A Protocol to Reduce Interobserver Variability in the Computed Tomography Measurement of Orbital Floor Fractures
Abstract
:Materials and Methods
Computed Tomography Orbits Image Acquisition
Detection of Orbital Fractures
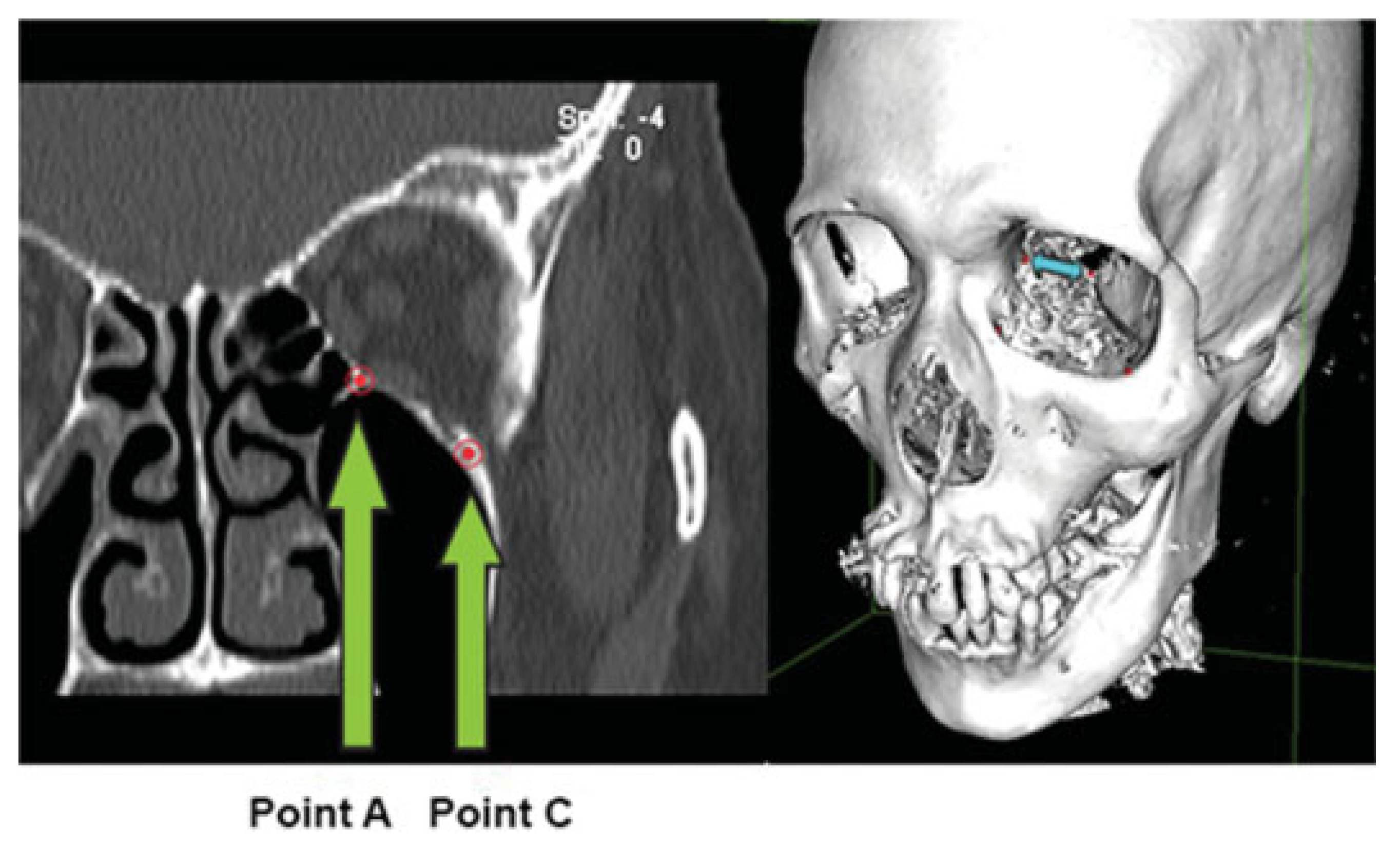
Measurement of Orbital Fractures
Statistical Analysis

Results
Discussion
Indications for Surgery in Orbital Floor Fractures
Advantages of Our Protocol





Measurement of Orbital Defect Area and Orbital Volume
Other Imaging Methods
Funding
Conflicts of Interest
References
- Laine, F.J.; Conway, W.F.; Laskin, D.M. Radiology of maxillofacial trauma. Curr. Probl. Diagn. Radiol. 1993, 22, 145–188. [Google Scholar] [PubMed]
- Lee, H.J.; Jilani, M.; Frohman, L.; Baker, S. CT of orbital trauma. Emerg. Radiol. 2004, 10, 168–172. [Google Scholar]
- Manchio, J.V.; Sati, S.; Rosman, D.A.; Bryan, D.J.; Lee, G.M.; Weinzweig, J. Role of sagittal reformatted computed tomographic images in the evaluation of orbital floor fractures. J. Craniofac Surg. 2010, 21, 1153–1157. [Google Scholar] [PubMed]
- Manson, P.N.; Grivas, A.; Rosenbaum, A.; Vannier, M.; Zinreich, J.; Iliff, N. Studies on enophthalmos: II. The measurement of orbital injuries and their treatment by quantitative computed tomography. Plast. Reconstr. Surg. 1986, 77, 203–214. [Google Scholar]
- Hawes, M.J.; Dortzbach, R.K. Surgery on orbital floor fractures. Influence of time of repair and fracture size. Ophthalmology 1983, 90, 1066–1070. [Google Scholar]
- Jin, H.R.; Shin, S.O.; Choo, M.J.; Choi, Y.S. Relationship between the extent of fracture and the degree of enophthalmos in isolated blowout fractures of the medial orbital wall. J. Oral. Maxillofac. Surg. 2000, 58, 617–620, discussion 620–621. [Google Scholar]
- Gilbard, S.M.; Mafee, M.F.; Lagouros, P.A.; Langer, B.G. Orbital blowout fractures. The prognostic significance of computed tomography. Ophthalmology 1985, 92, 1523–1528. [Google Scholar] [PubMed]
- Lelli, G.J., Jr.; Milite, J.; Maher, E. Orbital floor fractures: evaluation, indications, approach, and pearls from an ophthalmologist’s perspective. Facial Plast. Surg. 2007, 23, 190–199. [Google Scholar]
- Jin, H.R.; Shin, S.O.; Choo, M.J.; Choi, Y.S. Relationship between the extent of fracture and the degree of enophthalmos in isolated blowout fractures of the medial orbital wall. J. Oral. Maxillofac. Surg. 2000, 58, 617–620, discussion 620–621. [Google Scholar]
- Manson, P. Facial fractures. In Plastic Surgery, 2nd ed; Mathes, S., Ed.; Elsevier: Philadelphia, PA, USA, 2006. [Google Scholar]
- Schouman, T.; Courvoisier, D.S.; Van Issum, C.; Terzic, A.; Scolozzi, P. Can systematic computed tomographic scan assessment predict treatment decision in pure orbital floor blowout fractures? J. Oral. Maxillofac. Surg. 2012, 70, 1627–1632. [Google Scholar]
- Burnstine, M.A. Clinical recommendations for repair of isolated orbital floor fractures: an evidence-based analysis. Ophthalmology 2002, 109, 1207–1210, discussion 620–621, quiz 1212–1213. [Google Scholar] [PubMed]
- Ploder, O.; Klug, C.; Voracek, M.; Burggasser, G.; Czerny, C. Evaluation of computer-based area and volume measurement from coronal computed tomography scans in isolated blowout fractures of the orbital floor. J. Oral. Maxillofac. Surg. 2002, 60, 1267–1272, discussion 1273–1274. [Google Scholar] [PubMed]
- Connor, S.E.; Tan, G.; Fernando, R.; Chaudhury, N. Computed tomography pseudofractures of the mid face and skull base. Clin. Radiol. 2005, 60, 1268–1279. [Google Scholar]
- Schouman, T.; Courvoisier, D.S.; Imholz, B.; Van Issum, C.; Scolozzi, P. Computational area measurement of orbital floor fractures: reliability, accuracy and rapidity. Eur. J. Radiol. 2012, 81, 2251–2254. [Google Scholar]
- Charteris, D.G.; Chan, C.H.; Whitehouse, R.W.; Noble, J.L. Orbital volume measurement in the management of pure blowout fractures of the orbital floor. Br. J. Ophthalmol. 1993, 77, 100–102. [Google Scholar] [PubMed]
- Hwang, K.; You, S.H.; Sohn, I.A. Analysis of orbital bone fractures: a 12-year study of 391 patients. J. Craniofac Surg. 2009, 20, 1218–1223. [Google Scholar]
- Baumann, A.; Burggasser, G.; Gauss, N.; Ewers, R. Orbital floor reconstruction with an alloplastic resorbable polydioxanone sheet. Int. J. Oral. Maxillofac. Surg. 2002, 31, 367–373. [Google Scholar]
- Cai, E.Z.; Koh, Y.P.; Hing, E.C.; et al. Computer-assisted navigational surgery improves outcomes in orbital reconstructive surgery. J. Craniofac Surg. 2012, 23, 1567–1573. [Google Scholar]
- Wang, L.; Wang, J. On the positive correlation between the percentage of acute fracture of medial orbital wall and the degree of injury of affected medial rectus muscle by CT image. Eur. J. Radiol. 2012, 81, e58–e61. [Google Scholar] [CrossRef]
- Ploder, O.; Klug, C.; Voracek, M.; et al. A computer-based method for calculation of orbital floor fractures from coronal computed tomography scans. J. Oral. Maxillofac. Surg. 2001, 59, 1437–1442. [Google Scholar]
- Jaquiéry, C.; Aeppli, C.; Cornelius, P.; Palmowsky, A.; Kunz, C.; Hammer, B. Reconstruction of orbital wall defects: critical review of 72 patients. Int. J. Oral. Maxillofac. Surg. 2007, 36, 193–199. [Google Scholar] [PubMed]
- Ploder, O.; Oeckher, M.; Klug, C.; et al. Follow-up study of treatment of orbital floor fractures: relation of clinical data and software-based CT-analysis. Int. J. Oral. Maxillofac. Surg. 2003, 32, 257–262. [Google Scholar]
- Fan, X.; Li, J.; Zhu, J.; Li, H.; Zhang, D. Computer-assisted orbital volume measurement in the surgical correction of late enophthalmos caused by blowout fractures. Ophthal Plast. Reconstr. Surg. 2003, 19, 207–211. [Google Scholar]
- Raskin, E.M.; Millman, A.L.; Lubkin, V.; della Rocca, R.C.; Lisman, R.D.; Maher, E.A. Prediction of late enophthalmos by volumetric analysis of orbital fractures. Ophthal Plast. Reconstr. Surg. 1998, 14, 19–26. [Google Scholar]
- Kwon, J.; Barrera, J.E.; Most, S.P. Comparative computation of orbital volume from axial and coronal CT using three-dimensional image analysis. Ophthal Plast. Reconstr. Surg. 2010, 26, 26–29. [Google Scholar] [PubMed]
- Dolynchuk, K.N.; Tadjalli, H.E.; Manson, P.N. Orbital volumetric analysis: clinical application in orbitozygomatic complex injuries. J. Craniomaxillofac Trauma. 1996, 2, 56–63, discussion 64. [Google Scholar] [PubMed]
- Ye, J.; Kook, K.H.; Lee, SY. Evaluation of computer-based volume measurement and porous polyethylene channel implants in reconstruction of large orbital wall fractures. Invest. Ophthalmol. Vis. Sci. 2006, 47, 509–513. [Google Scholar]
- Jank, S.; Deibl, M.; Strobl, H.; et al. Intrarater reliability in the ultrasound diagnosis of medial and lateral orbital wall fractures with a curved array transducer. J. Oral. Maxillofac. Surg. 2006, 64, 68–73. [Google Scholar]
- Cruz, A.A.; Eichenberger, G.C. Epidemiology and management of orbital fractures. Curr. Opin. Ophthalmol. 2004, 15, 416–421. [Google Scholar]
- Qu, X.M.; Li, G.; Zhang, Z.Y.; Ma, X.C. Comparative dosimetry of dental cone-beam computed tomography and multi-slice computed tomography for oral and maxillofacial radiology [in Chinese]. Zhonghua Kou Qiang Yi Xue Za Zhi 2011, 46, 595–599. [Google Scholar]
- Chang, E.L.; Bernardino, C.R. Update on orbital trauma. Curr. Opin. Ophthalmol. 2004, 15, 411–415. [Google Scholar]
- Hoelzle, F.; Klein, M.; Schwerdtner, O.; et al. Intraoperative computed tomography with the mobile CT Tomoscan M during surgical treatment of orbital fractures. Int. J. Oral. Maxillofac. Surg. 2001, 30, 26–31. [Google Scholar]
- Papadopoulos, M.A.; Christou, P.K.; Christou, P.K.; et al. Three-dimensional craniofacial reconstruction imaging. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2002, 93, 382–393. [Google Scholar] [PubMed]
- Grivas, A.; Manson, P.N.; Vannier, M.W.; Rosenbaum, A. Post-traumatic orbit evaluation by three-dimensional surface reconstructions. Comput. Med. Imaging Graph. 1988, 12, 47–57. [Google Scholar]
- Ploder, O.; Klug, C.; Backfrieder, W.; Voracek, M.; Czerny, C.; Tschabitscher, M. 2Dand 3D-based measurements of orbital floor fractures from CT scans. J. Craniomaxillofac Surg. 2002, 30, 153–159. [Google Scholar] [PubMed]
- Deveci, M.; Oztürk, S.; Sengezer, M.; Pabuşcu, Y. Measurement of orbital volume by a 3-dimensional software program: an experimental study. J. Oral. Maxillofac. Surg. 2000, 58, 645–648. [Google Scholar] [PubMed]
- Kolk, A.; Pautke, C.; Schott, V.; et al. Secondary post-traumatic enophthalmos: high-resolution magnetic resonance imaging compared with multislice computed tomography in postoperative orbital volume measurement. J. Oral. Maxillofac. Surg. 2007, 65, 1926–1934. [Google Scholar]
- Loba, P.; Laudanska-Olszewska, I.; Majos, A.; Stefańczyk, L.; BroniarczykLoba, A. The use of dynamic magnetic resonance in the diagnosis of ocular motility disorders. Klin. Oczna 2011, 113, 52–55. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





© 2015 by the author. The Author(s) 2015.
Share and Cite
Ang, C.H.; Low, J.R.; Shen, J.Y.; Cai, E.Z.Y.; Hing, E.C.H.; Chan, Y.H.; Sundar, G.; Lim, T.C. A Protocol to Reduce Interobserver Variability in the Computed Tomography Measurement of Orbital Floor Fractures. Craniomaxillofac. Trauma Reconstr. 2015, 8, 289-298. https://doi.org/10.1055/s-0034-1399800
Ang CH, Low JR, Shen JY, Cai EZY, Hing ECH, Chan YH, Sundar G, Lim TC. A Protocol to Reduce Interobserver Variability in the Computed Tomography Measurement of Orbital Floor Fractures. Craniomaxillofacial Trauma & Reconstruction. 2015; 8(4):289-298. https://doi.org/10.1055/s-0034-1399800
Chicago/Turabian StyleAng, Chuan Han, Jin Rong Low, Jia Yi Shen, Elijah Zheng Yang Cai, Eileen Chor Hoong Hing, Yiong Huak Chan, Gangadhara Sundar, and Thiam Chye Lim. 2015. "A Protocol to Reduce Interobserver Variability in the Computed Tomography Measurement of Orbital Floor Fractures" Craniomaxillofacial Trauma & Reconstruction 8, no. 4: 289-298. https://doi.org/10.1055/s-0034-1399800
APA StyleAng, C. H., Low, J. R., Shen, J. Y., Cai, E. Z. Y., Hing, E. C. H., Chan, Y. H., Sundar, G., & Lim, T. C. (2015). A Protocol to Reduce Interobserver Variability in the Computed Tomography Measurement of Orbital Floor Fractures. Craniomaxillofacial Trauma & Reconstruction, 8(4), 289-298. https://doi.org/10.1055/s-0034-1399800