
Clinical Evaluation of Dexamethasone Plus Gentamycin Mouthwash Use in Combination with Total Glucosides of Paeony for Treatment of Oral Lichen Planus without Fungal Infection: A Comparative Study with Long-Term Follow-Up

Abstract
1. Introduction
2. Materials and Methods
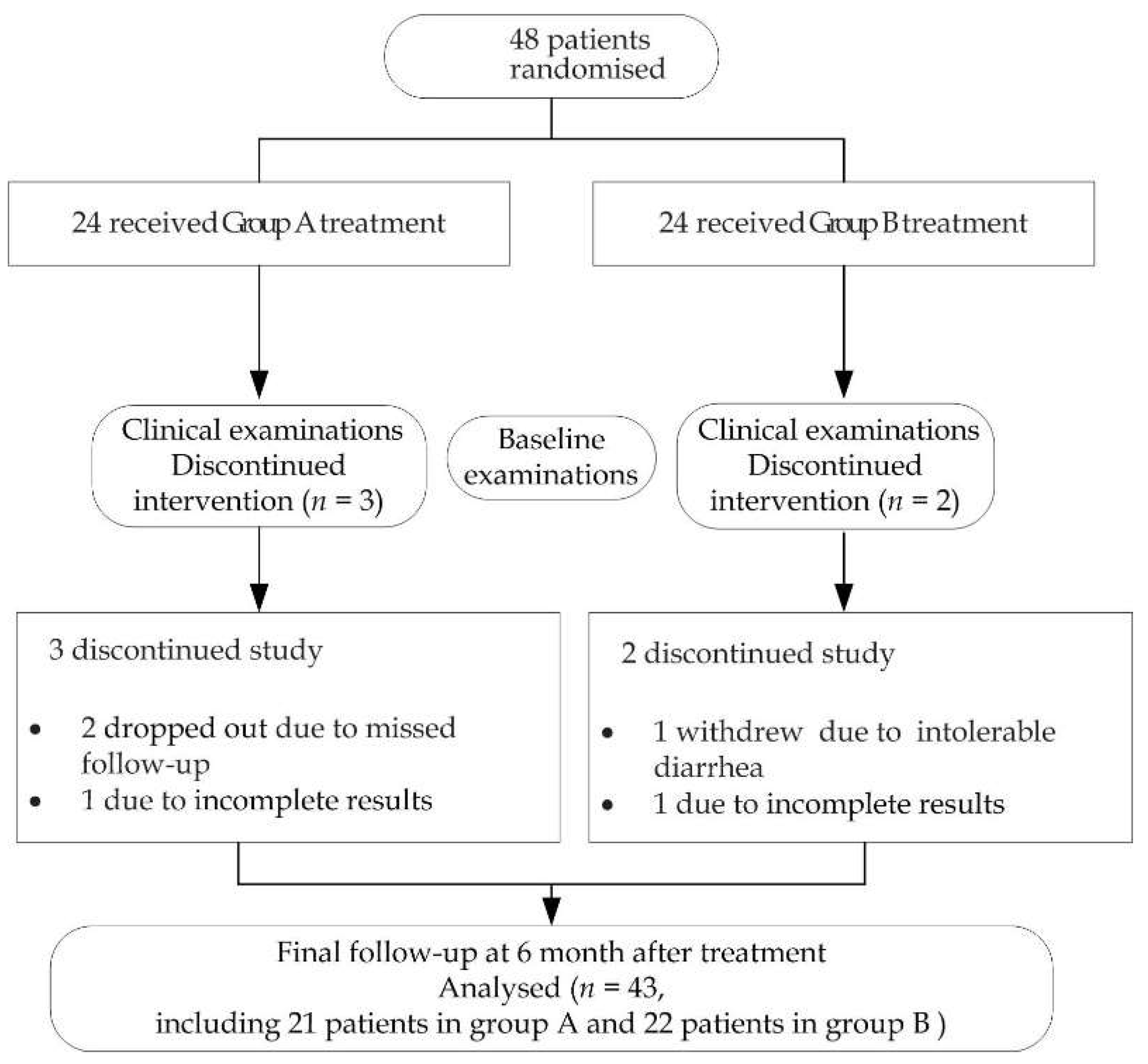
2.1. Patients
2.2. Treatment Protocol
2.3. Clinical Recording
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheng, Y.S.; Gould, A.; Kurago, Z.; Fantasia, J.; Muller, S. Diagnosis of oral lichen planus: A position paper of the American Academy of Oral and Maxillofacial Pathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 332–354. [Google Scholar] [CrossRef] [PubMed]
- Kurago, Z.B. Etiology and pathogenesis of oral lichen planus: An overview. Oral Surg. Oral Med. Oral Pathol. 2016, 122, 72–80. [Google Scholar] [CrossRef]
- Warnakulasuriya, S. Oral potentially malignant disorders: A comprehensive review on clinical aspects and management. Oral Oncol. 2020, 102, 104550. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, S.G.; Hirsch, S.A.; Gordon, S.C. The malignant transformation of oral lichen planus and oral lichenoid lesions: A systematic review. J. Am. Dent. Assoc. 2014, 145, 45–56. [Google Scholar] [CrossRef]
- Ioannides, D.; Vakirlis, E.; Kemeny, L.; Marinovic, B.; Massone, C.; Murphy, R.; Nast, A.; Ronnevig, J.; Ruzicka, T.; Cooper, S.M.; et al. European S1 guidelines on the management of lichen planus: A cooperation of the European Dermatology Forum with the European Academy of Dermatology and Venereology. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1403–1414. [Google Scholar] [CrossRef]
- Giustina, T.A.; Stewart, J.C.; Ellis, C.N.; Regezi, J.A.; Annesley, T.; Woo, T.Y.; Voorhees, J.J. Topical application of isotretinoin gel improves oral lichen planus. A double-blind study. Arch. Dermatol. 1986, 122, 534–536. [Google Scholar] [CrossRef] [PubMed]
- Łukaszewska-Kuska, M.; Ślebioda, Z.; Dorocka-Bobkowska, B. The effectiveness of topical forms of dexamethasone in the treatment of oral lichen planus—A systematic review. Oral Dis. 2022, 28, 2063–2071. [Google Scholar] [CrossRef] [PubMed]
- Carbone, M.; Goss, E.; Carrozzo, M.; Castellano, S.; Conrotto, D.; Broccoletti, R.; Gandolfo, S. Systemic and topical corticosteroid treatment of oral lichen planus: A comparative study with long-term follow-up. J. Oral. Pathol. Med. 2003, 32, 323–329. [Google Scholar] [CrossRef]
- Chen, L.Y.; Harnod, T.; Chang, Y.H.; Chen, H.; Ding, D.C. The Combination of Clindamycin and Gentamicin Is Adequate for Pelvic Inflammatory Disease: A Retrospective Cohort Study. J. Clin. Med. 2021, 10, 4145. [Google Scholar] [CrossRef]
- Lv, H.; Wang, L.; Liu, S.; Hu, W.; Wang, J.; Deng, X.; Gao, J. Synergistic Effect of Lithocholic Acid with Gentamicin against Gram-Positive Bacteria but Not against Gram-Negative Bacteria. Molecules 2022, 27, 2318. [Google Scholar] [CrossRef]
- Ou, H.Q.; Lu, X.S. Comparison between tacrolimus ointment and compound gentamicin gargle on treating oral lichen planus of erosive type. Clin. J. Chin. Med. 2018, 10, 114–115. [Google Scholar] [CrossRef]
- Li, J.; Chen, C.X.; Shen, Y.H. Effects of total glucosides from paeony (Paeonia lactiflora Pall) roots on experimental atherosclerosis in rats. J. Ethnopharmacol. 2011, 135, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Verma, K.K.; Mittal, R.; Manchanda, Y. Azathioprine for the treatment of severe erosive oral and generalized lichen planus. Acta Derm.-Venereol. 2001, 81, 378–379. [Google Scholar] [CrossRef] [PubMed]
- Torti, D.C.; Jorizzo, J.L.; McCarty, M.A. Oral lichen planus: A case series with emphasis on therapy. Arch. Dermatol. 2007, 143, 511–515. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Yu, J.; Wang, C.; Wei, W. The effects of total glucosides of paeony (TGP) and paeoniflorin (Pae) on inflammatory-immune responses in rheumatoid arthritis (RA). Funct. Plant Biol. 2019, 46, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.Y.; Ni, J.H.; Wang, X.; Feng, G.Z.; Li, H.D.; Bao, W.L.; Wang, Y.R.; You, K.Y.; Weng, H.B.; Shen, X.Y. Total glucosides of Paeony restores intestinal barrier function through inhibiting Lyn/Snail signaling pathway in colitis mice. Phytomed. Int. J. Phytother. Phytopharm. 2021, 87, 153590. [Google Scholar] [CrossRef]
- Zheng, L.W.; Hua, H.; Cheung, L.K. Traditional Chinese medicine and oral diseases: Today and tomorrow. Oral Dis. 2011, 17, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.L.; Cao, T.Y.; Wang, Y.F.; Yao, H.; Du, G.H.; Tian, Z.; Tang, G.Y. Clinical observation on the treatment of oral lichen planus with total glucosides of paeony capsule combined with corticosteroids. Int. Immunopharmacol. 2016, 36, 106–110. [Google Scholar] [CrossRef]
- Villa, A.; Sankar, V.; Bassani, G.; Johnson, L.B.; Sroussi, H. Dexamethasone solution and dexamethasone in Mucolox for the treatment of oral lichen planus: A preliminary study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Thongprasom, K.; Luangjarmekorn, L.; Sererat, T.; Taweesap, W. Relative efficacy of fluocinolone acetonide compared with triamcinolone acetonide in treatment of oral lichen planus. J. Oral Pathol. Med. 1992, 21, 456–458. [Google Scholar] [CrossRef]
- Seyed, J.K.; Maryam, B.; Tahereh, M.; Mahdieh-Sadat, M. Comparison of oral Nano-Curcumin with oral prednisolone on oral lichen planus: A randomized double-blinded clinical trial. BMC Complement. Med. 2020, 20, 328. [Google Scholar] [CrossRef]
- Lavaee, F.; Shadmanpour, M. Comparison of the effect of photodynamic therapy and topical corticosteroid on oral lichen planus lesions. Oral Dis. 2019, 25, 1954–1963. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Zhou, G.; Zeng, H.; Xiong, C.R.; Lin, M.; Zhou, H.M. A randomized double-blind, positive-control trial of topical thalidomide in erosive oral lichen planus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Hambly, J.L.; Haywood, A.; Hattingh, L.; Nair, R.G. Comparison between self-formulation and compounded-formulation dexamethasone mouth rinse for oral lichen planus: A pilot, randomized, cross-over trial. J. Investig. Clin. Dent. 2017, 8, e12225. [Google Scholar] [CrossRef] [PubMed]
- Gorsky, M.; Raviv, M.; Moskona, D.; Laufer, M.; Bodner, L. Clinical characteristics and treatment of patients with oral lichen planus in Israel. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 82, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wei, W. Anti-inflammatory and immunoregulatory effects of paeoniflorin and total glucosides of paeony. Pharmacol. Ther. 2020, 207, 107452. [Google Scholar] [CrossRef]
- Roopashree, M.R.; Gondhalekar, R.V.; Shashikanth, M.C.; George, J.; Thippeswamy, S.H.; Shukla, A. Pathogenesis of oral lichen planus—A review. J. Oral Pathol. Med. 2010, 39, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Yoke, P.C.; Tin, G.B.; Kim, M.J.; Rajaseharan, A.; Ahmed, S.; Thongprasom, K.; Chaimusik, M.; Suresh, S.; Machin, D.; Bee, W.H.; et al. A randomized controlled trial to compare steroid with cyclosporine for the topical treatment of oral lichen planus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Xiong, C.; Qi, J.; Deng, R.; Xie, L.; Li, C.; Nie, X. Total glucosides of paeony inhibits proliferation and promotes activation- induced cell death of mouse T cells in vitro. J. South. Med. Univ. 2020, 40, 118–124. [Google Scholar] [CrossRef]
- Marable, D.R.; Bowers, L.M.; Stout, T.L.; Stewart, C.M.; Berg, K.M.; Sankar, V.; DeRossi, S.S.; Thoppay, J.R.; Brennan, M.T. Oral candidiasis following steroid therapy for oral lichen planus. Oral Dis. 2016, 22, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Arendorf, T.M.; Walker, D.M. The prevalence and intra-oral distribution of Candida albicans in man. Arch. Oral Biol. 1980, 25, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jainkittivong, A.; Kuvatanasuchati, J.; Pipattanagovit, P.; Sinheng, W. Candida in oral lichen planus patients undergoing topical steroid therapy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Hou, X.; Wang, Z.; Jiang, L.; Xiong, C.; Zhou, M.; Chen, Q. Carriage rate and virulence attributes of oral Candida albicans isolates from patients with oral lichen planus: A study in an ethnic Chinese cohort. Mycoses 2009, 52, 161–165. [Google Scholar] [CrossRef]
- Luo, J.; Song, W.J.; Xu, Y.; Chen, G.Y.; Hu, Q.; Tao, Q.W. Benefits and Safety of Tripterygium Glycosides and Total Glucosides of Paeony for Rheumatoid Arthritis: An Overview of Systematic Reviews. Chin. J. Integr. Med. 2019, 25, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Chen, A.J.; Fang, S.; Li, H. Successful treatment of necrobiotic xanthogranuloma with total glucosides of paeony. Dermatol. Ther. 2014, 27, 304–306. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Zhang, B.Q.; Zhu, Y.M.; Yu, B.B.; Fu, L.; Zhou, L.L.; Zhou, X.P.; Lu, Y. The Effectiveness and Safety of Total Glucosides of Paeony in Primary Sjögren’s Syndrome: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2019, 10, 550. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Group A | Group B | p Values (A vs. B) | |
|---|---|---|---|---|
| n | 43 | 21 | 22 | |
| Gender | 0.586 | |||
| Male | 14 (32.6%) | 6 (28.6%) | 8 (36.4%) | |
| Female | 29 (67.4%) | 15 (71.4%) | 14 (63.6%) | |
| Age range (Years) | 49.79 ± 17.52 | 50.29 ± 18.8 | 49.32 ± 16.63 | 0.859 |
| Height | 164.98 ± 8.15 | 164.43 ± 7.71 | 165.50 ± 8.69 | 0.672 |
| Weight | 62.83 ± 13.16 | 62.24 ± 15.03 | 63.38 ± 11.41 | 0.779 |
| Type | 0.658 | |||
| Non-Erosive | 19 (44.2%) | 10 (47.6%) | 9 (40.9%) | |
| Erosive | 24 (55.0%) | 11 (52.4%) | 13 (59.1%) | |
| Sites of mucosal involvement | 0.079 | |||
| Buccal mucosa alone | 11 (25.6%) | 6 (28.6%) | 5 (22.7%) | |
| Buccal mucosa + gingiva | 10 (23.3%) | 2 (9.5%) | 8 (36.4%) | |
| Buccal mucosa + tongue | 9 (20.9%) | 8 (38.1%) | 1 (4.5%) | |
| Buccal mucosa + palate | 4 (9.3%) | 2 (9.5%) | 2 (9.1%) | |
| Buccal mucosa + lip | 4 (9.3%) | 2 (9.5%) | 2 (9.1%) | |
| Buccal mucosa + gingiva + tongue + lip | 1 (2.3%) | 0 (0.0%) | 1 (4.5%) | |
| Gingiva alone | 2 (4.7%) | 0 (0.0%) | 2 (9.1%) | |
| Gingiva + tongue | 1 (2.3%) | 0 (0.0%) | 1 (4.5%) | |
| Palate alone | 1 (2.3%) | 1 (4.8%) | 0 (0.0%) |
| Sign Score | VAS | |||||
|---|---|---|---|---|---|---|
| Group A (n = 21) | Group B (n = 22) | p Values | Group A (n = 21) | Group B (n = 22) | p Values | |
| Baseline | 3.95 ± 1.07 | 4.05 ± 1.13 | 0.795 | 6.38 ± 2.29 | 6.59 ± 2.32 | 0.745 |
| First follow-up | 3.38 ± 0.97 | 3.45 ± 1.18 | 0.838 | 5.33 ± 2.58 | 4.64 ± 1.79 | 0.281 |
| Second follow-up | 2.95 ± 1.07 | 2.27 ± 0.98 | 0.059 | 3.95 ± 1.77 | 2.59 ± 2.50 | 0.036 |
| Third follow-up | 2.81 ± 1.54 | 1.73 ± 1.08 | 0.003 | 2.48 ± 2.46 | 0.77 ± 1.19 | 0.009 |
| Fourth follow-up | 3.05 ± 1.53 | 1.68 ± 1.04 | <0.001 | 2.81 ± 2.66 | 0.59 ± 0.66 | 0.001 |
| Group | Course of Disease (Follow-Up) | ||||
|---|---|---|---|---|---|
| (A n = 21, B n = 22) | 1 | 2 | 3 | 4 | |
| Complete resolution | A | 0 (0.0%) | 0 (0.0%) | 1 (4.8%) | 1 (4.8%) |
| B | 0 (0%) | 1 (4.5%) | 4 (18.2%) | 4 (18.2%) | |
| Partial resolution | A | 7 (33.3%) | 11 (52.4%) | 13 (61.9%) | 12 (57.1%) |
| B | 10 (45.5%) | 14 (63.6%) | 14 (63.6%) | 15 (68.2%) | |
| No resolution | A | 14 (66.7%) | 10 (47.6%) | 7 (33.3%) | 8 (38.1%) |
| B | 12 (54.5%) | 7 (31.8%) | 4 (18.2%) | 3 (13.6%) | |
| Total effective rate | A | 7 (33.3%) | 11 (52.4%) | 14 (66.7%) | 13 (61.9%) |
| B | 10 (45.5%) | 15 (68.2%) | 18 (81.8%) | 19 (86.4%) | |
| p Values | 0.007 | ||||
| Sign Score | Single Site of Mucosal Involvement | More Sites of Mucosal Involvement | ||||
|---|---|---|---|---|---|---|
| Group A (n = 7) | Group B (n = 7) | p Values | Group A (n = 14) | Group B (n = 15) | p Values | |
| Baseline | 4.14 ± 1.07 | 3.14 ± 1.07 | 0.101 | 3.86 ± 1.10 | 4.47 ± 0.92 | 0.150 |
| First follow-up | 3.00 ± 0.00 | 3.00 ± 1.15 | 1.000 | 3.57 ± 1.16 | 3.67 ± 1.18 | 0.822 |
| Second follow-up | 3.43 ± 1.13 | 2.86 ± 0.38 | 0.348 | 2.71 ± 0.99 | 2.00 ± 1.07 | 0.092 |
| Third follow-up | 2.71 ± 1.89 | 2.57 ± 0.79 | 0.814 | 2.86 ± 1.41 | 1.33 ± 0.98 | <0.001 |
| Fourth follow-up | 3.00 ± 1.53 | 2.43 ± 0.79 | 0.348 | 3.07 ± 1.59 | 1.33 ± 0.98 | <0.001 |
| VAS | ||||||
| Baseline | 6.71 ± 1.50 | 6.14 ± 1.86 | 0.609 | 6.21 ± 2.64 | 6.67 ± 2.41 | 0.560 |
| First follow-up | 4.29 ± 1.60 | 4.71 ± 1.60 | 0.701 | 5.86 ± 2.85 | 4.60 ± 1.92 | 0.106 |
| Second follow-up | 3.43 ± 1.13 | 3.86 ± 2.85 | 0.701 | 4.21 ± 2.01 | 2.00 ± 2.17 | 0.005 |
| Third follow-up | 1.29 ± 1.25 | 1.29 ± 1.25 | 1.000 | 0.07 ± 2.73 | 0.53 ± 1.13 | 0.001 |
| Fourth follow-up | 2.14 ± 2.48 | 0.71 ± 0.49 | 0.202 | 3.14 ± 2.77 | 0.47 ± 0.74 | 0.001 |
| Single Site of Mucosal Involvement (Group A n = 7, Group B n = 7) | More Sites of Mucosal Involvement (Group A n = 14, Group B n = 15) | |||||||
|---|---|---|---|---|---|---|---|---|
| Follow-Up | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 |
| Group A | ||||||||
| Complete resolution | 0 (0.0%) | 0 (0.0%) | 1 (14.3%) | (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (7.1%) |
| Partial resolution | 3 (42.9%) | 5 (71.4%) | 4 (57.1%) | 5 (71.4%) | 4 (28.6%) | 6 (42.9%) | 9 (64.3%) | 7 (50.0%) |
| No resolution | 4 (57.1%) | 2 (28.6%) | 2 (28.6%) | 2 (28.6%) | 10 (71.4%) | 8 (57.1%) | 5 (35.7%) | 6 (42.9%) |
| Effective rate | 3 (42.9%) | 5 (71.4%) | 5 (71.4%) | 5 (71.4%) | 4 (28.6%) | 6 (42.9%) | 9 (64.3%) | 8 (57.1%) |
| Group B | ||||||||
| Complete resolution | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0%) | 1 (6.7%) | 4 (26.7%) | 4 (26.7%) |
| Partial resolution | 2 (28.6%) | 3 (42.9%) | 6 (85.7%) | 5 (71.4%) | 8 (53.3%) | 11 (73.3%) | 8 (53.3%) | 10 (66.7%) |
| No resolution | 5 (71.4%) | 4 (57.1%) | 1 (14.3%) | 2 (28.6%) | 7 (46.7%) | 3 (20.0%) | 3 (20.0%) | 1 (6.7%) |
| Total effective rate | 2 (28.6%) | 3 (42.9%) | 6 (85.7%) | 5 (71.4%) | 8 (53.3%) | 12 (80.0%) | 12 (80.0%) | 14 (93.3%) |
| p Values | 0.376 | 0.003 | ||||||
| Non-Erosive OLP (Group A n = 10, Group B n = 9) | Erosive OLP (Group A n = 11, Group B n = 13) | |||||||
|---|---|---|---|---|---|---|---|---|
| Follow-Up | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 |
| Group A | ||||||||
| Complete resolution | 0 (0.0%) | 0 (0.0%) | 1 (10.0%) | 1 (10.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Partial resolution | 5 (50.0%) | 7 (70.0%) | 7 (70.0%) | 7 (70.0%) | 2 (18.2%) | 4 (36.4%) | 6 (54.5%) | 5 (45.5%) |
| No resolution | 5 (50.0%) | 3 (30.0%) | 2 (20.0%) | 2 (20.0%) | 9 (81.8%) | 7 (63.6%) | 5 (45.5%) | 6 (54.5%) |
| Effective rate | 5 (50.0%) | 7 (70.0%) | 8 (80.0%) | 8 (80.0%) | 2 (18.2%) | 4 (36.4%) | 6 (54.5%) | 5 (45.5%) |
| Group B | ||||||||
| Complete resolution | 0 (0%) | 0 (0.0%) | 1 (11.1%) | 1 (11.1%) | 0 (0.0%) | 1 (7.7%) | 3 (23.1%) | 3 (23.1%) |
| Partial resolution | 4 (44.4%) | 7 (77.8%) | 7 (77.8%) | 7 (77.8%) | 6 (46.2%) | 7 (53.8%) | 7(53.8%) | 8 (61.5%) |
| No resolution | 5 (55.6%) | 2 (22.2%) | 1 (11.1%) | 1 (11.1%) | 7 (53.8%) | 5 (38.5%) | 3 (23.1%) | 2 (15.4%) |
| Effective rate | 4 (44.4%) | 7 (77.8%) | 8 (88.9%) | 8 (88.9%) | 6 (46.2%) | 8 (61.5%) | 10 (76.9%) | 11 (84.6%) |
| p Values | 0.582 | 0.037 | ||||||
| AEs | Group | Course of Disease (Follow-Up) | |||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| Oral AE | |||||
| Fungal infection (candidiasis) | A | 0 | 1 (4.2%) | 0 | 0 |
| B | 0 | 0 | 1 (4.2%) | 0 | |
| Systemic AE | |||||
| Gastrointestinal symptoms (diarrhea) | A | 0 | 0 | 0 | 0 |
| B | 1 (4.2%) | 0 | 0 | 0 | |
| Liver function (total bilirubin) | A | 0 | 0 | 0 | 0 |
| B | 0 | 0 | 0 | 1 (4.2%) | |
| p Values | 0.554 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Z.; Jia, Y.; Tao, L.; Liu, X.; Han, Y.; Wang, X. Clinical Evaluation of Dexamethasone Plus Gentamycin Mouthwash Use in Combination with Total Glucosides of Paeony for Treatment of Oral Lichen Planus without Fungal Infection: A Comparative Study with Long-Term Follow-Up. J. Clin. Med. 2022, 11, 7004. https://doi.org/10.3390/jcm11237004
Zhang Z, Jia Y, Tao L, Liu X, Han Y, Wang X. Clinical Evaluation of Dexamethasone Plus Gentamycin Mouthwash Use in Combination with Total Glucosides of Paeony for Treatment of Oral Lichen Planus without Fungal Infection: A Comparative Study with Long-Term Follow-Up. Journal of Clinical Medicine. 2022; 11(23):7004. https://doi.org/10.3390/jcm11237004
Chicago/Turabian StyleZhang, Zhihui, Yan Jia, Liyuan Tao, Xiaodan Liu, Ying Han, and Xiao Wang. 2022. "Clinical Evaluation of Dexamethasone Plus Gentamycin Mouthwash Use in Combination with Total Glucosides of Paeony for Treatment of Oral Lichen Planus without Fungal Infection: A Comparative Study with Long-Term Follow-Up" Journal of Clinical Medicine 11, no. 23: 7004. https://doi.org/10.3390/jcm11237004
APA StyleZhang, Z., Jia, Y., Tao, L., Liu, X., Han, Y., & Wang, X. (2022). Clinical Evaluation of Dexamethasone Plus Gentamycin Mouthwash Use in Combination with Total Glucosides of Paeony for Treatment of Oral Lichen Planus without Fungal Infection: A Comparative Study with Long-Term Follow-Up. Journal of Clinical Medicine, 11(23), 7004. https://doi.org/10.3390/jcm11237004