Orbital floor fractures are a common sequela of blunt trauma to the face. Floor fractures may be accom- panied by medial orbital wall fractures in 7 to 53% of cases [
1,
2,
3,
4]. However, isolated fractures of the medial orbi- tal wall are an uncommon occurrence and are oftentimes
asymptomatic. Although the indications for manage- ment of orbital floor fractures have been extensively discussed [
5,
6,
7,
8,
9,
10,
11]
, isolated medial wall fractures have re- ceived less attention in the published literature.The medial orbital wall differs from the floor in that there are multiple bony septae within the ethmoid sinus that provide reinforcement and support to the thin medial wall. This is felt to decrease the incidence of fracture of the medial wall [
12]. Similar to the orbital floor, there are two primary theories as to the mechanism of fractures to the medial wall. The ‘‘buckling theory’’ holds that there is transmission of force from an anterior blow that deforms but does not fracture the bony rim, which then causes the thinner medial orbital wall to fracture [
13]. ‘‘The hydraulic theory’’ maintains that a traumatic im- pact to the soft tissue of the orbit displaces the tissue into the orbital cavity, resulting in fracture of the orbital bones. Though cadaveric studies have supported the hydraulic theory most recently [
2], it is more likely that a combination of these two mechanisms plays a role in the pathophysiology of the fractures depending on the mechanism of the trauma. Medial wall fractures com- bined with orbital floor fractures have been shown in cadaveric studies to require an increase in energy from 4900 millijoules to 6860 millijoules [
14]. Additionally, it has been hypothesized that certain ethnic groups such as patients of black descent may be anatomically predis- posed toward medial wall fractures [
15,
16].
Often, medial wall fractures are diagnosed as incidental findings on computed tomographic (CT) scans in asymptomatic patients. In addition, unsuspected medial wall fractures may manifest if the patient blows his nose after trauma and develops subcutaneous em- physema. Less common, but of greater concern, are patients who present with abduction or adduction deficit from incarceration of the medial rectus in a medial wall fracture. Although ‘‘trapdoor’’ blowout fractures of the orbital floor commonly present with entrapment and limitation of vertical motility, medial wall fractures less often present with medial rectus incarceration. Unlike orbital floor fractures, where an entrapped inferior rectus is usually manifest by restriction of elevation of the globe, patients with medial rectus entrapment in isolated medial wall fractures are more likely to present with findings consistent with paresis of the entrapped muscle rather than restrictive limitation of excursions. The motility dysfunction caused by an entrapped medial rectus muscle also has been reported to have a delayed onset several days following the initial trauma. This is felt to presumably be due to ischemia of the entrapped muscle with loss of function [
17].
Medial wall fractures should be suspected in any patient who has suffered blunt periocular trauma. Ex- amination of these patients should include a full oph- thalmic exam to rule out associated ocular injuries. Special attention should be paid toward evaluation of horizontal motility and measurement of globe displace- ment and enophthalmos. Although soft tissue signs of medial wall fracture, including periorbital edema and ecchymosis, subcutaneous emphysema, and epistaxis, may be present [
18], many patients with medial wall frac- tures are asymptomatic, and imaging may pick up the fracture as an incidental finding.
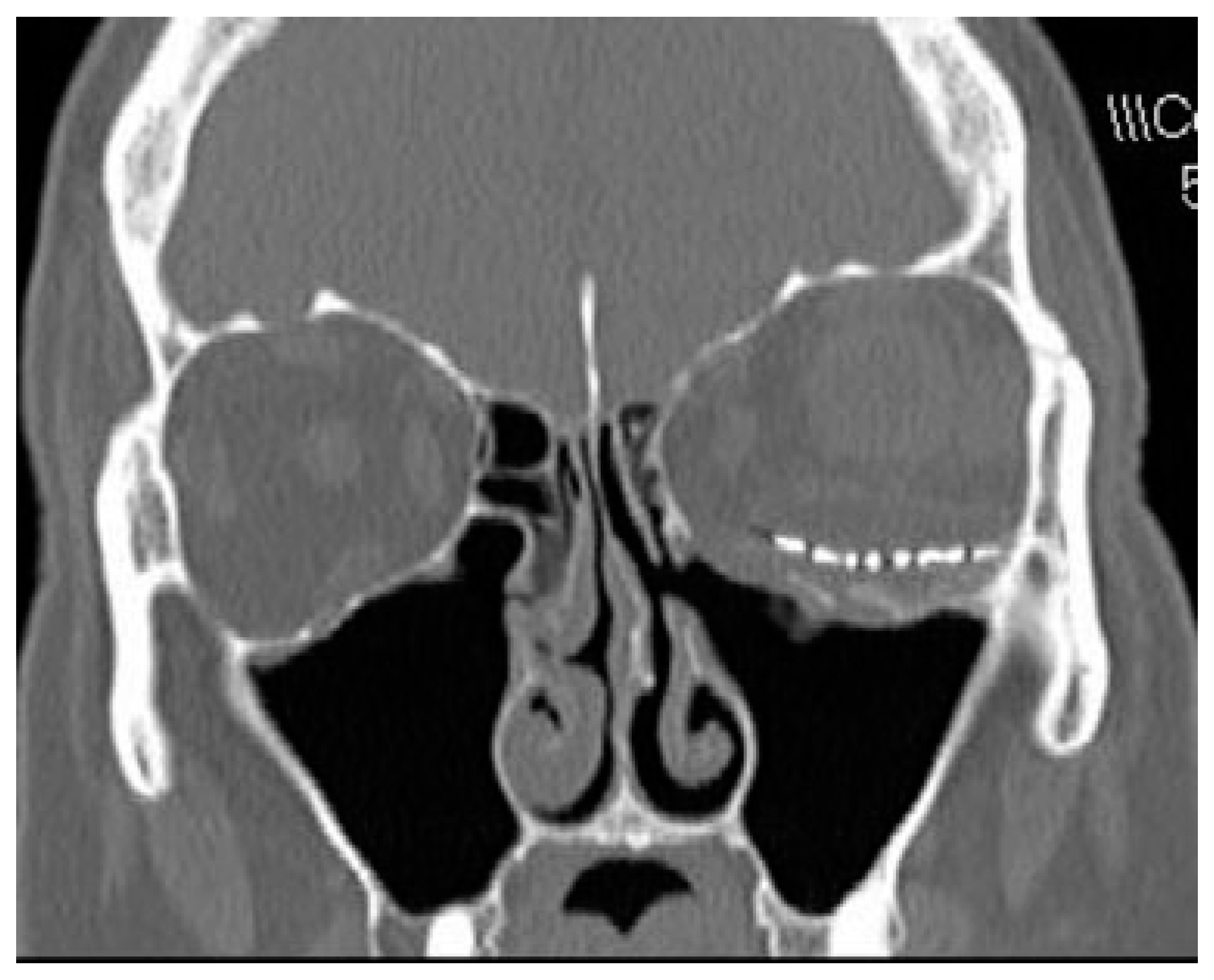
CT scans with coronal and axial views are the imaging modality of choice in suspected orbital fracture cases. On CT scan, subtle medial wall fractures can be detected by comparing the distance from the midline to the medial wall on the injured and uninjured sides. The fractured side will often show a decreased distance in comparison to the unaffected side (
Figure 1). However, CT scan may show minimal displacement of the medial wall
if the elastic bone returns back to its original position once the deforming pressure is released and the medial wall defect may ‘‘self-seal.’’ Plain film imaging for medial wall fractures is considered obsolete and can only detect less than 50% of fractures [
18]
.“Trapdoor fracture” of the orbital floor is well described. This occurs more commonly in the pediatric population, which tends to have more elastic and thicker bones [
8,
17,
19]. Similarly, medial wall orbital fractures with entrapment of extraocular muscle are largely limited to the pediatric population [
17]. In this situation, the initial blow may cause the orbital contents to be displaced into the sinus through a bone that has partially fractured and formed a hinge. Once the pressure from the blow is released, the bone returns to its original position, trap- ping the orbital contents in the ethmoid sinus. Patients with orbital floor trapdoor fractures often present with minimal soft tissue signs of trauma, leading Jordan et al. to designate them as ‘‘white-eyed blowout’’ fractures [
8]. We have similarly found that patients with isolated medial wall trapdoor fractures also have minimal ecchy- mosis or swelling [
17]. These patients may show limitations of both abduction and adduction.
Patients with medial wall fractures may present with varying motility deficits. Although most patients with isolated medial wall fractures without entrapment are not expected to have motility deficits, patients with incarceration of the medial rectus within the fracture site will experience limitation of movement on horizontal versions. This may present either as a limitation of abduction, adduction, or both. Although one would expect limited abduction due to mechanical restriction of the entrapped medial rectus muscle to dominate, surprisingly, this is less common than paretic limitation of adduction of the affected eye [
17]. The variable degree of abduction limitation probably reflects the variable amount of ‘‘slack’’ medial rectus anterior to the site of entrapment. If there is a surplus of muscle length present anterior to the entrapment site, then there will be little or no restriction of abduction. If there is little excessively ‘‘slack’’ muscle present anterior to the fracture site, then restriction of the abduction will be more prominent. Patients with a tightly entrapped medial rectus in the fracture site can also demonstrate retraction of the palpebral fissure associated with their restricted lateral gaze [
9] due to the force generated by the lateral rectus muscle tugging against the tightly entrapped medial rectus.
Limitation of adduction may reflect either paresis of the medial rectus muscle or loss of mechanical advantage to generate force to adduct the globe. Often, the adduction deficit reflects a combination of anterior displacement of the effective point of origin from the orbital apex up to the fracture site, in combination with paresis due to ischemia and/or neuropraxia of the en- trapped and ischemic medial rectus muscle [
17]. This may
occur due to a relative ‘‘compartment syndrome’’ caused by tight incarceration of the muscle within the fracture sight [
10]
. This may have delayed onset and progress over time as progressive ischemia develops [
17]
.The pattern of motility dysfunction in patients with incarcerated medial wall fractures likely depends on the location of the entrapment along the medial wall and the relative laxity of muscle anterior to this point. More anterior fractures will have an effective anterior origin of the muscle, which will limit adduction. In addition, greater laxity of the medial rectus anterior to the entrap- ment will also minimize adduction due to a reduced force vector generated by contracture. The amount of laxity also will affect the abduction deficit. Patients with minimal laxity anterior to the fracture will show me- chanical restriction of abduction, and patients with relative laxity of the medial rectus may retain normal adduction[
17] (
Figure 2).
Exophthalmometry is also used to measure rela- tive enophthalmos or exophthalmos in patients with medial wall fractures. Without an exophthalmometer, this can be evaluated by allowing patients to lean their head back and viewing relative globe position from below (
Figure 3). Enophthalmos after orbital fracture can be the result of fat necrosis and atrophy, entrapment of
tissues within a fracture causing retention of the globe in a recessed position, cicatricial contracture of tissue, or prolapse of orbital contents [
6]
.Enophthalmos is an uncommon sign in patients with isolated medial wall fractures but is twice as common in patients with combined medial wall and floor fractures [
18]. In the largest series of isolated medial wall fractures, only one patient presented with enoph- thalmos [
17].
Entrapment of the inferior rectus has been re- ported to cause an oculocardiac reflex with globe ex- cursions, and there has been one reported case of a similar bradycardiac response with attempted abduction with isolated medial wall fracture with medial rectus muscle entrapment [
17,
20]. Patients who exhibit an oculo- cardiac reflex require immediate treatment. The in- creased vagal tone from soft tissue entrapment results from an altered trigeminal pathway via the reticular formation to the visceral motor nuclei. These patients are at risk for cardiac syncope and necessitate immediate surgery [
5].
Indications for surgical intervention with medial wall fractures include clinically significant enophthal- mos, evidence of entrapment of medial rectus muscle on imaging associated with diplopia, and/or nausea, vomit- ing, or bradycardia with attempted eye movement. Patients with normal motility regardless of size of fracture may be followed to see if clinically significant enophthalmos develops. If it does, it can be repaired satisfactorily even after prolonged interval after injury [
17]. It has been our experience that large isolated medial wall fractures rarely lead to clinically significant enophthal- mos. With long-term follow-up, these patients do not require any intervention and do well.
Patient with medial rectus entrapment trapdoor fractures need early intervention as there may be reduced blood flow and nerve compression leading to permanent injury to the muscle [
8,
19]. Although traditionally a 2-week observation period was recommended in orbital blowout fractures to allow for posttraumatic edema to resolve, current management favors early intervention when frank extraocular muscle entrapment is present [
7,
19]. In the largest published series of isolated medial wall fractures, early intervention resulted in ultimate resolu- tion of diplopia in all patients with entrapment [
17].
Our favorite approach is a transcaruncular medial orbitotomy of the medial wall [
17]. This has replaced the traditional percutaneous frontoethmoidal approach. Others have advocated endoscopic endonasal fracture reduction, but we have no experience with this technique and favor the direct view of the fracture site and intra- orbital contents afforded by the transcaruncular ap- proach. In all surgical interventions, repositioning the prolapsed soft tissue into the orbit is a priority. Allo- plastic material, if needed, may then be placed along the medial wall to retain the soft tissue in place in the orbit and prevent it from prolapsing back into the ethmoid sinus. Smaller fractures may benefit from release and repositioning of the prolapsed soft tissue and removal of the loose bone without implant placement. In the series presented by Brannan et al., eight of nine patients with medial wall fracture did not have an implant placed with minimal postoperative residual enophthalmos [
17]. After removal of the medial wall, enophthalmos did not develop in these patients. One patient, who had an
implant placed, presented with enophthalmos and had sustained the injury several months prior. Use of autol- ogous bone grafts is feasible but largely obsolete secon- dary to the development of excellent alloplastic materials. Endoscopic nasal approaches may also involve the placement of a temporary balloon to maintain the alloplastic graft in place [
21]
. Surgical intervention is not without the complications of vision loss, worsening diplopia, and infection of implant material or implant migration [
5]
.In summary, medial wall fractures can provide a diagnostic and management challenge to surgeons. Ocular motility and relative enophthalmos are critical components of the workup of these patients. The vast majority of nondisplaced fractures without entrapment do not require surgery. Of note, ‘‘trapdoor’’ fractures are much more likely to require early intervention to prevent permanent injury to the muscle. Once released, muscle function and resulting diplopia are expected to improve over time.
{kind=link}
{kind=link}
{kind=link}