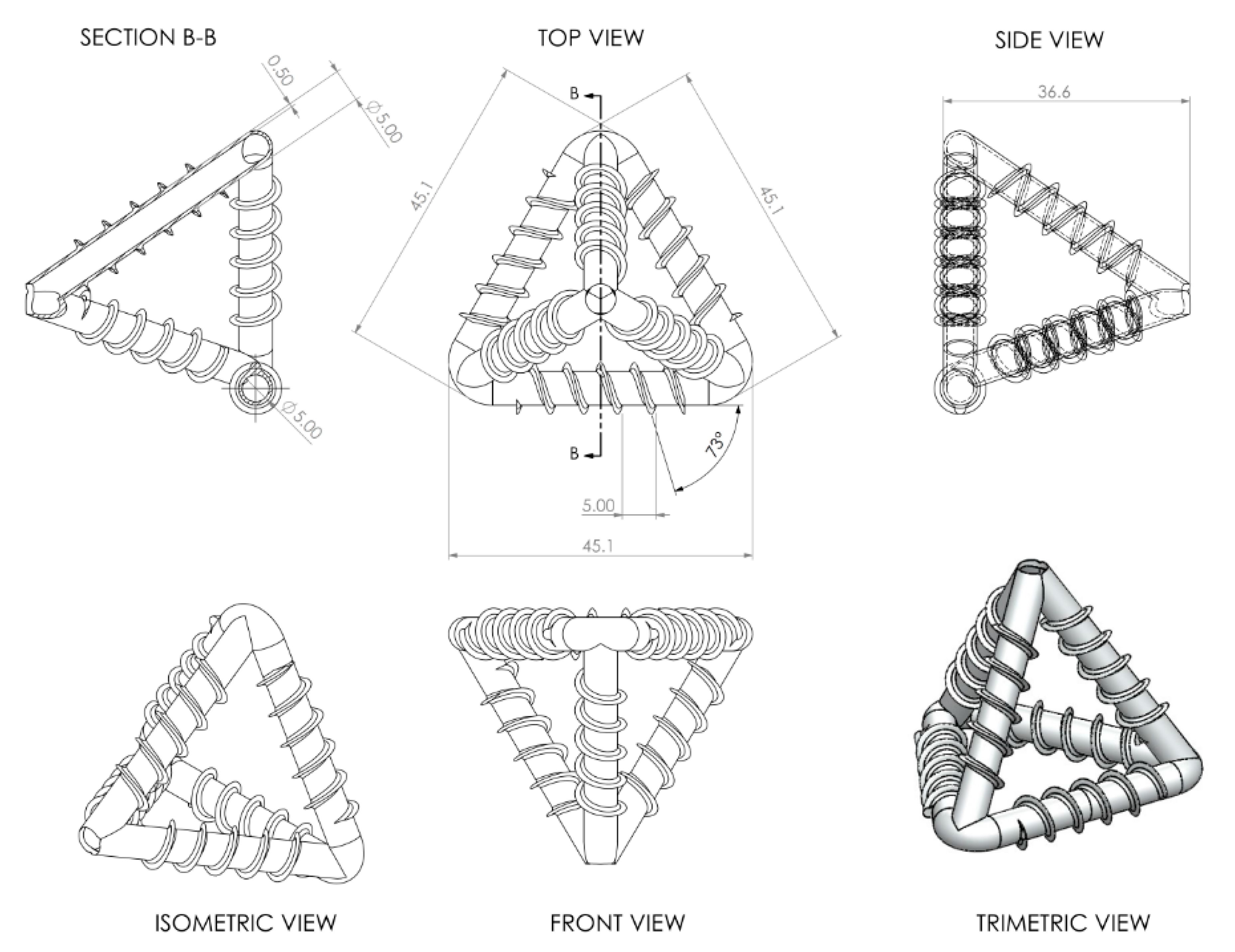
2.2. MVN Ligament Design
- Both clear and white PLA (Polylactic acid) materials are suitable for the MVNs although clear PLA tubes are more likely to rupture at the required serviceability crack opening.
- Spiral rib patterns provide better bond than annular rib patterns and therefore are more likely to result in tube rupture at the required crack opening, with both 3 mm and 5 mm pitch rib patterns being viable, although 5 mm are preferred from a 3D-printing viewpoint.
- Rupture at the required crack opening is more likely to occur in thinner walled tubes (0.25 mm), although these have a greater permeability than thicker walled tubes (0.5 mm) (see discussion in Appendix A.1).
2.3. Encapsulation Environment and Selection of Healing Agents
3. Experimental Materials and Methods
3.1. MVN Design
3.2. Experimental Details
3.2.1. Mix Details
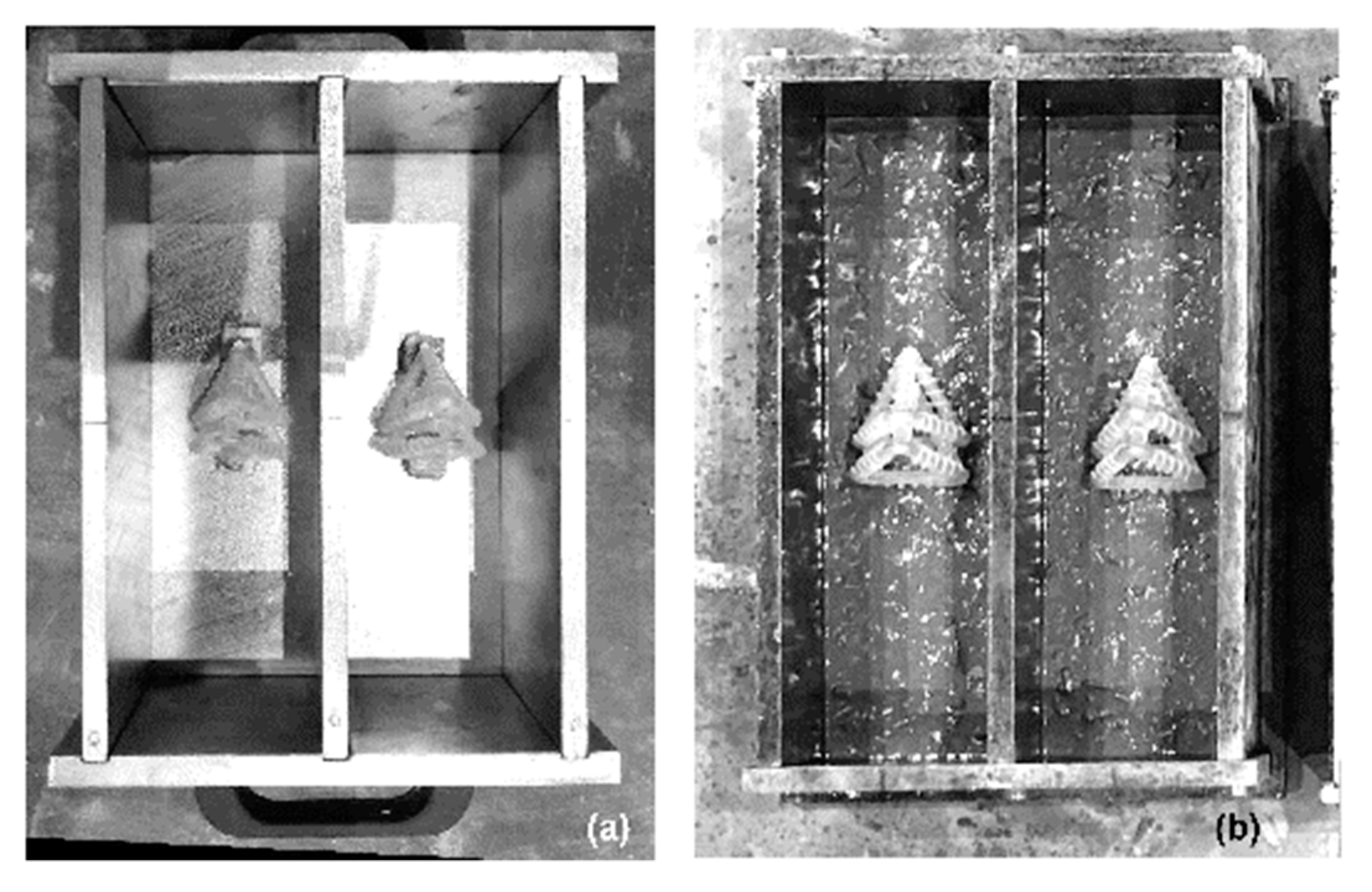
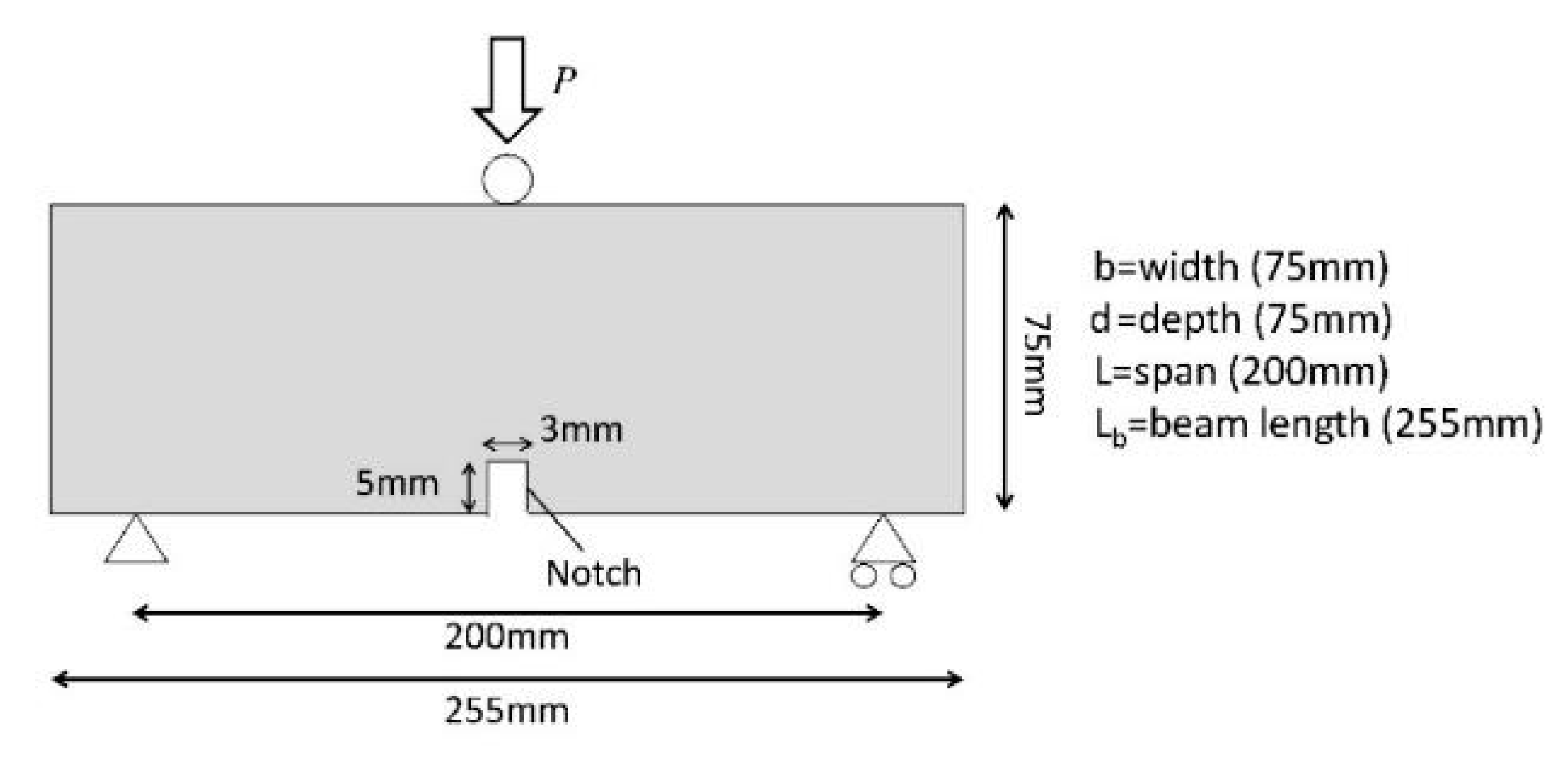
3.2.2. Experimental Arrangement
3.2.3. Experimental Programme
- the level of damage: the effect of the damage was studied by loading the samples until a crack opening of 0.4 mm was achieved;
- the amount of water available for the reaction between SS and CH to form a C-S-H gel: this was studied by placing the specimens in a sealed container covered with a damp hessian cloth to provide high relative humidity values (>90%) at a constant room temperature (ca. 20 °C) following the pre-cracking phase;
- the healing period: the time of healing after the pre-cracking phase was increased to 21 days.
4. Experimental Results
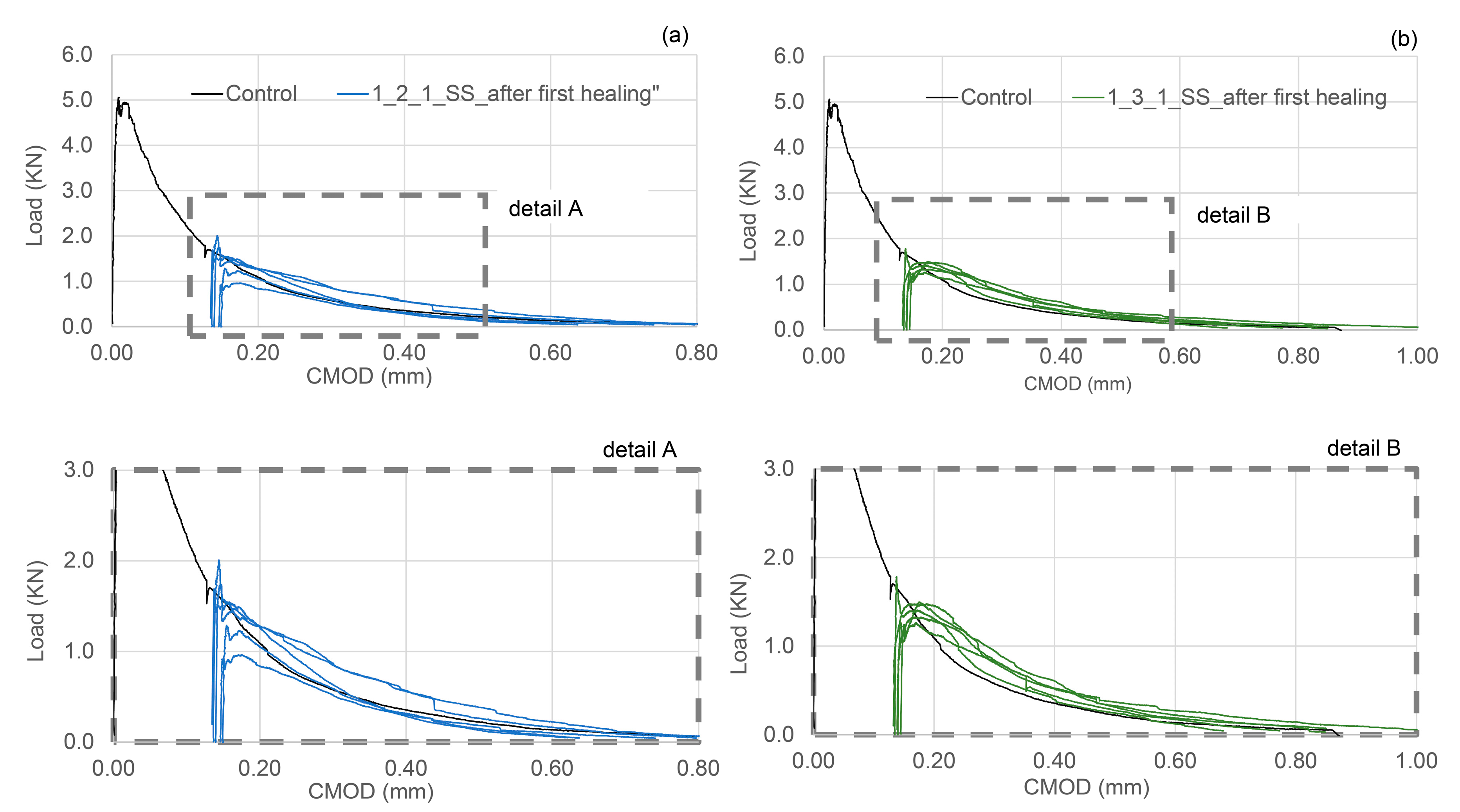
4.1. Group 1 Results
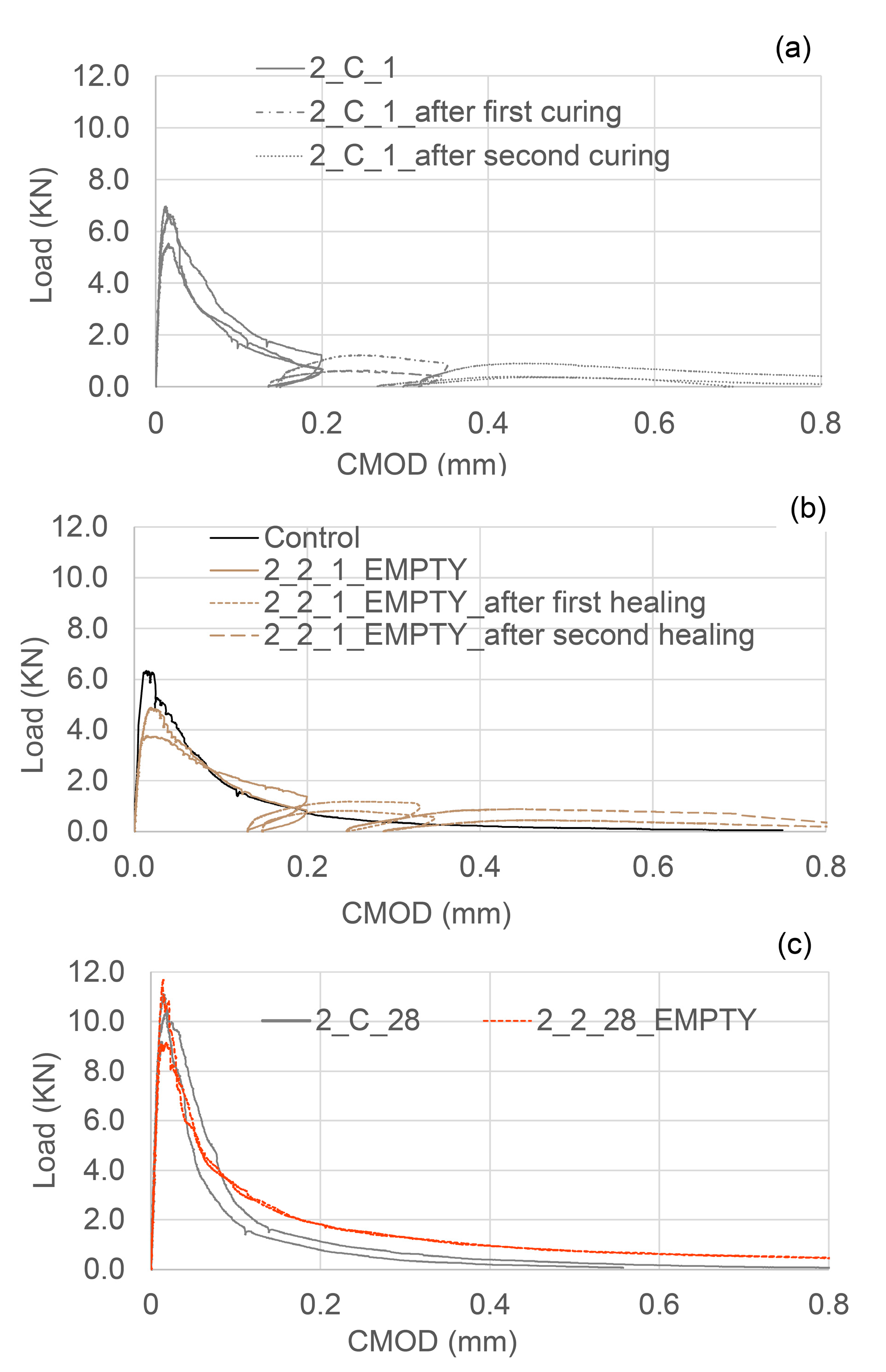
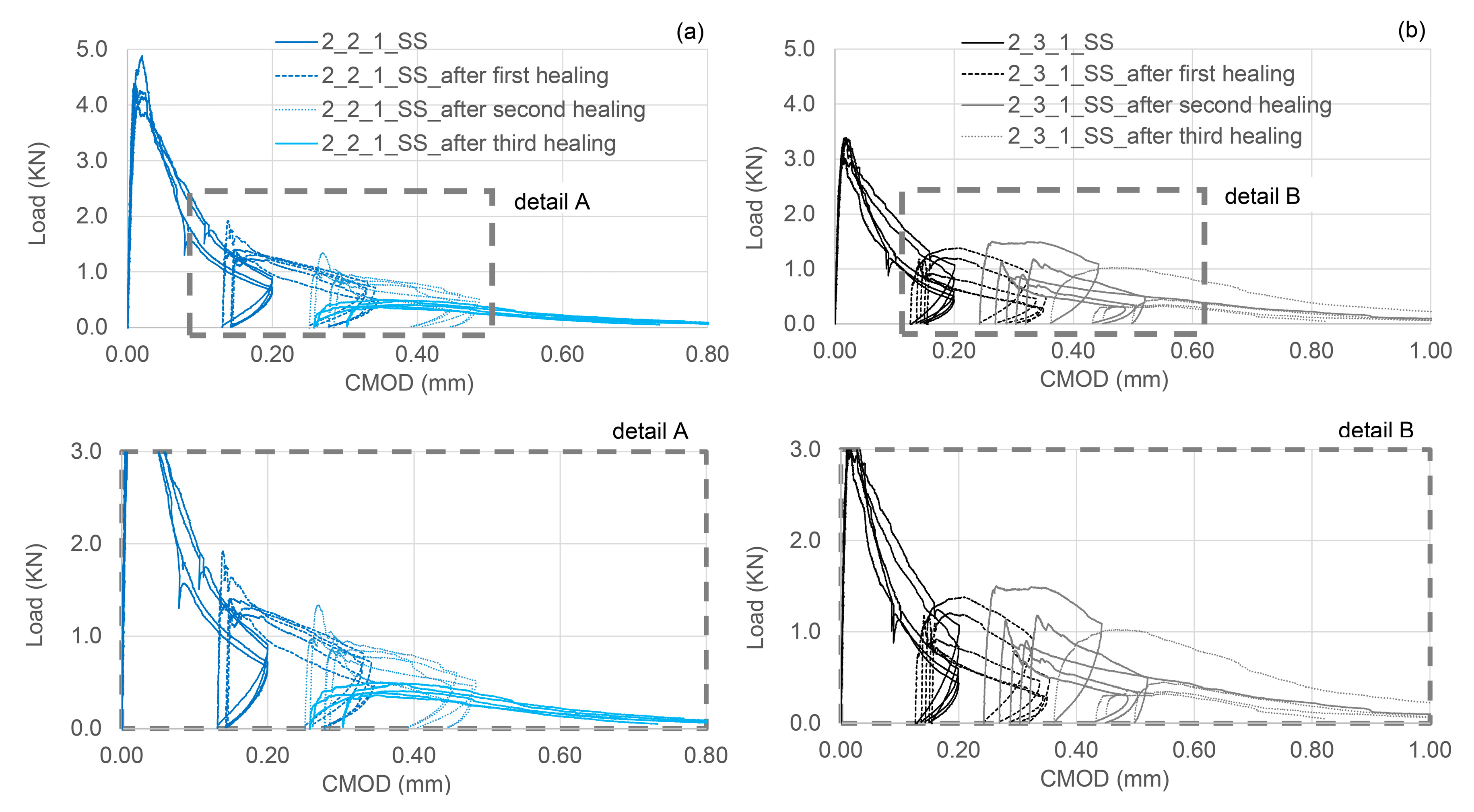
4.2. Group 2 Results
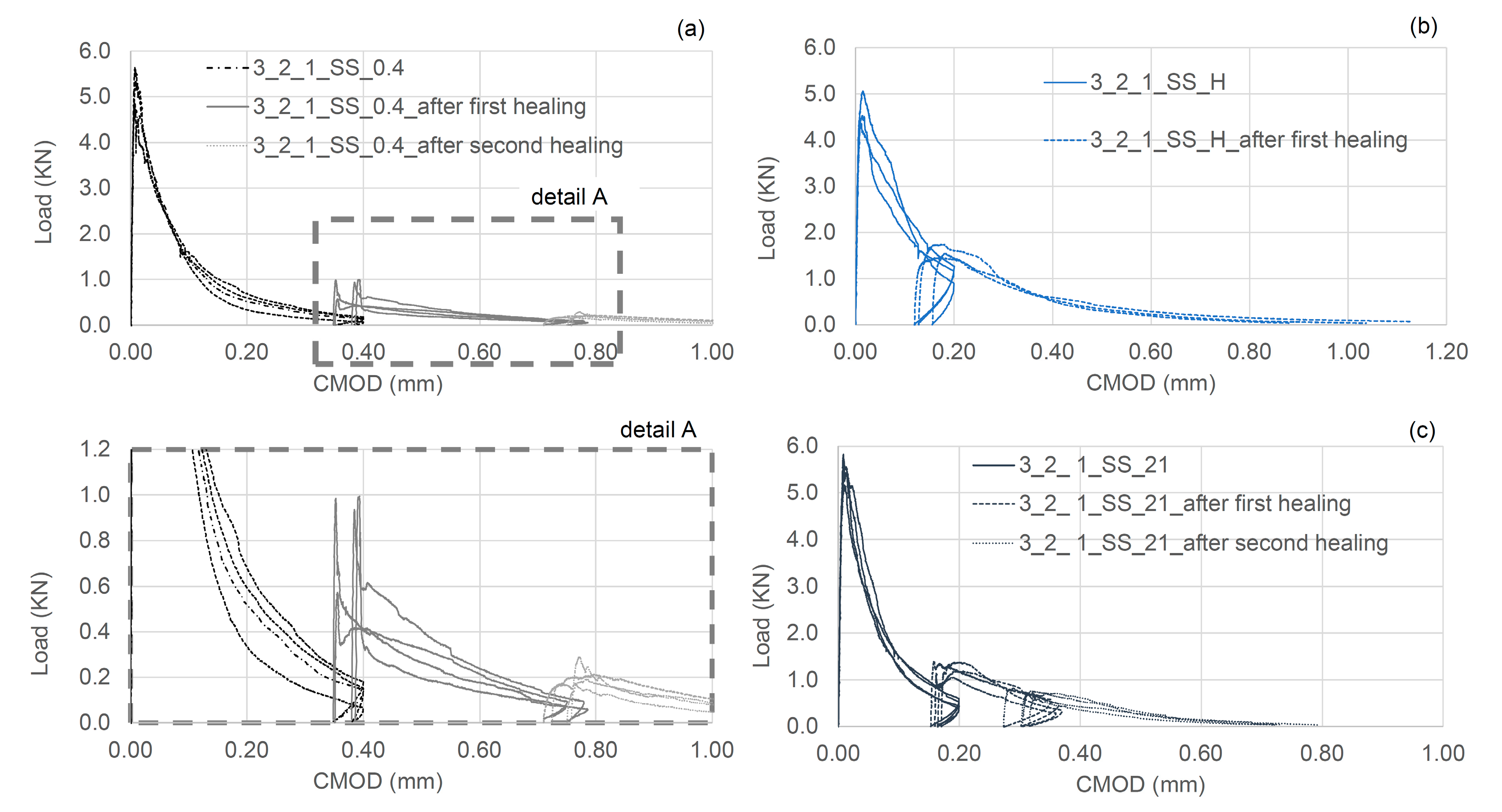
4.3. Group 3 Results
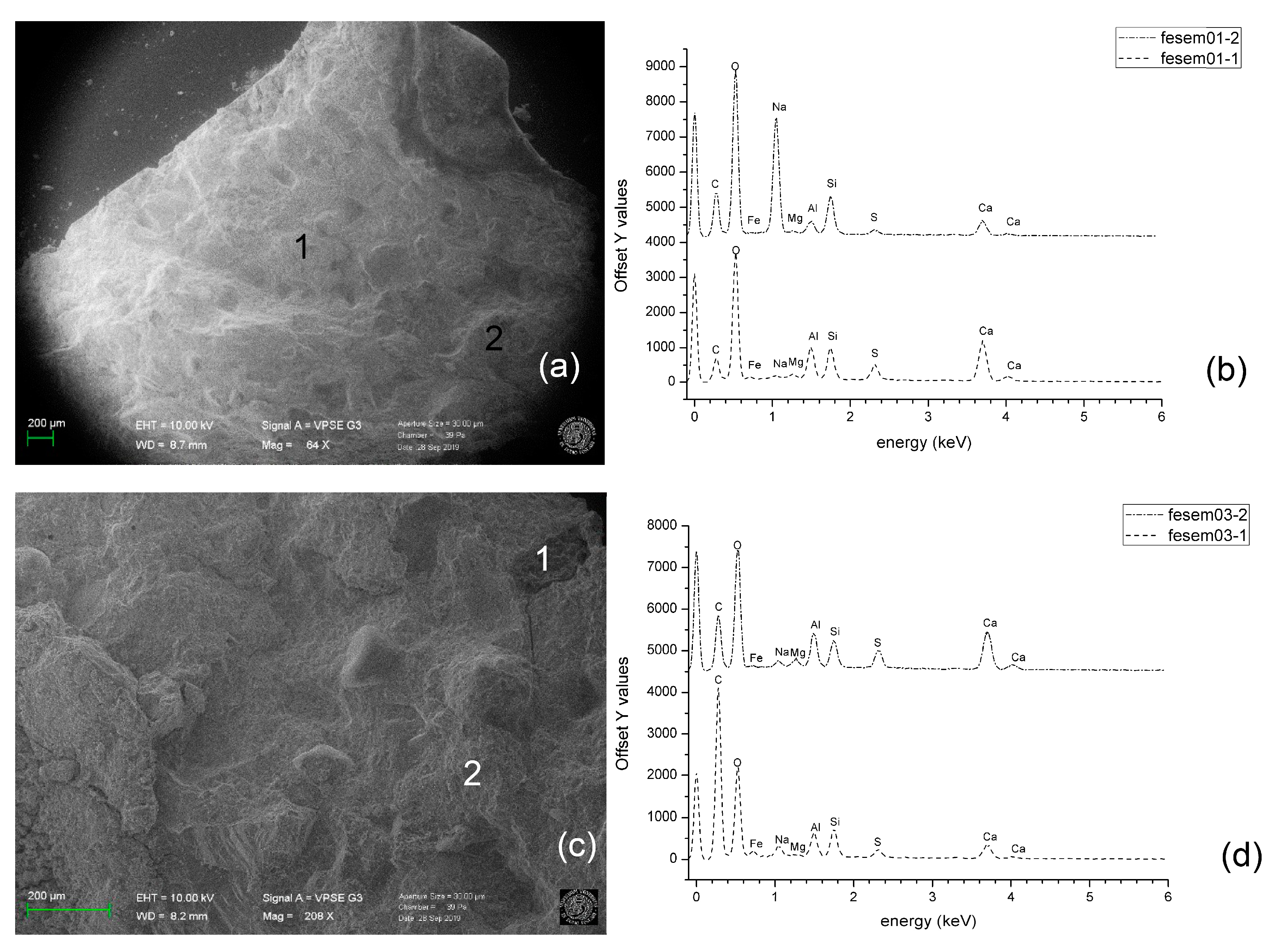
4.4. SEM/EDS Analyses
4.5. Summary Remarks
5. Conclusions
- The 3D printed Mini Vascular Networks (MVNs) form the basis of a viable self-healing system for concrete.
- Clear PLA is the most appropriate material for the MVNs, from amongst the 3D printed plastic filament materials tested.
- A spiral bond pattern with 5 mm pitch ribs provides sufficient bond between the MVN ligaments and the concrete matrix to ensure that the hollow ligament tubes rupture when crossed by a serviceability-size concrete crack.
- A double thickness (2 mm × 0.25 mm) ligament wall provides the best balance between impermeability and strength; the former being required to prevent premature healing-agent curing and the latter being such as to ensure rupture at the appropriate crack opening.
- The MVNs store sufficient healing agent to cure serviceability-sized cracks in concrete.
- The MVN system of interconnected channels overcomes the problems associated with capillary suction forces that prevent healing agents being released from closed-end tubular capsules.
- MVNs filled with SS can produce strength and stiffness recoveries of 20% and 75–80% respectively in prismatic concrete beams.
- The presence of MVNs has little effect on the pre-healed strength of concrete elements in which they are embedded.
- MVN systems filled with SS can heal multiple occurrences of damage, with (representative) strength and stiffness healing recoveries of 20%, 11%, 0% and 80%, 40% and 5% respectively for the first, second and third loading cycles.
- Samples with a high level of damage (i.e., a CMOD of 0.4 mm), characterised by a negligible residual flexural strength after the pre-cracking phase, exhibited significant healing behaviour; with strength and stiffness recoveries of 17% and 35% respectively.
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
Appendix A
Appendix A.1. MVN Ligament Design
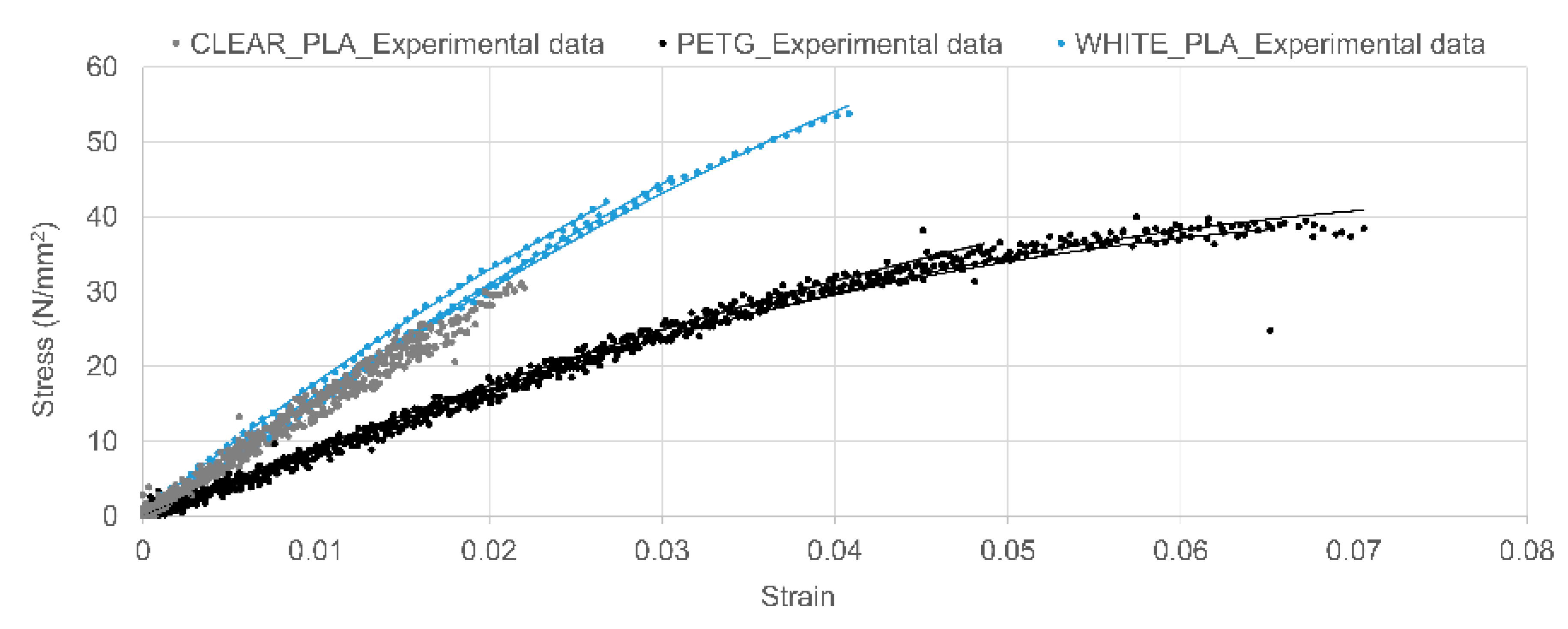
- Direct tension tests on 100 mm long 4 mm diameter bar specimens formed from different materials;
- The materials investigated included two forms of polylactic acid, (PLA) (i.e., clear-PLA and white-PLA) and polyethene terephthalate glycol-modified, (PETG).
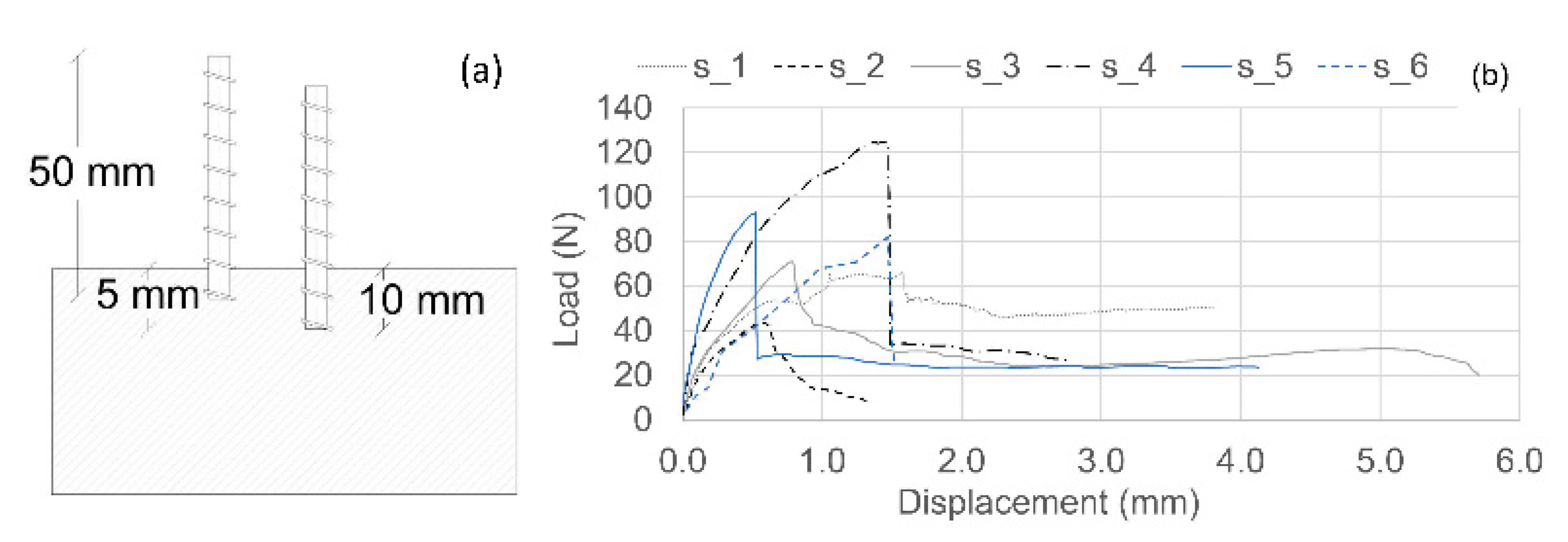
- Three sets of tests using 3D-printed tubular specimens, namely; (i) direct tension tests; (ii) direct pull-out tests, in which a tensile load was applied to the free end of a tube partially embedded in a cementitious block, and (iii) three-point bend tests on cementitious beams with embedded tubes. The parameters varied in these tests were the following:
- Filament material (PLA and PETG);
- External diameter (4 or 5 mm);
- Wall thickness (0.25 or 0.4 mm);
- Rib profile and spacing (annular or spiral ribs, spacing 3 mm or 5 mm).
Appendix A.1.1. Quantification of the Desired Ligament Behaviour
Appendix A.1.2. Direct Tension Tests on Solid Bar Specimens


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Filament | Datasheet | Experimental | ||||
|---|---|---|---|---|---|---|
| Strain at Rupture % | Tensile Modulus MPa | Tensile Stress at Rupture MPa | Strain at Rupture % (CoV%) | Tensile Modulus MPa (CoV%) | Tensile Stress at Rupture MPa (CoV%) | |
| Clear PLA a | 5.2 | 2346 | 45.6 | 2.0 (2) | 1502 (5) | 28.6 (10) |
| White PLA b | 6.0 | 3600 | 53.0 | 3.3 (18) | 1578 (4) | 46.9 (11) |
| PET-G c | 22.7 | 2020 | 50.4 | 6.1 (15) | 872 (1) | 36.3 (11) |
Appendix A.1.3. Pull-Out Tests on Tubular Samples

| Sample | Material | Rib Pattern (mm) | Outer Diameter (mm) | Wall Thickness (mm) | Peak Force (N) | Bond Strength (MPa) | Rupture Stress (MPa) | ||
|---|---|---|---|---|---|---|---|---|---|
| Embedment Depth | 10 mm | s_1 | white PLA | annular pitch, 5 | 4 | 0.25 | 71.7 | 0.57 | 24.3 |
| s_2 | PETG | annular pitch, 5 | 4 | 0.40 | 43.6 | 0.35 | 9.6 | ||
| s_3 | clear PLA | spiral pitch,3 | 5 | 0.25 | 71.1 | 0.45 | 19.1 | ||
| s_4 | clear PLA | spiral pitch,3 | 6 | 0.25 | 124.8 | 0.66 | 27.6 | ||
| 5 mm | s_5 | clear PLA | spiral pitch,3 | 5 | 0.25 | 93.0 | 1.18 | 24.9 | |
| s_6 | PETG | annular pitch, 5 | 4 | 0.40 | 81.2 | 1.31 | 14.2 |
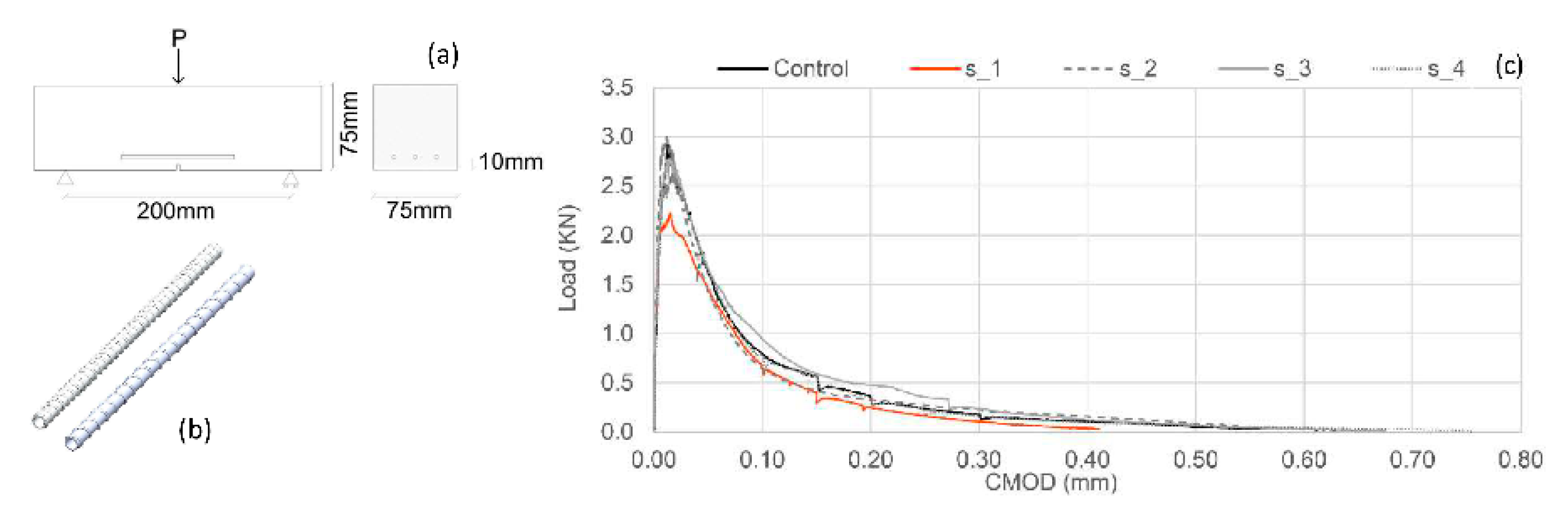
Appendix A.1.4. Three-Point Bend Tests

| Sample | Material | Rib Pattern (mm) | Outer Diameter (mm) | Wall Thickness (mm) | Peak Load (kN) |
|---|---|---|---|---|---|
| Control | - | - | - | - | 2.9 |
| s_1 | clear PLA | spiral, pitch 5mm | 5 | 0.25 | 2.2 |
| s_2 | clear PLA | annular, pitch 5mm | 4 | 0.40 | 3.0 |
| s_3 | clear PLA | spiral, pitch 5mm | 5 | 0.40 | 2.8 |
| s_4 | clear PLA | spiral, pitch 3mm | 5 | 0.25 | 2.6 |
Appendix A.1.5. Conclusions from Preliminary Tests
Appendix A.2. Healing Agent
| Types of Coatings | Desiccator | State of CA | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Waterproof PVA/Water 0.5:1 | Waterproof PVA/Water 1:1 | PVA Glue | Epoxy Hardener | Paraffin Wax | 24 h | 24 h | 48 h | 72 h | |||
| 1 Layer | 2 Layers | 1 Layer | 2 Layers | 1 Layer | 1 Layer | 1 Layer | |||||
| PC20 | S a | ||||||||||
| + | + | s | |||||||||
| + | + | L b | s/l c | s | |||||||
| + | + | l | s/l | s | |||||||
| + | + | l | l | s | |||||||
| + | + | s | |||||||||
| + | + | l | s | ||||||||
| + | + | l | s/l | s | |||||||
| PC60 | l | s/l | s/l | ||||||||
| + | + | l | s/l | s/l | |||||||
| PC90 | l | s | |||||||||
References
- Roig-Flores, M.; Moscato, S.; Ferrara, L. Self-capability of concrete with crystalline admixtures in different environments. Constr. Build. Mater. 2015, 86, 1–11. [Google Scholar] [CrossRef]
- Ferrara, L.; Krelani, V.; Carsana, M. A ‘‘fracture testing’’ based approach to assess crack healing of concrete. Constr. Build. Mater. 2014, 68, 535–551. [Google Scholar] [CrossRef]
- De Nardi, C.; Bullo, S.; Ferrara, L.; Ronchin, L.; Vavasori, A. Effectiveness of crystalline admixtures and lime/cement coated granules in engineered self-healing capacity of lime mortars. Mater. Struct. 2017, 50, 190–202. [Google Scholar] [CrossRef]
- Homma, D.; Mihashi, H.; Nishiwaki, T. Self-Healing capability of fibre reinforced cementitious composites. J. Adv. Concr. Technol. 2009, 7, 217–228. [Google Scholar] [CrossRef]
- Dry, C. Matrix cracking repair and filling using active and passive modes for smart timed release of chemicals from fibers into cement matrices. Smart Mater. Struct. 1994, 3, 118. [Google Scholar] [CrossRef]
- Lee, H.; Wong, H.; Buenfeld, N. Potential of superabsorbent polymer for self-sealing cracks in concrete. Adv. Appl. Ceram. 2010, 109, 296–302. [Google Scholar] [CrossRef]
- White, S.; Sottos, N.; Geubelle, P. Autonomic healing of polymer composites. Nature 2001, 409, 794–797. [Google Scholar] [CrossRef]
- Dry, C. Timed release of chemicals into cementitious material after the material has hardened to repair cracks, rebond fibers, and increase flexural toughening. In Fracture Mechanics: 25th Volume, ASTM STP 1220; American Society for Testing and Materials: Philadelphia, PA, USA, 1994. [Google Scholar]
- Dry, C.; McMillan, W. Three-part methylmethacrylate adhesive system. Smart Mater. Struct. 1994, 53, 291. [Google Scholar]
- Tsangouri, E. A decade of research on self-healing concrete. In Sustainable Construction and Building Materials; Hemeda, S., Ed.; IntechOpen: London, UK, 2018; pp. 21–36. [Google Scholar]
- Joseph, C.; Gardner, D.; Jefferson, A.; Isaacs, B.; Lark, B. Self-healing cementitious materials: A review of recent work. Proc. Inst. Civ. Eng. Constr. Mater. 2011, 164, 29–41. [Google Scholar] [CrossRef]
- Van Tittelboom, K.; De Belie, N. Self-healing concrete: Suitability of different healing agents. Int. J. 3R’s 2010, 1, 12–21. [Google Scholar]
- Sun, L.; Yu, W.; Ge, Q. Experimental research on the self-healing performance of micro-cracks in concrete bridge. Adv. Mater. Res. 2011, 250–253, 28–32. [Google Scholar] [CrossRef]
- Li, V.; Lim, Y.; Chan, Y. Feasibility study of a passive smart self-healing cementitious composite. Compos. Part B Eng. B 1998, 29, 819–827. [Google Scholar] [CrossRef]
- Gardner, D.; Jefferson, A.; Hoffman, E.; Lark, R. Simulation of the capillaryflow of an autonomic healing agent in discretecracks in cementitious materials. Cem. Concr. Res. 2014, 58, 35–44. [Google Scholar] [CrossRef]
- Dry, C. Design of self-growing, self-sensing and self-repairing materials for engineering applications. In Proceedings of the Society of Photo-Optical Instrumentation Engineers (SPIE), Melbourne, Australia, 13–15 December 2000; Wilson, A.R., Asanuma, H., Eds.; SPIE: Bellingham, WA, USA, 2001; pp. 23–29. [Google Scholar]
- Mihashi, H.; Kaneko, Y.; Nishiwaki, T.; Otsuka, K. Fundamental study on development of intelligent concrete characterized by self-healing capability for strength. Trans. Jpn. Concr. Inst. 2000, 22, 441–450. [Google Scholar]
- Mihashi, H.; Nishiwaki, T. Development of engineered self-healing and self-repairing concrete-state-of-the-art report. J. Adv. Concr. Technol. 2012, 10, 170–184. [Google Scholar] [CrossRef]
- Van Tittelboom, K.; De Belie, N.; Van Loo, D.; Jacobs, P. Self-healing efficiency of cementitious materials containing tubular capsules filled with healing agent. Cem. Concr. Compos. 2011, 33, 497–505. [Google Scholar] [CrossRef]
- Huang, H.; Guang, Y. Application of sodium silicate solution as self-healing agent in cementitious materials. In International RILEM Conference on Advances in Construction Materials through Science and Engineering; Leung, C., WAN, K.T., Eds.; RILEM Publications SARL: Paris, France, 2011; pp. 530–536. [Google Scholar]
- Gilford, S.; Hassan, M.; Rupnow, T.; Barbato, M.; Okeil, M.; Asadi, A. Dicyclopentadiene and sodium silicate microencapsulation for self-healing of concrete. J. Mater. Civ. Eng. 2014, 26, 886–896. [Google Scholar] [CrossRef]
- Pelletier, M.; Brown, R.; Shukla, A.; Bose, A. Self-Healing Concrete with a Microencapsulated Healing Agent. 2011. Available online: https://pdfs.semanticscholar.org/e48b/937bde7c53 ce059d464822ebc837a31647dc.pdf (accessed on 25 October 2019).
- Formia, A.; Terranova, S.; Antonaci, P.; Pugno, N.T.M. Setup of extruded cementitious hollow tubes ascontaining/releasing devices in self-healing systems. Materials 2015, 8, 1897–1923. [Google Scholar] [CrossRef]
- Joseph, C.; Lark, R.; Isaacs, B.; Gardner, D.; Jefferson, A. Experimental investigation of adhesive-based self-healing of cementitious materials. Mag. Concr. Res. 2010, 62, 831–843. [Google Scholar] [CrossRef]
- Minnebo, P.; Thierens, G.; de Valck, G.; van Tittelboom, K.; de Belie, N.; van Hemelrijck, D.; Tsangouri, E. A novel design of autonomously healed concrete: Towards a vascular healing network. Materials 2017, 10, 49. [Google Scholar] [CrossRef]
- Sangadji, S.; Schlangen, E. Self healing of concrete structure—Novel approach using porous network concrete. J. Adv. Concr. Technol. 2012, 10, 185–194. [Google Scholar] [CrossRef]
- Davies, R.; Jefferson, A.; Lark, R.; Gardner, D. A novel 2d vascular network in cementitious materials. In Proceedings of the Concrete—Innovation and Design, Fib Symposium, Copenhagen, Denmark, 18–20 May 2015. [Google Scholar]
- Dry, C. Repair and prevention of damage due to transverse shrinkage cracks in bridge decks. Smart Struct. Mater. 1999, 3671, 253–256. [Google Scholar]
- Davies, R.; Teall, O.; Pilegis, M.; Kanellopoulos, A.; Sharma, T.; Jefferson, A.; Gardner, D.; Al-Tabbaa, A.; Paine, K.; Lark, R. Large scale application of self-healing concrete: Design, construction, and testing. Front. Mater. 2018, 5, 51. [Google Scholar] [CrossRef]
- Greenwood, N.; Earnshaw, A. Chemistry of the Elements; Elsevier: Oxford, UK, 1997. [Google Scholar]
- Ferrara, L.; Krelani, V.; Moretti, F.; Roig Flores, M.; Serna Ros, P. Effects of autogenous healing on the recovery of mechanical performance of High Performance Fibre Reinforced Cementitious Composites (HPFRCCs): Part 1. Cem. Concr. Compos. 2017, 83, 76–100. [Google Scholar] [CrossRef]
- Feiteira, J.; Gruyaert, E.; de Belie, N. Self-healing of moving cracks in concrete by means of encapsulated polymer precursors. Constr. Build. Mater. 2016, 102, 671–678. [Google Scholar] [CrossRef]
- Neville, A. Properties of Concrete; Longman: London, UK, 1981. [Google Scholar]
- Forgacs, G. Perfusable vascular networks. Nat. Mater. 2012, 11, 746–747. [Google Scholar] [CrossRef]
- Sheppard, W. Corrosion and Chemical Resistant Masonry Materials Handbook; U.S. Department of Energy Office of Scientific and Technical Information: Oak Ridge, TN, USA, 1986.















| Variant |  |  |  |
|---|---|---|---|
| PLA filament | white | white/clear | clear |
| Printing orientation (ϑ) | flat | flat | Axis x + 15°; y + 15° |
| Outer wall print speed | 60 mm/s | 50 mm/s | 40 mm/s |
| Printing temperature | 210 °C | 200 °C | 195 °C |
| Ribs | - | Annular | Spiral |
| Edge length (mm) | 40 | 42 | 44 |
| Wall thickness (mm) | 1 | 0.5 | 0.5 × (0.25 × 2 a) |
| Inner diameter (mm) | 3 | 3.5 | 5 |
| Ink evidence during the flexural test | no | no | yes |
| Volume of healing agent | 1.7 cm3 | 2.4 cm3 | 5.2 cm3 |
| Impermeability | no | no | yes |
| Sample Designation | No. Samples | No. TETs | Healing Agent | CMOD (mm) | First Curing/Healing Period (days) | CMOD (mm) | Second Curing/Healing Period (days) | |
|---|---|---|---|---|---|---|---|---|
| GROUP 1 | 1_C_1 | 3 | 0 | - | - | 1 | - | - |
| 1_C_1 | 3 | 0 | - | - | 14 | - | - | |
| 1_2_1 EMPTY | 3 | 2 | - | - | 14 | - | - | |
| 1_2_1_SS | 5 | 2 | SS | 0.2 | 14 | - | - | |
| 1_3_1_SS | 5 | 3 | SS | 0.2 | 14 | - | - | |
| GROUP 2 | 2_C_1 | 3 | 0 | - | 0.2 | 14 | 0.2 | 14 |
| 2_C_28 | 3 | 0 | - | - | 28 | - | - | |
| 2_C_1 s | 3 | 0 | - | - | 14 | - | - | |
| 2_2_28 EMPTY s | 3 | 0 | - | - | 28 | - | - | |
| 2_2_1_EMPTY s | 3 | 0 | - | 0.2 | 14 | 0.2 | 14 | |
| 2_2_1_SS s | 5 | 2 | SS | 0.2 | 14 | 0.2 | 14 | |
| 2_3_1_SS s | 5 | 3 | SS | 0.2 | 14 | 0.2 | 14 | |
| GROUP 3 | 3_2_1_SS_0.4 | 3 | 2 | SS | 0.4 | 14 | 0.4 | 14 |
| 3_2_1_SS_H * | 3 | 2 | SS | 0.2 | 21 | - | - | |
| 3_2_ 1_SS_21 | 3 | 2 | SS | 0.2 | 21 | - | - |
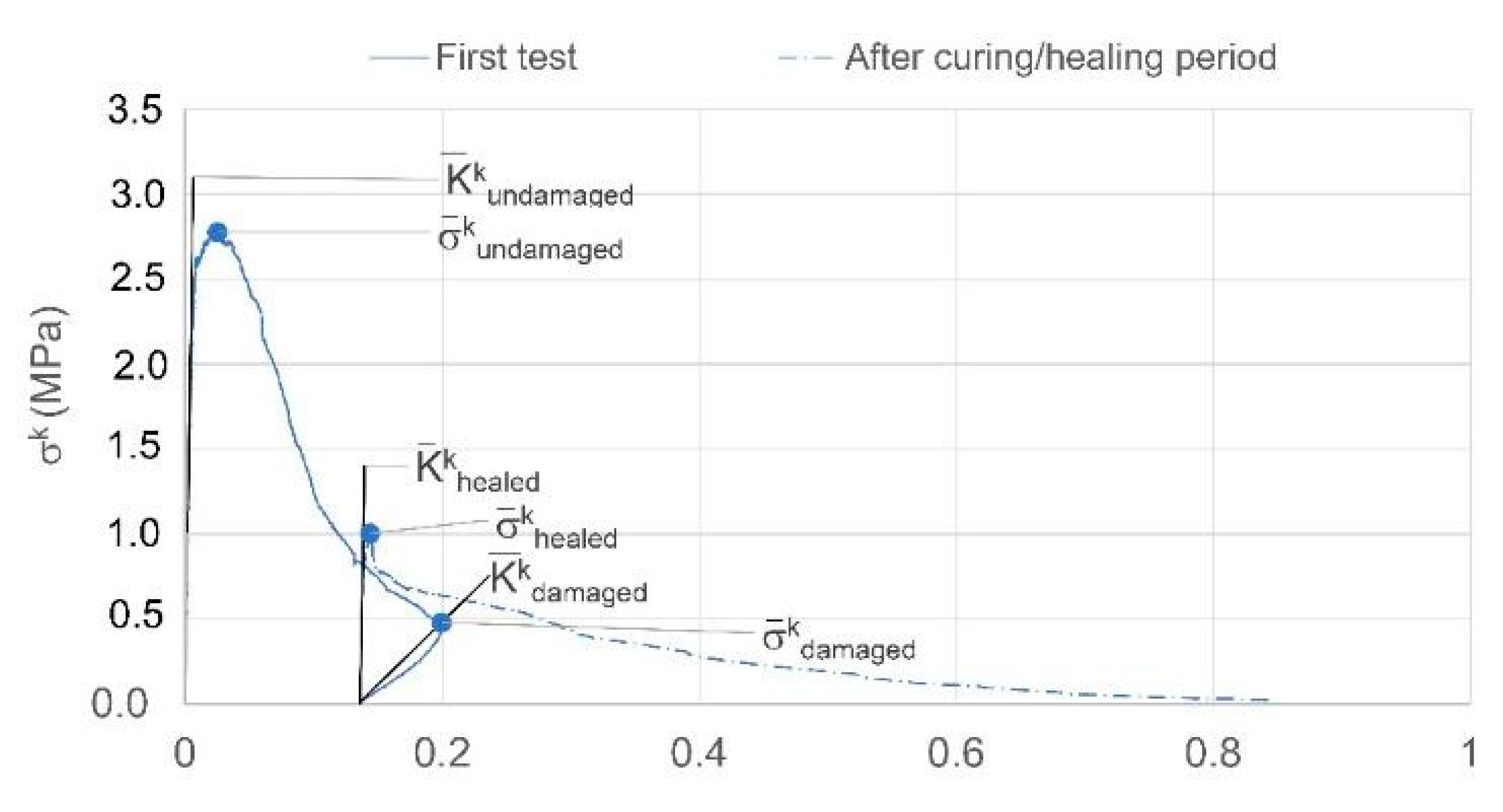
| Group 1 | First Healing Cycle | |||||
|---|---|---|---|---|---|---|
| σk_1undamaged MPa (CoV%) | σk_1damaged MPa (CoV%) | σk_14healed MPa (CoV%) | ||||
| 1_C_1 | 3.83 (5) | - | - | - | - | - |
| 1_C_1 | 4.29 (2) | 0.54 (12) | 0.60 (22) | 2 | 8 | 23 |
| 1_2_1_EMPTY | 3.41 (3) | - | - | |||
| 1_2_1_SS | 3.71 (12) | 0.58 (22) | 1.10 (24) | 16 | 73 | 36 |
| 1_3_1_SS | 3.52 (9) | 0.70(7) | 1.00 (12) | 12 | 67 | 85 |
| Flexural Strength (MPa) (CoV%) | ||||||||
|---|---|---|---|---|---|---|---|---|
| 1st Healing Cycle | 2nd Healing Cycle | 3rd Healing Cycle | ||||||
| Group 2 | σk_1undamaged | σk_28undamaged | σk_1damaged | σk_14healed | σk_14damaged | σk_28healed | σk_28damaged | σk_42healed |
| 2_C_1 | 4.22 (10) | 0.51 (12) | 0.58 (22) | 0.37 (39) | 0.39 (45) | - | - | |
| 2_C_28 | - | 7.26 (8) | - | - | - | - | - | - |
| 2_C_1 s | 3.86 (3) | - | - | - | - | - | - | - |
| 2_2_28 EMPTY s | - | 7.40 (12) | - | - | - | - | - | - |
| 2_2_1_EMPTY s | 3.41 (9) | - | 0.9 (14) | 0.9 (12) | 0.5 (24) | 0.47 (32) | - | - |
| 2_2_1_SS s | 3.16 (7) | - | 0.55 (17) | 1.05 (16) | 0.42 (18) | 0.72 (17) | 0.30 (27) | 0.30 (12) |
| 2_3_1_SS s | 3.22 (5) | - | 0.67 (31) | 1.19 (10) | 0.48 (49) | 0.78 (22) | 0.39 (54) | 0.38 (52) |
| 1st Healing Cycle | 2nd Healing Cycle | 3rd Healing Cycle | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Group_2 | (%) | (%) | (%) | (%) | (%) | (%) | (%) | (%) | (%) |
| 2_C_1 | 2 | 7 | 26 | 1 | 2 | 12 | - | - | - |
| 2_C_28 | - | - | - | - | - | - | - | ||
| 2_C_1s | - | - | - | - | - | - | - | - | - |
| 2_2_28 EMPTYs | - | - | - | - | - | - | - | ||
| 2_2_1_EMPTYs | 0 | 0 | - | 0 | 0 | 0 | - | - | - |
| 2_2_1_SSs | 19 | 75 | - | 11 | 40 | 47 | 0 | 5 | 24 |
| 2_3_1_SSs | 20 | 79 | - | 11 | 33 | 48 | 0 | 9 | 44 |
| 1st Healing Cycle | 2nd Healing Cycle | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Group_3 | σk_1undamaged (CoV%) (MPa) | σk_1damaged (CoV%) (MPa) | σk_14healed (CoV%) (MPa) | (%) | (%) | (%) | σk_14damaged (CoV%) (MPa) | σk_28healed (CoV%) (MPa) | (%) | (%) | (%) |
| 3_C_1 | 4.02 (6) | - | - | - | - | - | - | ||||
| 3_2_1_SS_0.4 | 3.73 (7) | 0.08 (42) | 0.69 (3) | 17 | 35 | - | 0.05 (19) | 0.16 (20) | 3 | 4 | 8 |
| 3_2_1_SS_H * | 3.31 (6) | 0.76 (15) | 1.12 (7) | 14 | 40 | 89 | - | - | - | - | - |
| σk_1undamaged (CoV%) (MPa) | σk_1damaged (CoV%) (MPa) | σk_21healed (CoV%) (MPa) | (%) | (%) | (%) | σk_21damaged (CoV%) (MPa) | σk_42healed (CoV%) (MPa) | (%) | (%) | (%) | |
| 3_2_1_SS_21 | 3.96 (4) | 0.33 (11) | 0.90(9) | 16 | 67 | - | 0.29 (29) | 0.52 (8) | 6 | 24 | 21 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Nardi, C.; Gardner, D.; Jefferson, A.D. Development of 3D Printed Networks in Self-Healing Concrete. Materials 2020, 13, 1328. https://doi.org/10.3390/ma13061328
De Nardi C, Gardner D, Jefferson AD. Development of 3D Printed Networks in Self-Healing Concrete. Materials. 2020; 13(6):1328. https://doi.org/10.3390/ma13061328
Chicago/Turabian StyleDe Nardi, Cristina, Diane Gardner, and Anthony Duncan Jefferson. 2020. "Development of 3D Printed Networks in Self-Healing Concrete" Materials 13, no. 6: 1328. https://doi.org/10.3390/ma13061328
APA StyleDe Nardi, C., Gardner, D., & Jefferson, A. D. (2020). Development of 3D Printed Networks in Self-Healing Concrete. Materials, 13(6), 1328. https://doi.org/10.3390/ma13061328