Association Between Endocrine Therapy and Fracture Risk in Women with Breast Cancer in Germany—A Retrospective Cohort Study



Simple Summary
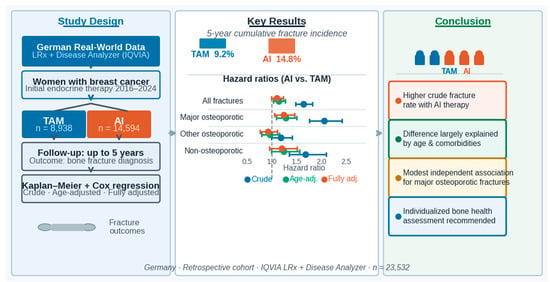
Abstract
1. Introduction
2. Methods
2.1. Data Sources
2.2. Study Population and Outcomes
2.3. Statistical Analyses
3. Results
3.1. Basic Characteristics of the Study Sample
3.2. Cumulative Incidence of Fractures
3.3. Association Between AI Therapy and Fracture Risk
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2023 Breast Cancer Collaborators. Global, regional, and national burden of breast cancer among females, 1990–2023, with forecasts to 2050: A systematic analysis for the Global Burden of Disease Study 2023. Lancet Oncol. 2026, 27, 302–326. [Google Scholar] [CrossRef]
- Smolarz, B.; Nowak, A.Z.; Romanowicz, H. Breast Cancer—Epidemiology, Classification, Pathogenesis and Treatment (Review of Literature). Cancers 2022, 14, 2569. [Google Scholar] [CrossRef]
- Harbeck, N.; Penault-Llorca, F.; Cortes, J.; Gnant, M.; Houssami, N.; Poortmans, P.; Ruddy, K.; Tsang, J.; Cardoso, F. Breast cancer. Nat. Rev. Dis. Prim. 2019, 5, 66. [Google Scholar] [CrossRef] [PubMed]
- Tong, C.W.S.; Wu, M.; Cho, W.C.S.; To, K.K.W. Recent Advances in the Treatment of Breast Cancer. Front. Oncol. 2018, 8, 227. [Google Scholar] [CrossRef] [PubMed]
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef]
- Font, R.; Buxó, M.; Ameijide, A.; Martínez, J.M.; Marcos-Gragera, R.; Carulla, M.; Puigdemont, M.; Vilardell, M.; Civit, S.; Viñas, G.; et al. Using population-based data to evaluate the impact of adherence to endocrine therapy on survival in breast cancer through the web-application BreCanSurvPred. Sci. Rep. 2022, 12, 8097. [Google Scholar] [CrossRef]
- Burciu, O.M.; Merce, A.G.; Cerbu, S.; Iancu, A.; Popoiu, T.A.; Cobec, I.M.; Sas, I.; Dimofte, G.M. Current Endocrine Therapy in Hormone-Receptor-Positive Breast Cancer: From Tumor Biology to the Rationale for Therapeutic Tunning. Medicina 2025, 61, 1280. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative Group. Aromatase inhibitors versus tamoxifen in early breast cancer: Patient-level meta-analysis of the randomised trials. Lancet 2015, 386, 1341–1352. [Google Scholar] [CrossRef]
- Tseng, O.L.; Spinelli, J.J.; Gotay, C.C.; Ho, W.Y.; McBride, M.L.; Dawes, M.G. Aromatase inhibitors are associated with a higher fracture risk than tamoxifen: A systematic review and meta-analysis. Ther. Adv. Musculoskelet. Dis. 2018, 10, 71–90. [Google Scholar] [CrossRef]
- Qu, H.; Wang, J.; Wang, Z.; Guan, B.; Zheng, Y. Impact of different endocrine therapies on bone mineral density and fracture risk in postmenopausal breast cancer patients: A meta-analysis. Front. Med. 2025, 12, 1665389. [Google Scholar] [CrossRef]
- Cho, H.; Kim, B.; Han, K.; Kim, S.; Cho, I.Y.; Shin, D.W. Increased risk of fracture among breast cancer patients: A nationwide retrospective cohort study. J. Cancer Surviv. 2026. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.H.; Tsai, C.F.; Hsu, Y.C.; Wu, C.Y.; Yang, H.Y. Aromatase inhibitors therapy and major osteoporotic fracture risk in postmenopausal breast cancer patients: A nationwide real-world cohort study. Breast Cancer Res. 2025, 27, 95. [Google Scholar] [CrossRef] [PubMed]
- Leslie, W.D.; Morin, S.N.; Lix, L.M.; Niraula, S.; McCloskey, E.V.; Johansson, H.; Harvey, N.C.; Kanis, J.A. Performance of FRAX in Women with Breast Cancer Initiating Aromatase Inhibitor Therapy: A Registry-Based Cohort Study. J. Bone Miner. Res. 2019, 34, 1428–1435. [Google Scholar] [CrossRef]
- Kwak, M.K.; Lee, S.; Lee, J.Y.; Park, J.W.; Jeon, Y.J.; Yoo, B.N.; Bak, J.K.; Kim, H.Y.; Lee, Y.K. Differential fracture risk in breast cancer patients based on endocrine therapy and age: A nationwide cohort study. Osteoporos. Int. 2025, 36, 2519–2530. [Google Scholar] [CrossRef]
- Blanchette, P.S.; Lam, M.; Le, B.; Richard, L.; Shariff, S.Z.; Ouédraogo, A.M.; Pritchard, K.I.; Raphael, J.; Vandenberg, T.; Fernandes, R.; et al. The association between endocrine therapy use and osteoporotic fracture among post-menopausal women treated for early-stage breast cancer in Ontario, Canada. Breast 2021, 60, 295–301. [Google Scholar] [CrossRef]
- Kostev, K.; Wang, Y.; Singh, R.; Kalder, M.; Loosen, S.H.; Roderburg, C.; Konrad, M.; Jacob, L. German longitudinal prescription database (LRx): Description of characteristics, use in pharmacoepidemiological research, and limitations. Int. J. Clin. Pharmacol. Ther. 2024, 62, 20–28. [Google Scholar] [CrossRef]
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, S.; Kostev, K. Basic characteristics and representativeness of the German Disease Analyzer database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef]
- Rabaglio, M.; Sun, Z.; Price, K.N.; Castiglione-Gertsch, M.; Hawle, H.; Thürlimann, B.; Mouridsen, H.; Campone, M.; Forbes, J.F.; Paridaens, R.J.; et al. Bone fractures among postmenopausal patients with endocrine-responsive early breast cancer treated with 5 years of letrozole or tamoxifen in the BIG 1-98 trial. Ann. Oncol. 2009, 20, 1489–1498. [Google Scholar] [CrossRef]
- Neuner, J.M.; Shi, Y.; Kong, A.L.; Kamaraju, S.; Smith, E.C.; Smallwood, A.J.; Laud, P.W.; Charlson, J.A. Fractures in a nationwide population-based cohort of users of breast cancer hormonal therapy. J. Cancer Surviv. 2018, 12, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Kyvernitakis, I.; Kostev, K.; Hadji, P. The tamoxifen paradox—Influence of adjuvant tamoxifen on fracture risk in pre- and postmenopausal women with breast cancer. Osteoporos. Int. 2018, 29, 2557–2564. [Google Scholar] [CrossRef]
- Ensrud, K.E. Epidemiology of fracture risk with advancing age. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 1236–1242. [Google Scholar] [CrossRef]
- Buzkova, P.; Cauley, J.A.; Fink, H.A.; Robbins, J.A.; Mukamal, K.J.; Barzilay, J.I. Age-Related Factors Associated With The Risk of Hip Fracture. Endocr. Pract. 2023, 29, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Eastell, R.; Hannon, R.A.; Cuzick, J.; Dowsett, M.; Clack, G.; Adams, J.E.; ATAC Trialists’ Group. Effect of an aromatase inhibitor on BMD and bone turnover markers: 2-year results of the Anastrozole, Tamoxifen, Alone or in Combination (ATAC) trial. J. Bone Miner. Res. 2006, 21, 1215–1223. [Google Scholar] [CrossRef]
- Rachner, T.D.; Göbel, A.; Jaschke, N.P.; Hofbauer, L.C. Challenges in Preventing Bone Loss Induced by Aromatase Inhibitors. J. Clin. Endocrinol. Metab. 2020, 105, dgaa463. [Google Scholar] [CrossRef] [PubMed]
- Hadji, P.; Aapro, M.S.; Body, J.J.; Gnant, M.; Brandi, M.L.; Reginster, J.Y.; Zillikens, M.C.; Glüer, C.C.; de Villiers, T.; Baber, R.; et al. Management of Aromatase Inhibitor-Associated Bone Loss (AIBL) in postmenopausal women with hormone sensitive breast cancer: Joint position statement of the IOF, CABS, ECTS, IEG, ESCEO IMS, and SIOG. J. Bone Oncol. 2017, 7, 1–12. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fracture Category | ICD-10 Codes | Description |
|---|---|---|
| Major osteoporotic fractures (MOF) | M80 | Osteoporosis with current pathological fracture |
| S72.0–S72.2, S72.9 | Hip fractures | |
| S22.0 | Thoracic vertebra fracture | |
| S32.0 | Lumbar vertebra fracture | |
| S42.2–S42.4, S42.9 | Proximal humerus fractures | |
| S52.5, S52.9 | Distal forearm fractures | |
| Other osteoporotic fractures | S22.1–S22.5, S22.8–S22.9 | Other thoracic fractures |
| S32.1–S32.5, S32.7–S32.8 | Pelvic and other lumbar fractures | |
| S82.0–S82.9 | Lower leg fractures | |
| S92.0–S92.9 | Foot fractures | |
| Non-osteoporotic or undefined fractures | S02.0–S02.9 | Skull and facial bones |
| S12.0–S12.9 | Cervical spine | |
| S42.0, S42.1, S42.7, S42.8 | Clavicle, scapula, shoulder | |
| S52.0–S52.4, S52.6–S52.8 | Other forearm fractures | |
| S62.0–S62.9 | Wrist and hand | |
| S72.3–S72.4, S72.7–S72.8 | Other femur fractures | |
| T02 | Multiple fractures | |
| T08 | Spine unspecified | |
| T10 | Upper limb unspecified | |
| T12 | Lower limb unspecified |
| Variable | Patients Treated with TAM (%) | Patients Treated with AIs (%) | p Value |
|---|---|---|---|
| n | 8938 | 14,594 | |
| Age (Mean, SD) | 66.7 (11.7) | 60.2 (13.5) | <0.001 |
| Age ≤ 55 | 3818 (42.7) | 1860 (12.7) | <0.001 |
| Age 56–65 | 1927 (21.6) | 3835 (26.3) | |
| Age 66–75 | 1698 (19.0) | 4184 (28.7) | |
| Age > 75 | 1495 (16.7) | 4715 (32.3) | |
| Co-diagnoses | |||
| Osteoporosis | 448 (5.0) | 966 (6.6) | <0.001 |
| Bone fractures | 421 (4.7) | 1030 (7.1) | <0.001 |
| Bone metastasis | 36 (0.4) | 324 (2.2) | <0.001 |
| Diabetes mellitus | 958 (10.7) | 2516 (17.2) | <0.001 |
| Hypertension | 2395 (26.8) | 5291 (36.3) | <0.001 |
| Dyslipidemia | 1297 (14.5) | 2864 (19.6) | <0.001 |
| Obesity | 571 (6.4) | 1175 (8.1) | <0.001 |
| Depression | 1371 (15.3) | 2327 (15.9) | 0.215 |
| Chronic bronchitis and COPD | 499 (5.6) | 992 (6.8) | <0.001 |
| Thyroid gland disorders | 162 (1.8) | 285 (2.0) | 0.444 |
| Rheumatoid arthritis | 150 (1.7) | 275 (1.9) | 0.249 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Share and Cite
Kostev, K.; Peters, M.; Sievert, H.; Kalder, M. Association Between Endocrine Therapy and Fracture Risk in Women with Breast Cancer in Germany—A Retrospective Cohort Study. Curr. Oncol. 2026, 33, 322. https://doi.org/10.3390/curroncol33060322
Kostev K, Peters M, Sievert H, Kalder M. Association Between Endocrine Therapy and Fracture Risk in Women with Breast Cancer in Germany—A Retrospective Cohort Study. Current Oncology. 2026; 33(6):322. https://doi.org/10.3390/curroncol33060322
Chicago/Turabian StyleKostev, Karel, Maximilian Peters, Henning Sievert, and Matthias Kalder. 2026. "Association Between Endocrine Therapy and Fracture Risk in Women with Breast Cancer in Germany—A Retrospective Cohort Study" Current Oncology 33, no. 6: 322. https://doi.org/10.3390/curroncol33060322
APA StyleKostev, K., Peters, M., Sievert, H., & Kalder, M. (2026). Association Between Endocrine Therapy and Fracture Risk in Women with Breast Cancer in Germany—A Retrospective Cohort Study. Current Oncology, 33(6), 322. https://doi.org/10.3390/curroncol33060322