
Elevated IgG and IgM Autoantibodies to Advanced Glycation End Products of Vascular Elastin in Hypertensive Patients with Type 2 Diabetes: Relevance to Disease Initiation and Progression



Abstract
:1. Introduction
2. Materials and Methods
2.1. Screening of the Patients and Controls
2.2. Immunological and Biochemical Assays
2.2.1. Determination of Anti-AGE EL IgM and Anti-AGE EL IgG Antibodies
2.2.2. Determination of MMP-2 and MMP-9
2.2.3. Biochemical Analysis
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
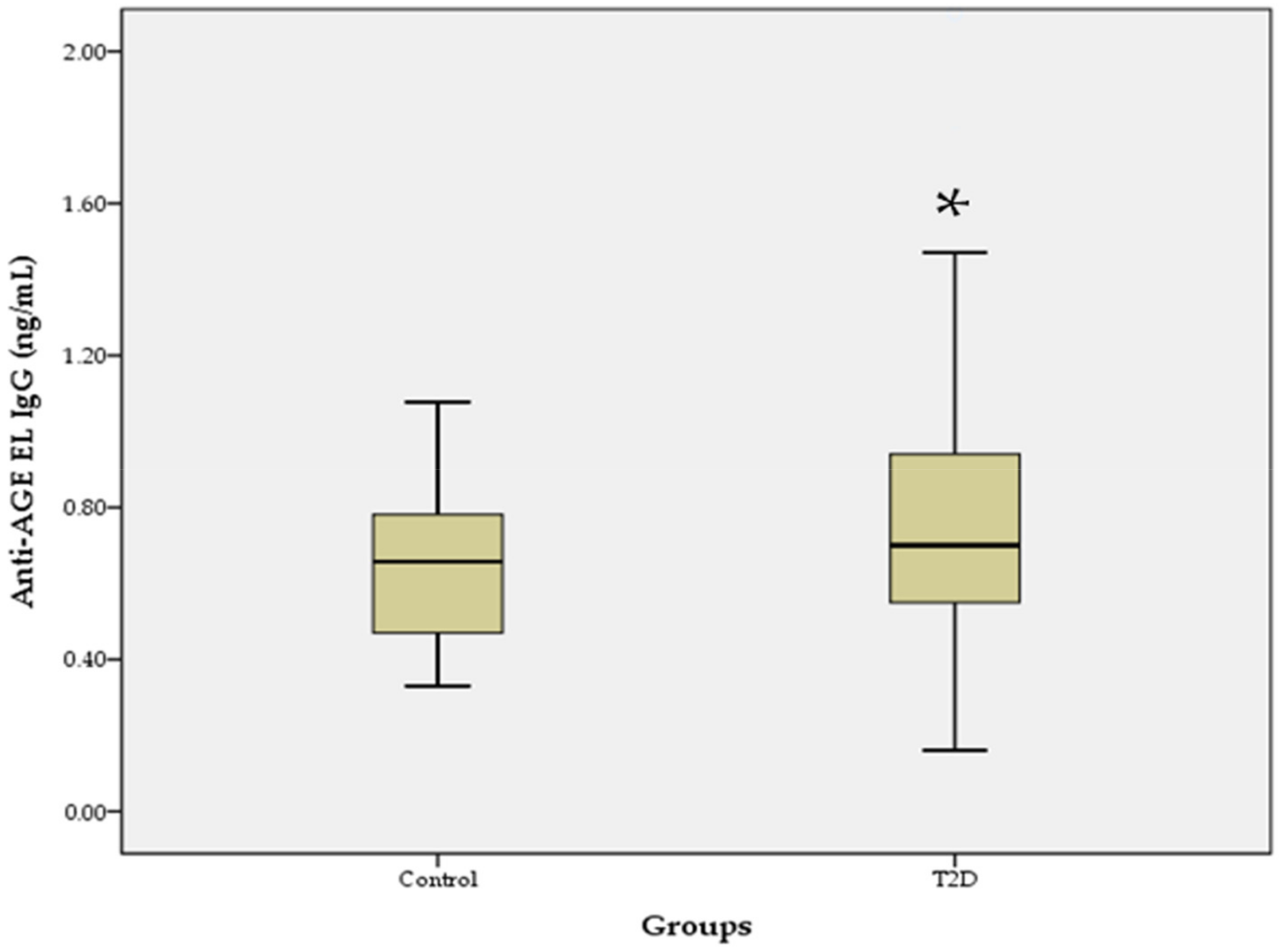
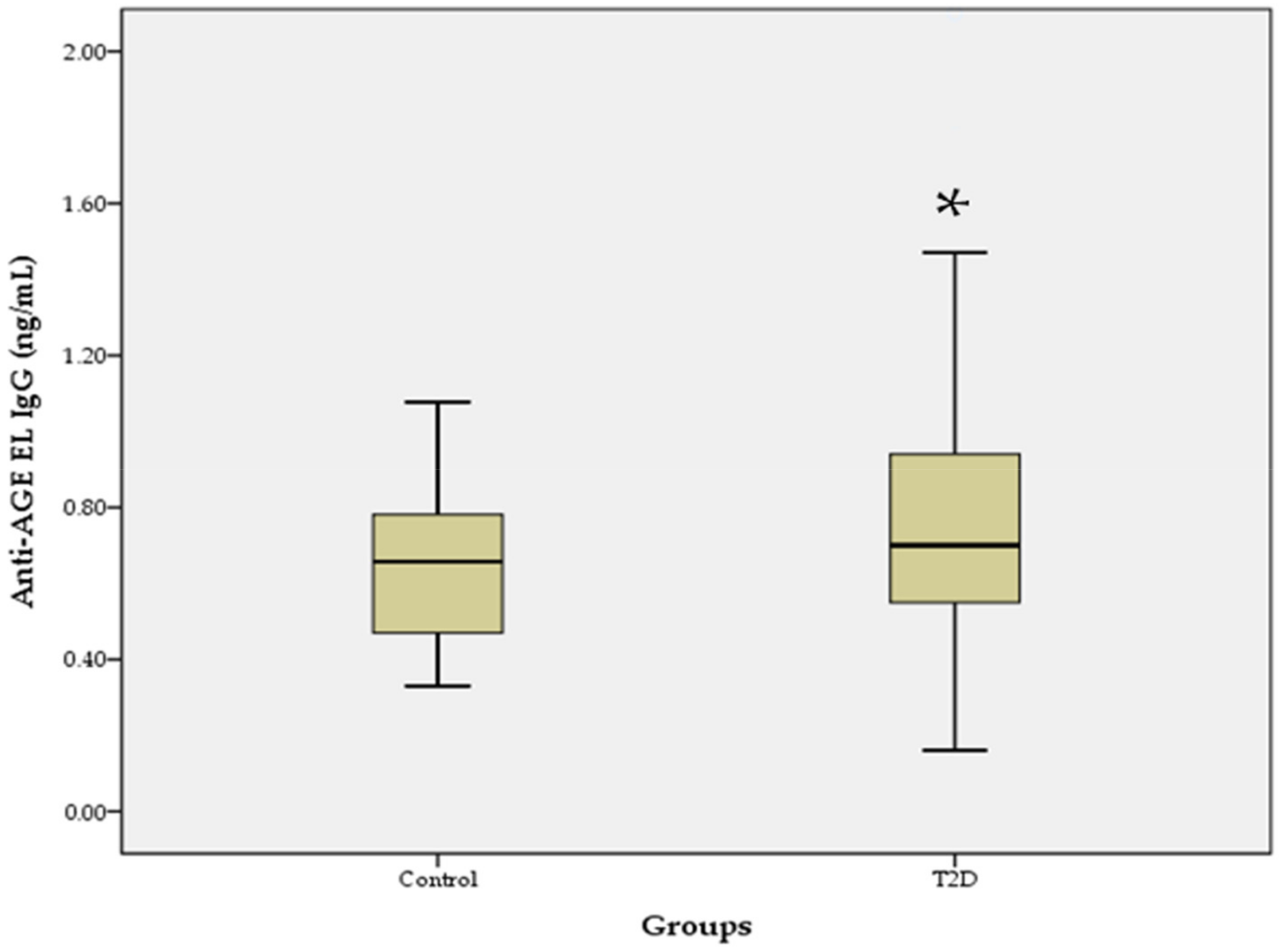
3.2. Comparison of Anti-AGE EL Antibody Levels between the T2D Group and Controls
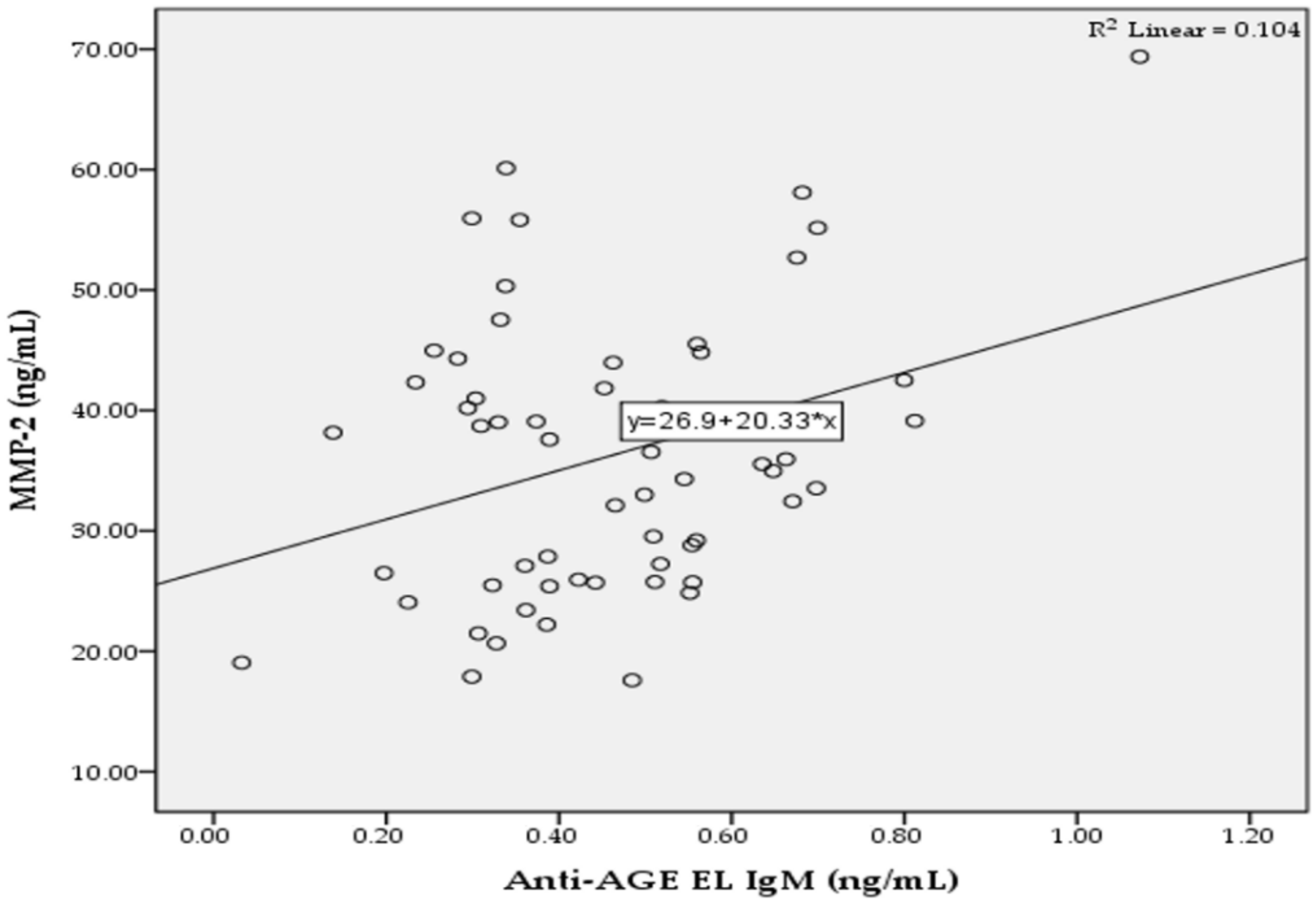
3.3. Correlation between Anti-AGE EL Antibody Levels and Clinical Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cho, N.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef]
- Dougherty, T.; Heile, M. Type 2 diabetes in the US managed care setting: The burden of disease and rationale for an oral glucagon-like peptide-1 receptor agonist. Am. J. Manag. Care 2020, 26, S325–S334. [Google Scholar] [PubMed]
- Bachmann, K.N.; Wang, T.J. Biomarkers of cardiovascular disease: Contributions to risk prediction in individuals with diabetes. Diabetologia 2018, 61, 987–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turk, Z.; Ljubic, S.; Turk, N.; Benko, B. Detection of autoantibodies against advanced glycation end products and AGE-immune complexes in serum of patients with diabetes mellitus. Clin. Chim. Acta 2001, 303, 105–115. [Google Scholar] [CrossRef]
- Prasad, A.; Bekker, P.; Tsimikas, S. Advanced glycation end products and diabetic cardiovascular disease. Cardiol. Rev. 2012, 20, 177–183. [Google Scholar] [CrossRef]
- Singh, V.P.; Bali, A.; Singh, N.; Jaggi, A.S. Advanced glycation end products and diabetic complications. Korean J. Physiol. Pharmacol. 2014, 18, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Rungratanawanich, W.; Qu, Y.; Wang, X.; Essa, M.M.; Song, B.J. Advanced glycation end products (AGEs) and other adducts in aging-related diseases and alcohol-mediated tissue injury. Exp. Mol. Med. 2021, 53, 168–188. [Google Scholar] [CrossRef]
- Fournet, M.; Bonté, F.; Desmoulière, A. Glycation damage: A possible hub for major pathophysiological disorders and aging. Aging Dis. 2018, 9, 880–900. [Google Scholar] [CrossRef] [Green Version]
- Peppa, M.; Raptis, S.A. Advanced glycation end products and cardiovascular disease. Curr. Diabetes Rev. 2008, 4, 92–100. [Google Scholar] [CrossRef]
- Sell, D.R.; Monnier, V.M. Molecular basis of arterial stiffening: Role of glycation—A mini-review. Gerontology 2012, 58, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Khan, M.S.; Akhter, F.; Khan, M.S.; Khan, A.; Ashraf, J.M.; Pandey, R.P.; Shahab, U. Glycoxidation of biological macromolecules: A critical approach to halt the menace of glycation. Glycobiology 2014, 24, 979–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snedeker, J.G.; Gautieri, A. The role of collagen crosslinks in ageing and diabetes—The good, the bad, and the ugly. Muscles Ligaments Tendons J. 2014, 4, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Brüel, A.; Oxlund, H. Changes in biomechanical properties, composition of collagen and elastin, and advanced glycation endproducts of the rat aorta in relation to age. Atherosclerosis 1996, 127, 155–165. [Google Scholar] [CrossRef]
- Hamada, Y.; Araki, N.; Horiuchi, S.; Hotta, N. Role of polyol pathway in nonenzymatic glycation. Nephrol. Dial. Transplant. 1996, 11, 95–98. [Google Scholar] [CrossRef] [Green Version]
- Khalid, M.; Petroianu, G.; Adem, A. Advanced glycation end products and diabetes mellitus: Mechanisms and perspectives. Biomolecules 2022, 12, 542. [Google Scholar] [CrossRef]
- Misciagna, G.; Michele, G.D.; Trevisan, M. Non enzymatic glycated proteins in the blood and cardiovascular disease. Curr. Pharm. Des. 2007, 13, 3688–3695. [Google Scholar] [CrossRef]
- Briones, A.M.; Arribas, S.M.; Salaices, M. Role of extracellular matrix in vascular remodeling of hypertension. Curr. Opin. Nephrol. Hypertens. 2010, 19, 187–194. [Google Scholar] [CrossRef]
- Cocciolone, A.J.; Hawes, J.Z.; Staiculescu, M.C.; Johnson, E.O.; Murshed, M.; Wagenseil, J.E. Elastin, arterial mechanics, and cardiovascular disease. Am. J. Physiol.-Heart Circ. Physiol. 2018, 315, H189–H205. [Google Scholar] [CrossRef]
- Winlove, C.; Parker, K.; Avery, N.; Bailey, A. Interactions of elastin and aorta with sugars in vitro and their effects on biochemical and physical properties. Diabetologia 1996, 39, 1131–1139. [Google Scholar] [CrossRef]
- Duca, L.; Blaise, S.; Romier, B.; Laffargue, M.; Gayral, S.; El Btaouri, H.; Kawecki, C.; Guillot, A.; Martiny, L.; Debelle, L.; et al. Matrix ageing and vascular impacts: Focus on elastin fragmentation. Cardiovasc. Res. 2016, 110, 298–308. [Google Scholar] [CrossRef] [Green Version]
- Nicoloff, G.; Weiss, A.S.; Iotova, V.; Tzaneva, V.; Petrova, C.; Domuschieva, N.; Nikolov, A.; Tzvetanov, P.; Christova, P. Abnormal levels of serum antielastin antibodies in children with diabetes mellitus type 1. J. Investig. Med. 2006, 54, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Nikolov, A.; Blazhev, A.; Tzekova, M.; Kostov, K.; Popovski, N. Serum levels of antibodies to advanced glycation end products in patients with type 2 diabetes mellitus and hypertension. Folia Med. 2020, 62, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Nicoloff, G.; Baydanoff, S.; Stanimirova, N.; Petrova, C.; Christova, P. An association of anti-elastin IgA antibodies with development of retinopathy in diabetic children. Gen. Pharmacol. 2000, 35, 83–87. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Yamamoto, H. Receptor for advanced glycation end-products-mediated inflammation and diabetic vascular complications. J. Diabetes Investig. 2011, 2, 155–157. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Park, S.; Lakatta, E.G. RAGE signaling in inflammation and arterial aging. Front. Biosci. 2009, 14, 1403–1413. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, N. Advanced glycation endproducts—Role in pathology of diabetic complications. Diabetes Res. Clin. Pract. 2005, 67, 3–21. [Google Scholar] [CrossRef]
- Baydanoff, S.; Konova, E.; Dosheva, I.; Dorovski, P. Non-enzymatic glycation of elastin. Glycosylation Dis. 1994, 1, 53–58. [Google Scholar] [CrossRef]
- Itariu, B.K.; Stulnig, T.M. Autoimmune aspects of type 2 diabetes mellitus—A mini-review. Gerontology 2014, 60, 189–196. [Google Scholar] [CrossRef]
- Baydanoff, S.; Konova, E.; Ivanova, N. Determination of anti-AGE antibodies in human serum. Glycoconj. J. 1996, 13, 335–339. [Google Scholar] [CrossRef]
- Nicoloff, G.; Baydanoff, S.; Petrova, C.; Christova, P. Antibodies to advanced glycation end products in children with diabetes mellitus. Vascul. Pharmacol. 2002, 39, 39–45. [Google Scholar] [CrossRef]
- Prasad, K.; Mishra, M. Do advanced glycation end products and its receptor play a role in pathophysiology of hypertension? Int. J. Angiol. 2017, 26, 1–11. [Google Scholar] [PubMed] [Green Version]
- Ahmad, M.N.; Farah, A.I.; Al-Qirim, T.M. The cardiovascular complications of diabetes: A striking link through protein glycation. Rom. J. Intern. Med. 2020, 58, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Goldin, A.; Beckman, J.A.; Schmidt, A.M.; Creager, M.A. Advanced glycation end products: Sparking the development of diabetic vascular injury. Circulation 2006, 114, 597–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geha, R.S.; Rosen, F.S. The genetic basis of immunoglobulin-class switching. N. Engl. J. Med. 1994, 330, 1008–1009. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Patron, C.; Radomski, M.W.; Davidge, S.T. Vascular matrix metalloproteinase-2 cleaves big endothelin-1 yielding a novel vasoconstrictor. Circ. Res. 1999, 85, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Thrailkill, K.M.; Bunn, R.C.; Moreau, C.S.; Cockrell, G.E.; Simpson, P.M.; Coleman, H.N.; Frindik, J.P.; Kemp, S.F.; Fowlkes, J.L. Matrix metalloproteinase-2 dysregulation in type 1 diabetes. Diabetes Care 2007, 30, 2321–2326. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Fernandez, N.; Jacobs-Cachá, C.; Mora-Gutiérrez, J.M.; Vergara, A.; Orbe, J.; Soler, M.J. Matrix metalloproteinases in diabetic kidney disease. J. Clin. Med. 2020, 9, 472. [Google Scholar] [CrossRef] [Green Version]
- Mohammad, G.; Kowluru, R.A. Matrix metalloproteinase-2 in the development of diabetic retinopathy and mitochondrial dysfunction. Lab. Investig. 2010, 90, 1365–1372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmelzer, C.E.; Duca, L. Elastic fibers: Formation, function, and fate during aging and disease. FEBS J. 2021, 298, 3704–3730. [Google Scholar] [CrossRef]
- Heinz, A. Elastases and elastokines: Elastin degradation and its significance in health and disease. Crit. Rev. Biochem. Mol. Biol. 2020, 55, 252–273. [Google Scholar] [CrossRef]
- Gui, F.; You, Z.; Fu, S.; Wu, H.; Zhang, Y. Endothelial dysfunction in diabetic retinopathy. Front. Endocrinol. 2020, 11, 591. [Google Scholar] [CrossRef] [PubMed]
- Elmarakby, A.A.; Sullivan, J.C. Relationship between oxidative stress and inflammatory cytokines in diabetic nephropathy. Cardiovasc. Ther. 2012, 30, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Pertyńska-Marczewska, M.; Kiriakidis, S.; Wait, R.; Beech, J.; Feldmann, M.; Paleolog, E.M. Advanced glycation end products upregulate angiogenic and pro-inflammatory cytokine production in human monocyte/macrophages. Cytokine 2004, 28, 35–47. [Google Scholar] [CrossRef]
- Ganter, U.; Arcone, R.; Toniatti, C.; Morrone, G.; Ciliberto, G. Dual control of C-reactive protein gene expression by interleukin-1 and interleukin-6. EMBO J. 1989, 8, 3773–3779. [Google Scholar] [CrossRef]
- Pickup, J.; Mattock, M.; Chusney, G.; Burt, D. NIDDM as a disease of the innate immune system: Association of acute-phase reactants and interleukin-6 with metabolic syndrome X. Diabetologia 1997, 40, 1286–1292. [Google Scholar] [CrossRef] [Green Version]
- Tan, K.C.B.; Chow, W.S.; Tam, S.; Bucala, R.; Betteridge, J. Association between acute-phase reactants and advanced glycation end products in type 2 diabetes. Diabetes Care 2004, 27, 223–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jialal, I.; Devaraj, S.; Venugopal, S.K. C-reactive protein: Risk marker or mediator in atherothrombosis? Hypertension 2004, 44, 6–11. [Google Scholar] [CrossRef]
- Korça, E.; Piskovatska, V.; Börgermann, J.; Navarrete Santos, A.; Simm, A. Circulating antibodies against AGE-modified proteins in patients with coronary atherosclerosis. Sci. Rep. 2020, 10, 17105. [Google Scholar] [CrossRef]
- Kostov, K.; Blazhev, A. Use of glycated hemoglobin (A1c) as a biomarker for vascular risk in type 2 diabetes: Its relationship with matrix metalloproteinases-2, -9 and the metabolism of collagen IV and elastin. Medicina 2020, 56, 231. [Google Scholar] [CrossRef]
- Peterszegi, G.; Mandet, C.; Texier, S.; Robert, L.; Bruneval, P. Lymphocytes in human atherosclerotic plaque exhibit the elastin-laminin receptor: Potential role in atherogenesis. Atherosclerosis 1997, 135, 103–107. [Google Scholar] [CrossRef]
- Peterszegi, G.; Texier, S.; Robert, L. Human helper and memory lymphocytes exhibit an inducible elastin-laminin receptor. Int. Arch. Allergy Immunol. 1997, 114, 218–223. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variables | Healthy Control Subjects | Patients with T2D |
|---|---|---|
| (n = 20) | (n = 59) | |
| Sex, Male/Female | 10/10 | 25/34 |
| Age, years 1 | 61.5 ± 11.4 | 60.8 ± 14.7 |
| Duration of T2D 1 | N/A | 10.1 ± 7.8 |
| SBP, mmHg 1 | 121.5 ± 8.6 | 149.2 ±16.7 *** |
| DBP, mmHg 1 | 78.2 ± 7.5 | 83.0 ± 10.4 |
| BMI, kg/m2 1 | 24.9 ± 2.4 | 28.4 ± 4.5 *** |
| HbA1c (%) 1 | N/A | 7.5 ± 1.8 |
| TC, mmol/L 1 | 4.2 ± 0.7 | 5.2 ± 1.8 * |
| LDL-C, mmol/L 1 | 2.8 ± 0.8 | 3.0 ± 1.1 |
| HDL-C, mmol/L 1 | 1.2 ± 0.2 | 1.0 ± 0.3 *** |
| TG, mmol/L 1 | 1.4 ± 0.4 | 2.7 ± 3.0 |
| CRP, mg/L 1 | 1.1 ± 0.9 | 8.4 ± 7.9 *** |
| MMP-2, ng/mL 1 | 30.6 ± 1.8 | 36.2 ± 1.5 * |
| MMP-9, ng/mL 1 | 25.8 ± 2.8 | 38.4 ± 2.6 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostov, K.; Blazhev, A. Elevated IgG and IgM Autoantibodies to Advanced Glycation End Products of Vascular Elastin in Hypertensive Patients with Type 2 Diabetes: Relevance to Disease Initiation and Progression. Pathophysiology 2022, 29, 426-434. https://doi.org/10.3390/pathophysiology29030034
Kostov K, Blazhev A. Elevated IgG and IgM Autoantibodies to Advanced Glycation End Products of Vascular Elastin in Hypertensive Patients with Type 2 Diabetes: Relevance to Disease Initiation and Progression. Pathophysiology. 2022; 29(3):426-434. https://doi.org/10.3390/pathophysiology29030034
Chicago/Turabian StyleKostov, Krasimir, and Alexander Blazhev. 2022. "Elevated IgG and IgM Autoantibodies to Advanced Glycation End Products of Vascular Elastin in Hypertensive Patients with Type 2 Diabetes: Relevance to Disease Initiation and Progression" Pathophysiology 29, no. 3: 426-434. https://doi.org/10.3390/pathophysiology29030034
APA StyleKostov, K., & Blazhev, A. (2022). Elevated IgG and IgM Autoantibodies to Advanced Glycation End Products of Vascular Elastin in Hypertensive Patients with Type 2 Diabetes: Relevance to Disease Initiation and Progression. Pathophysiology, 29(3), 426-434. https://doi.org/10.3390/pathophysiology29030034