Autogenous Dentin Graft in Bone Defects after Lower Third Molar Extraction: A Split-Mouth Clinical Trial

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.2.1. Inclusion Criteria
- Patients of either sex aged between 18 and 25 years.
- Indications for bilateral extraction of impacted LTMs.
- Presence of lower second molars.
- Patients in good health (ASA I or II).
- Patients able to understand and carry out instructions given by the researchers.
2.2.2. Exclusion Criteria
- Pregnant or lactating women.
- Patients in treatment with nonsteroidal anti-inflammatory drugs (NSAIDs).
- Patients with periodontal diseases.
2.3. Sample Size, Blinding, and Randomization
2.4. Surgical Procedure
2.5. Evaluation of Outcomes
2.5.1. Pre-Operative Variables
- Facial measurements were taken with silk thread measuring trago-pogonion distance, external labial commissure to the tragus, and from the gonion to the external canthus of the eye, following Amin and Laskins’ modified criteria for evaluating post-operative inflammation [22].
- Mouth opening capacity was measured with an analogue caliper (Acha®, Eibar, Spain), measuring a straight line from upper incisor edge to lower incisor edge to subsequently evaluate reductions in post-operative mouth open capacity.
2.5.2. Intra-Operative Variables
2.5.3. Post-Operative Variables
- Inflammation was evaluated by measuring facial patterns 48 h and 1 week after surgery. Mouth opening capacity was measured at the same times with an analogue caliper.
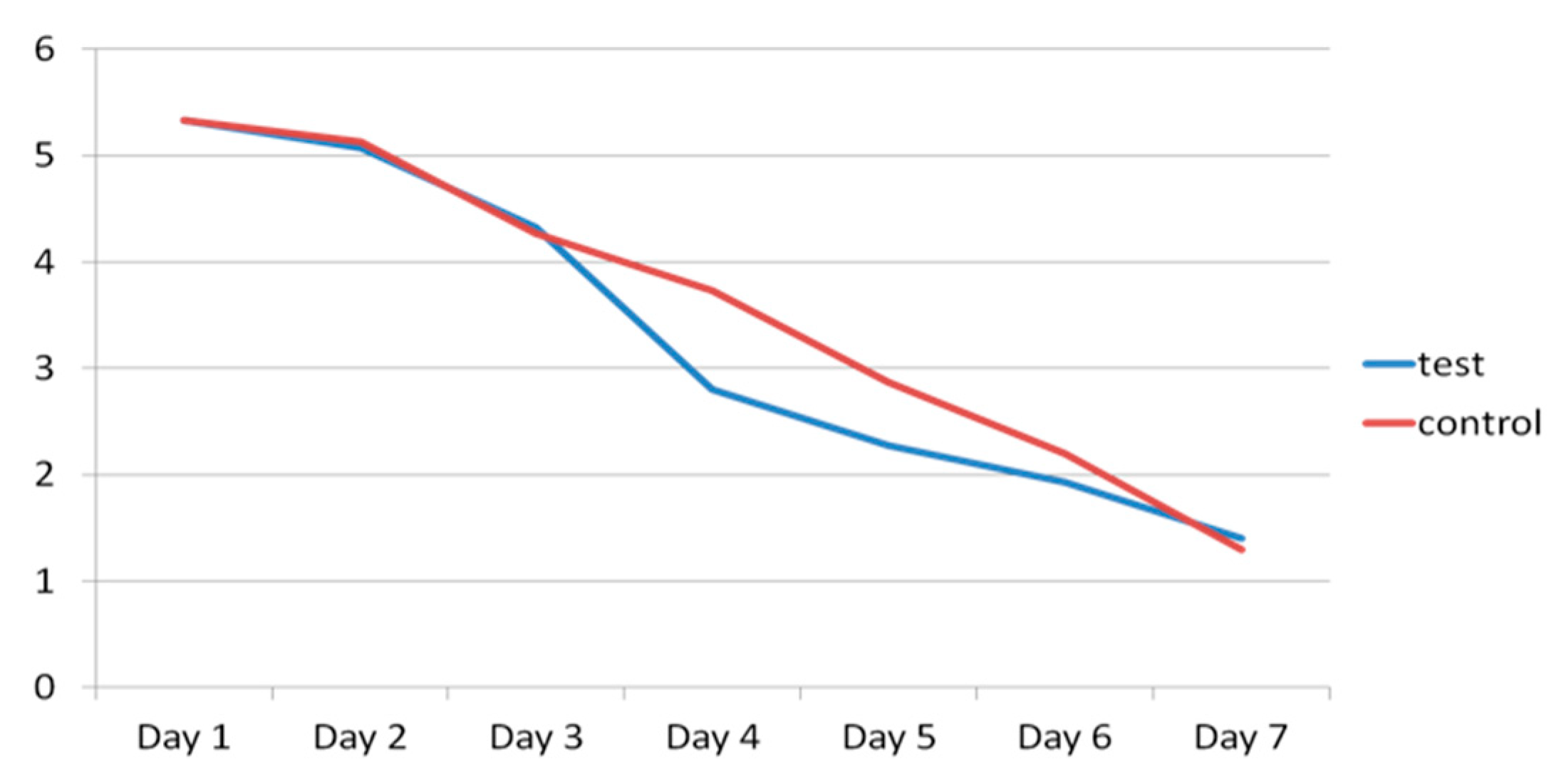
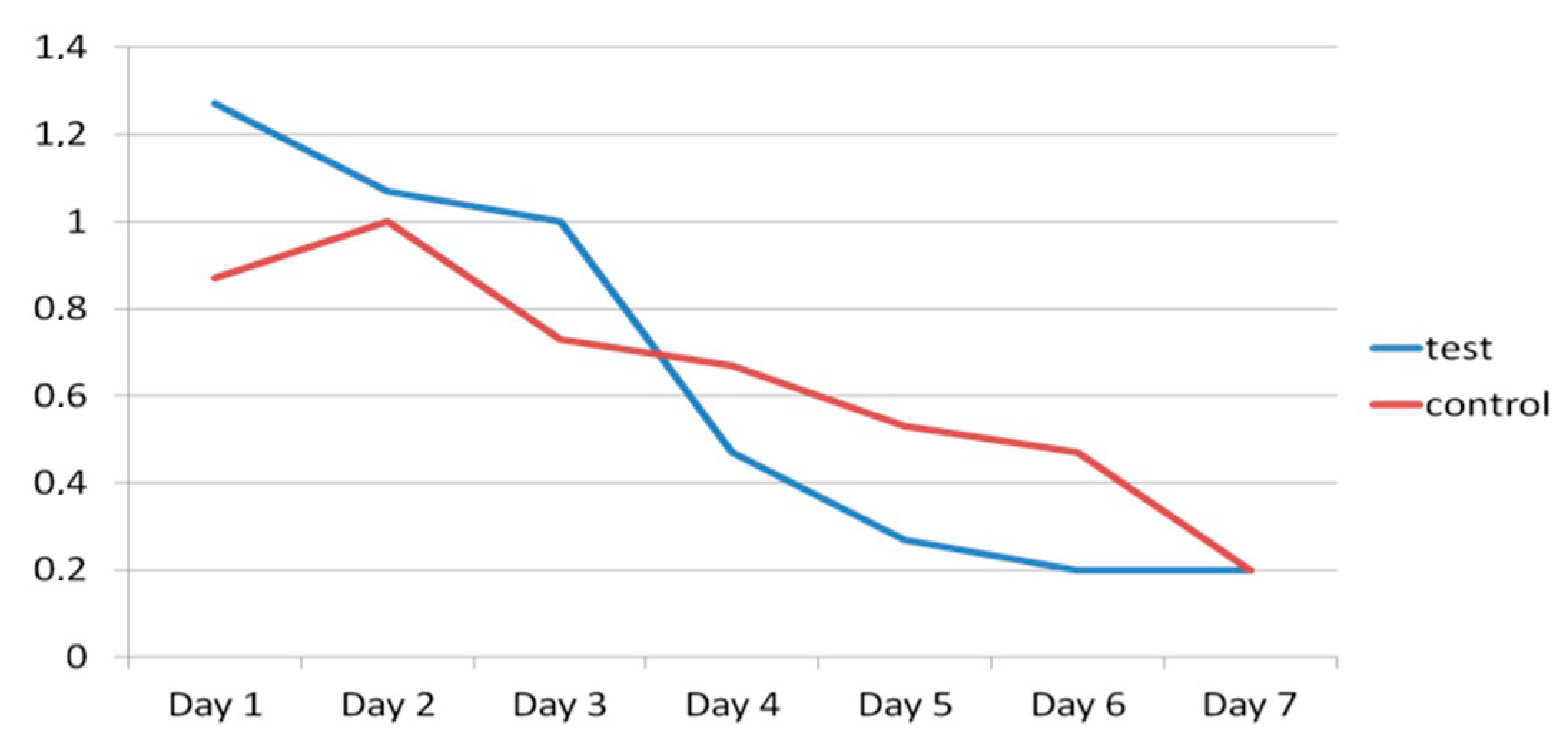
- Pain was evaluated using a visual analogue scale (VAS) scored as 1–10, 1 representing minimal pain and 10 maximum pain, every day for 7 days after extraction surgery. The number of rescue analgesics taken (1, 2 or 3 per day) during the 7 days after surgery was recorded.
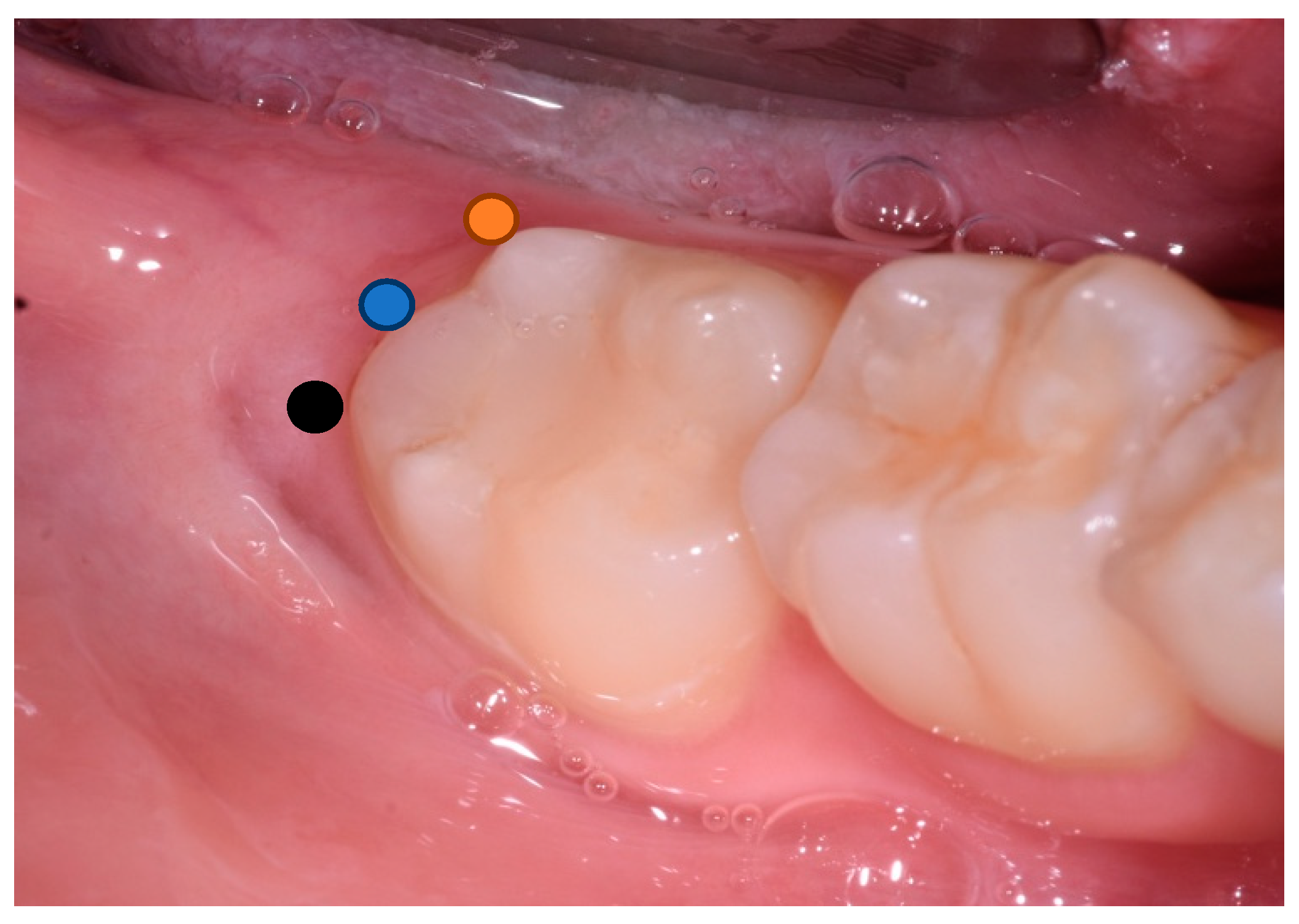
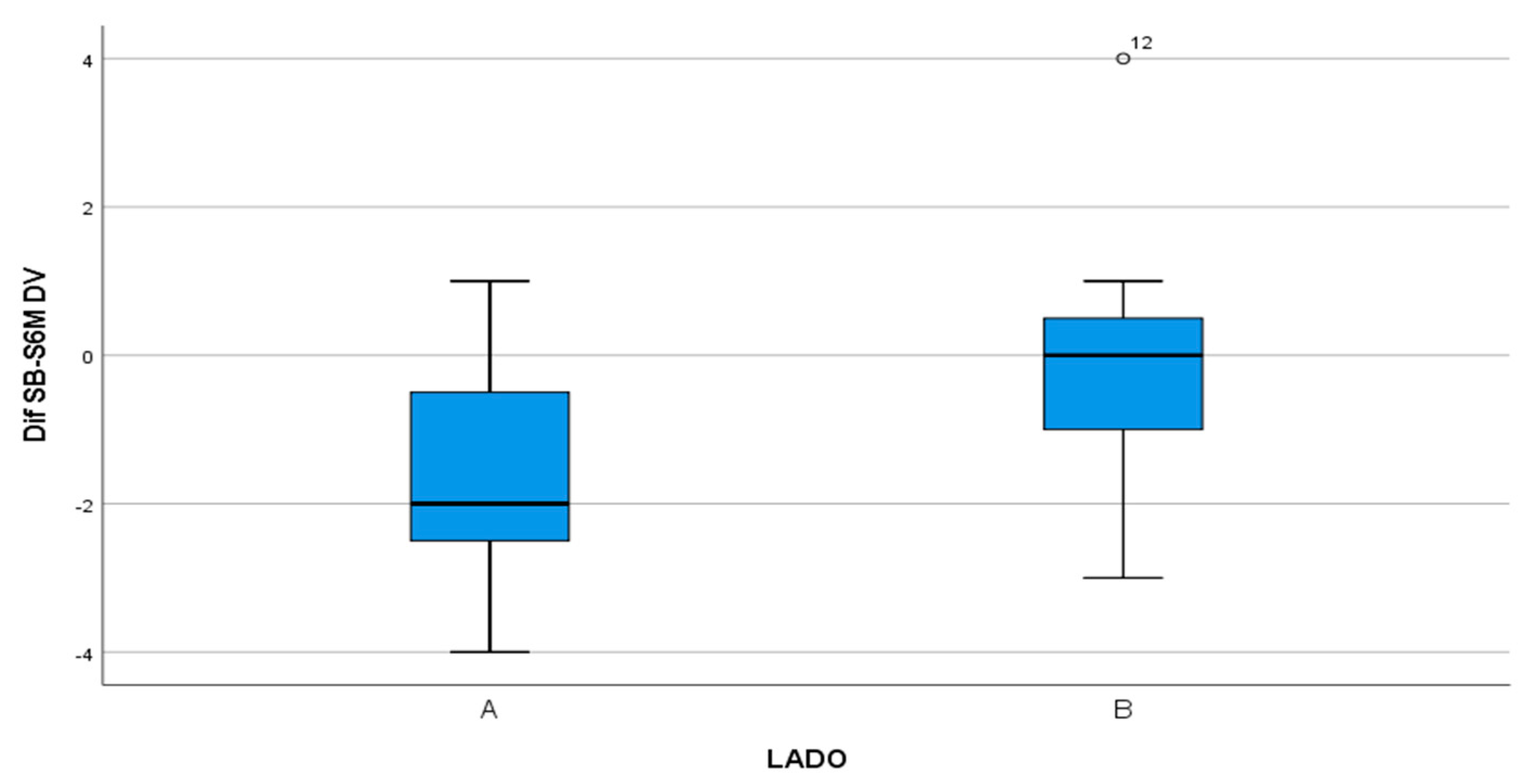
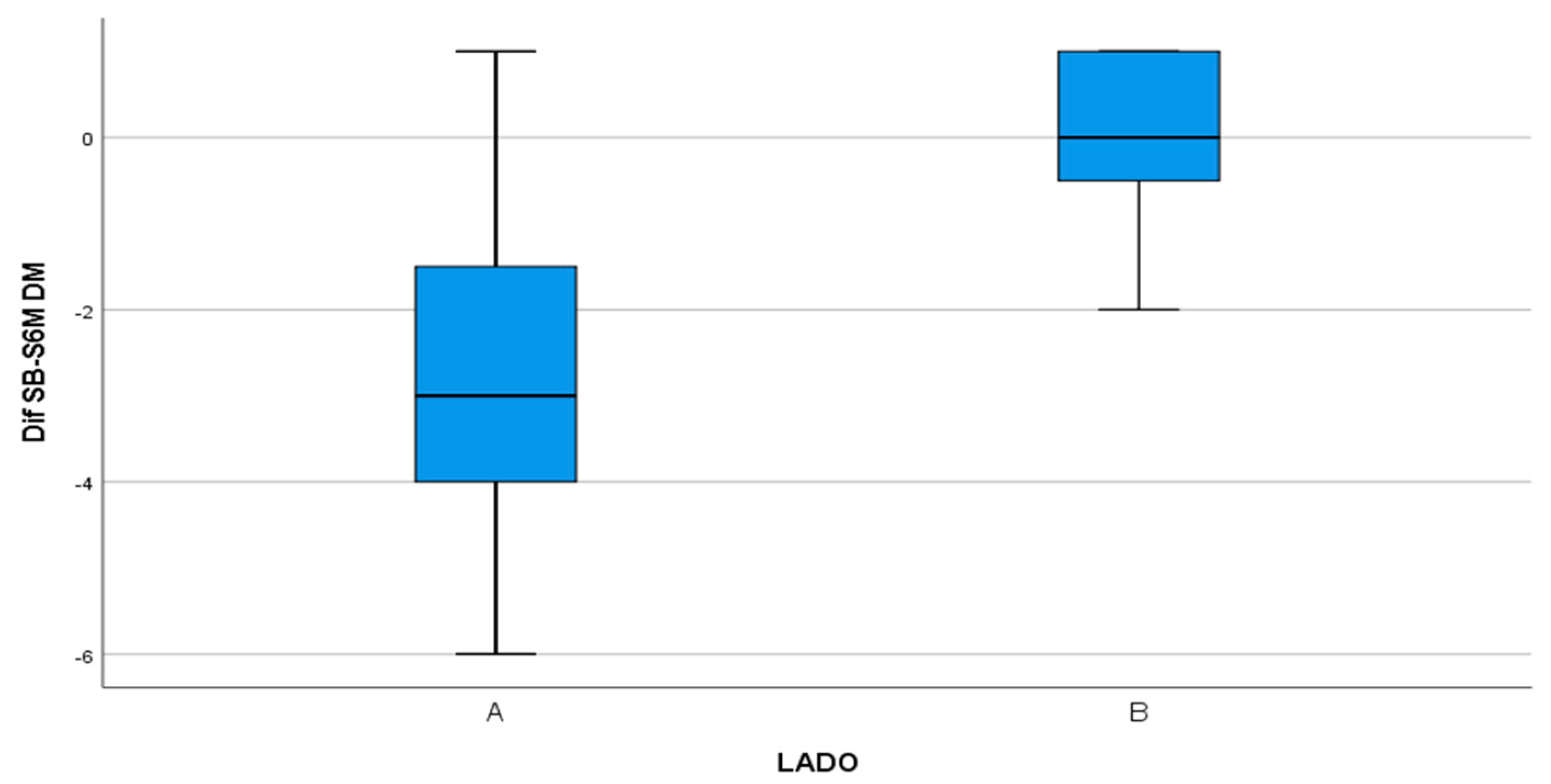
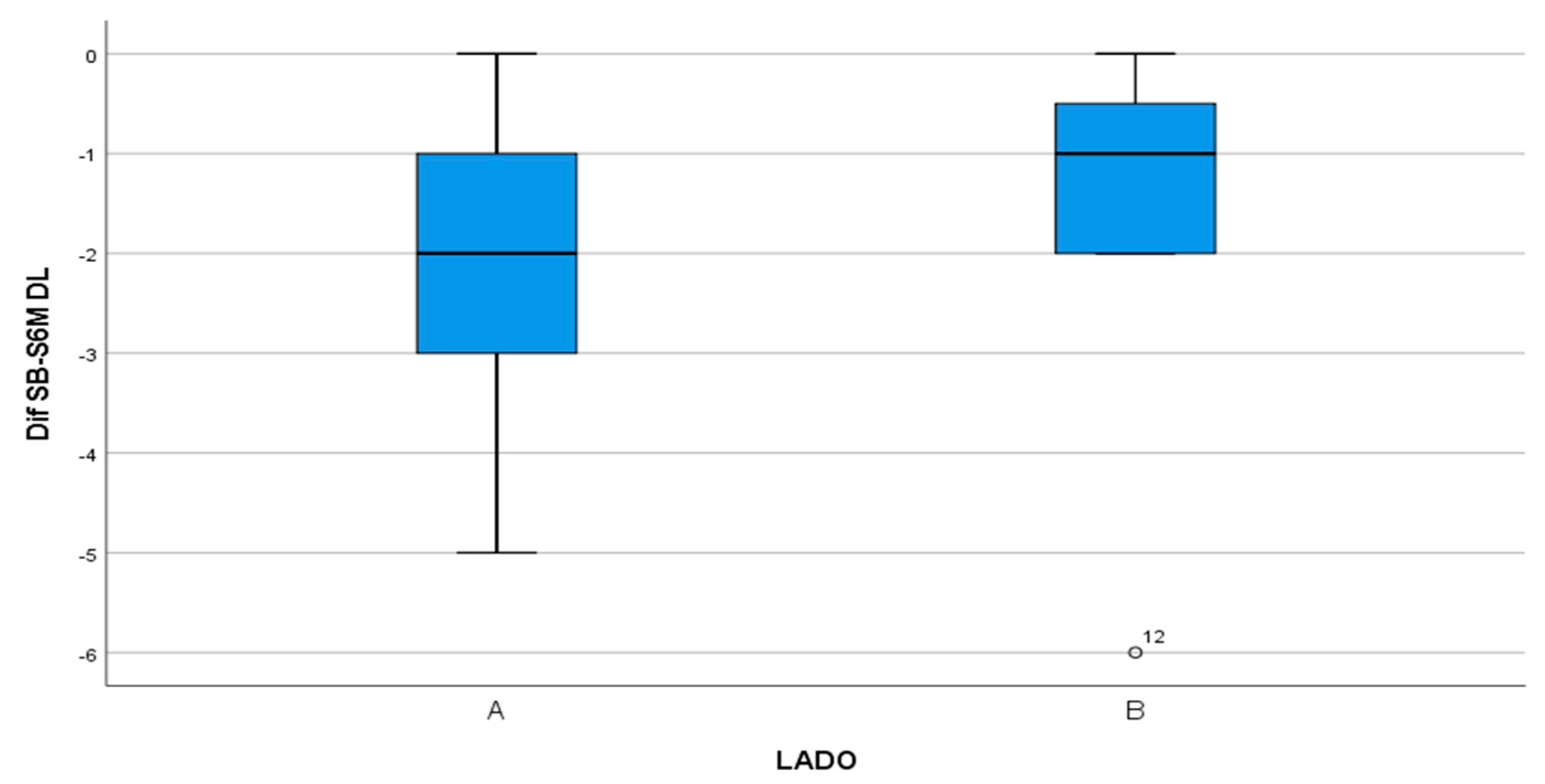
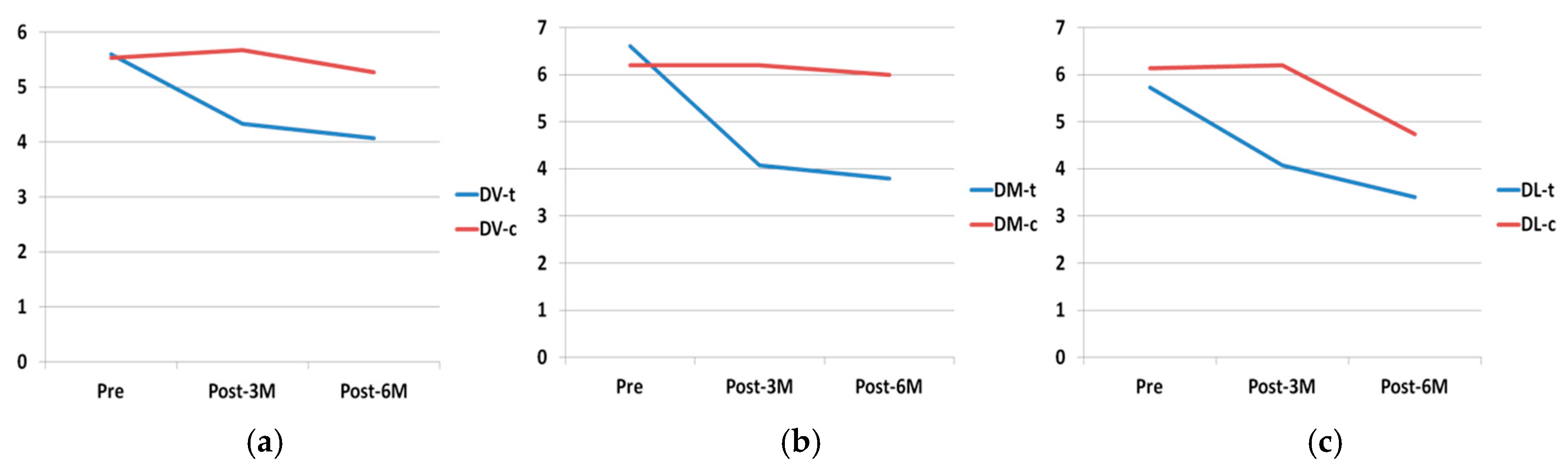
- Probing depth was measured 3 and 6 months after surgery at the DV, DM and DL points on the distal aspect of the second molar as shown in Figure 3.
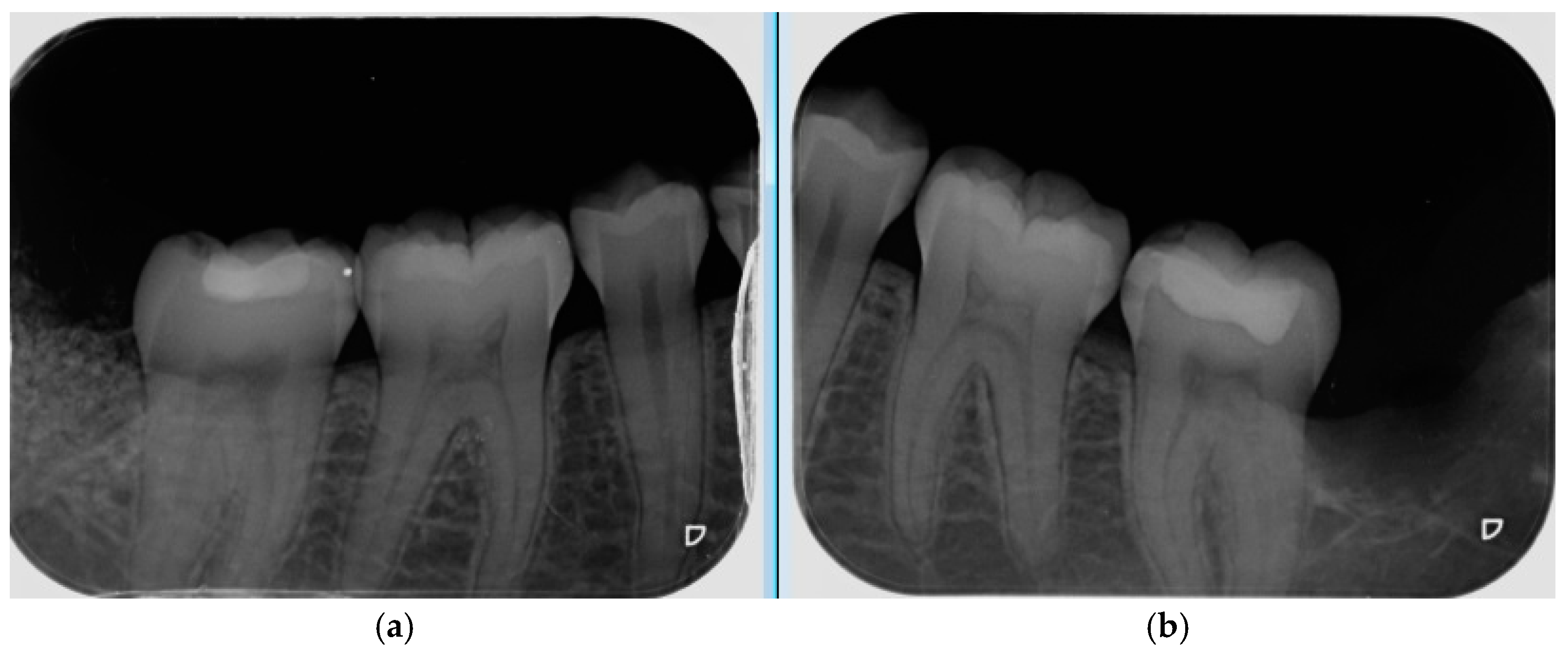
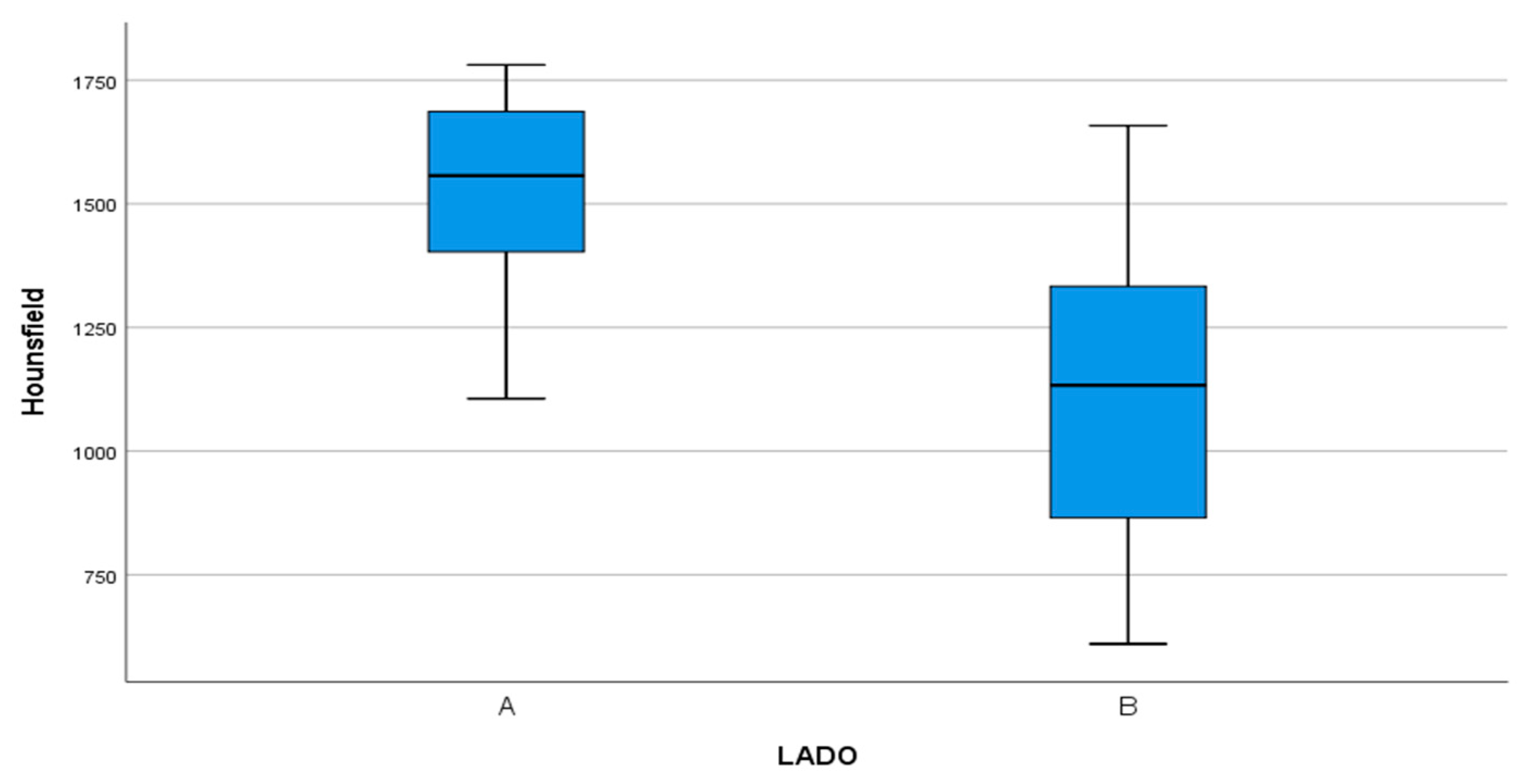
- Bone density, the degree of corticalization, and crestal bone height maintenance were measured 6 months after surgery on CBCT sagittal slices in all patients (Figure 6), using the same equipment (Newtom VGI evo, QR srl-Verone, Italy).
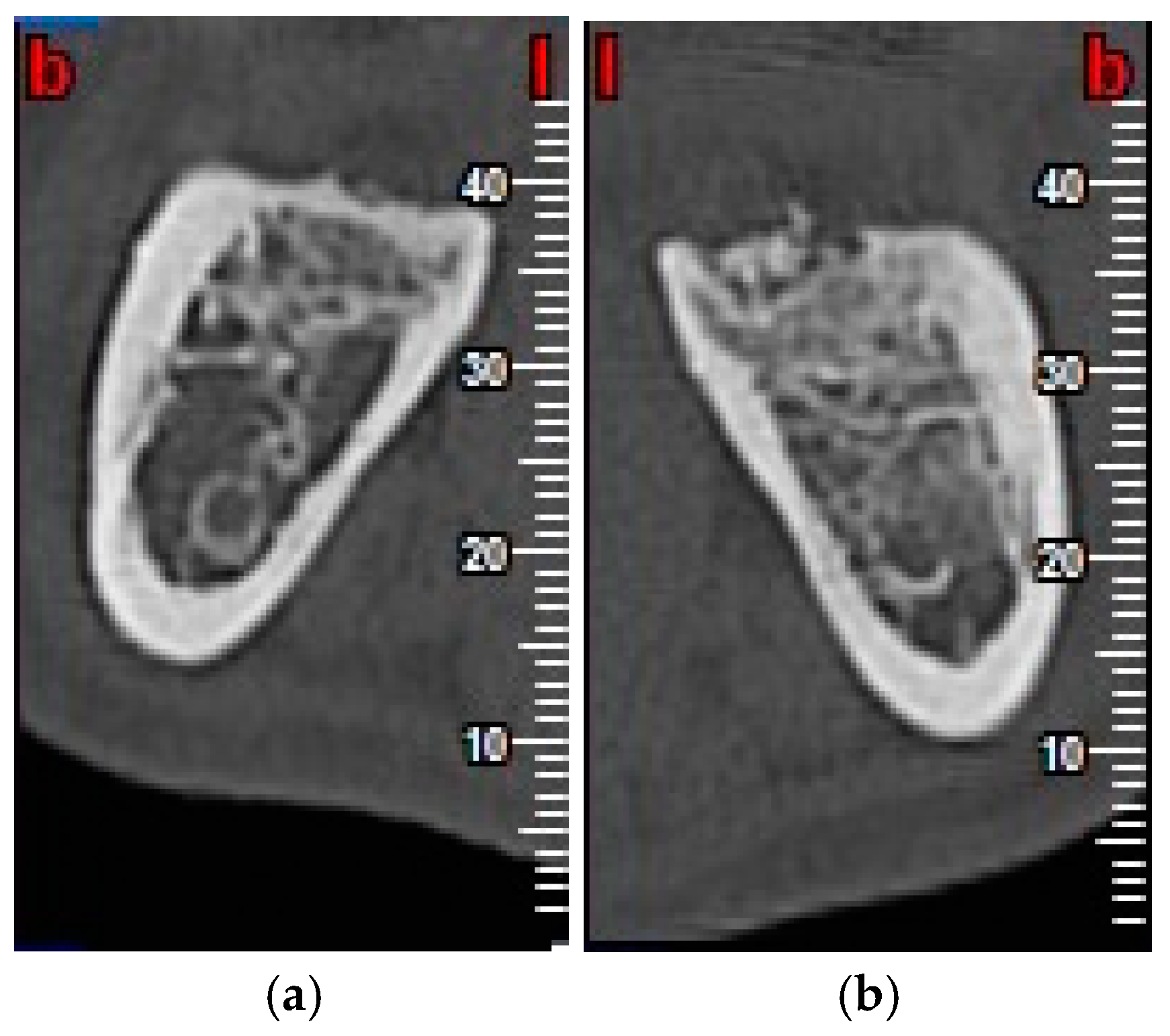
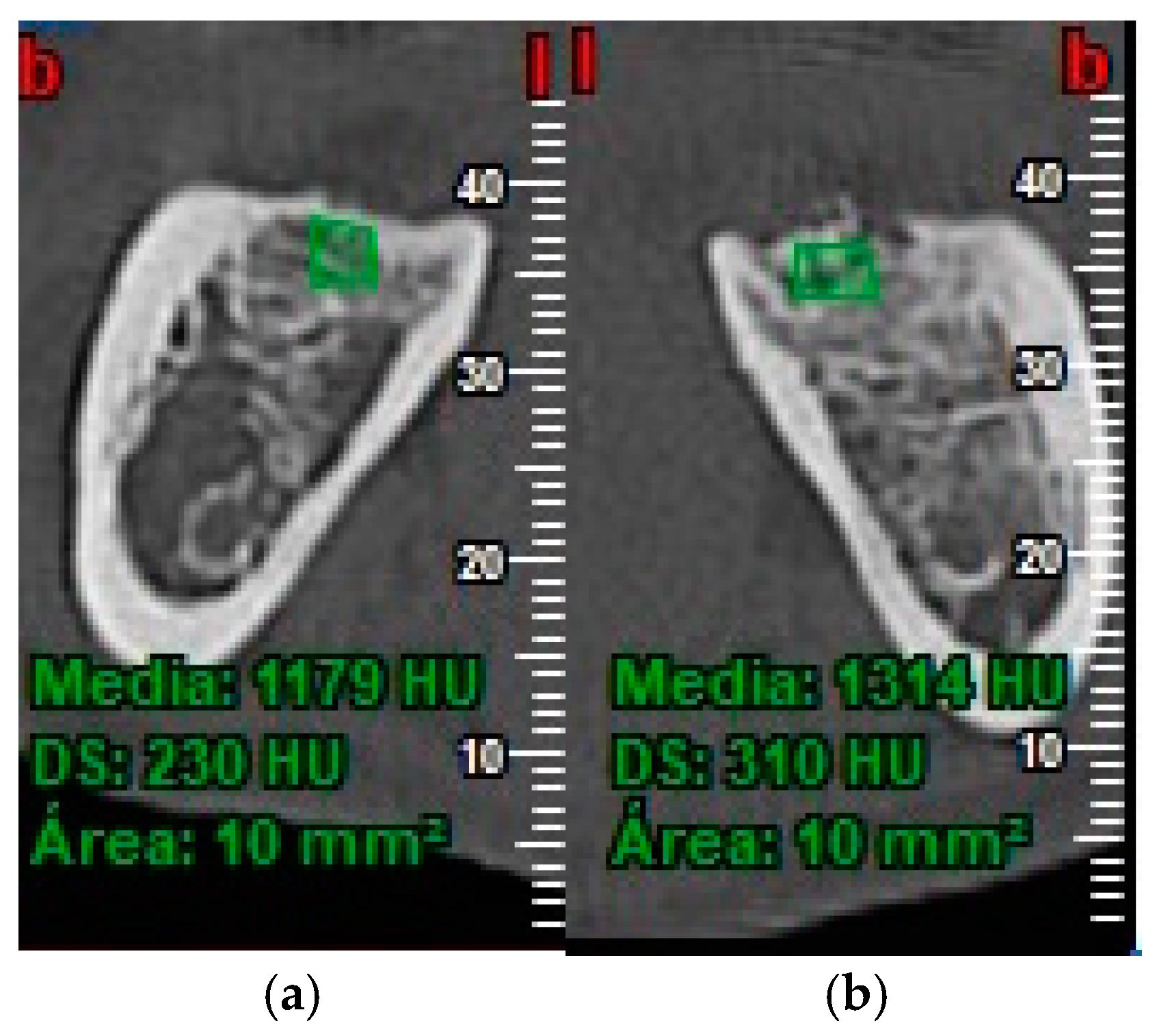
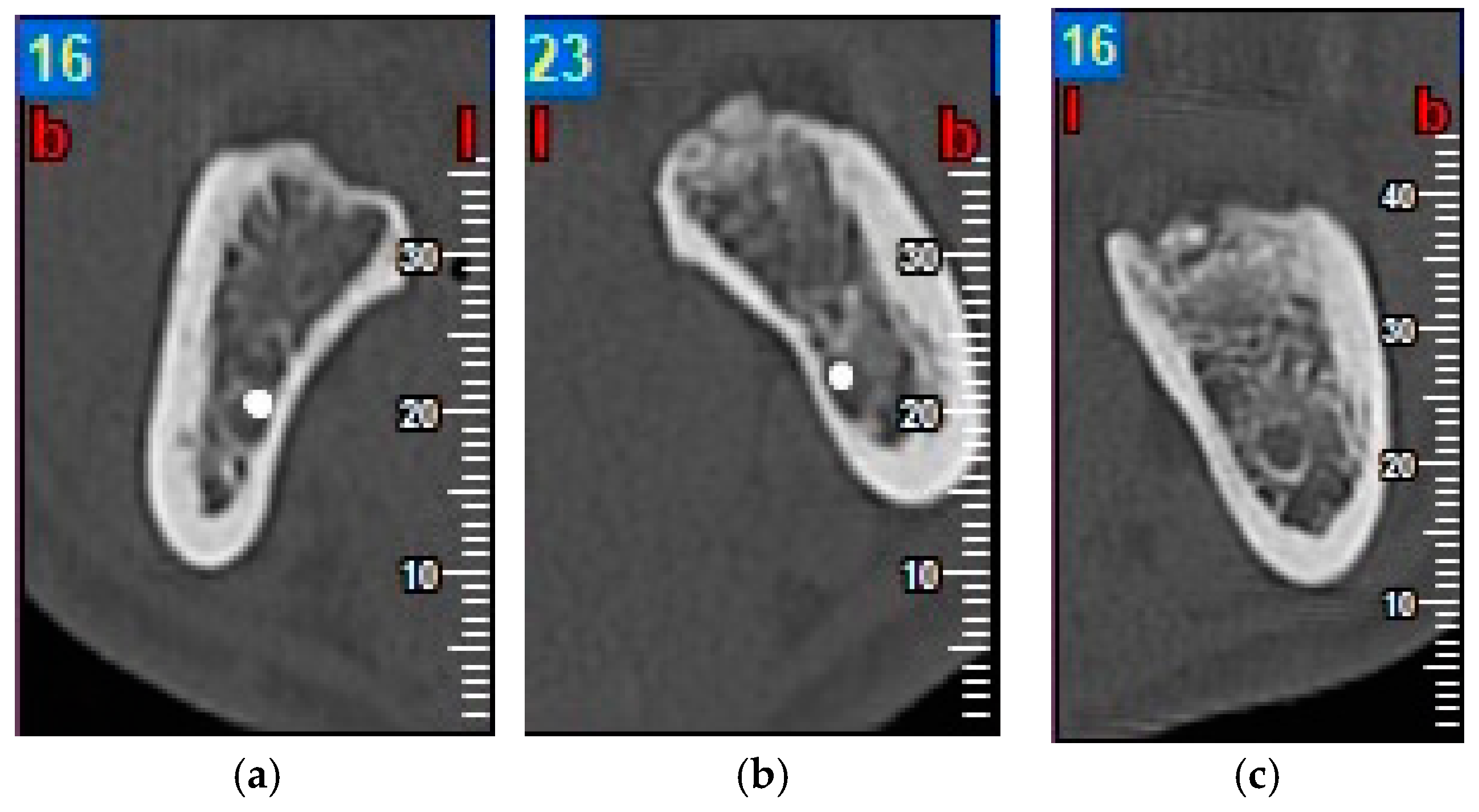
- Bone density was measured in Hounsfield units (HU) (Figure 7).
- The degree of corticalization was classified as complete (cortical ≥ 1 mm), incomplete, or absent (Figure 8).
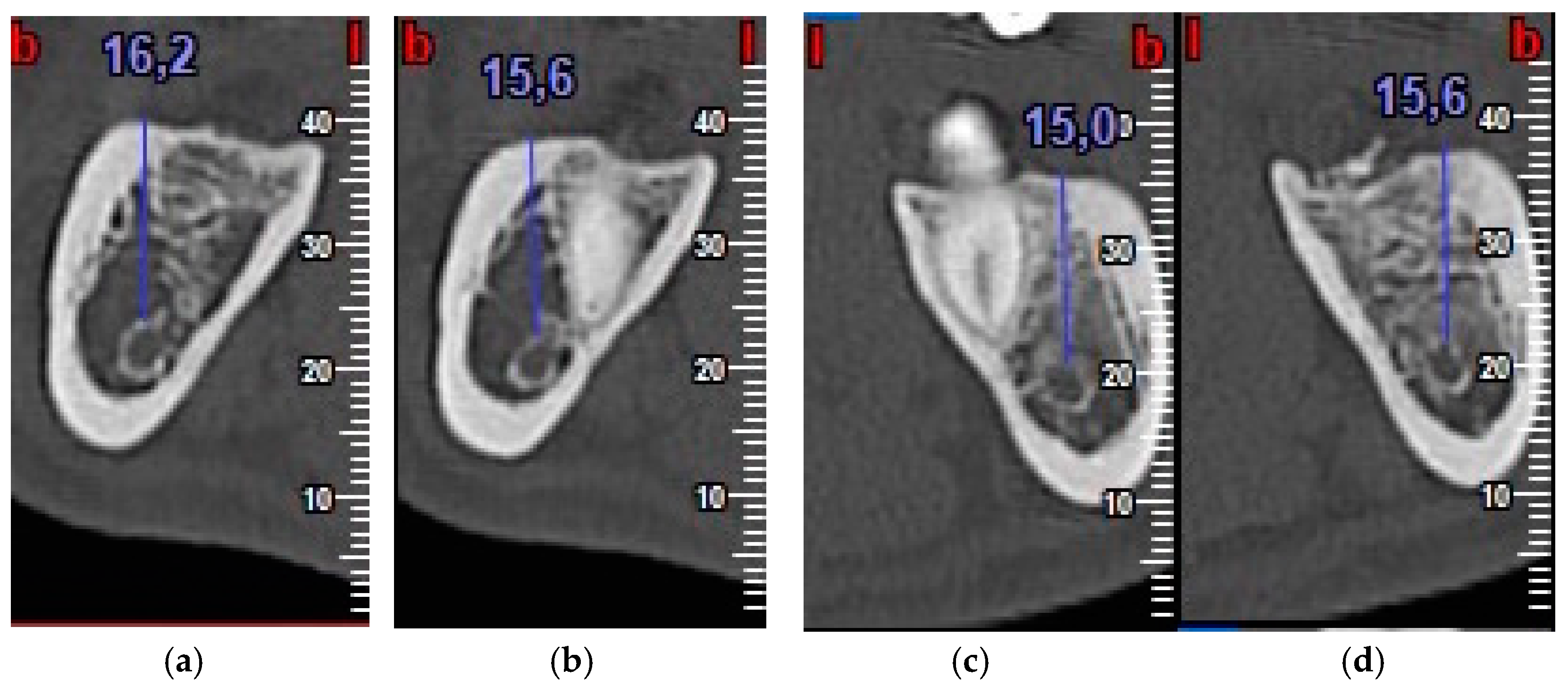
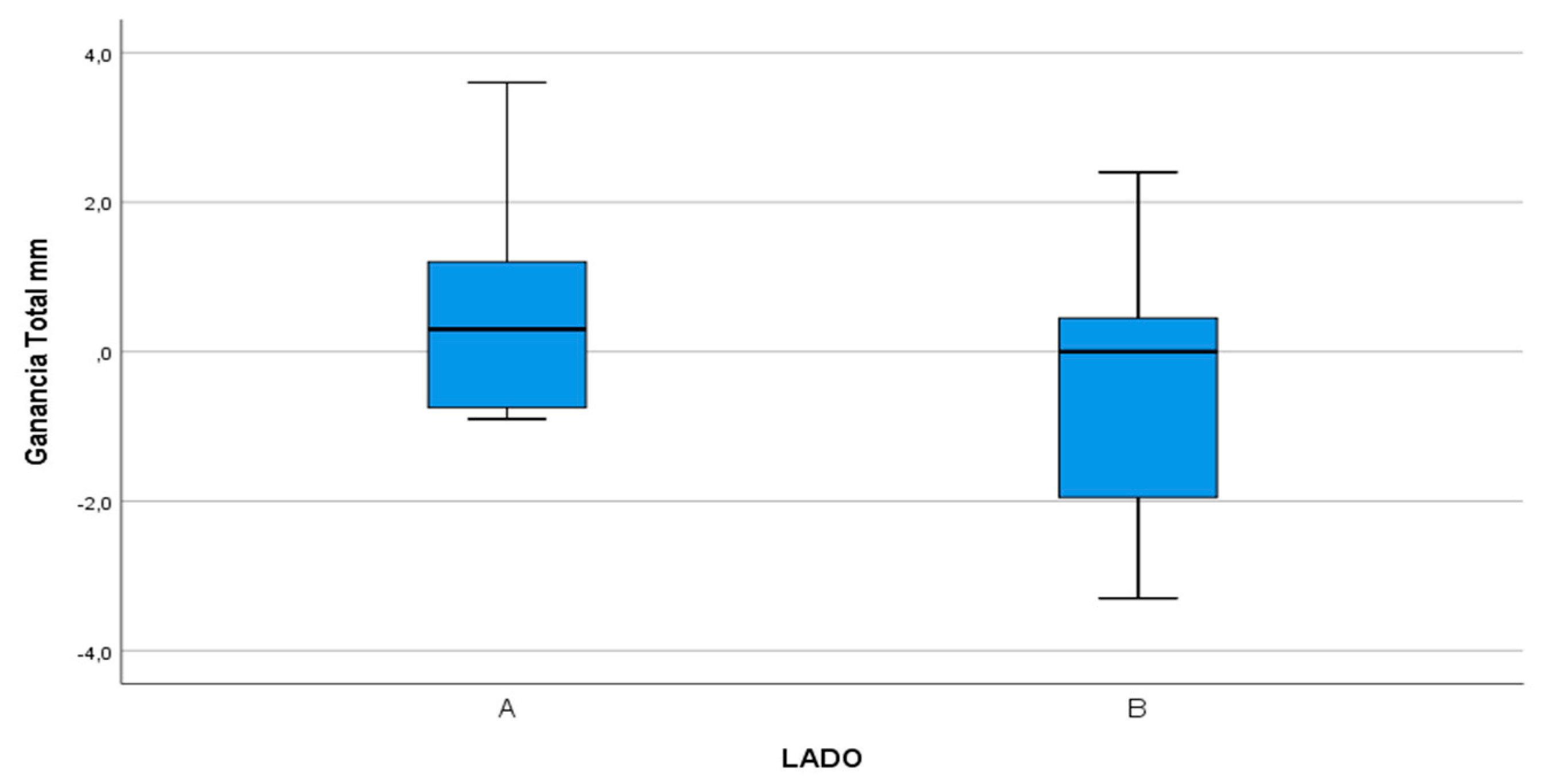
- Distance from the IAN to the bone crest was measured at the distal aspect of the lower second molar, at the center of the third molar alveolus (Figure 9).
2.6. Statistical Analysis
3. Results
3.1. Probing Depth (PD)
3.2. Bone Density
3.3. Degree of Corticalization
3.4. IAN-Crestal Bone Distance
3.5. Pain, Inflammation and Mouth Opening Capacity
3.6. Intra- and Post-Operative Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Coleman, M.; McCormick, A.; Laskin, D.M. The incidence of periodontal defects distal to the maxillary second molar after impacted third molar extraction. J. Oral Maxillofac. Surg. 2011, 69, 319–321. [Google Scholar] [CrossRef] [PubMed]
- Ge, J.; Hu, Y.; Yang, C.; Zhengc, J. Autogenous bone grafting for treatment of osseous defect after impacted mandibular third molar extraction: A randomized controlled trial. Clin. Implant Dent. Relat. Res. 2017, 19, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Leung, W.K.; Theilade, E.; Comfort, M.B.; Lim, P.L. Microbiology of the pericoronal pouch in mandibular third molar pericoronitis. Oral Microbiol. Immunol. 1993, 8, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Kan, K.W.; Liu, J.K.S.; Lo, E.C.M.; Corbet, E.F.; Leung, W.K. Residual periodontal defects distal to the mandibular second molar 6–36 months after impacted third molar extraction. A retrospective cross-sectional study of young adults. J. Clin. Periodontol. 2002, 29, 1004–1011. [Google Scholar] [CrossRef]
- Richardson, D.T.; Dodson, T.B. Risk of periodontal defects after third molar surgery: An exercise in evidence-based clinical decision-making. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2005, 100, 133–137. [Google Scholar] [CrossRef]
- Sammartino, G.; Tia, M.; Bucci, T.; Wang, H.-L. Prevention of mandibular third molar extraction-associated periodontal defects: A comparative study. J. Periodontol. 2009, 80, 389–396. [Google Scholar] [CrossRef]
- Barbato, L.; Kalemaj, Z.; Buti, J.; Baccini, M.; La Marca, M.; Duvina, M.; Tonelli, P. Effect of surgical intervention for removal of mandibular third molar on periodontal healing of adjacent mandibular second molar: A systematic review and bayesian network meta-analysis. J. Periodontol. 2016, 87, 291–302. [Google Scholar] [CrossRef]
- Haugen, H.J.; Lyngstadaas, S.; Rossi, F.; Perale, G. Bone grafts: Which is the ideal biomaterial? J. Clin. Periodontol. 2019, 46, 92–102. [Google Scholar] [CrossRef]
- Moussa, N.T.; Dym, H. Maxillofacial bone grafting materials. Dent. Clin. N. Am. 2020, 64, 473–490. [Google Scholar] [CrossRef]
- Hassan, K.S.; Marei, H.F.; Alagl, A. Does grafting of third molar extraction sockets enhance periodontal measures in 30- to 35-year-old patients? J. Oral Maxillofac. Surg. 2012, 70, 757–764. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Kim, S.-G.; Byeon, J.-H.; Lee, H.-J.; Um, I.-U.; Lim, C.P.; Kim, S.-Y. Development of a novel bone grafting material using autogenous teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, 496–503. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, G.; Miziara, M.; Da Silva, E.; Ferreira, E.; Biulchi, A.; Alves, J. Enhanced bone formation during healing process of tooth sockets filled with demineralized human dentine matrix. Aust. Dent. J. 2013, 58, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Kabir, A.; Murata, M.; Akazawa, T.; Kusano, K.; Yamada, K.; Ito, M. Evaluation of perforated demineralized dentin scaffold on bone regeneration in critical-size sheep iliac defects. Clin. Oral Implant. Res. 2017, 28, e227–e235. [Google Scholar] [CrossRef] [PubMed]
- Gual-Vaqués, P.; Polis-Yanes, C.; Estrugo-Devesa, A.; Ayuso-Montero, R.; Marí-Roig, A.; López-López, J. Autogenous teeth used for bone grafting: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2017, 23, e112–e119. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-Y.; Kim, Y.-K.; Yi, Y.-J.; Choi, J.-H. Clinical evaluation of ridge augmentation using autogenous tooth bone graft material: Case series study. J. Korean Assoc. Oral Maxillofac. Surg. 2013, 39, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Pang, K.; Um, I.-W.; Kim, Y.-K.; Woo, J.-M.; Lee, J. Autogenous demineralized dentin matrix from extracted tooth for the augmentation of alveolar bone defect: A prospective randomized clinical trial in comparison with anorganic bovine bone. Clin. Oral Implant. Res. 2016, 28, 809–815. [Google Scholar] [CrossRef]
- Valdec, S.; Pasic, P.; Soltermann, A.; Thoma, D.S.; Stadlinger, B.; Rücker, M. Alveolar ridge preservation with autologous particulated dentin—A case series. Int. J. Implant Dent. 2017, 3, 12. [Google Scholar] [CrossRef]
- Del Canto-Díaz, A.; De Elío-Oliveros, J.; Del Canto-Díaz, M.; Alobera-Gracia, M.-A.; Del Canto-Pingarrón, M.; Martínez-González, J.-M. Use of autologous tooth-derived graft material in the post-extraction dental socket. Pilot study. Med. Oral Patol. Oral Cir. Bucal 2018, 24, e53–e60. [Google Scholar] [CrossRef]
- Jeong, K.-I.; Kim, S.-G.; Kim, Y.-K.; Oh, J.-S.; Jeong, M.; Park, J.-J. Clinical study of graft materials using autogenous teeth in maxillary sinus augmentation. Implant Dent. 2011, 20, 471–475. [Google Scholar] [CrossRef]
- Kabir, A.; Murata, M.; Kusano, K.; Akazawa, T.; Shibata, T. Autogenous demineralized dentin graft for third molar socket regeneration—A case report. Dentistey 2015, 5, 11–14. [Google Scholar] [CrossRef]
- Ramanauskaite, A.; Sahin, D.; Sader, R.; Becker, J.; Schwarz, F. Efficacy of autogenous teeth for the reconstruction of alveolar ridge deficiencies: A systematic review. Clin. Oral Investig. 2019, 23, 4263–4287. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.M.; Laskin, D.M. Prophylactic use of indomethacin for prevention of postsurgical complications after removal of impacted third molars. Oral Surg. Oral Med. Oral Pathol. 1983, 55, 448–451. [Google Scholar] [CrossRef]
- Janjua, O.S.; Baig, Z.; Manzoor, A.; Abbas, T. Accuracy of pederson and modified parant scale for predicting difficulty level of mandibular third molars. Arch. Orofac. Sci. 2013, 8, 9–13. [Google Scholar]
- Kugelberg, C.F.; Ahlström, U.; Ericson, S.; Hugoson, A. Periodontal healing after impacted lower third molar surgery. Int. J. Oral Surg. 1985, 14, 29–40. [Google Scholar] [CrossRef]
- Pons-Vicente, O.; Valmaseda-Castellón, E.; Berini-Aytés, L.; Gay-Escoda, C. Effect on pocket depth and attachment level of manual versus ultrasonic scaling of lower second molars following lower third molar extraction: A randomized controlled trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, e11–e19. [Google Scholar] [CrossRef]
- Dodson, T.B. Is There a Role for Reconstructive Techniques to Prevent Periodontal Defects After Third Molar Surgery? J. Oral Maxillofac. Surg. 2005, 63, 891–896. [Google Scholar] [CrossRef]
- Petsos, H.; Korte, J.; Eickholz, P.; Hoffmann, T.; Borchard, R. Surgical removal of third molars and periodontal tissues of adjacent second molars. J. Clin. Periodontol. 2016, 43, 453–460. [Google Scholar] [CrossRef]
- Ramírez, V.; Marró, P.; López, R. Effect of mechanical debridement on distal periodontal aspects of second molars after the extraction of third molars: A systematic review. J. Periodontol. 2012, 83, 595–601. [Google Scholar] [CrossRef]
- Lee, C.-T.; Hum, L.; Chen, Y.-W. The effect of regenerative periodontal therapy in preventing periodontal defects after the extraction of third molars. J. Am. Dent. Assoc. 2016, 147, 709–719. [Google Scholar] [CrossRef]
- Camps-Font, O.; Caro-Bonfill, C.; Sánchez-Garcés, M.À.; Gay-Escoda, C. Periodontal regenerative therapy for preventing bone defects distal to mandibular second molars after surgical removal of impacted third molars: A systematic review and meta-analysis of randomized clinical trials. J. Oral Maxillofac. Surg. 2018, 76, 2482–2514. [Google Scholar] [CrossRef]
- Reis-Filho, C.R.; Silva, E.R.; Martins, A.B.; Pessoa, F.F.; Gomes, P.V.; De Araújo, M.S.; Miziara, M.N.; Alves, J.B. Demineralised human dentine matrix stimulates the expression of VEGF and accelerates the bone repair in tooth sockets of rats. Arch. Oral Boil. 2012, 57, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Faria, A.I.; Gallas-Torreira, M.; Lopez-Raton, M. Mandibular second molar periodontal healing after impacted third molar extraction in young adults. J. Oral Maxillofac. Surg. 2012, 70, 2732–2741. [Google Scholar] [CrossRef] [PubMed]
- Minetti, E.; Giacometti, E.; Gambardella, U.; Contessi, M.; Ballini, A.; Marenzi, G.; Celko, M.; Mastrangelo, F. Alveolar socket preservation with different autologous graft materials: Preliminary results of a multicenter pilot study in human. Materials 2020, 13, 1153. [Google Scholar] [CrossRef] [PubMed]
- Pohl, S.; Binderman, I.; Tomac, J. Maintenance of alveolar ridge dimensions utilizing an extracted tooth dentin particulate autograft and platelet-rich fibrin: A retrospective radiographic cone-beam computed tomography study. Materials 2020, 13, 1083. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Hazar, D.; Becker, K.; Sader, R.; Becker, J. Efficacy of autogenous tooth roots for lateral alveolar ridge augmentation and staged implant placement. A prospective controlled clinical study. J. Clin. Periodontol. 2018, 45, 996–1004. [Google Scholar] [CrossRef]
- Cobo-Vázquez, C.; Fernández-Tresguerres, I.; Ortega-Aranegui, R.; López-Quiles, J. Effects of localmelatonin application on post-extraction sockets after third molar surgery. A pilot study. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e628–e633. [Google Scholar] [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Test Group (Dentin) | Control Group (Coagulate) |
|---|---|---|
| Position | Mesioangular: 6/15 (40%) | Mesioangular: 8/15 (53.4%) |
| Horizontal: 3/15 (20%) | Horizontal: 3/15 (20%) | |
| Vertical: 6/15 (40%) | Vertical: 4/15 (26.6%) | |
| Situation | Partial coverage 5/15 (33.3%) | Partial coverage: 6/15 (40%) |
| Total coverage (submucosal): 7/15 (46.7%) | Total coverage (submucosal): 6/15 (40%) | |
| Total coverage (included): 3/15 (20%) | Total coverage (included): 3/15 (20%) | |
| Surgical difficulty (Parant) | Type 1: 0/15 (0%) | Type 1: 1/15 (6.7%) |
| Type 2: 9/15 (60%) | Type 2: 7/15 (46.6%) | |
| Type 3: 6/15 (40%) | Type 3: 7/15 (46.6%) | |
| Type 4: 0/15 (0%) | Type 4: 0/15 (0%) | |
| Proximity to the mandibular canal | 3/15 (20%) | 3/15 (20%) |
| Surgical time | 26.2 min | 12.38 min |
| Group | Test Group (Dentin) | Control Group (Coagulate) |
|---|---|---|
| Patient 1 | Vertical | Vertical |
| Partial coverage | Partial coverage | |
| Type 2 | Type 1 | |
| Patient 2 | Mesioangular | Mesioangular |
| Total coverage (submucosal) | Total coverage (submucosal) | |
| Type 2 | Type 2 | |
| Patient 3 | Horizontal | Horizontal |
| Partial coverage | Total coverage (submucosal) | |
| Type 3 | Type 3 | |
| Patient 4 | Mesioangular | Mesioangular |
| Total coverage (submucosal) | Partial coverage | |
| Type 2 | Type 2 | |
| Patient 5 | Mesioangular | Mesioangular |
| Total coverage (submucosal) | Partial coverage | |
| Type 3 | Type 3 | |
| Patient 6 | Horizontal | Horizontal |
| Total coverage (included) | Total coverage (included) | |
| Type 3 | Type 3 | |
| Patient 7 | Vertical | Mesioangular |
| Total coverage (included) | Total coverage (included) | |
| Type 3 | Type 3 | |
| Patient 8 | Mesioangular | Mesioangular |
| Total coverage (submucosal) | Total coverage (submucosal) | |
| Type 3 | Type 3 | |
| Patient 9 | Mesioangular | Mesioangular |
| Total coverage (submucosal) | Total coverage (submucosal) | |
| Type 2 | Type 2 | |
| Patient 10 | Horizontal | Vertical |
| Total coverage (included) | Total coverage (included) | |
| Type 3 | Type 3 | |
| Patient 11 | Vertical | Mesioangular |
| Total coverage (submucosal) | Total coverage (submucosal) | |
| Type 2 | Type 2 | |
| Patient 12 | Vertical | Mesioangular |
| Partial coverage | Total coverage (submucosal) | |
| Type 2 | Type 2 | |
| Patient 13 | Vertical | Horizontal |
| Partial coverage | Partial coverage | |
| Type 2 | Type 3 | |
| Patient 14 | Vertical | Vertical |
| Total coverage (submucosal) | Partial coverage | |
| Type 2 | Type 2 | |
| Patient 15 | Mesioangular | Vertical |
| Partial coverage | Partial coverage | |
| Type 2 | Type 2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Labrador, L.; Martín-Ares, M.; Ortega-Aranegui, R.; López-Quiles, J.; Martínez-González, J.M. Autogenous Dentin Graft in Bone Defects after Lower Third Molar Extraction: A Split-Mouth Clinical Trial. Materials 2020, 13, 3090. https://doi.org/10.3390/ma13143090
Sánchez-Labrador L, Martín-Ares M, Ortega-Aranegui R, López-Quiles J, Martínez-González JM. Autogenous Dentin Graft in Bone Defects after Lower Third Molar Extraction: A Split-Mouth Clinical Trial. Materials. 2020; 13(14):3090. https://doi.org/10.3390/ma13143090
Chicago/Turabian StyleSánchez-Labrador, Luis, María Martín-Ares, Ricardo Ortega-Aranegui, Juan López-Quiles, and José María Martínez-González. 2020. "Autogenous Dentin Graft in Bone Defects after Lower Third Molar Extraction: A Split-Mouth Clinical Trial" Materials 13, no. 14: 3090. https://doi.org/10.3390/ma13143090
APA StyleSánchez-Labrador, L., Martín-Ares, M., Ortega-Aranegui, R., López-Quiles, J., & Martínez-González, J. M. (2020). Autogenous Dentin Graft in Bone Defects after Lower Third Molar Extraction: A Split-Mouth Clinical Trial. Materials, 13(14), 3090. https://doi.org/10.3390/ma13143090