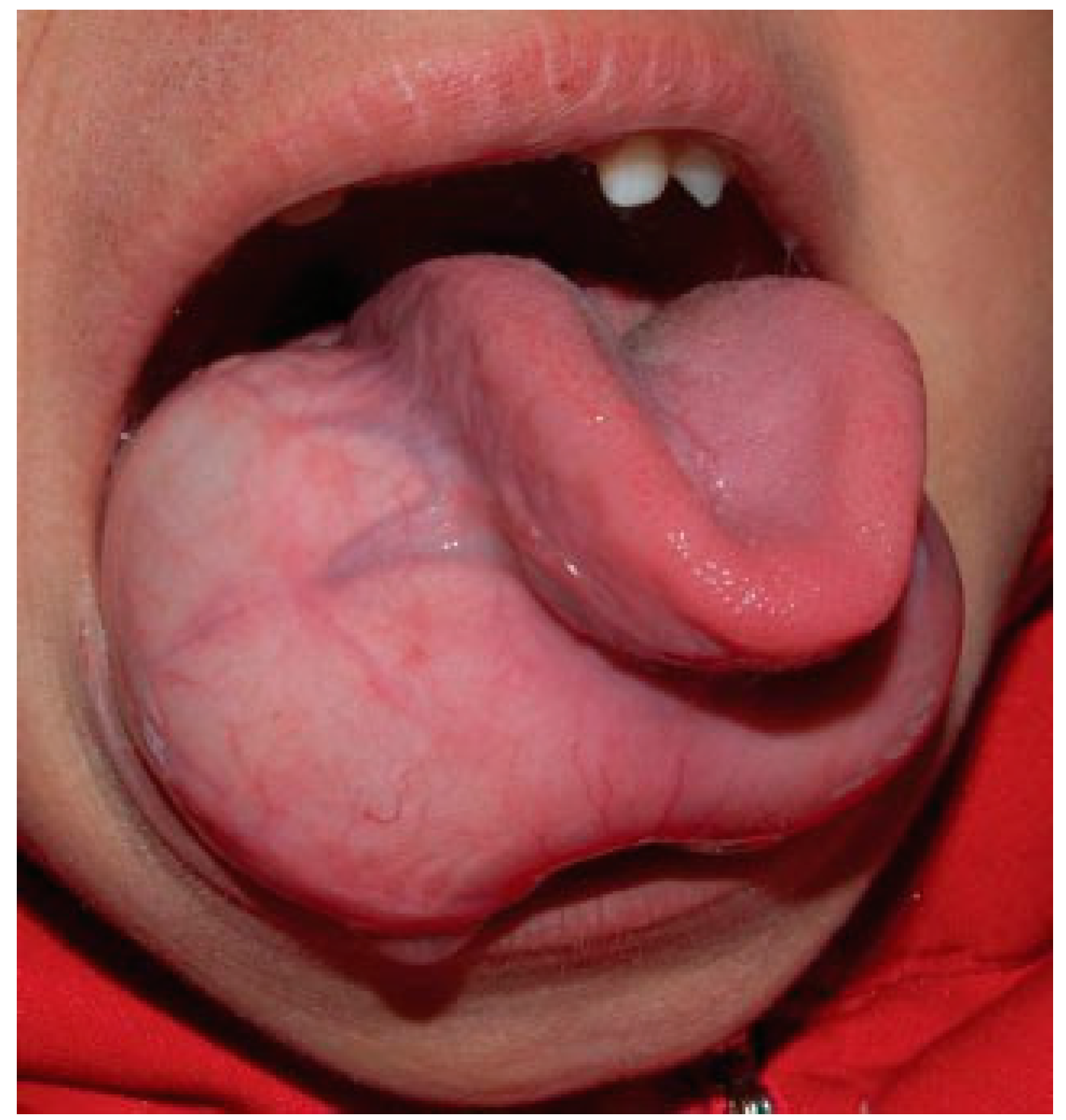
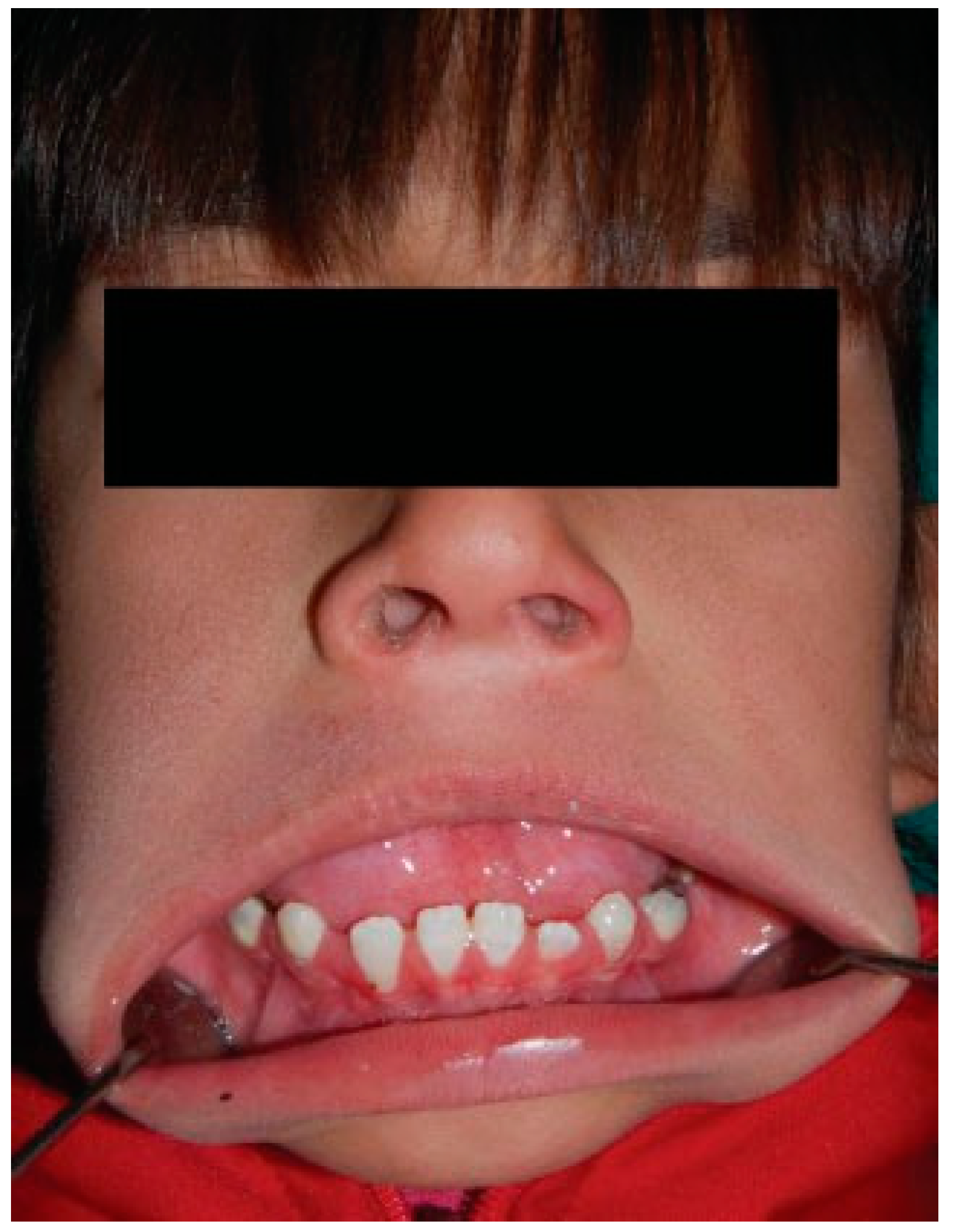
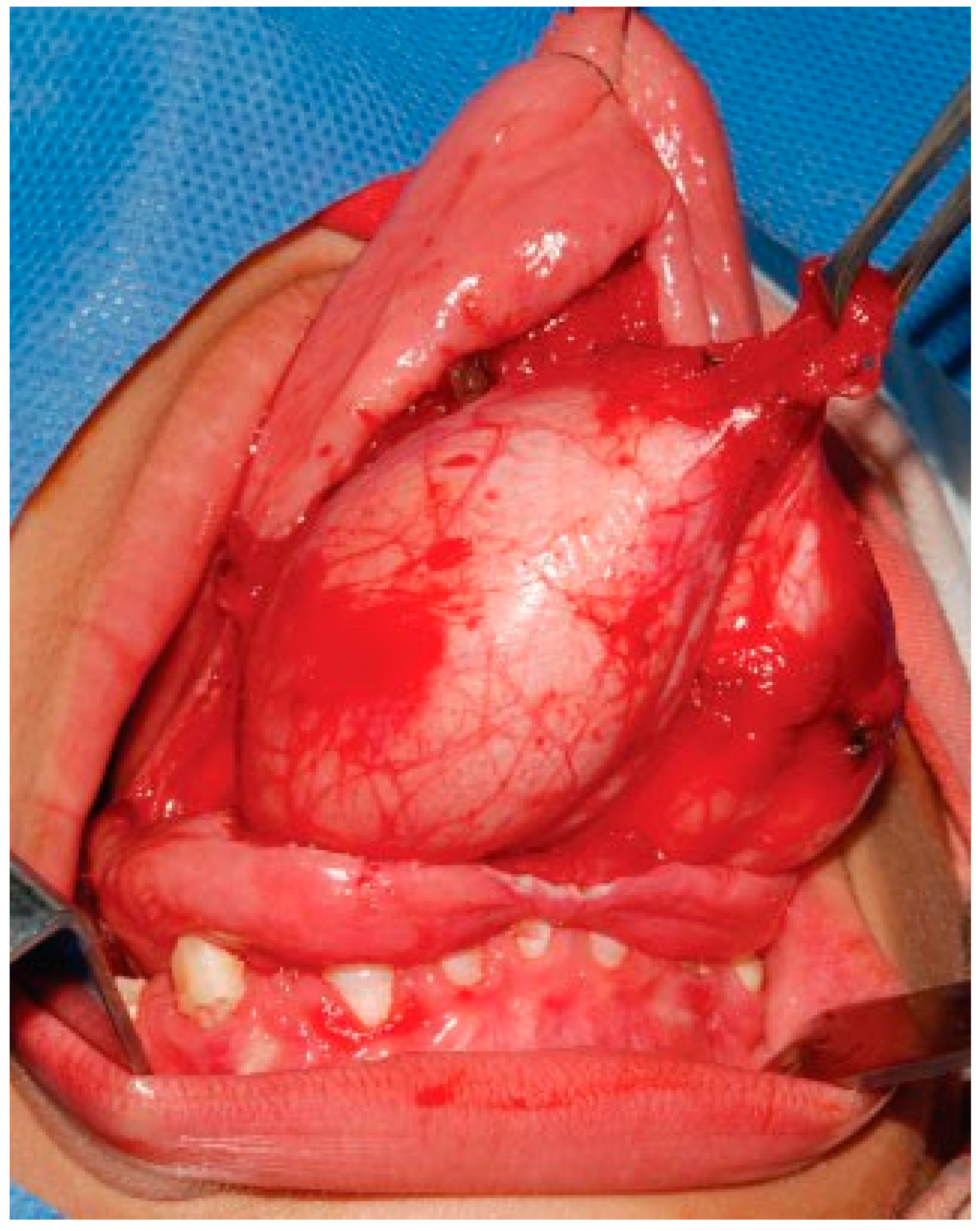
Large Sublingual Dermoid Cyst: A Case of Mandibular Prognathism
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Case Report
Discussion




References
- Rapidis, A.D.; Angelopoulos, A.P.; Scouteris, C. Dermoid cyst of the floor of the mouth. Report of a case. Br J Oral Surg 1981, 19, 43–51. [Google Scholar] [PubMed]
- Pryor, S.G.; Lewis, J.E.; Weaver, A.L.; Orvidas, L.J. Pediatric dermoid cysts of the head and neck. Otolaryngol Head Neck Surg 2005, 132, 938–942. [Google Scholar]
- Pirgousis, P.; Fernandes, R. Giant submental dermoid cysts with near total obstruction of the oral cavity: Report of 2 cases. J Oral Maxillofac Surg 2011, 69, 532–535. [Google Scholar] [PubMed]
- Marino, R.; Pentenero, M.; Familiari, U.; Gandolfo, S. Dermoid cysts of the floor of the mouth: A case report. J Clin Case Rep 2012, 2, 1–4. [Google Scholar]
- Priya Jeyaraj, W.; Sahoo, B. A case of an unusually large sublingual dermoid cyst of the maxillofacial region. J Dent Med Sci 2012, 2, 19–25. [Google Scholar]
- New, G.B.; Erich, J.B. Dermoid cysts of head and neck. Surg Gynecol Obstet 1937, 65, 48. [Google Scholar]
- Graham, R.M.; Thomson, E.F.; Woodwards, R.T.; Sloan, P. Lateral dermoid cyst. Br J Oral Maxillofac Surg 2008, 46, 131–132. [Google Scholar]
- King, R.C.; Smith, B.R.; Burk, J.L. Dermoid cyst in the floor of the mouth. Review of the literature and case reports. Oral Surg Oral Med Oral Pathol 1994, 78, 567–576. [Google Scholar] [CrossRef]
- Armstrong, J.E.; Darling, M.R.; Bohay, R.N.; Cobb, G.; Lawen, D.; Daley, T.D. Trans-geniohyoid dermoid cyst: Considerations on a combined oral and dermal surgical approach and on histogenesis. J Oral Maxillofac Surg 2006, 64, 1825–1830. [Google Scholar]
- Teszler, C.B.; El-Naaj, I.A.; Emodi, O.; Luntz, M.; Peled, M. Dermoid cysts of the lateral floor of the mouth: A comprehensive anatomo-surgical classification of cysts of the oral floor. J Oral Maxillofac Surg 2007, 65, 327–332. [Google Scholar] [CrossRef]
- Mathur, S.K.; Menon, P.R. Dermoid cyst of the tongue: Report of a case. Oral Surg Oral Med Oral Pathol 1980, 50, 217–218. [Google Scholar] [CrossRef]
- Ulbright, T.M.; Srigley, J.R. Dermoid cyst of the testis: A study of five postpubertal cases, including a pilomatrixoma-like variant, with evidence supporting its separate classification from mature testicular teratoma. Am J Surg Pathol 2001, 25, 788–793. [Google Scholar] [CrossRef]
- Di Francesco, A.; Chiapasco, M.; Biglioli, F.; Ancona, D. Intraoral approach to large dermoid cysts of the floor of the mouth: A technical note. Int J Oral Maxillofac Surg 1995, 24, 233–235. [Google Scholar] [CrossRef]
- Longo, F.; Maremonti, P.; Mangone, G.M.; De Maria, G.; Califano, L. Midline (dermoid) cysts of the floor of the mouth: Report of 16 cases and review of surgical techniques. Plast Reconstr Surg 2003, 112, 1560–1565. [Google Scholar] [CrossRef] [PubMed]
- Ariyoshi, Y.; Shimahara, M. Magnetic resonance imaging of a submental dermoid cyst: Report of a case. J Oral Maxillofac Surg 2003, 61, 507–510. [Google Scholar] [CrossRef] [PubMed]
- El-Hakim, I.E.; Alyamani, A. Alternative surgical approaches for excision of dermoid cyst of the floor of mouth. Int J Oral Maxillofac Surg 2008, 37, 497–499. [Google Scholar] [CrossRef] [PubMed]
- Koca, H.; Seckin, T.; Sipahi, A.; Kazanc, A. Epidermoid cyst in the floor of the mouth: Report of a case. Quintessence Int 2007, 38, 473–477. [Google Scholar]
- Raveenthiran, V.; Sam, C.J.; Srinivasan, S.K. A simple approach to airway management for a giant sublingual dermoid cyst. Can J Anaesth 2006, 53, 1265–1266. [Google Scholar] [CrossRef]
- Brusati, R.; Galioto, S.; Tullio, A.; Moscato, G. The midline sagittal glossotomy for treatment of dermoid cysts of the mouth floor. J Oral Maxillofac Surg 1991, 49, 875–878. [Google Scholar] [CrossRef]
- Yeschua, R.; Bab, I.A.; Wexler, M.R.; Neuman, Z. Dermoid cyst of the floor of the mouth in an infant. (Case report). J Maxillofac Surg 1977, 5, 211–213. [Google Scholar] [CrossRef]
- Faerber, T.H.; Hiatt, W.R.; Dunlap, C. Congenital teratoid cyst of the floor of the mouth. J Oral Maxillofac Surg 1988, 46, 487–490. [Google Scholar] [PubMed]
- Gordon, P.E.; Faquin, W.C.; Lahey, E.; Kaban, L.B. Floor-of-mouth dermoid cysts: Report of 3 variants and a suggested change in terminology. J Oral Maxillofac Surg 2013, 71, 1034–1041. [Google Scholar] [PubMed]
- Sanghera, P.; El Modir, A.; Simon, J. Malignant transformation within a dermoid cyst: A case report and literature review. Arch Gynecol Obstet 2006, 274, 178–180. [Google Scholar] [PubMed]
- Moss, M. Kraus, B.S., Reidel, R.A., Eds.; The functional matrix. In Vistas in Orthodontics; Lea & Febiger: Philadelphia, PA, USA, 1962; pp. 85–98. [Google Scholar]
© 2016 by the author. The Author(s) 2016.
Share and Cite
Berbel, P.; Ostrosky, A.; Tosti, F. Large Sublingual Dermoid Cyst: A Case of Mandibular Prognathism. Craniomaxillofac. Trauma Reconstr. 2016, 9, 345-348. https://doi.org/10.1055/s-0036-1581062
Berbel P, Ostrosky A, Tosti F. Large Sublingual Dermoid Cyst: A Case of Mandibular Prognathism. Craniomaxillofacial Trauma & Reconstruction. 2016; 9(4):345-348. https://doi.org/10.1055/s-0036-1581062
Chicago/Turabian StyleBerbel, Pablo, Alejandro Ostrosky, and Franco Tosti. 2016. "Large Sublingual Dermoid Cyst: A Case of Mandibular Prognathism" Craniomaxillofacial Trauma & Reconstruction 9, no. 4: 345-348. https://doi.org/10.1055/s-0036-1581062
APA StyleBerbel, P., Ostrosky, A., & Tosti, F. (2016). Large Sublingual Dermoid Cyst: A Case of Mandibular Prognathism. Craniomaxillofacial Trauma & Reconstruction, 9(4), 345-348. https://doi.org/10.1055/s-0036-1581062