A Clue to the Existence of Bonding between Bone and Implant Surface: An In Vivo Study



Abstract
1. Introduction
2. Materials and Methods
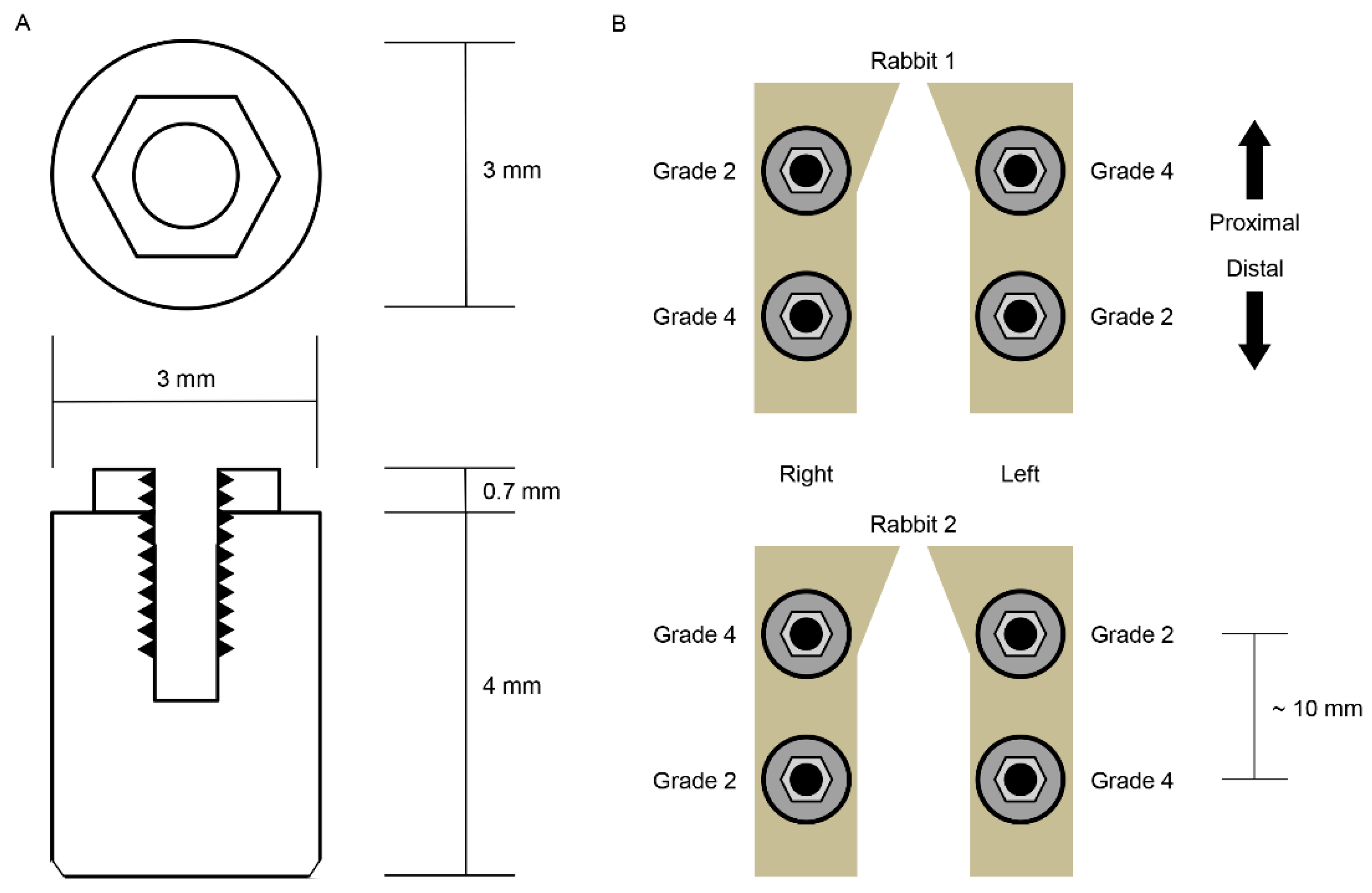
2.1. Implant Preparation
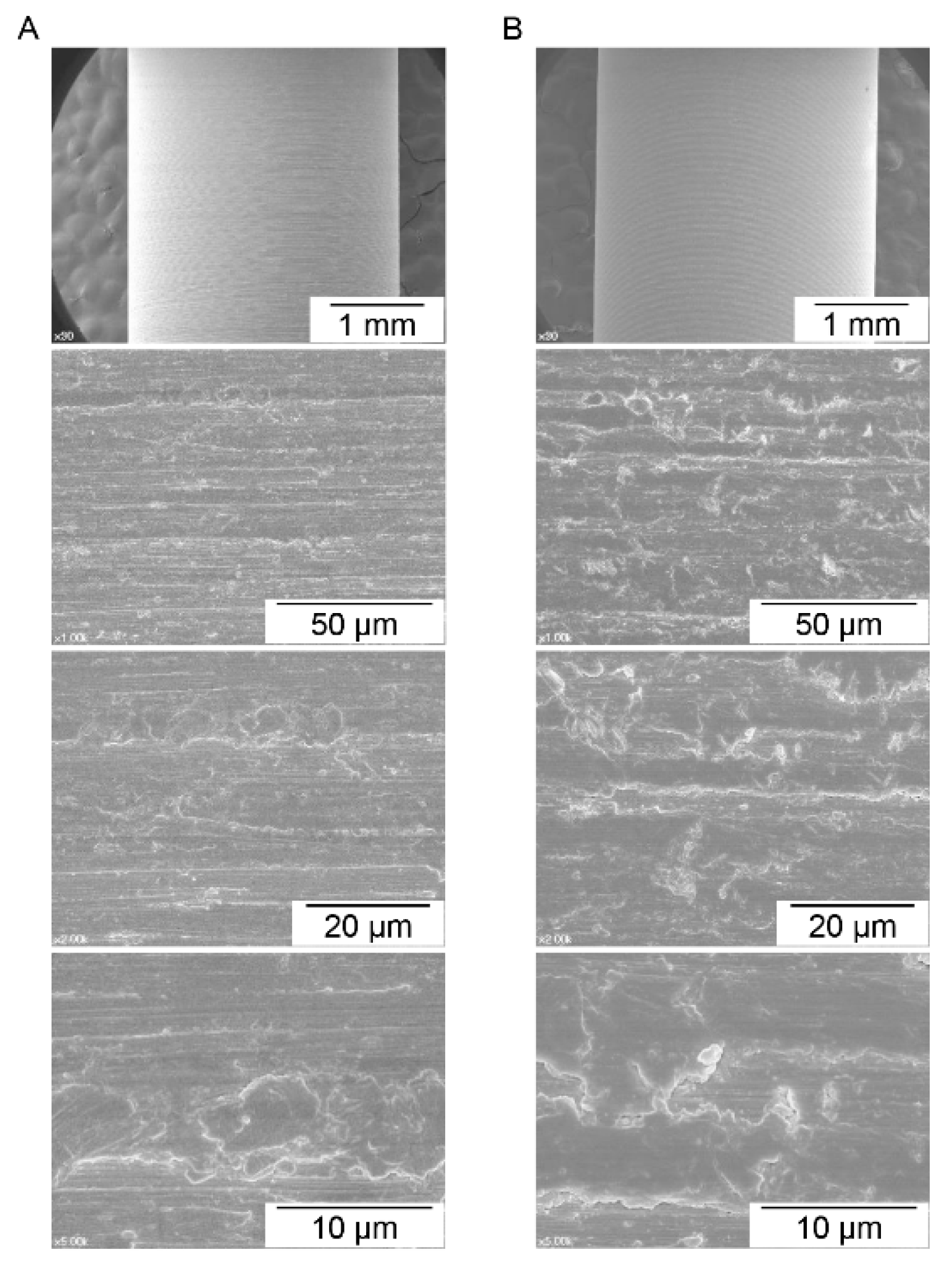
2.2. Surface Characteristics Analysis
2.3. In Vivo Implant Surgery and Euthanasia
2.4. Measurement of Three-Dimensional Bone–Implant Contact Area
2.5. Measurement of Shear Bond Strength of Bone and Implant
2.6. Statistics
3. Results
3.1. Surface Characteristics Analysis
3.2. Three-Dimensional Bone–Implant Contact Area and Shear Bond Strength
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Block, M.S. Dental Implants: The Last 100 Years. J. Oral Maxillofac. Surg. 2018, 76, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Brånemark, P.I.; Zarb, G.A.; Albrektsson, T. Tissue-Integrated Prostheses: Osseointegration in Clinical Dentistry; Quintessence Publishing: Chicago, IL, USA, 1985. [Google Scholar]
- Brunski, J. On Implant Prosthodontics: One Narrative, Twelve Voices-2. Int. J. Prosthodont. 2018, 31, s15–s22. [Google Scholar] [PubMed]
- Albrektsson, T. On Implant Prosthodontics: One Narrative, Twelve Voices-1. Int. J. Prosthodont. 2018, 31, s11–s14. [Google Scholar] [PubMed]
- Jemt, T. On Implant Prosthodontics: One Narrative, Twelve Voices-4. Int. J. Prosthodont. 2018, 31, s31–s34. [Google Scholar] [PubMed]
- Trindade, R.; Albrektsson, T.; Galli, S.; Prgomet, Z.; Tengvall, P.; Wennerberg, A. Osseointegration and foreign body reaction: Titanium implants activate the immune system and suppress bone resorption during the first 4 weeks after implantation. Clin. Implant. Dent. Relat. Res. 2018, 20, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving bioscience research reporting: The ARRIVE guidelines for reporting animal research. Osteoarthr. Cartil. 2012, 20, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Park, J.I.; Chae, J.S.; Yeo, I.L. Comparison of micro-computed tomography and histomorphometry in the measurement of bone–implant contact ratios. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Kwon, T.K.; Lee, H.J.; Min, S.K.; Yeo, I.S. Evaluation of early bone response to fluoride-modified and anodically oxidized titanium implants through continuous removal torque analysis. Implant. Dent. 2012, 21, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Yeo, I.S.; Kwon, T.K. Removal Torque Analysis of Chemically Modified Hydrophilic and Anodically Oxidized Titanium Implants with Constant Angular Velocity for Early Bone Response in Rabbit Tibia. Tissue Eng. Regen. Med. 2013, 10, 252–259. [Google Scholar] [CrossRef]
- Gracco, A.; Giagnorio, C.; Incerti Parenti, S.; Alessandri Bonetti, G.; Siciliani, G. Effects of thread shape on the pullout strength of miniscrews. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Nonhoff, J.; Moest, T.; Schmitt, C.M.; Weisel, T.; Bauer, S.; Schlegel, K.A. Establishment of a new pull-out strength testing method to quantify early osseointegration-An experimental pilot study. J. Cranio-Maxillofac. Surg. 2015, 43, 1966–1973. [Google Scholar] [CrossRef] [PubMed]
- Velasco, E.; Monsalve-Guil, L.; Jimenez, A.; Ortiz, I.; Moreno-Munoz, J.; Nunez-Marquez, E.; Pegueroles, M.; Perez, R.A.; Gil, F.J. Importance of the Roughness and Residual Stresses of Dental Implants on Fatigue and Osseointegration Behavior. In Vivo Study in Rabbits. J. Oral Implantol. 2016, 42, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Nakada, H.; Takahashi, T.; Fujita, K.; Tanimoto, Y.; Sakae, T.; Kimoto, S.; Kawai, Y. Potential for acceleration of bone formation after implant surgery by using a dietary supplement: An animal study. J. Oral Rehabil. 2015, 42, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Yashwant, A.V.; Dilip, S.; Krishnaraj, R.; Ravi, K. Does Change in Thread Shape Influence the Pull Out Strength of Mini Implants? An In vitro Study. J. Clin. Diagn. Res. 2017, 11, ZC17–ZC20. [Google Scholar] [CrossRef] [PubMed]
- Yeo, I.S. Reality of dental implant surface modification: A short literature review. Open Biomed. Eng. J. 2014, 8, 114–119. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Element | Cp-Ti Grade 2 | Cp-Ti Grade 4 | p-Value |
|---|---|---|---|
| Carbon (C) | 3.66% ± 0.21% | 4.03% ± 0.39% | 2.3 × 10−1 |
| Oxygen (O) | 1.15% ± 0.10% | 3.21% ± 0.29% | 3.0 × 10−4 * |
| Iron (Fe) | 0.26% ± 0.02% | 0.39% ± 0.05% | 2.0 × 10−2 * |
| Titanium (Ti) | 94.93% ± 0.32% | 92.38% ± 0.13% | 2.1 × 10−4 * |
| Grade 2 cp-Ti | Grade 4 cp-Ti | p-Value | |
|---|---|---|---|
| 3D BIC area (mm2) | 12.7 ± 1.2 | 11.5 ± 1.6 | 0.35 |
| 3D BIC ratio (%) | 33.6 ± 3.2 | 30.5 ± 4.3 | 0.35 |
| Implant removal torque (Ncm) | 2.9 ± 0.4 | 1.9 ± 0.3 | 0.052 |
| Torque per unit (Ncm/cm2) | 23.2 ± 3.5 | 16.5 ± 1.0 | 0.032 * |
| Shear bond strength (MPa) | 1.5 ± 0.2 | 1.1 ± 0.1 | 0.032 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, T.-K.; Choi, J.-Y.; Park, J.-I.; Yeo, I.-S.L. A Clue to the Existence of Bonding between Bone and Implant Surface: An In Vivo Study. Materials 2019, 12, 1187. https://doi.org/10.3390/ma12071187
Kwon T-K, Choi J-Y, Park J-I, Yeo I-SL. A Clue to the Existence of Bonding between Bone and Implant Surface: An In Vivo Study. Materials. 2019; 12(7):1187. https://doi.org/10.3390/ma12071187
Chicago/Turabian StyleKwon, Taek-Ka, Jung-Yoo Choi, Jae-Il Park, and In-Sung Luke Yeo. 2019. "A Clue to the Existence of Bonding between Bone and Implant Surface: An In Vivo Study" Materials 12, no. 7: 1187. https://doi.org/10.3390/ma12071187
APA StyleKwon, T.-K., Choi, J.-Y., Park, J.-I., & Yeo, I.-S. L. (2019). A Clue to the Existence of Bonding between Bone and Implant Surface: An In Vivo Study. Materials, 12(7), 1187. https://doi.org/10.3390/ma12071187