

Similar Patterns of Dysautonomia in Myalgic Encephalomyelitis/Chronic Fatigue and Post-COVID-19 Syndromes

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Symptom Assessment Tools
2.2.2. Assessment of Autonomic Nervous System Function
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of Participants
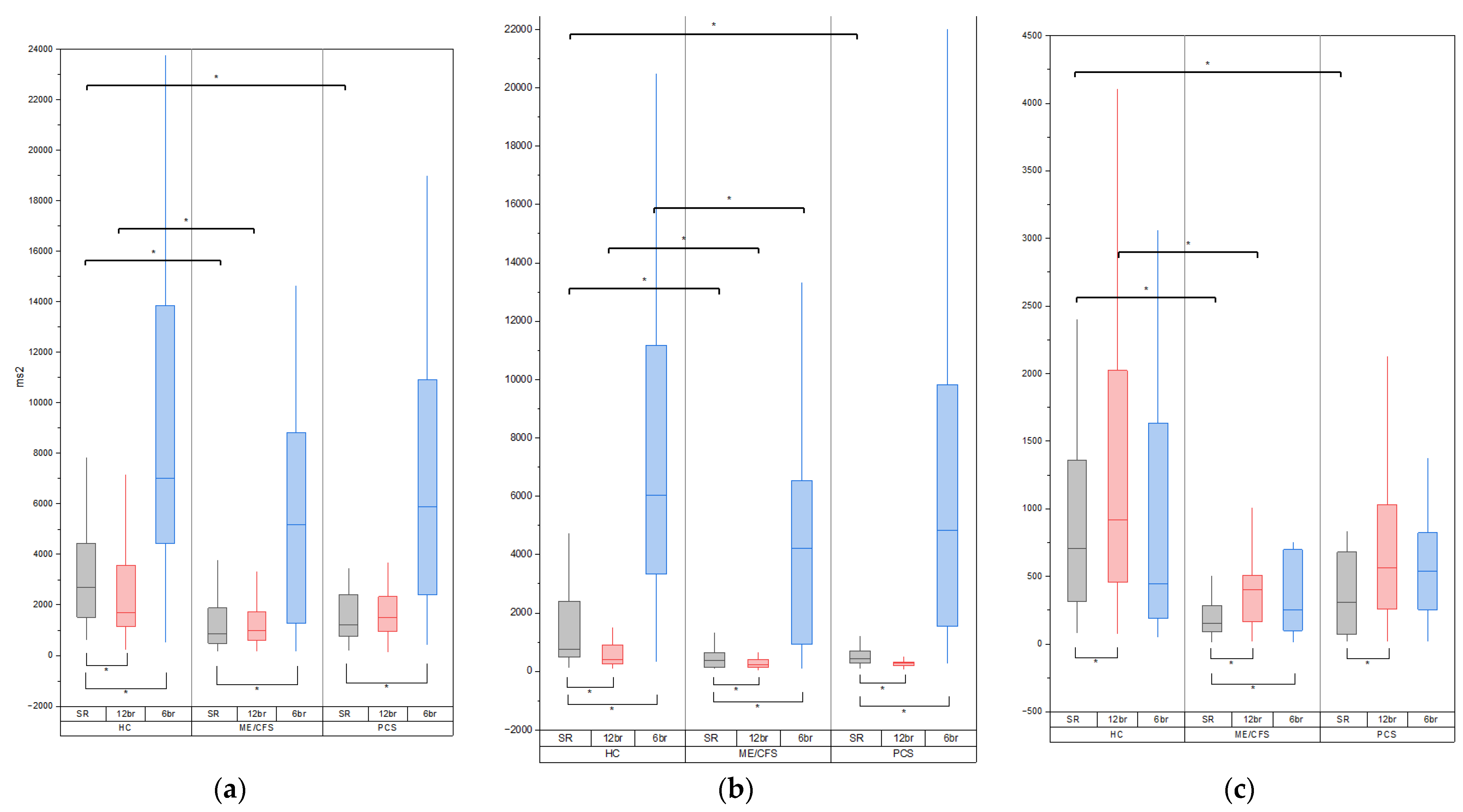
3.2. Baseline Variability Indices
3.3. Variability Indices during Breathing at 12 Breaths per Minute
3.4. Variability Indices during Breathing at 6 Breaths per Minute
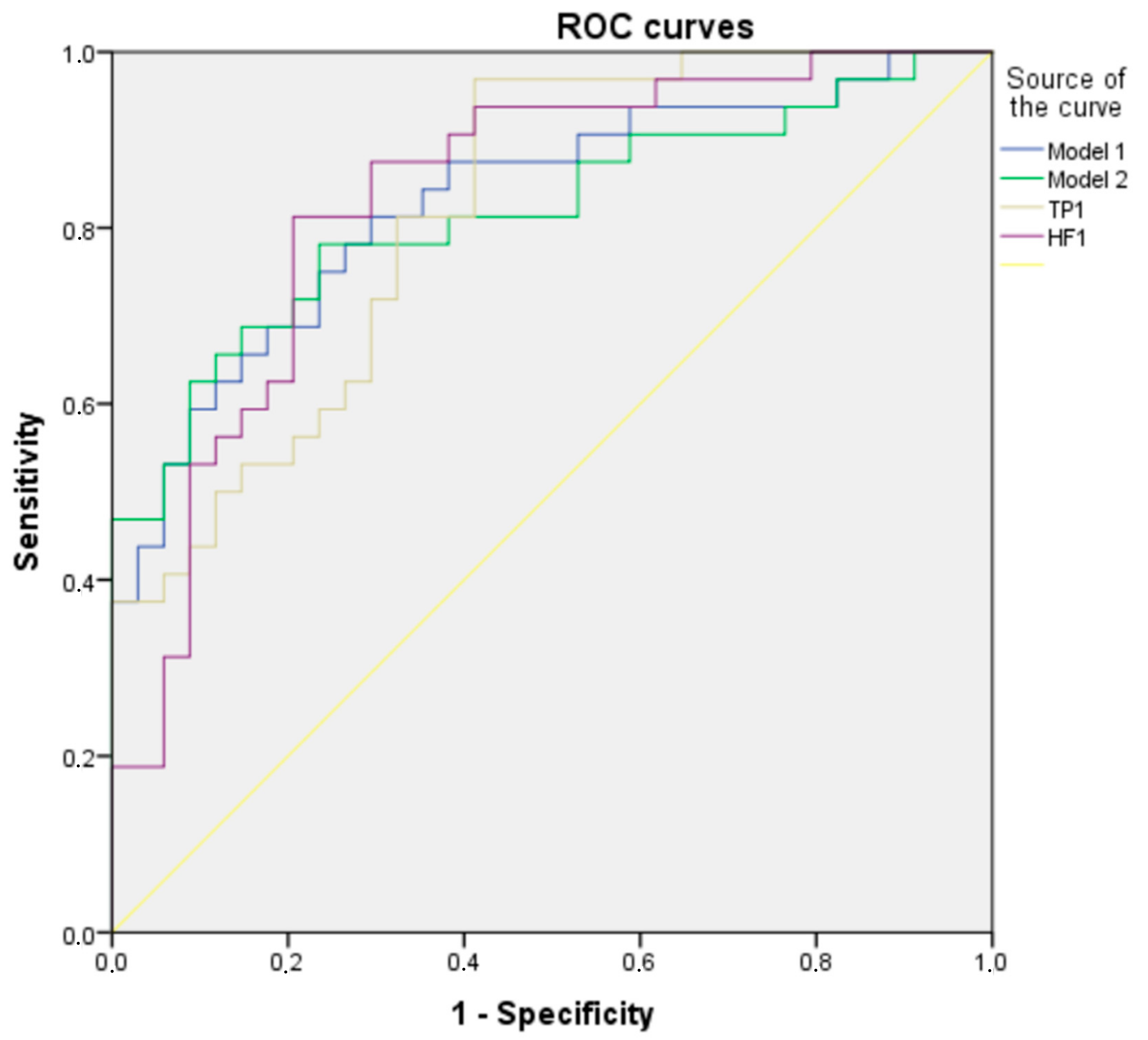
3.5. Multifactorial Logistic Regression Analysis of ME/CFS Group
3.6. Correlations between Heart Rate and Arterial Blood Pressure Variability Parameters and Clinical Characteristics in Patient Groups
3.7. Baroreflex Sensitivity and Baroreflex Effectiveness Index
4. Discussion
4.1. Clinical Characteristics of the Patients with ME/CFS and PCC
4.2. HRV and BPV in Patients with ME/CFS and PCC
4.3. Correlation Analysis of HRV and BPV Indices with Clinical Features of the Patients
4.4. Baroreflex Sensitivity in Patients
4.5. Mechanisms of Dysautonomia in ME/CFS and PCC and a Potential Link with Cardiovascular Diseases
5. Limitations and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Chu, L.; Valencia, I.J.; Garvert, D.W.; Montoya, J.G. Onset patterns and course of myalgic encephalomyelitis/chronic fatigue syndrome. Front. Pediatr. 2019, 7, 427132. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Dorri, J.A. ME/CFS and Post-Exertional Malaise among Patients with Long COVID. Neurol. Int. 2023, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Tate, W.P.; Walker, M.O.M.; Peppercorn, K.; Blair, A.L.H.; Edgar, C.D. Towards a Better Understanding of the Complexities of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Long COVID. Int. J. Mol. Sci. 2023, 24, 5124. [Google Scholar] [CrossRef] [PubMed]
- van Campen, C.L.M.C.; Visser, F.C. Orthostatic Intolerance in Long-Haul COVID after SARS-CoV-2: A Case-Control Comparison with Post-EBV and Insidious-Onset Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Patients. Healthcare 2022, 10, 2058. [Google Scholar] [CrossRef]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet. Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- Komaroff, A.L.; Lipkin, W.I. ME/CFS and Long COVID share similar symptoms and biological abnormalities: Road map to the literature. Front. Med. 2023, 10, 1187163. [Google Scholar] [CrossRef]
- Macarova, J.A.; Malakhova, S.A.; Novitskaya, T.A.; Shapkina, V.A.; Churilov, L.P. COVID-19 and Vasa vasorum: New Atherogenic Factor? A Case Report and Autopsy Findings. Diagnostics 2023, 13, 1097. [Google Scholar] [CrossRef]
- Nunes, J.M.; Kell, D.B.; Pretorius, E. Cardiovascular and haematological pathology in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): A role for viruses. Blood Rev. 2023, 60, 101075. [Google Scholar] [CrossRef]
- Shafiq, M.A.; Ellingson, C.A.; Krätzig, G.P.; Dorsch, K.D.; Neary, J.P.; Singh, J. Differences in Heart Rate Variability and Baroreflex Sensitivity between Male and Female Athletes. J. Clin. Med. 2023, 12, 3916. [Google Scholar] [CrossRef]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef]
- Carruthers, B.M.; Jain, A.K.; De Meirleir, K.L.; Peterson, D.L.; Klimas, N.G.; Lerner, A.M.; Bested, A.C.; Flor-Henry, P.; Joshi, P.; Powles, A.C.P.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Chronic Fatigue Syndr. 2003, 11, 7–115. [Google Scholar] [CrossRef]
- IOM (Institute of Medicine). Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Nacul, L.; Jérôme Authier, F.; Scheibenbogen, C.; Lorusso, L.; Bergliot Helland, I.; Alegre Martin, J.; Adella Sirbu, C.; Marit Mengshoel, A.; Polo, O.; Behrends, U.; et al. European Network on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (EUROMENE): Expert Consensus on the Diagnosis, Service Provision, and Care of People with ME/CFS in Europe. Medicina 2021, 57, 510. [Google Scholar] [CrossRef] [PubMed]
- Smets, E.M.A.; Garssen, B.; Bonke, B.; De Haes, J.C.J.M. The multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J. Psychosom. Res. 1995, 39, 315–325. [Google Scholar] [CrossRef]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Pivovarov, V. Information-measuring system for functionaldiagnostics of nervous regulation of blood circulation. Part II.The implementation. Autom. Remote Control 2011, 72, 671–676. [Google Scholar] [CrossRef]
- Di Rienzo, M.; Parati, G.; Castiglioni, P.; Tordi, R.; Mancia, G.; Pedotti, A. Baroreflex effectiveness index: An additional measure of baroreflex control of heart rate in daily life. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2001, 280, R744–R751. [Google Scholar] [CrossRef] [PubMed]
- Pohlert, T. PMCMRplus: Calculate Pairwise Multiple Comparisons of Mean Rank Sums Extended. R Package Version 1.9.10. Available online: https://cran.r-project.org/package=PMCMRplus (accessed on 10 November 2023).
- Twomey, R.; Demars, J.; Franklin, K.; Nicole Culos-Reed, S.; Weatherald, J.; Wrightson, J.G. Chronic Fatigue and Postexertional Malaise in People Living With Long COVID: An Observational Study. Phys. Ther. 2022, 102, pzac005. [Google Scholar] [CrossRef]
- Hayano, J.; Yuda, E. Pitfalls of assessment of autonomic function by heart rate variability. J. Physiol. Anthropol. 2019, 38, 3. [Google Scholar] [CrossRef]
- Russo, M.A.; Santarelli, D.M.; O’Rourke, D. The physiological effects of slow breathing in the healthy human. Breathe 2017, 13, 298–309. [Google Scholar] [CrossRef]
- Skytioti, M.; Elstad, M. Respiratory Sinus Arrhythmia is Mainly Driven by Central Feedforward Mechanisms in Healthy Humans. Front. Physiol. 2022, 13, 768465. [Google Scholar] [CrossRef]
- Saboul, D.; Pialoux, V.; Hautier, C. The breathing effect of the LF/HF ratio in the heart rate variability measurements of athletes. Eur. J. Sport Sci. 2014, 14, S282–S288. [Google Scholar] [CrossRef]
- Zaccaro, A.; Piarulli, A.; Laurino, M.; Garbella, E.; Menicucci, D.; Neri, B.; Gemignani, A. How Breath-Control Can Change Your Life: A Systematic Review on Psycho-Physiological Correlates of Slow Breathing. Front. Hum. Neurosci. 2018, 12, 353. [Google Scholar] [CrossRef]
- Frith, J.; Zalewski, P.; Klawe, J.J.; Pairman, J.; Bitner, A.; Tafil-Klawe, M.; Newton, J.L. Impaired blood pressure variability in chronic fatigue syndrome—A potential biomarker. QJM Int. J. Med. 2012, 105, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Escorihuela, R.M.; Capdevila, L.; Castro, J.R.; Zaragozà, M.C.; Maurel, S.; Alegre, J.; Castro-Marrero, J. Reduced heart rate variability predicts fatigue severity in individuals with chronic fatigue syndrome/myalgic encephalomyelitis. J. Transl. Med. 2020, 18, 4. [Google Scholar] [CrossRef] [PubMed]
- Boissoneault, J.; Letzen, J.; Robinson, M.; Staud, R. Cerebral blood flow and heart rate variability predict fatigue severity in patients with chronic fatigue syndrome. Brain Imaging Behav. 2019, 13, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Reyes del Paso, G.A.; Contreras-Merino, A.M.; de la Coba, P.; Duschek, S. The cardiac, vasomotor, and myocardial branches of the baroreflex in fibromyalgia: Associations with pain, affective impairments, sleep problems, and fatigue. Psychophysiology 2021, 58, e13800. [Google Scholar] [CrossRef]
- Mueller, B.R.; Ray, C.; Benitez, A.; Robinson-Papp, J. Reduced cardiovagal baroreflex sensitivity is associated with postural orthostatic tachycardia syndrome (POTS) and pain chronification in patients with headache. Front. Hum. Neurosci. 2023, 17, 1068410. [Google Scholar] [CrossRef]
- Skow, R.J.; Garza, N.A.; Nandadeva, D.; Stephens, B.Y.; Wright, A.N.; Grotle, A.K.; Young, B.E.; Fadel, P.J. Impact of COVID-19 on cardiac autonomic function in healthy young adults: Potential role of symptomatology and time since diagnosis. Am. J. Physiol. Heart Circ. Physiol. 2022, 323, H1206–H1211. [Google Scholar] [CrossRef]
- Brognara, F.; Castania, J.A.; Kanashiro, A.; Dias, D.P.M.; Salgado, H.C. Physiological Sympathetic Activation Reduces Systemic Inflammation: Role of Baroreflex and Chemoreflex. Front. Immunol. 2021, 12, 637845. [Google Scholar] [CrossRef]
- Amorim, M.R.; de Deus, J.L.; Pereira, C.A.; da Silva, L.E.V.; Borges, G.S.; Ferreira, N.S.; Batalhão, M.E.; Antunes-Rodrigues, J.; Carnio, E.C.; Tostes, R.C.; et al. Baroreceptor denervation reduces inflammatory status but worsens cardiovascular collapse during systemic inflammation. Sci. Rep. 2020, 10, 6990. [Google Scholar] [CrossRef] [PubMed]
- Al-kuraishy, H.M.; Al-Gareeb, A.I.; Qusti, S.; Alshammari, E.M.; Gyebi, G.A.; Batiha, G.E.S. COVID-19-Induced Dysautonomia: A Menace of Sympathetic Storm. ASN Neuro 2021, 13, 17590914211057635. [Google Scholar] [CrossRef] [PubMed]
- Azcue, N.; Del Pino, R.; Acera, M.; Fernández-Valle, T.; Ayo-Mentxakatorre, N.; Pérez-Concha, T.; Murueta-Goyena, A.; Lafuente, J.V.; Prada, A.; López de Munain, A.; et al. Dysautonomia and small fiber neuropathy in post-COVID condition and Chronic Fatigue Syndrome. J. Transl. Med. 2023, 21, 814. [Google Scholar] [CrossRef]
- Wirth, K.J.; Löhn, M. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and Comorbidities: Linked by Vascular Pathomechanisms and Vasoactive Mediators? Medicina 2023, 59, 978. [Google Scholar] [CrossRef] [PubMed]
- Braga, J.; Lepra, M.; Kish, S.J.; Rusjan, P.M.; Nasser, Z.; Verhoeff, N.; Vasdev, N.; Bagby, M.; Boileau, I.; Husain, M.I.; et al. Neuroinflammation after COVID-19 with Persistent Depressive and Cognitive Symptoms. JAMA Psychiatry 2023, 80, 787–795. [Google Scholar] [CrossRef]
- Wang, M.; Pan, W.; Xu, Y.; Zhang, J.; Wan, J.; Jiang, H. Microglia-Mediated Neuroinflammation: A Potential Target for the Treatment of Cardiovascular Diseases. J. Inflamm. Res. 2022, 15, 3083–3094. [Google Scholar] [CrossRef]
- Ziegler, M.G. Atherosclerosis and Blood Pressure Variability. Hypertension 2018, 71, 403–405. [Google Scholar] [CrossRef]
- Zambach, C.; Fedorowski, A.; Gerward, S.; Johansson, M.; Engström, G.; Hamrefors, V. Subclinical atherosclerosis and risk factors in relation to autonomic indices in the general population. J. Hypertens. 2023, 41, 759–767. [Google Scholar] [CrossRef]
- Takahashi, M.; Miyai, N.; Nagano, S.; Utsumi, M.; Oka, M.; Yamamoto, M.; Shiba, M.; Uematsu, Y.; Nishimura, Y.; Takeshita, T.; et al. Orthostatic Blood Pressure Changes and Subclinical Markers of Atherosclerosis. Am. J. Hypertens. 2015, 28, 1134–1140. [Google Scholar] [CrossRef]
- Sheng, Y.; Zhu, L. The crosstalk between autonomic nervous system and blood vessels. Int. J. Physiol. Pathophysiol. Pharmacol. 2018, 10, 17. [Google Scholar]
- Chistiakov, D.A.; Ashwell, K.W.; Orekhov, A.N.; Bobryshev, Y.V. Innervation of the arterial wall and its modification in atherosclerosis. Auton. Neurosci. 2015, 193, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Giunta, S.; Xia, S.; Pelliccioni, G.; Olivieri, F. Autonomic nervous system imbalance during aging contributes to impair endogenous anti-inflammaging strategies. GeroScience 2023. [Google Scholar] [CrossRef] [PubMed]
- Rivera, M.C.; Mastronardi, C.; Silva-Aldana, C.T.; Arcos-Burgos, M.; Lidbury, B.A. Myalgic encephalomyelitis/chronic fatigue syndrome: A comprehensive review. Diagnostics 2019, 9, 91. [Google Scholar] [CrossRef] [PubMed]
- Simula, S.; Vanninen, E.; Lehto, S.; Hedman, A.; Pajunen, P.; Syvänne, M.; Hartikainen, J. Heart rate variability associates with asymptomatic coronary atherosclerosis. Clin. Auton. Res. 2014, 24, 31–37. [Google Scholar] [CrossRef]
- Huikuri, H.V.; Jokinen, V.; Syvänne, M.; Nieminen, M.S.; Airaksinen, K.E.J.; Ikäheimo, M.J.; Koistinen, J.M.; Kauma, H.; Kesäniemi, A.Y.; Majahalme, S.; et al. Heart Rate Variability and Progression of Coronary Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 1999, 19, 1979–1985. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | ME/CFS | PCC | HC | p-Value of Kruskal– Wallis Test | p-Value of Dunn Test ME/CFS vs. HC | p-Value of Dunn Test PCC vs. HC |
|---|---|---|---|---|---|---|
| Age (years) | 35.00 (30.0–41.25) | 35.00 (29.50–41.50) | 34.50 (21.25–43.75) | 0.302 | N/A | N/A |
| BMI (kg/m2) | 23.41 (19.45–28.70) | 23.51 (20.54–27.86) | 22.07 (20.14–25.41) | 0.649 | N/A | N/A |
| Gender | ||||||
| Male | 8 (23.53%) | 6 (20.69%) | 10 (31.25%) | 0.612 * | N/A | N/A |
| Female | 26 (76.47%) | 23 (79.31%) | 22 (68.75%) | |||
| HADS | ||||||
| Anxiety | 10.00 (5.75–12.00) | 10.00 (6.00–12.00) | 6.00 (2.00–8.00) | 0.000 | 0.001 | 0.001 |
| Depression | 10.00 (7.75–11.25) | 9.00 (6.00–10.00) | 3.00 (1.25–4.00) | 0.000 | 0.000 | 0.000 |
| MFI-20 | ||||||
| General fatigue | 19.00 (17.75–20.00) | 18.00 (14.50–20.00) | 8.00 (5.25–9.75) | 0.000 | 0.000 | 0.000 |
| Physical fatigue | 17.50 (15.00–19.00) | 16.00 (14.00–18.00) | 7.00 (5.00–9.75) | 0.000 | 0.000 | 0.000 |
| Reduced activity | 18.00 (16.00–19.00) | 16.00 (12.5–19.00) | 7.50 (4.25–11.00) | 0.000 | 0.000 | 0.000 |
| Reduced motivation | 13.50 (11.00–16.00) | 12.00 (9.50–15.00) | 8.00 (6.00–9.00) | 0.000 | 0.000 | 0.000 |
| Mental fatigue | 16.50 (15.00–18.00) | 13.00 (11.00–16.00) | 6.00 (4.00–9.00) | 0.000 | 0.000 | 0.000 |
| IPAQ | ||||||
| Total score IPAQ (MET-min/Week) | 1857.00 (590.25–2841.00) | 1506.00 (1039.50–2814.00) | 3027.00 (1606.50–5399.00) | 0.007 | 0.004 | 0.010 |
| Variable | ME/CFS | PCC | HC | p-Value of Kruskal– Wallis Test | p-Value of Dunn Test ME/CFS vs. HC | p-Value of Dunn Test PCC vs. HC |
|---|---|---|---|---|---|---|
| Heart rate variability | ||||||
| TP (ms2) | 852.45 (469.03–1912.88) | 1358.10 (834.15–2687.15) | 2709.05 (1483.38–4454.36) | 0.000 | 0.000 | 0.003 |
| LF (ms2) | 367.10 (137.45–635.13) | 429.20 (279.65–867.70) | 759.30 (477.33–2480.68) | 0.000 | 0.000 | 0.013 |
| HF (ms2) | 152.90 (91.93–284.78) | 335.00 (102.45–717.10) | 703.70 (311.00–1394.80) | 0.000 | 0.000 | 0.006 |
| VLF (ms2) | 256.15 (192.03–619.38) | 469.20 (237.10–814.60) | 727.50 (431.85–1014.80) | 0.000 | 0.000 | 0.027 |
| LF/HF | 2.14 (1.20–4.13) | 1.46 (1.02–4.01) | 1.25 (0.71–2.31) | 0.080 | N/A | N/A |
| Beat-to-beat systolic arterial blood pressure variability | ||||||
| TP (mmHg2) | 50.15 (23.38–66.78) | 42.20 (26.85–65.80) | 41.35 (22.15–63.15) | 0.763 | N/A | N/A |
| LF (mmHg2) | 13.95 (6.45–21.85) | 13.50 (8.80–23.30) | 9.50 (6.30–19.68) | 0.550 | N/A | N/A |
| HF (mmHg2ms2) | 7.80 (4.38–16.73) | 8.40 (3.60–11.45) | 8.50 (4.48–14.28) | 0.987 | N/A | N/A |
| VLF (mmHg2ms2) | 20.30 (10.08–31.83) | 17.50 (7.80–29.60) | 12.90 (5.63–33.60) | 0.388 | N/A | N/A |
| LF/HF | 1.63 (0.77–2.43) | 1.79 (1.20–2.92) | 1.11 (0.65–2.85) | 0.314 | N/A | N/A |
| Beat-to-beat diastolic arterial blood pressure variability | ||||||
| TP (mmHg2ms2) | 12.95 (7.38–25.28) | 12.80 (8.05–25.35) | 11.75 (7.60–20.53) | 0.738 | N/A | N/A |
| LF (mmHg2ms2) | 5.15 (2.93–7.98) | 5.30 (3.15–8.70) | 4.45 (2.25–7.90) | 0.882 | N/A | N/A |
| HF (mmHg2ms2) | 1.50 (0.90–2.15) | 1.10 (0.70–2.50) | 1.45 (0.70–2.68) | 0.945 | N/A | N/A |
| VLF (mmHg2ms2) | 5.75 (3.03–12.15) | 6.20 (2.80–13.15) | 4.45 (2.83–13.48) | 0.882 | N/A | N/A |
| LF/HF | 3.39 (1.84–5.53) | 3.91 (2.35–6.83) | 3.02 (2.17–5.74) | 0.885 | N/A | N/A |
| Variable | ME/CFS | PCC | HC | p-Value of Kruskal–Wallis Test | p-Value of Dunn Test ME/CFS vs. HC | p-Value of Dunn Test PCC vs. HC |
|---|---|---|---|---|---|---|
| Heart rate variability at 12 breaths/min | ||||||
| TP (ms2) | 998.90 (573.93–1729.15) | 1506.80 (948.90–2410.35) | 1682.35 (1120.95–3607.90) | 0.002 | 0.000 | 0.108 |
| LF (ms2) | 226.55 (140.28–399.68) | 272.60 (198.90–329.50) | 402.7 (237.35–908.75) | 0.005 | 0.002 | 0.023 |
| HF (ms2) | 399.15 (162.38–529.75) | 564.50 (253.85–1095.35) | 920.45 (439.75–2023.70) | 0.001 | 0.0021 | 0.050 |
| Beat-to-beat systolic arterial blood pressure variability at 12 breaths/min | ||||||
| TP (mmHg2ms2) | 49.30 (24.85–65.45) | 42.40 (26.00–97.60) | 33.00 (18.85–49.18) | 0.223 | N/A | N/A |
| LF (mmHg2) | 11.90 (5.93–21.33) | 9.60 (4.75–23.10) | 5.75 (3.70–10.85) | 0.018 | 0.009 | 0.023 |
| HF (mmHg2ms2) | 14.74 (6.08–32.05) | 12.80 (6.40–35.80) | 13.80 (8.38–22.50) | 0.972 | N/A | N/A |
| Beat-to-beat diastolic arterial blood pressure variability at 12 breaths/min | ||||||
| TP (mmHg2ms2) | 12.35 (7.48–22.78) | 13.90 (7.15–20.60) | 9.35 (4.63–14.55) | 0.071 | N/A | N/A |
| LF (mmHg2ms2) | 4.10 (2.13–6.90) | 4.10 (1.85–8.15) | 2.70 (1.73–4.70) | 0.158 | N/A | N/A |
| HF (mmHg2) | 3.35 (1.45–5.83) | 2.60 (1.00–6.40) | 1.45 (0.93–3.15) | 0.041 | 0.013 | 0.095 |
| Heart rate variability at 6 breaths/min | ||||||
| TP (ms2) | 5179.75 (1260.90–8857.20) | 5891.10 (2363.10–11,520.45) | 7007.30 (4443.65–14,608.75) | 0.061 | N/A | N/A |
| LF (ms2) | 4220.15 (921.70–6590.25) | 4824.30 (1528.40–9957.70) | 6022.40 (3333.65–11,796.05) | 0.034 | 0.009 | 0.126 |
| HF (ms2) | 249.90 (98.28–698.98) | 536.10 (231.55–1099.25) | 442.90 (183.50–1643.08) | 0.093 | N/A | N/A |
| Beat-to-beat systolic arterial blood pressure variability at 6 breaths/min | ||||||
| TP (mmHg2ms2) | 77.20 (43.58–136.63) | 84.40 (48.90–157.35) | 62.90 (39.38–96.05) | 0.258 | N/A | N/A |
| LF (mmHg2ms2) | 53.60 (22.05–106.18) | 57.70 (27.30–122.60) | 39.25 (22.23–69.70) | 0.166 | N/A | N/A |
| HF (mmHg2ms2) | 5.35 (2.80–10.85) | 5.20 (2.65–8.95) | 3.15 (1.93–6.23) | 0.058 | N/A | N/A |
| Beat-to-beat diastolic arterial blood pressure variability at 6 breaths/min | ||||||
| TP (mmHg2ms2) | 21.15 (11.45–39.48) | 17.90 (12.70–35.20) | 15.30 (10.45–27.23) | 0.525 | N/A | N/A |
| LF (mmHg2ms2) | 14.25 (5.23–26.93) | 12.60 (6.35–27.00) | 9.40 (5.05–20.80) | 0.463 | N/A | N/A |
| HF (mmHg2ms2) | 1.70 (1.10–2.53) | 2.10 (1.40–3.80) | 1.10 (0.70–3.38) | 0.142 | N/A | N/A |
| Variable | Adj. B | Adj. OR (95% CI) | p Value |
|---|---|---|---|
| Model 1 | |||
| TP of HRV during spontaneous breathing | −0.001 | 0.999 (0.999–1.002) | 0.001 * |
| TP of RV during spontaneous breathing | 0.002 | 1.002 (1.000–1.004) | 0.044 * |
| Hosmer Lemeshow test, p-value = 0.952; constant = 0.504 | |||
| Model 2 | |||
| LF of HRV during spontaneous breathing | −0.001 | 0.999 (0.998–1.000) | 0.012 * |
| HF of HRV at 12 breaths/min | −0.001 | 0.999 (0.998–1.000) | 0.047 * |
| TP of RV during spontaneous breathing | 0.002 | 1.002 (1.000–1.003) | 0.088 |
| Hosmer Lemeshow test, p-value = 0.730; constant = 0.562 | |||
| Variable | TP of HRV at SR | HF of HRV at SR | Model 1 | Model 2 |
|---|---|---|---|---|
| AUC (95% CI) | 0.819 (0.720–0.918) | 0.834 (0.735–0.933) | 0.830 (0.730–0.929) | 0.817 (0.712–0.922) |
| Cut-off (maximum Youden’s index) | 1047.95 | 286.95 | 0.580 | 0.496 |
| Sensitivity %, (95% CI) | 96.9% | 81.3% | 73.5% | 85.3% |
| Specificity %, (95% CI) | 58.8% | 79.4% | 75% | 68.8% |
| Cut-off (Se = Sp) | 1587.55 | 296.95 | 0.603 | 0.612 |
| Sensitivity %, (95% CI) | 71.9% | 78.1% | 70.6% | 76.5% |
| Specificity %, (95% CI) | 70.6% | 79.4% | 81.3% | 75% |
| Age | BMI | HADS-D | HADS-A | GF | PF | RA | RM | MF | Total IPAQ Score | |
|---|---|---|---|---|---|---|---|---|---|---|
| Spontaneous respiration | ||||||||||
| HC | ||||||||||
| − * | ||||||||||
| ME/CFS | ||||||||||
| LFHR | −0.462 | |||||||||
| PCC | ||||||||||
| LFHR | −0.477 | |||||||||
| Breathing at 12 breaths per minute | ||||||||||
| HC | ||||||||||
| − * | ||||||||||
| ME/CFS | ||||||||||
| HFSBP | −0.442 | |||||||||
| TPHR | −0.444 | |||||||||
| HFHR | −0.522 | |||||||||
| PCC | ||||||||||
| HFDBP | −0.497 | |||||||||
| LFSBP | 0.492 | |||||||||
| Breathing at 6 breaths per minute | ||||||||||
| HC | ||||||||||
| LFSBP | 0.465 | |||||||||
| ME/CFS | ||||||||||
| TPSBP | 0.441 | |||||||||
| LFSBP | 0.452 | 0.443 | ||||||||
| TPHR | −0.452 | |||||||||
| LFHR | −0.486 | |||||||||
| TPDBP | 0.513 | |||||||||
| LFDBP | 0.601 | |||||||||
| PCC | ||||||||||
| TPHR | −0.523 | |||||||||
| LFHR | −0.547 | |||||||||
| HFHR | −0.584 | |||||||||
| Variable | ME/CFS | PCC | HC | p-Value ME/CFS vs. HC | p-Value PCC vs. HC | |
|---|---|---|---|---|---|---|
| BRSup | 4.42 (2.88–6.28) | 5.91 (3.54–7.92) | 7.40 (4.90–14.03) | 0.001 | 0.000 | 0.065 |
| BRSdown | 4.85 (2.93–7.42) | 5.24 (3.97–8.48) | 9.15 (6.42–12.01) | 0.000 | 0.000 | 0.003 |
| BRSmean | 4.60 (3.12–6.40) | 5.99 (3.88–8.48) | 8.45 (5.25–13.40) | 0.001 | 0.000 | 0.024 |
| BEI_up | 0.57 (0.43–0.80) | 0.64 (0.44–0.78) | 0.70 (0.56–0.88) | 0.045 | 0.020 | 0.064 |
| BEI_down | 0.45 (0.37–0.62) | 0.44 (0.29–0.77) | 0.49 (0.36–0.82) | 0.680 | N/A | N/A |
| BR_up | 16.00 (7.50–25.00) | 18.00 (10.00–27.50) | 18.50 (9.25–29.00) | 0.597 | N/A | N/A |
| BR_down | 19.00 (9.00–25.75) | 12.00 (6.00–24.00) | 19.5 (7.00–32.75) | 0.346 | N/A | N/A |
| BRX_up | 10.5 (4.75–18.00) | 9.00 (5.50–14.00) | 5.50 (2.00–9.00) | 0.014 | 0.007 | 0.023 |
| BRX_down | 18.5 (9.00–25.00) | 14.00 (5.00–23.00) | 16.00 (5.00–21.50) | 0.338 | N/A | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryabkova, V.A.; Rubinskiy, A.V.; Marchenko, V.N.; Trofimov, V.I.; Churilov, L.P. Similar Patterns of Dysautonomia in Myalgic Encephalomyelitis/Chronic Fatigue and Post-COVID-19 Syndromes. Pathophysiology 2024, 31, 1-17. https://doi.org/10.3390/pathophysiology31010001
Ryabkova VA, Rubinskiy AV, Marchenko VN, Trofimov VI, Churilov LP. Similar Patterns of Dysautonomia in Myalgic Encephalomyelitis/Chronic Fatigue and Post-COVID-19 Syndromes. Pathophysiology. 2024; 31(1):1-17. https://doi.org/10.3390/pathophysiology31010001
Chicago/Turabian StyleRyabkova, Varvara A., Artemiy V. Rubinskiy, Valeriy N. Marchenko, Vasiliy I. Trofimov, and Leonid P. Churilov. 2024. "Similar Patterns of Dysautonomia in Myalgic Encephalomyelitis/Chronic Fatigue and Post-COVID-19 Syndromes" Pathophysiology 31, no. 1: 1-17. https://doi.org/10.3390/pathophysiology31010001
APA StyleRyabkova, V. A., Rubinskiy, A. V., Marchenko, V. N., Trofimov, V. I., & Churilov, L. P. (2024). Similar Patterns of Dysautonomia in Myalgic Encephalomyelitis/Chronic Fatigue and Post-COVID-19 Syndromes. Pathophysiology, 31(1), 1-17. https://doi.org/10.3390/pathophysiology31010001