
Hemoadsorption in Complex Cardiac Surgery—A Single Center Experience


 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ball, L.; Costantino, F.; Pelosi, P. Postoperative complications of patients undergoing cardiac surgery. Curr. Opin. Crit. Care 2016, 22, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Chakravarthy, M. Modifying risks to improve outcome in cardiac surgery: An anesthesiologist’s perspective. Ann. Card Anaesth. 2017, 20, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Yadava, O.P.; Narayan, P.; Padmanabhan, C.; Sajja, L.R.; Sarkar, K.; Varma, P.K.; Jawali, V. IACTS position statement on “2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization”: Section 7.1—A consensus document. Indian J. Thorac. Cardiovasc. Surg. 2022, 38, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Aittokallio, J.; Uusalo, P.; Kallioinen, M.; Jarvisalo, M.J. Markers of Poor Prognosis in Patients Requiring Continuous Renal Replacement Therapy After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2020, 34, 3329–3335. [Google Scholar] [CrossRef] [PubMed]
- Busse, L.W.; Barker, N.; Petersen, C. Vasoplegic syndrome following cardiothoracic surgery-review of pathophysiology and update of treatment options. Crit. Care 2020, 24, 36. [Google Scholar] [CrossRef]
- Laffey, J.G.; Boylan, J.F.; Cheng, D.C. The systemic inflammatory response to cardiac surgery: Implications for the anesthesiologist. Anesthesiology 2002, 97, 215–252. [Google Scholar] [CrossRef]
- CytoSorbents. CytoSorbents. CytoSorb 300mL Device. In Instructions for Use; CytoSorbents Inc.: Monmouth Junction, NJ, USA, 2021; Available online: www.cytosorb.com (accessed on 8 August 2022).
- Poli, E.C.; Rimmele, T.; Schneider, A.G. Hemoadsorption with CytoSorb ((R)). Intensive Care Med. 2019, 45, 236–239. [Google Scholar] [CrossRef]
- Barton, H.; Zechendorf, E.; Ostareck, D.; Ostareck-Lederer, A.; Stoppe, C.; Zayat, R.; Philipp, T.-S.; Marx, G.; Bickenbach, J. Prognostic Value of GDF-15 in Predicting Prolonged Intensive Care Stay following Cardiac Surgery: A Pilot Study. Dis. Markers 2021, 2021, 5564334. [Google Scholar] [CrossRef]
- Crawford, T.C.; Magruder, J.T.; Grimm, J.C.; Suarez-Pierre, A.; Sciortino, C.M.; Mandal, K.; Zehr, K.J.; Conte, J.V.; Higgings, R.S.; Cameron, D.E.; et al. Complications After Cardiac Operations: All Are Not Created Equal. Ann. Thorac. Surg. 2017, 103, 32–40. [Google Scholar] [CrossRef]
- Bianco, V.; Kilic, A.; Gleason, T.G.; Aranda-Michel, E.; Habertheuer, A.; Wang, Y.; Navid, F.; Kacin, A.; Sultan, I. Reoperative Cardiac Surgery Is a Risk Factor for Long-Term Mortality. Ann. Thorac. Surg. 2020, 110, 1235–1242. [Google Scholar] [CrossRef]
- Zhang, S.; Huang, S.; Tiemuerniyazi, X.; Song, Y.; Feng, W. A Meta-Analysis of Early, Mid-term and Long-Term Mortality of On-Pump vs. Off-Pump in Redo Coronary Artery Bypass Surgery. Front. Cardiovasc. Med. 2022, 9, 869987. [Google Scholar] [CrossRef] [PubMed]
- Nierhaus, A.; Morales, J.; Wendt, D.; Scheier, J.; Gutzler, D.; Jarczak, D.; Born, F.; Hagl, C.; Deliargyris, E.; Mehta, Y. Comparison of the CytoSorb ((R)) 300 mL and Jafron HA380 hemoadsorption devices: An in vitro study. Minim. Invasive Ther. Allied Technol. 2022, 31, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Ranucci, M.; Baryshnikova, E.; Crapelli, G.B.; Rahe-Meyer, N.; Menicanti, L.; Frigiola, A.; Surgical Clinical Outcome REsearch (SCORE) Group. Randomized, double-blinded, placebo-controlled trial of fibrinogen concentrate supplementation after complex cardiac surgery. J. Am. Heart Assoc. 2015, 4, e002066. [Google Scholar] [CrossRef] [PubMed]
- Park, C.B.; Suri, R.M.; Burkhart, H.M.; Greason, K.L.; Dearani, J.A.; Schaff, H.V.; Sundt, T.M., III. Identifying patients at particular risk of injury during repeat sternotomy: Analysis of 2555 cardiac reoperations. J. Thorac. Cardiovasc. Surg. 2010, 140, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, R.; Dharmadjati, B.B.; Mulia, E.P.B.; Rachmi, D.A. Vasoplegia: Mechanism and Management Following Cardiopulmonary Bypass. Eurasian J. Med. 2022, 54, 92–99. [Google Scholar] [CrossRef]
- Gruda, M.C.; Ruggeberg, K.G.; O’Sullivan, P.; Guliashvili, T.; Scheirer, A.R.; Golobish, T.D.; Capponi, V.J.; Chan, P.P. Broad adsorption of sepsis-related PAMP and DAMP molecules, mycotoxins, and cytokines from whole blood using CytoSorb (R) sorbent porous polymer beads. PLoS ONE 2018, 13, e0191676. [Google Scholar] [CrossRef]
- Haidari, Z.; Wendt, D.; Thielmann, M.; Mackowiak, M.; Neuhauser, M.; Jakob, H.; Ruhparwar, A.; El-Gabry, M. Intraoperative Hemoadsorption in Patients with Native Mitral Valve Infective Endocarditis. Ann. Thorac. Surg. 2020, 110, 890–896. [Google Scholar] [CrossRef]
- Mehta, Y.; Singh, A.; Singh, A.; Gupta, A.; Bhan, A. Modulating the Inflammatory Response with Hemadsorption (CytoSorb) in Patients Undergoing Major Aortic Surgery. J. Cardiothorac. Vasc. Anesth. 2021, 35, 673–675. [Google Scholar] [CrossRef]
- Saller, T.; Hagl, C.; Woitsch, S.; Li, Y.; Niedermayer, S.; Born, F.; Luehr, M.; Kammerer, T.; Pichlmaier, M.; Scheiermann, P.; et al. Haemadsorption improves intraoperative haemodynamics and metabolic changes during aortic surgery with hypothermic circulatory arrest. Eur. J. Cardiothorac. Surg. 2019, 56, 731–737. [Google Scholar] [CrossRef]
- Nemeth, E.; Kovacs, E.; Racz, K.; Soltesz, A.; Szigeti, S.; Kiss, N.; Csikos, G.; Koritsanszky, K.B.; Berzsenyi, V.; Trembickij, G.; et al. Impact of intraoperative cytokine adsorption on outcome of patients undergoing orthotopic heart transplantation-an observational study. Clin. Transpl. 2018, 32, e13211. [Google Scholar] [CrossRef]
- Boss, K.; Jahn, M.; Wendt, D.; Haidari, Z.; Demircioglu, E.; Thielmann, M.; Ruhparwar, A.; Kribben, A.; Bartosz, T. Extracorporeal cytokine adsorption: Significant reduction of catecholamine requirement in patients with AKI and septic shock after cardiac surgery. PLoS ONE 2021, 16, e0246299. [Google Scholar] [CrossRef] [PubMed]
- Traeger, K.; Skrabal, C.; Fischer, G.; Datzmann, T.; Schroeder, J.; Fritzler, D.; Hartmann, J.; Liebold, A.; Reinelt, H. Hemoadsorption treatment of patients with acute infective endocarditis during surgery with cardiopulmonary bypass–a case series. Int. J. Artif. Organs 2017, 40, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Traeger, K.; Skrabal, C.; Fischer, G.; Schroeder, J.; Marenski, L.; Liebold, A.; Reinelt, H.; Datzmann, T. Hemoadsorption treatment with CytoSorb ((R)) in patients with extracorporeal life support therapy: A case series. Int. J. Artif. Organs 2020, 43, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Hou, K.; Chen, Q.; Zhu, X.; Shen, X.; Zou, L.; Mu, X.; Sun, X. Correlation Between Vasoactive-Inotropic Score and Postoperative Acute Kidney Injury after Cardiovascular Surgery. Heart Surg. Forum 2021, 24, E282–E292. [Google Scholar] [CrossRef] [PubMed]
- Baysal, P.K.; Guzelmeric, F.; Kahraman, E.; Gurcu, M.E.; Erkilinc, A.; Orki, T. Is Vasoactive-Inotropic Score a Predictor for Mortality and Morbidity in Patients Undergoing Coronary Artery Bypass Surgery? Braz. J. Cardiovasc. Surg. 2021, 36, 802–806. [Google Scholar] [CrossRef]
- Belletti, A.; Lerose, C.C.; Zangrillo, A.; Landoni, G. Vasoactive-Inotropic Score: Evolution, Clinical Utility, and Pitfalls. J. Cardiothorac. Vasc. Anesth. 2021, 35, 3067–3077. [Google Scholar] [CrossRef]
- Kalisnik, J.M.; Leiler, S.; Mamdooh, H.; Zibert, J.; Bertsch, T.; Vogt, F.A.; Bagaev, E.; Fittkau, M.; Fischlein, T. Single-Centre Retrospective Evaluation of Intraoperative Hemoadsorption in Left-Sided Acute Infective Endocarditis. J. Clin. Med. 2022, 11, 3954. [Google Scholar] [CrossRef]
- Haidari, Z.; Demircioglu, E.; Boss, K.; Tyczynski, B.; Thielmann, M.; Schmack, B.; Kribben, A.; Weymann, A.; El Gabry, M.; Ruhparwar, A.; et al. Intraoperative hemoadsorption in high-risk patients with infective endocarditis. PLoS ONE 2022, 17, e0266820. [Google Scholar] [CrossRef]
- Calabro, M.G.; Febres, D.; Recca, G.; Lembo, R.; Fominskiy, E.; Scandroglio, A.M.; Zangrillo, A.; Pappalardo, F. Blood Purification with CytoSorb in Critically Ill Patients: Single-Center Preliminary Experience. Artif. Organs 2019, 43, 189–194. [Google Scholar] [CrossRef]
- Tripathi, R.; Morales, J.; Lee, V.; Gibson, C.M.; Mack, M.J.; Schneider, D.J.; Douketis, J.; Sellke, F.W.; Ohman, M.E.; Thourani, V.H.; et al. Antithrombotic Drug Removal from Whole Blood Using Haemoadsorption with a Porous Polymer Bead Sorbent. Eur. Heart J. Cardiovasc. Pharmacother. 2022, pvac036. [Google Scholar] [CrossRef]
- Matejic-Spasic, M.; Hassan, K.; Thielmann, M.; Geidel, S.; Storey, R.F.; Schmoeckel, M.; Adamson, H.; Deliargyris, E.N.; Wendt, D. Management of perioperative bleeding risk in patients on antithrombotic medications undergoing cardiac surgery—A systematic review. J. Thorac. Dis. 2022, 14, 3030–3044. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean (CI) or Median [IQR] | ||||
|---|---|---|---|---|
| Variables | Overall (n = 52) | CS Group (n = 23) | Control Group (n = 29) | p-Value |
| Age, years | 61 [51.5, 65.5] | 64 [60.0, 68.0] | 57 [47.0, 61.0] | 0.01 |
| Sex–male, % (n) | 63.5 (33) | 60.9 (14) | 65.5 (19) | 0.73 |
| Redo procedures, % (n) | 34.6 (18) | 21.7 (5) | 44.8 (13) | 0.08 |
| Lactate mmol/L | 1.36 [1.0, 2.1] | 1.25 [0.8, 2.1] | 1.40 [1.1, 2.1] | 0.38 |
| EuroSCORE II, % | 4.6 [2.2, 14.2] | 7.3 [2.7, 21.4] | 4.4 [1.5, 9.2] | 0.17 |
| Mechanical ventilation, % (n) | 15.4 (8) | 21.7 (5) | 10.3 (3) | 0.26 |
| Intra-aortic balloon pump (IABP), % (n) | 9.6 (5) | 21.7 (5) | 0 | <0.01 |
| Continuous renal replacement therapy (CRRT), % (n) | 1.9 (1) | 4.3 (1) | 0 | 0.26 |
| Inotropes, % (n) | 25.0 (13) | 34.8 (8) | 17.2 (5) | 0.15 |
| Hemoglobin (Hb), g/dL | 12.0 [10.2, 13.5] | 11.5 [9.5, 12.8] | 12.6 [11.2, 13.8] | 0.08 |
| White blood cell count (WBC), N × 109/L | 9.2 (6.3, 11.9) | 8.2 (5.9, 11.4) | 10.6 (6.4, 12.0) | 0.64 |
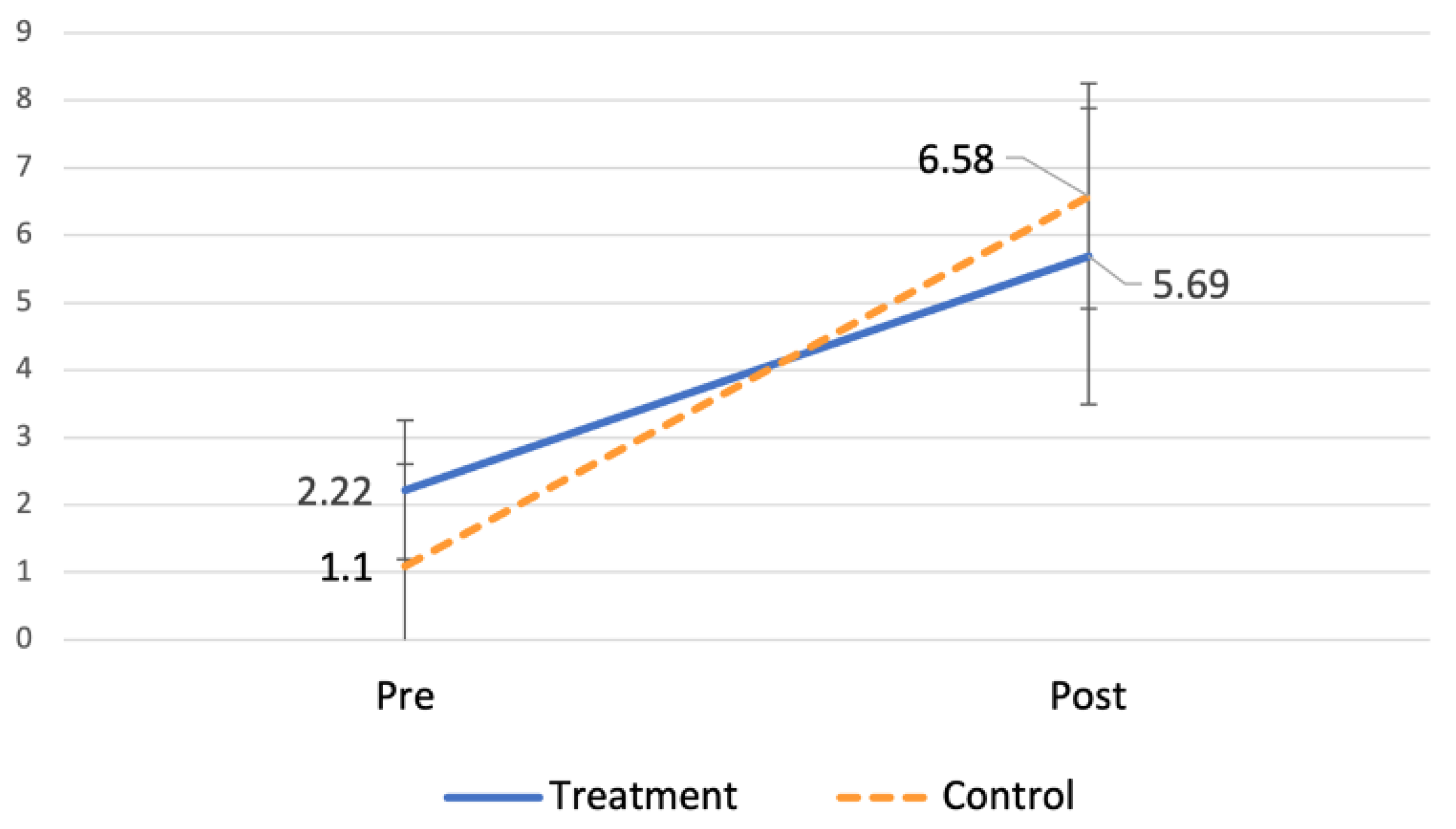
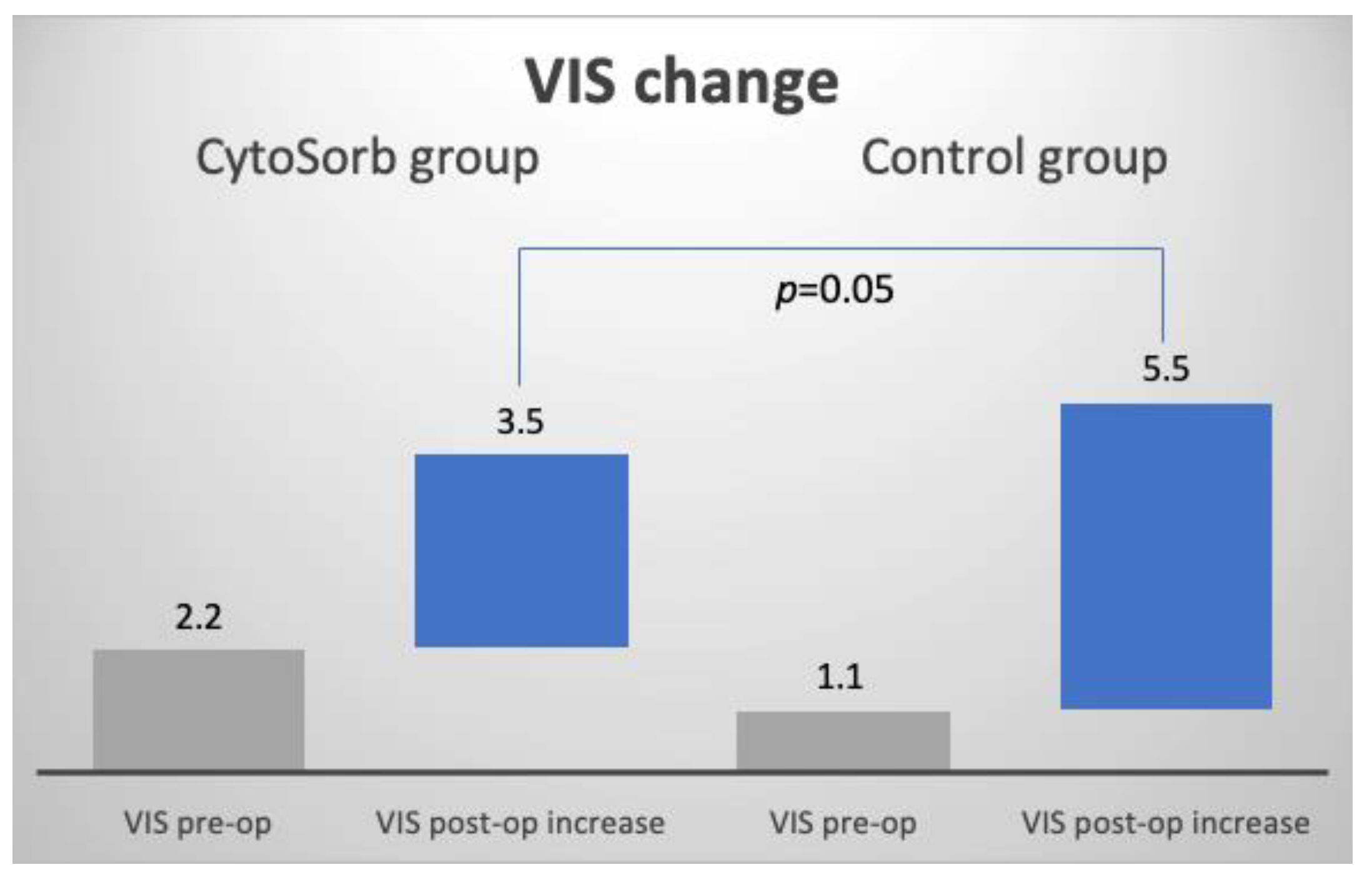
| Vasoactive-inotropic score (VIS) | 1.6 (0.7, 2.5) | 2.2 (0.7, 3.7) | 1.1 (0.1, 2.1) | 0.20 |
| CPB time, min | 211 [167.5, 275.5] | 217 [171.0, 264.0] | 211 [164.0, 278.0] | 0.99 |
| Cross-clamp time, min | 143 [115.0, 181.0] | 122 [100.0, 156.0] | 154 [131.5, 195.5] | 0.04 |
| CPB temperature, °C | 31 [28, 32] | 30 [28, 32] | 32 [28, 32] | 0.30 |
| Mean (CI Difference) | ||||
|---|---|---|---|---|
| Variable | CS Group | Control Group | Delta | p-Value |
| VIS mean change 1 | 3.5 (2.2, 4.8) | 5.5 (3.6, 7.4) | 2 (−0.4, 4.4) | 0.05 |
| Median [IQR], Mean (CI), or Proportion % (n) | ||||
|---|---|---|---|---|
| Variable | Overall | CS Group | Control Group | p-Value |
| Mortality, % (n) | 15.7 (8) * | 9.1 (2) * | 20.7 (6) | 0.26 |
| VIS post-op | 6.2 (4.8, 7.5) | 5.7 (4.2, 7.2) | 6.6 (4.5, 8.7) | 0.53 |
LoS, days
| ||||
| 3 [2, 5] | 4 [3, 6] | 3 [2, 4] | 0.28 | |
| 2.5 [1, 4] | 3 [2, 4] | 2 [1, 3] | 0.14 | |
| 6 [5, 8] | 6 [5, 8] | 6 [5, 8] | 0.74 | |
| CRRT post-op, % (n) | 9.6 (5) | 8.7 (2) | 10.3 (3) | 0.84 |
| Mechanical ventilation post-op, % (n) | 96.2 (50) | 95.7 (22) | 96.6 (28) | 0.87 |
| Duration of mechanical ventilation, days | 1 [1, 2] | 1 [1, 2] | 1 [1, 2] | 0.83 |
Lactates post-op
| ||||
| 2.3 [1.6, 3.1] | 1.8 [1.3, 3.1] | 2.7 [−3.1, 1.1] | 0.13 | |
| 3.5 [2.0, 6.0] | 3.8 [2.5, 7.8] | 3.2 [1.9, 5.8] | 0.24 | |
| 2.3 [1.4, 4.6] | 2.9 [1.9, 4.6] | 1.8 [1.4, 3.0] | 0.15 | |
| 1.8 [1.3, 3.7] | 1.9 [1.4, 3.2] | 1.6 [1.1, 3.8] | 0.52 | |
Total blood loss, mL
| ||||
| 759 [591, 1181] | 903 [647, 1200] | 715 [445, 1089] | 0.08 | |
| 570 [400, 920] | 700 [460, 990] | 510 [400, 640] | 0.12 | |
| 1512 [1046, 2019] | 1475 [998, 1941] | 1677 [1115, 2337] | 0.23 | |
Blood product usage, units
| ||||
| 4 [3, 5] | 4 [3, 6] | 4 [2, 5] | 0.26 | |
| 0 [0, 4] | 0 [0, 3] | 1 [0, 4] | 0.38 | |
| 0 [0, 0] | 0 [0, 0] | 0 [0, 4] | 0.48 | |
| 0 [0, 0] | 0 [0, 0] | 0 [0, 0] | 0.28 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manohar, M.; Jawali, V.; Neginahal, S.; GT, S.; Muniraj, G.; Chakravarthy, M. Hemoadsorption in Complex Cardiac Surgery—A Single Center Experience. J. Clin. Med. 2022, 11, 7005. https://doi.org/10.3390/jcm11237005
Manohar M, Jawali V, Neginahal S, GT S, Muniraj G, Chakravarthy M. Hemoadsorption in Complex Cardiac Surgery—A Single Center Experience. Journal of Clinical Medicine. 2022; 11(23):7005. https://doi.org/10.3390/jcm11237005
Chicago/Turabian StyleManohar, Murali, Vivek Jawali, Siddu Neginahal, Sudarshan GT, Geetha Muniraj, and Murali Chakravarthy. 2022. "Hemoadsorption in Complex Cardiac Surgery—A Single Center Experience" Journal of Clinical Medicine 11, no. 23: 7005. https://doi.org/10.3390/jcm11237005
APA StyleManohar, M., Jawali, V., Neginahal, S., GT, S., Muniraj, G., & Chakravarthy, M. (2022). Hemoadsorption in Complex Cardiac Surgery—A Single Center Experience. Journal of Clinical Medicine, 11(23), 7005. https://doi.org/10.3390/jcm11237005