Periorbital Trauma: A New Classification
Abstract
:Patients and Methods
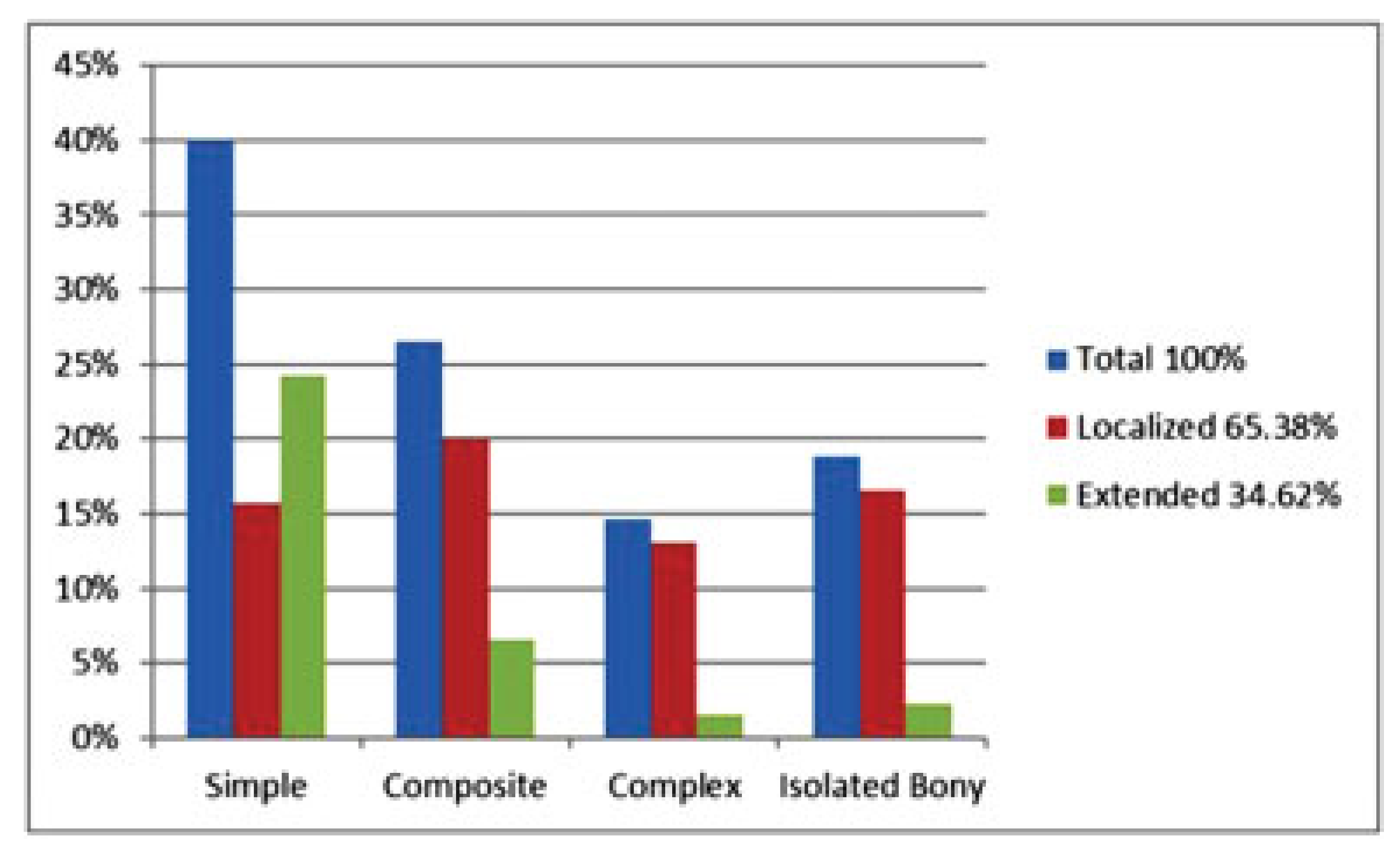
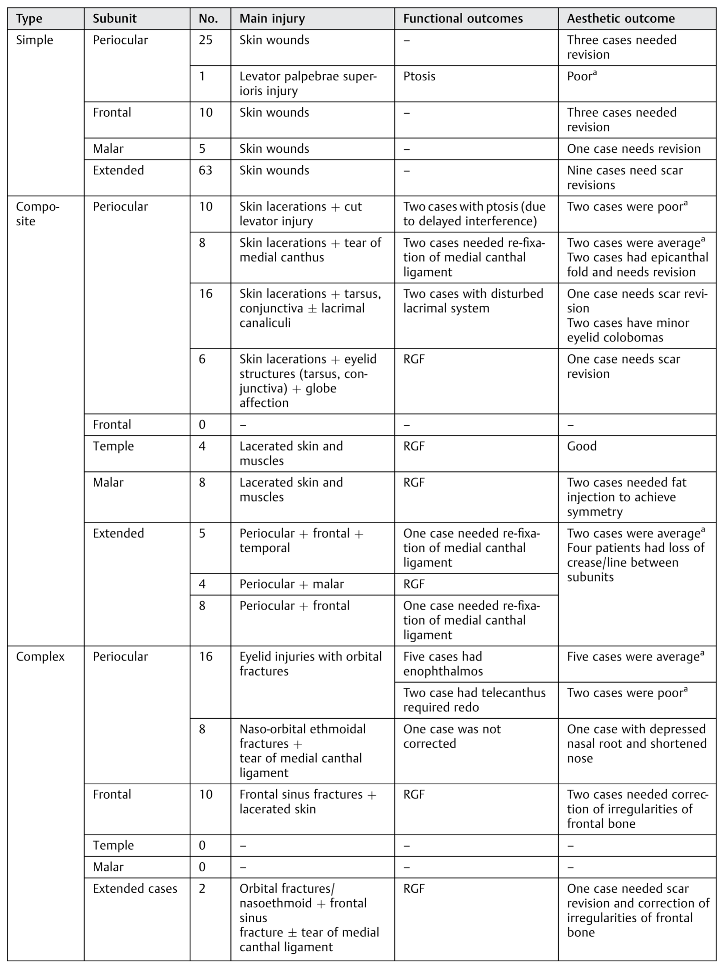
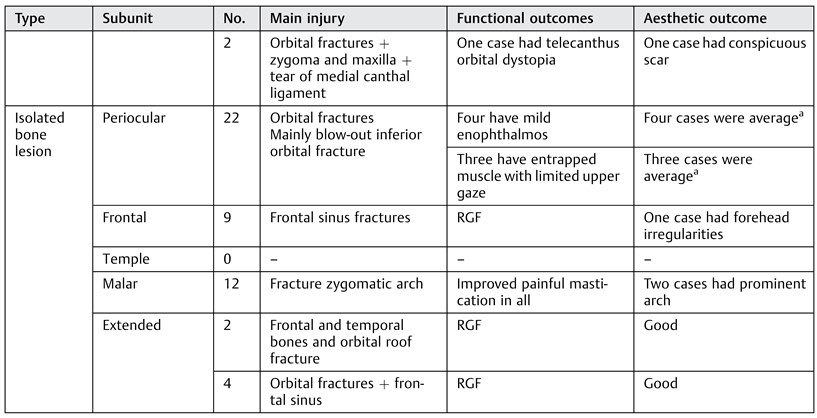
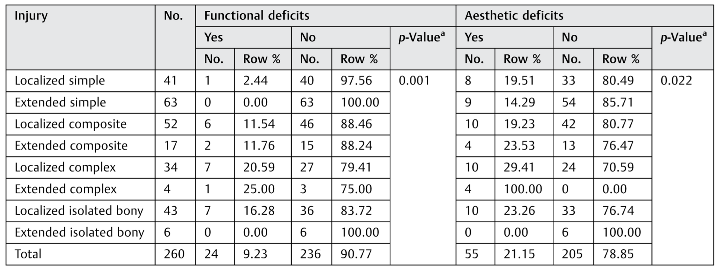
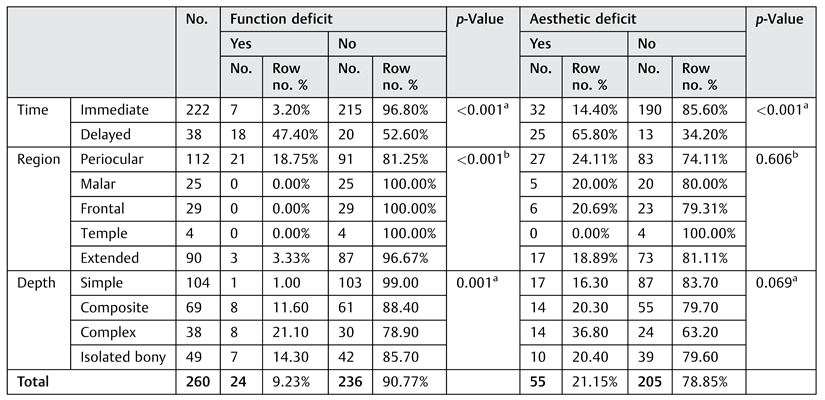
Results
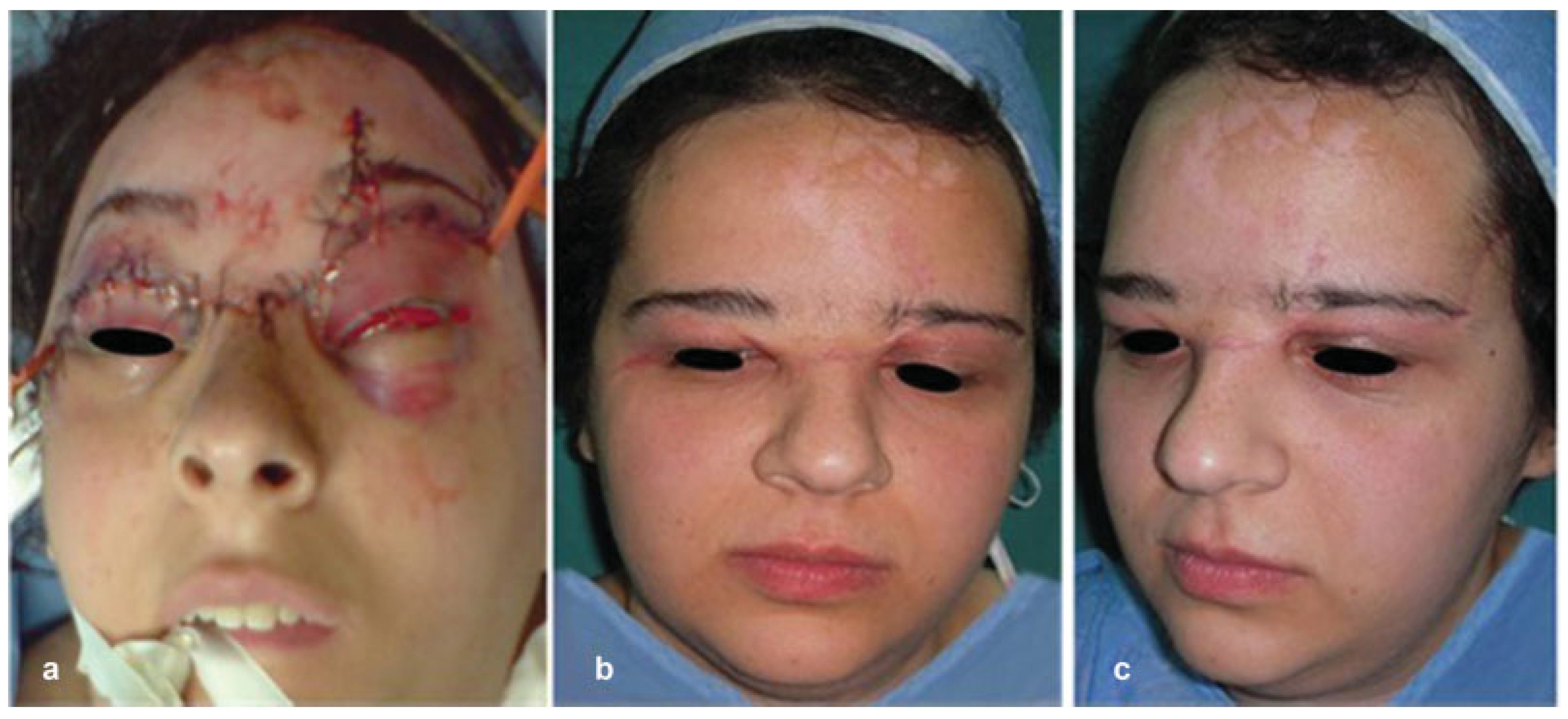
Cases Showing Improper Management of Periorbital Injuries
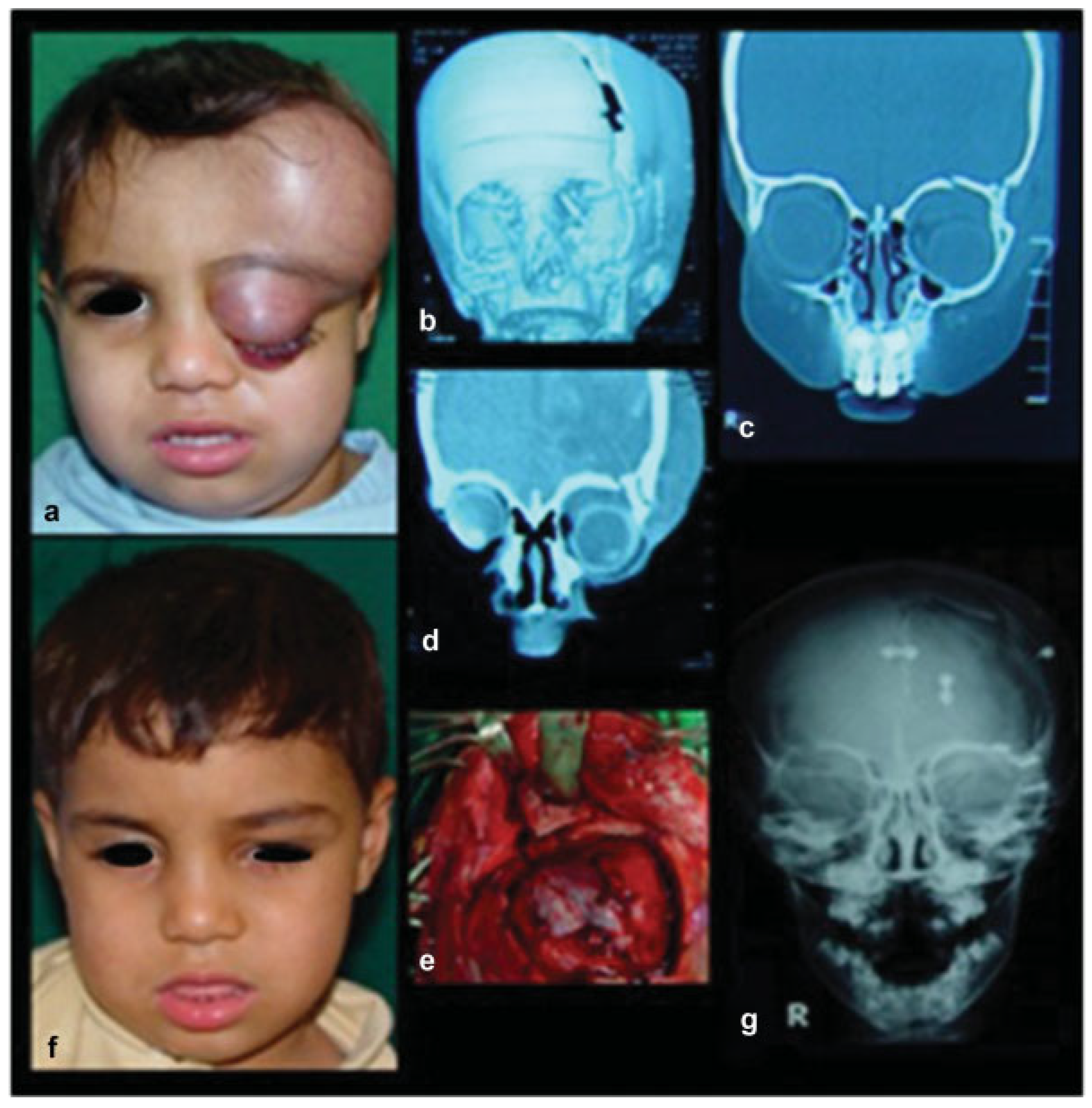
Case 1
Case 2
Case 4
Case 5
- I.
- General approach to periorbital trauma:
- Primary trauma survey.
- Management of life-threatening conditions.
- Primary ophthalmic survey.
- Assessment of concomitant injuries.
- Complete history and general examination.
- Thorough complete head and neck examination.
- Facial CT.
- Full ophthalmic assessment.
- Routine investigations.
- Consulting other specialties if needed.
- Counseling patients and/or their relatives.
- Preinjury photographs if available.
- Documentation.
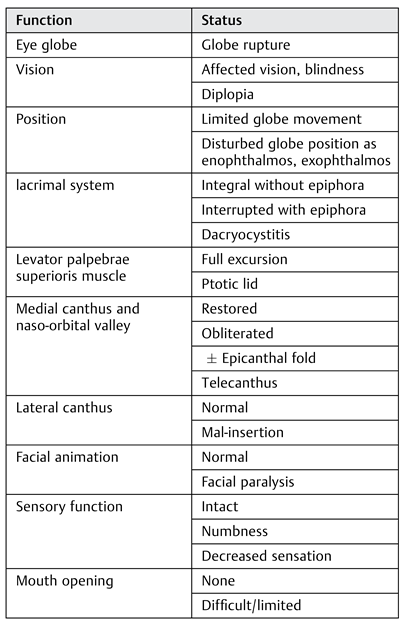
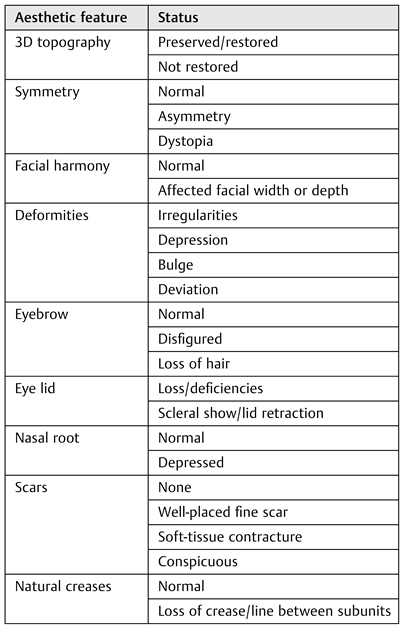
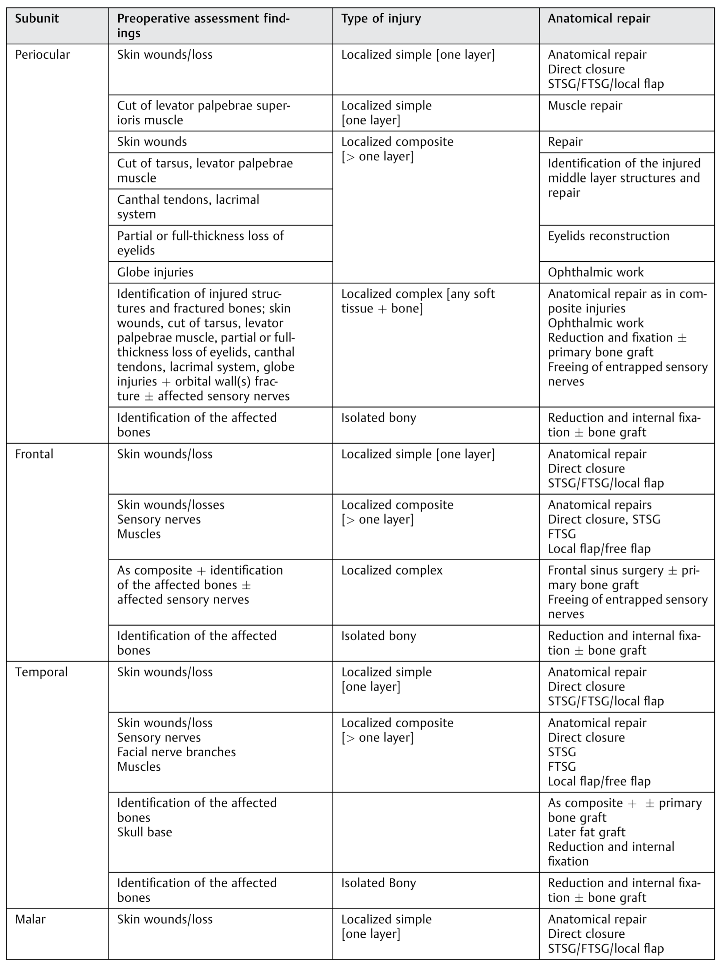
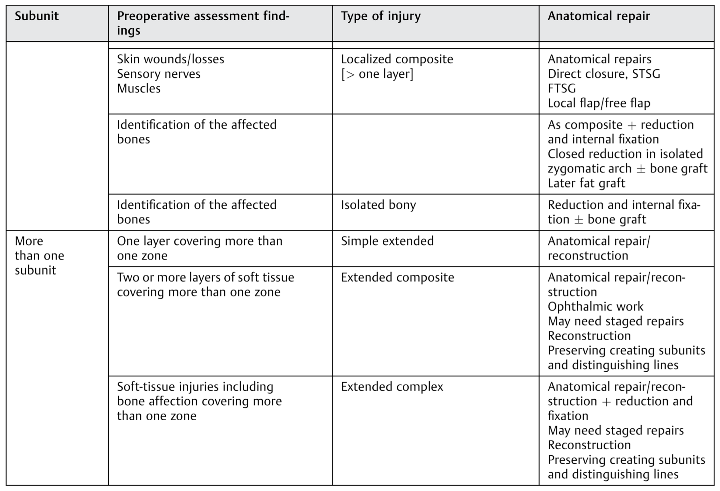
- I.
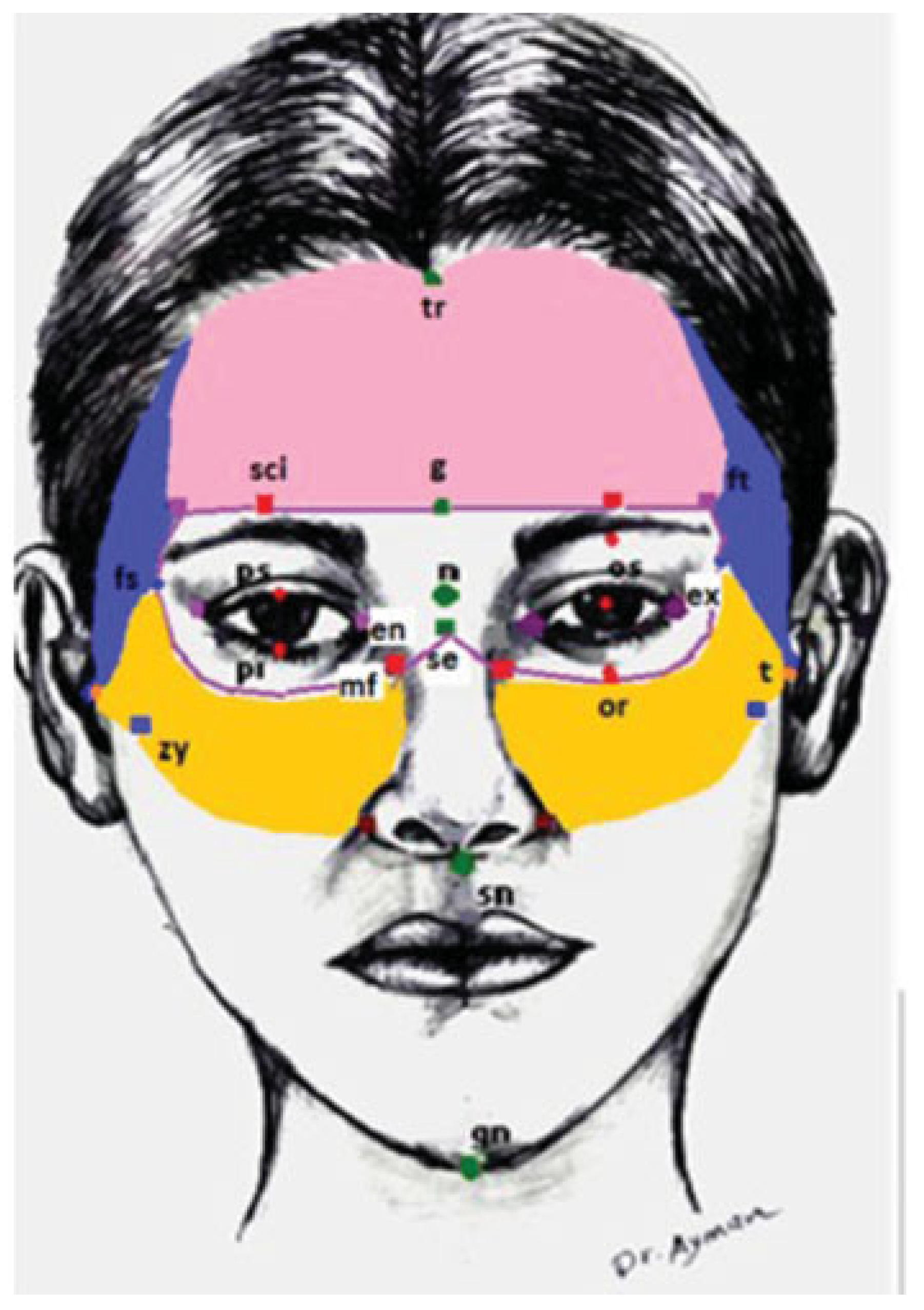
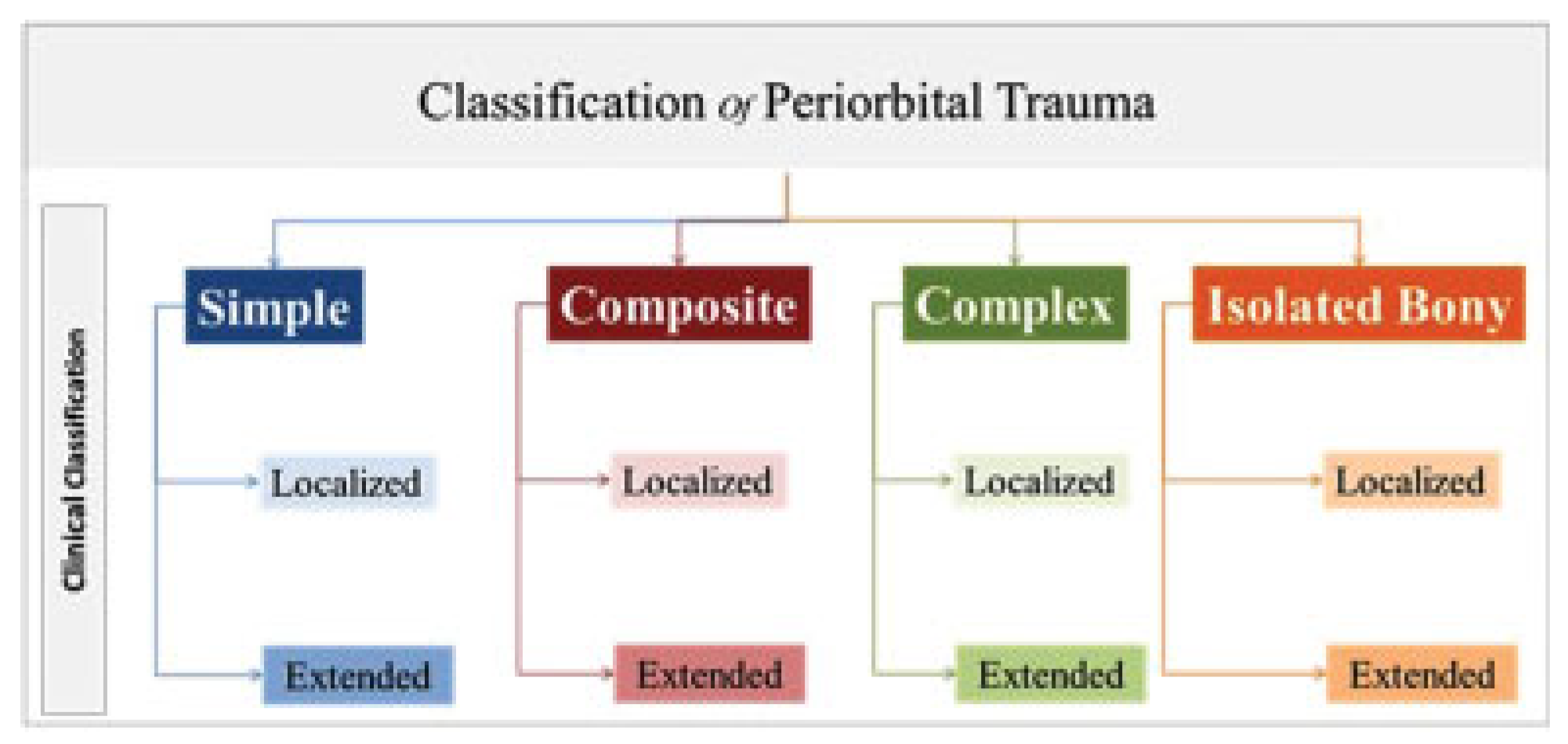
- Categorization of periorbital injuries:
Discussion
Conclusion
Disclosure
References
- Yüce, S.; Demir, Z.; Selçuk, C.T.; Celebioğlu, S. Reconstruction of periorbital region defects: a retrospective study. Ann Maxillofac Surg 2014, 4, 45–50. [Google Scholar] [CrossRef]
- Berli, J.U.; Merbs, S.L.; Grant, M.P. Reconstruction of periorbital soft tissue defects. Facial Plast Surg 2014, 30, 561–569. [Google Scholar] [CrossRef]
- Mathes, D.W.; Edwards, J.A.; Anzai, Y.; Neligan, P.C. A functional periorbital subunit allograft: vascular, anatomic, and technical considerations for future subunit facial transplantation. J Plast Reconstr Aesthet Surg 2014, 67, 1371–1377. [Google Scholar] [PubMed]
- Sosin, M.; Mundinger, G.S.; Dorafshar, A.H.; et al. Optimizing recon- struction with periorbital transplantation: clinical indications and anatomic considerations. Plast Reconstr Surg Glob Open 2016, 4, e628. [Google Scholar] [PubMed]
- Özkaya Mutlu, Ö.; Egemen, O.; Dilber, A.; Üsçetin, I. Aesthetic unit- based reconstruction of periorbital defects. J Craniofac Surg 2016, 27, 429–432. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, H.M.; Jelks, G.W. Periocular reconstruction: a systematic approach. Plast Reconstr Surg 1993, 91, 1017–1024, discussion 1025–1026. [Google Scholar] [CrossRef]
- Bowman, P.H.; Fosko, S.W.; Hartstein, M.E. Periocular reconstruction. Semin Cutan Med Surg 2003, 22, 263–272. [Google Scholar]
- Cannon, P.S.; McCormick, A.; Leatherbarrow, B. The use of soft tissue expanders in periocular reconstruction: a case series. Ophthal Plast Reconstr Surg 2011, 27, 232–235. [Google Scholar]
- Imola, M.J.; Ducic, Y.; Adelson, R.T. The secondary correction of post- traumatic craniofacial deformities. Otolaryngol Head Neck Surg 2008, 139, 654–660. [Google Scholar]
- Gruss, J.S.; Whelan, M.F.; Rand, R.P.; Ellenbogen, R.G. Lessons learnt from the management of 1500 complex facial fractures. Ann Acad Med Singapore 1999, 28, 677–686. [Google Scholar]
- Cooter, R.D.; David, D.J. Computer-based coding of fractures in the craniofacial region. Br J Plast Surg 1989, 42, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Osler, T.; Baker, S.P.; Long, W. A modification of the injury severity score that both improves accuracy and simplifies scoring. J Trauma 1997, 43, 922–925, discussion 925–926. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, S.C.; Dierks, E.J.; Kademani, D.; et al. Application of a facial injury severity scale in craniomaxillofacial trauma. J Oral Maxillofac Surg 2006, 64, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, Y.; El-Maaytah, M.; Ma, L.; Liu, L.; Zhou, L.D. Maxillofacial Injury Severity Score: proposal of a new scoring system. Int J Oral Maxillofac Surg 2006, 35, 109–114. [Google Scholar] [CrossRef]
- Ahmad, Z.; Nouraei, R.; Holmes, S. Towards a classification system for complex craniofacial fractures. Br J Oral Maxillofac Surg 2012, 50, 490–494. [Google Scholar] [CrossRef]
- Sahni, V. Maxillofacial trauma scoring systems: review article. Injury 2016, 47, 1388–1392. [Google Scholar] [CrossRef]
- Cohen, M.A.; Boyes-Varley, G. Penetrating injuries to the maxillo- facial region. J Oral Maxillofac Surg 1986, 44, 197–202. [Google Scholar] [CrossRef]
- Harris, A.M.P.; Wood, R.E.; Nortjé, C.J.; Grotepass, F. Deliberately inflicted, penetrating injuries of the maxillofacial region (Jael’s syndrome). Report of 4 cases. J Craniomaxillofac Surg 1988, 16, 60–63. [Google Scholar] [CrossRef]
- Grobbelaar, A.; Knottenbelt, J.D. Retained knife blades in stab wounds of the face: is simple withdrawal safe? Injury 1991, 22, 29–31. [Google Scholar] [CrossRef]
- Thorne, C.H. Gunshot wounds to the face. Current concepts. Clin Plast Surg 1992, 19, 233–244. [Google Scholar] [CrossRef]
- Chen, A.Y.; Stewart, M.G.; Raup, G. Penetrating injuries of the face. Otolaryngol Head Neck Surg 1996, 115, 464–470. [Google Scholar] [PubMed]
- Demetriades, D.; Chahwan, S.; Gomez, H.; Falabella, A.; Velmahos, G.; Yamashita, D. Initial evaluation and management of gunshot wounds to the face. J Trauma 1998, 45, 39–41. [Google Scholar] [CrossRef]
- Hollier, L.; Grantcharova, E.P.; Kattash, M. Facial gunshot wounds: a 4-year experience. J Oral Maxillofac Surg 2001, 59, 277–282. [Google Scholar] [CrossRef]
- Motamedi, M.H. Primary management of maxillofacial hard and soft tissue gunshot and shrapnel injuries. J Oral Maxillofac Surg 2003, 61, 1390–1398. [Google Scholar] [CrossRef]
- Daya, N.P.; Liversage, H.L. Penetrating stab wound injuries to the face. SADJ 2004, 59, 55–59. [Google Scholar] [PubMed]
- McLean, J.N.; Moore, C.E.; Yellin, S.A. Gunshot wounds to the face– acute management. Facial Plast Surg 2005, 21, 191–198. [Google Scholar] [PubMed]
- Agrillo, A.; Sassano, P.; Mustazza, M.C.; Filiaci, F. Complex-type pene- trating injuries of craniomaxillofacial region. J Craniofac Surg 2006, 17, 442–446. [Google Scholar]
- Kesting, M.R.; Hölzle, F.; Pox, C.; Thurmüller, P.; Wolff, K.D. Animal bite injuries to the head: 132 cases. Br J Oral Maxillofac Surg 2006, 44, 235–239. [Google Scholar]
- Kaufman, Y.; Cole, P.; Hollier, L. Contemporary issues in facial gunshot wound management. J Craniofac Surg 2008, 19, 421–427. [Google Scholar] [CrossRef]
- Stefanopoulos, P.K. Management of facial bite wounds. Oral Maxillofac Surg Clin North Am 2009, 21, 247–257. [Google Scholar]
- Meer, M.; Siddiqi, A.; Morkel, J.A.; Janse van Rensburg, P.; Zafar, S. Knife inflicted penetrating injuries of the maxillofacial region: a descriptive, record-based study. Injury 2010, 41, 77–81. [Google Scholar]
- Yardley, A.M.; Hoskin, A.K.; Hanman, K.; Wan, S.L.; Mackey, D.A. Animal- inflicted ocular and adnexal injuries in children: a systematic review. Surv Ophthalmol 2015, 60, 536–546. [Google Scholar] [PubMed]
- Mokal, N.J.; Desai, M.F. Secondary correction of post-traumatic cra- niofacial deformities. J Craniofac Surg 2014, 25, 1658–1664. [Google Scholar]
- Simon, B.; Letourneau, P.; Vitorino, E.; McCall, J. Pediatric minor head trauma: indications for computed tomographic scanning revis- ited. J Trauma 2001, 51, 231–237, discussion 237–238. [Google Scholar] [PubMed]
- Katzen, J.T.; Jarrahy, R.; Eby, J.B.; Mathiasen, R.A.; Margulies, D.R.; Shahinian, H.K. Craniofacial and skull base trauma. J Trauma 2003, 54, 1026–1034. [Google Scholar] [PubMed]
- Ono, K.; Wada, K.; Takahara, T.; Shirotani, T. Indications for computed tomography in patients with mild head injury. Neurol Med Chir (Tokyo) 2007, 47, 291–297, discussion 297–298. [Google Scholar]
- Denny, A.D.; Bonawitz, S.C. Clostridial infection following severe facial trauma. Ann Plast Surg 1994, 33, 313–316. [Google Scholar]
- Jayamanne, D.G.; Bell, R.W.; Allen, E.D. Orbital cellulitis–an unusual presentation and late complication of severe facial trauma. Br J Oral Maxillofac Surg 1994, 32, 187–189. [Google Scholar]
- Thomas, J.R.; Frost, T.W. Immediate versus delayed repair of skin defects following resection of carcinoma. Otolaryngol Clin North Am 1993, 26, 203–213. [Google Scholar]
- Menick, F.J. Defects of the nose, lip, and cheek: rebuilding the composite defect. Plast Reconstr Surg 2007, 120, 887–898. [Google Scholar]
- Kretlow, J.D.; McKnight, A.J.; Izaddoost, S.A. Facial soft tissue trauma. Semin Plast Surg 2010, 24, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Berthe, J.V.; Pelc, P.; Jortay, A.; Coessens, B.C. Do multiple consecutive head and neck reconstructions improve the patients functional outcome? Acta Otorhinolaryngol Belg 2002, 56, 391–397. [Google Scholar] [PubMed]
- Elbarbary, A.S.; Ali, A. Medial canthopexy of old unrepaired naso- orbito-ethmoidal (noe) traumatic telecanthus. J Craniomaxillofac Surg 2014, 42, 106–112. [Google Scholar]
- Becelli, R.; Renzi, G.; Mannino, G.; Cerulli, G.; Iannetti, G. Posttraumatic obstruction of lacrimal pathways: a retrospective analysis of 58 consecutive naso-orbitoethmoid fractures. J Craniofac Surg 2004, 15, 29–33. [Google Scholar] [PubMed]
- Kelly, C.P.; Cohen, A.J.; Yavuzer, R.; Moreira-Gonzalez, A.; Jackson, I.T. Medial canthopexy: a proven technique. Ophthal Plast Reconstr Surg 2004, 20, 337–341. [Google Scholar]
- Reifler, D.M. Management of canalicular laceration. Surv Ophthalmol 1991, 36, 113–132. [Google Scholar]
- Evans, G.R.; Daniels, M.; Hewell, L. An evidence-based approach to zygomatic fractures. Plast Reconstr Surg 2011, 127, 891–897. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
 |
 |
 |
 |
 |
 |
 |
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2019 by the author. The Author(s) 2019.
Share and Cite
Sadek, E.Y.; Elbarbary, A.; Safe, I.I. Periorbital Trauma: A New Classification. Craniomaxillofac. Trauma Reconstr. 2019, 12, 228-240. https://doi.org/10.1055/s-0039-1677808
Sadek EY, Elbarbary A, Safe II. Periorbital Trauma: A New Classification. Craniomaxillofacial Trauma & Reconstruction. 2019; 12(3):228-240. https://doi.org/10.1055/s-0039-1677808
Chicago/Turabian StyleSadek, Eman Yahya, Amir Elbarbary, and Ikram I. Safe. 2019. "Periorbital Trauma: A New Classification" Craniomaxillofacial Trauma & Reconstruction 12, no. 3: 228-240. https://doi.org/10.1055/s-0039-1677808
APA StyleSadek, E. Y., Elbarbary, A., & Safe, I. I. (2019). Periorbital Trauma: A New Classification. Craniomaxillofacial Trauma & Reconstruction, 12(3), 228-240. https://doi.org/10.1055/s-0039-1677808