MET Exon 14 Skipping Mutations in Lung Cancer: Clinical–Pathological Characteristics and Immune Microenvironment

 ,
,
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patients
2.2. Multiplex Immunofluorescence (mIF)
2.3. Data Analysis
3. Results
3.1. Clinicopathologic Characteristics
3.2. Infiltrating Immune Cells
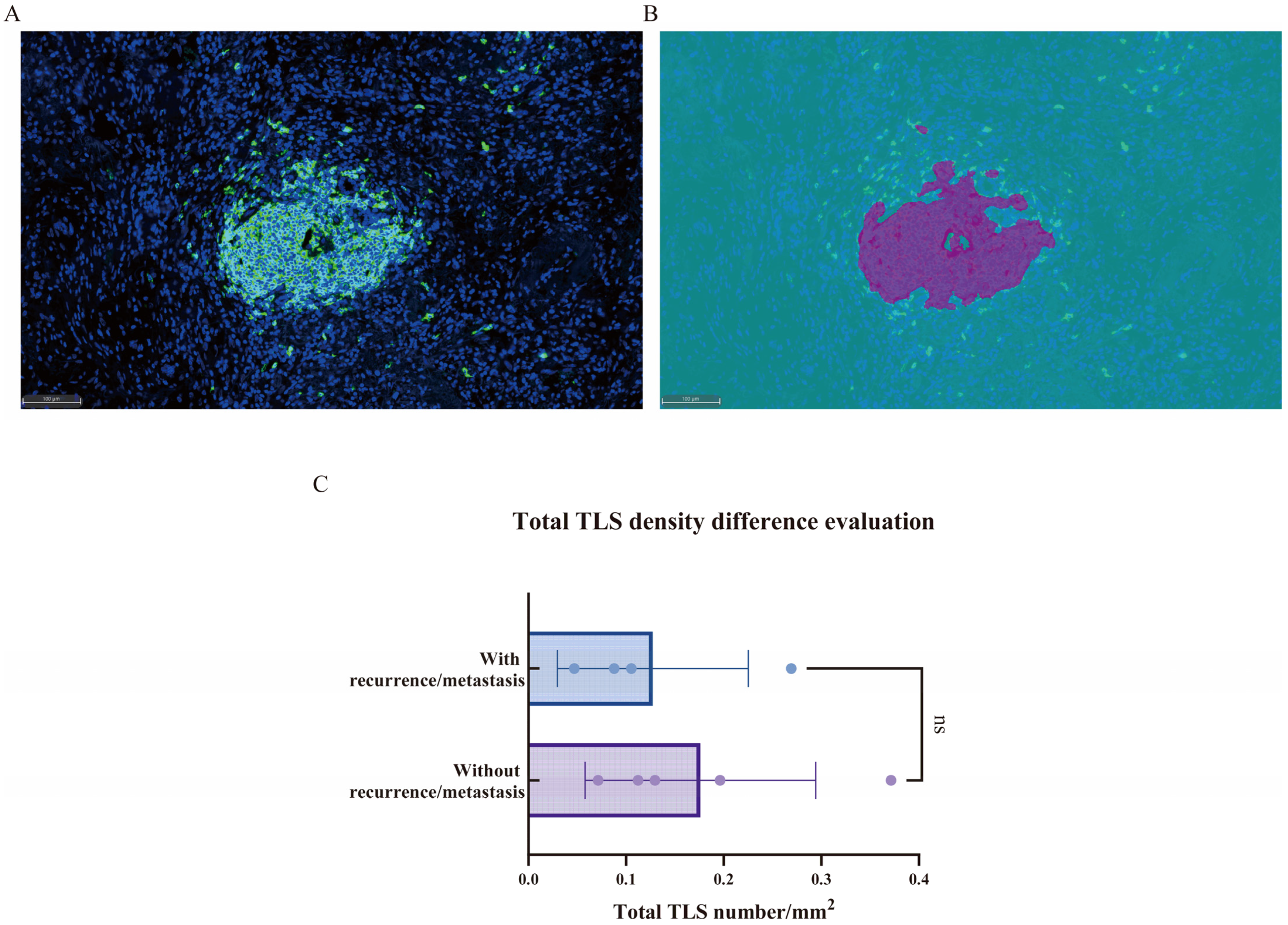
3.3. Tertiary Lymphoid Structures (TLSs)
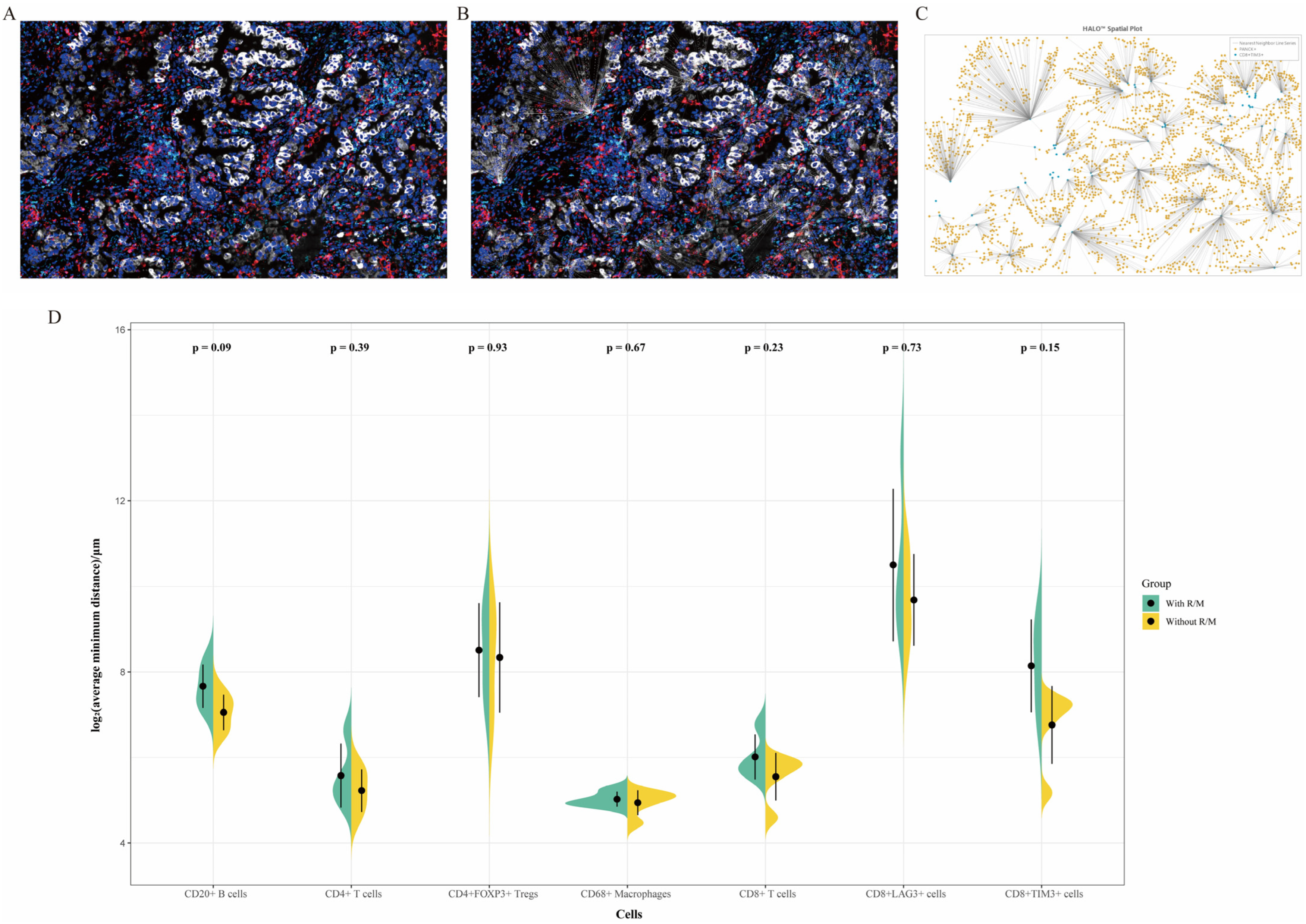
3.4. Nearest Neighbor Analysis
3.5. Factors Associated with Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salgia, R.; Sattler, M.; Scheele, J.; Stroh, C.; Felip, E. The promise of selective MET inhibitors in non-small cell lung cancer with MET exon 14 skipping. Cancer Treat. Rev. 2020, 87, 102022. [Google Scholar] [CrossRef]
- Remon, J.; Hendriks, L.E.L.; Mountzios, G.; García-Campelo, R.; Saw, S.P.L.; Uprety, D.; Recondo, G.; Villacampa, G.; Reck, M. MET alterations in NSCLC—Current Perspectives and Future Challenges. J. Thorac. Oncol. 2023, 18, 419–435. [Google Scholar] [CrossRef]
- Fujino, T.; Suda, K.; Mitsudomi, T. Lung Cancer with MET exon 14 Skipping Mutation: Genetic Feature, Current Treatments, and Future Challenges. Lung Cancer 2021, 12, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Mazieres, J.; Vioix, H.; Pfeiffer, B.M.; Campden, R.I.; Chen, Z.; Heeg, B.; Cortot, A.B. MET Exon 14 Skipping in NSCLC: A Systematic Literature Review of Epidemiology, Clinical Characteristics, and Outcomes. Clin. Lung Cancer 2023, 24, 483–497. [Google Scholar] [CrossRef]
- Awad, M.M.; Oxnard, G.R.; Jackman, D.M.; Savukoski, D.O.; Hall, D.; Shivdasani, P.; Heng, J.C.; Dahlberg, S.E.; Jänne, P.A.; Verma, S.; et al. MET Exon 14 Mutations in Non–Small-Cell Lung Cancer Are Associated With Advanced Age and Stage-Dependent MET Genomic Amplification and c-Met Overexpression. J. Clin. Oncol. 2016, 34, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Schrock, A.B.; Frampton, G.M.; Suh, J.; Chalmers, Z.R.; Rosenzweig, M.; Erlich, R.L.; Halmos, B.; Goldman, J.; Forde, P.; Leuenberger, K.; et al. Characterization of 298 Patients with Lung Cancer Harboring MET Exon 14 Skipping Alterations. J. Thorac. Oncol. 2016, 11, 1493–1502. [Google Scholar] [CrossRef] [PubMed]
- Tong, J.H.; Yeung, S.F.; Chan, A.W.H.; Chung, L.Y.; Chau, S.L.; Lung, R.W.M.; Tong, C.Y.; Chow, C.; Tin, E.K.Y.; Yu, Y.H.; et al. MET Amplification and Exon 14 Splice Site Mutation Define Unique Molecular Subgroups of Non–Small Cell Lung Carcinoma with Poor Prognosis. Clin. Cancer Res. 2016, 22, 3048–3056. [Google Scholar] [CrossRef]
- Wolf, J.; Seto, T.; Han, J.-Y.; Reguart, N.; Garon, E.B.; Groen, H.J.M.; Tan, D.S.W.; Hida, T.; de Jonge, M.; Orlov, S.V.; et al. Capmatinib in MET Exon 14–Mutated or MET-Amplified Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 944–957. [Google Scholar] [CrossRef]
- Paik, P.K.; Felip, E.; Veillon, R.; Sakai, H.; Cortot, A.B.; Garassino, M.C.; Mazieres, J.; Viteri, S.; Senellart, H.; Van Meerbeeck, J.; et al. Tepotinib in Non–Small-Cell Lung Cancer with MET Exon 14 Skipping Mutations. N. Engl. J. Med. 2020, 383, 931–943. [Google Scholar] [CrossRef]
- Socinski, M.A.; Pennell, N.A.; Davies, K.D. MET Exon 14 Skipping Mutations in Non-Small-Cell Lung Cancer: An Overview of Biology, Clinical Outcomes, and Testing Considerations. JCO Precis. Oncol. 2021, 5, 653–663. [Google Scholar] [CrossRef]
- Xia, Y.; Tian, P.; Zhou, M.; Zhao, J.; Jin, Y.; Guo, Z.; Li, X.; Lu, W.; Miao, D.; Lu, Y.; et al. Ensartinib for advanced or metastatic non-small-cell lung cancer with MET exon 14 skipping mutations (EMBRACE): A multi-center, single-arm, phase 2 trial. eClinicalMedicine 2025, 81, 103099. [Google Scholar] [CrossRef] [PubMed]
- Krebs, M.G.; Cho, B.C.; Hiret, S.; Han, J.-Y.; Lee, K.H.; Llácer Pérez, C.; De Braud, F.; Haura, E.B.; Sanborn, R.E.; Yang, J.C.-H.; et al. Amivantamab in Participants with Advanced Non-small Cell Lung Cancer (NSCLC) and MET Exon 14 Skipping Mutations: Final Results From the CHRYSALIS Study. J. Thorac. Oncol. 2025; ahead of print. [Google Scholar] [CrossRef]
- Dantoing, E.; Piton, N.; Salaun, M.; Thiberville, L.; Guisier, F. Anti-PD1/PD-L1 Immunotherapy for Non-Small Cell Lung Cancer with Actionable Oncogenic Driver Mutations. Int. J. Mol. Sci. 2021, 22, 6288. [Google Scholar] [CrossRef] [PubMed]
- Sabari, J.K.; Leonardi, G.C.; Shu, C.A.; Umeton, R.; Montecalvo, J.; Ni, A.; Chen, R.; Dienstag, J.; Mrad, C.; Bergagnini, I.; et al. PD-L1 expression, tumor mutational burden, and response to immunotherapy in patients with MET exon 14 altered lung cancers. Ann. Oncol. 2018, 29, 2085–2091. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, H. Regulation of immune microenvironment may enable MET-altered NSCLC patients to benefit from immune checkpoint inhibitors. Lung Cancer 2021, 154, 221–223. [Google Scholar] [CrossRef]
- Blasi, M.; Kuon, J.; Lüders, H.; Misch, D.; Kauffmann-Guerrero, D.; Hilbrandt, M.; Kazdal, D.; Falkenstern-Ge, R.-F.; Hackanson, B.; Dintner, S.; et al. First-line immunotherapy for lung cancer with MET exon 14 skipping and the relevance of TP53 mutations. Eur. J. Cancer 2024, 199, 113556. [Google Scholar] [CrossRef] [PubMed]
- Pateriya, A.; Nema, R.; Mishra, A.; Kumar, A.; Shrivastava, A. Decreased Expression of CD247 and CD4 Immune Marker Predicts Poor Prognosis in Triple Negative Breast Cancer. Asian Pac. J. Cancer Prev. 2024, 25, 3187–3197. [Google Scholar] [CrossRef]
- Wessel, R.E.; Ageeb, N.; Obeid, J.M.; Mauldin, I.S.; Goundry, K.A.; Hanson, G.F.; Hossain, M.; Lehman, C.; Gentzler, R.D.; Wages, N.A.; et al. Spatial colocalization and combined survival benefit of natural killer and CD8 T cells despite profound MHC class I loss in non-small cell lung cancer. J. Immunother. Cancer 2024, 12, e009126. [Google Scholar] [CrossRef]
- Stover, D.G.; Salgado, R.; Savenkov, O.; Ballman, K.; Mayer, E.L.; Magbanua, M.J.M.; Loi, S.; Vater, M.; Glover, K.; Watson, M.; et al. Association between tumor-infiltrating lymphocytes and survival in patients with metastatic breast cancer receiving first-line chemotherapy: Analysis of CALGB 40502. npj Breast Cancer 2024, 10, 75. [Google Scholar] [CrossRef]
- Fu, R.; Zhang, C.; Song, M.M.; Gao, X.; Li, F.; Cai, M.; Jiang, B.Y.; Yang, X.N.; Wu, Y.L.; Zhong, W.Z. A single-cell map of patients with non-small cell lung cancer harboring rare-driver mutations after anti-PD-1 treatment. Cancer Lett. 2025, 616, 217595. [Google Scholar] [CrossRef]
- Kievit, H.; Muntinghe-Wagenaar, M.B.; Abdulahad, W.H.; Rutgers, A.; Hijmering-Kappelle, L.B.M.; Hiddinga, B.I.; Ubbels, J.F.; Wijsman, R.; van der Leij, M.J.; Bijzet, J.; et al. Baseline Blood CD8+ T Cell Activation Potency Discriminates Responders from Non-Responders to Immune Checkpoint Inhibition Combined with Stereotactic Radiotherapy in Non-Small-Cell Lung Cancer. Cancers 2024, 16, 2592. [Google Scholar] [CrossRef]
- Lee, M.-C.; Hummelink, K.; van der Noort, V.; Muller, M.; Schouten, R.D.; van den Heuvel, M.M.; Thommen, D.S.; Smit, E.F.; Meijer, G.A.; Monkhorst, K. Head-to-head comparison of composite and individual biomarkers to predict clinical benefit to PD-1 blockade in non-small cell lung cancer. PLoS ONE 2024, 19, e0293707. [Google Scholar] [CrossRef]
- Im, S.J.; Obeng, R.C.; Nasti, T.H.; McManus, D.; Kamphorst, A.O.; Gunisetty, S.; Prokhnevska, N.; Carlisle, J.W.; Yu, K.; Sica, G.L.; et al. Characteristics and anatomic location of PD-1(+)TCF1(+) stem-like CD8 T cells in chronic viral infection and cancer. Proc. Natl. Acad. Sci. USA 2023, 120, e2221985120. [Google Scholar] [CrossRef]
- Yang, G.; Cai, S.; Hu, M.; Li, C.; Yang, L.; Zhang, W.; Sun, J.; Sun, F.; Xing, L.; Sun, X. Functional status and spatial architecture of tumor-infiltrating CD8+ T cells are associated with lymph node metastases in non-small cell lung cancer. J. Transl. Med. 2023, 21, 320. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.L.; Ou, D.L.; Bai, L.Y.; Chen, C.W.; Lin, L.; Huang, S.F.; Cheng, A.L.; Jeng, Y.M.; Hsu, C. Exploring Markers of Exhausted CD8 T Cells to Predict Response to Immune Checkpoint Inhibitor Therapy for Hepatocellular Carcinoma. Liver Cancer 2021, 10, 346–359. [Google Scholar] [CrossRef] [PubMed]
- Lopez de Rodas, M.; Nagineni, V.; Ravi, A.; Datar, I.J.; Mino-Kenudson, M.; Corredor, G.; Barrera, C.; Behlman, L.; Rimm, D.L.; Herbst, R.S.; et al. Role of tumor infiltrating lymphocytes and spatial immune heterogeneity in sensitivity to PD-1 axis blockers in non-small cell lung cancer. J. Immunother. Cancer 2022, 10, e004440. [Google Scholar] [CrossRef] [PubMed]
- Dhiab, R.B.; Loyaux, R.; Garinet, S.; Bastide, M.; Léonard-Goyet, S.; Fabre, E.; Mansuet-Lupo, A.; Gibault, L.; Jouveshomme, S.; Giroux-Leprieur, E.; et al. MET exon 14 skipping mutations in non-small-cell lung cancer a 3 years screening experience. Sci. Rep. 2025, 15, 19347. [Google Scholar] [CrossRef]
- Xie, M.; Lin, X.; Bao, X.; Liang, Y.; Deng, H.; Song, J.; Ma, X.; Zhang, X.; Yao, J.; Pan, L.; et al. Tertiary Lymphoid Structure in Tumor Microenvironment and Immunotherapy of Lung Cancer. Arch. Bronconeumol. 2024, 60 (Suppl. 2), S77–S85. [Google Scholar] [CrossRef]
- Liu, Y.; Xiong, L.; Cai, R.; Chen, Y.; Ye, J.; Shen, B.; Zhou, G. Recent Progress of Tertiary Lymphoid Structure in Prognosis and Immunotherapy of Non-small Cell Lung Cancer. Zhongguo Fei Ai Za Zhi 2023, 26, 615–620. [Google Scholar] [CrossRef]
- Ma, L.; Qin, X.; Yu, A.; Liu, H.; Pan, D.; Gao, Y.; Wu, Z.; Chen, Z.; Han, Z. Clinicopathological and prognostic value of tertiary lymphoid structures in lung cancer: A meta-analysis. Clin. Transl. Oncol. 2024, 27, 1092–1104. [Google Scholar] [CrossRef]
- Mei, S.Q.; Liu, J.Q.; Huang, Z.J.; Luo, W.C.; Peng, Y.L.; Chen, Z.H.; Deng, Y.; Xu, C.R.; Zhou, Q. Identification of a risk score model based on tertiary lymphoid structure-related genes for predicting immunotherapy efficacy in non-small cell lung cancer. Thorac. Cancer 2024, 15, 1119–1131. [Google Scholar] [CrossRef]
- Xiaoxu, D.; Min, X.; Chengcheng, C. Immature central tumor tertiary lymphoid structures are associated with better prognosis in non-small cell lung cancer. BMC Pulm. Med. 2024, 24, 155. [Google Scholar] [CrossRef] [PubMed]
- Belderbos, R.A.; Corneth, O.B.J.; Dumoulin, D.; Hendriks, R.W.; Aerts, J.; Willemsen, M. Atypical B cells (CD21-CD27-IgD-) correlate with lack of response to checkpoint inhibitor therapy in NSCLC. Eur. J. Cancer 2024, 196, 113428. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Deng, Y.; Zhang, M.; Zhang, Q. Spatial tertiary lymphoid structures imply response to anti-PD-1 plus anlotinib in advanced non-small cell lung cancer. Immunology 2024, 173, 536–551. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Hu, T.; Zhao, J.; Zhu, Q.; Wang, J.; Huang, Z.; Xiang, C.; Zhao, R.; Zhu, C.; Lu, S.; et al. Novel molecular subtypes of METex14 non-small cell lung cancer with distinct biological and clinical significance. npj Precis. Oncol. 2024, 8, 159. [Google Scholar] [CrossRef]
- Masugi, Y.; Abe, T.; Ueno, A.; Fujii-Nishimura, Y.; Ojima, H.; Endo, Y.; Fujita, Y.; Kitago, M.; Shinoda, M.; Kitagawa, Y.; et al. Characterization of spatial distribution of tumor-infiltrating CD8(+) T cells refines their prognostic utility for pancreatic cancer survival. Mod. Pathol. 2019, 32, 1495–1507. [Google Scholar] [CrossRef]
- Mi, H.; Sivagnanam, S.; Betts, C.B.; Liudahl, S.M.; Jaffee, E.M.; Coussens, L.M.; Popel, A.S. Quantitative Spatial Profiling of Immune Populations in Pancreatic Ductal Adenocarcinoma Reveals Tumor Microenvironment Heterogeneity and Prognostic Biomarkers. Cancer Res. 2022, 82, 4359–4372. [Google Scholar] [CrossRef]
- Yang, L.; Zhang, W.; Sun, J.; Yang, G.; Cai, S.; Sun, F.; Xing, L.; Sun, X. Functional status and spatial interaction of T cell subsets driven by specific tumor microenvironment correlate with recurrence of non-small cell lung cancer. Front. Immunol. 2022, 13, 1022638. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | With Recurrence/Metastasis | Without Recurrence/ Metastasis | p Value |
|---|---|---|---|
| n = 6 (%) | n = 51 (%) | ||
| Age (years) | 0.665 | ||
| ≤60 | 1 (16.7) | 15 (29.4) | |
| >60 | 5 (83.3) | 36 (70.6) | |
| Gender | 0.025 | ||
| Male | 6 (100.0) | 24 (47.1) | |
| Female | 0 (0.0) | 27 (52.9) | |
| Smoking status | 0.000 | ||
| Current smokers | 0 (0.0) | 13 (25.5) | |
| Former smokers | 5 (83.3) | 2 (3.9) | |
| Never smokers | 1 (16.7) | 36 (70.6) | |
| T stage | 0.000 | ||
| T1a | 0 (0.0) | 8 (15.7) | |
| T1b | 0 (0.0) | 25 (49.0) | |
| T1c | 1 (16.7) | 13 (25.5) | |
| T2a | 3 (50.0) | 1 (2.0) | |
| T2b | 1(16.7) | 1 (2.0) | |
| T3 | 0 (0.0) | 2 (3.9) | |
| T4 | 1(16.7) | 1 (2.0) | |
| N stage | 0.194 | ||
| N0 | 4 (66.7) | 45 (86.0) | |
| N1 | 2 (33.3) | 4 (10.5) | |
| N2 | 0 (0.0) | 2 (3.5) | |
| Histology | 0.731 | ||
| Adenocarcinoma in situ | 0 (0.0) | 1 (2.0) | |
| Minimally invasive adenocarcinoma | 0 (0.0) | 8 (15.7) | |
| Invasive adenocarcinoma | 6 (100.0) | 39 (76.5) | |
| Squamous cell carcinoma | 0 (0.0) | 1 (2.0) | |
| Adenocarcinoma with sarcomatoid carcinoma | 0 (0.0) | 2 (3.9) | |
| Intravascular carcinoma embolus | 0.044 | ||
| Present | 3 (50.0) | 6 (11.8) | |
| Absent | 3 (50.0) | 45 (88.2) | |
| Pleural infiltration | 0.060 | ||
| Present | 3 (50.0) | 7 (13.7) | |
| Absent | 3 (50.0) | 44 (86.3) | |
| PD-L1 tumor proportion scale | 0.631 | ||
| ≥50% | 3 (50.0) | 11 (21.6) | |
| ≥1% and <50% | 1 (16.7) | 8 (15.7) | |
| <1% | 2 (33.3) | 21 (41.2) | |
| Unknown | 0 (0.0) | 11 (21.6) |
| Variables | HR (95%CI) | p-Value |
|---|---|---|
| Age | 0.78 (0.59–1.05) | 0.099 |
| Density of TIM3+ cells | 0.99 (0.99–1.00) | 0.089 |
| Density of CD8+TIM3+ cells | 0.89 (0.80–1.01) | 0.064 |
| Density of TIM3+ cells in the stroma | 0.99 (0.99–1.00) | 0.058 |
| Density of CD8+TIM3+ cells in the stroma | 0.91 (0.83–1.01) | 0.078 |
| Density of CD8+LAG3- cells in the stroma | 0.99 (0.98–1.00) | 0.095 |
| Average minimum distance of CD8+TIM3+ cells | 1.01 (1.00–1.02) | 0.064 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xue, Q.; Wang, Y.; Zheng, Q.; Huang, Z.; Lin, Y.; Jin, Y.; Li, Y. MET Exon 14 Skipping Mutations in Lung Cancer: Clinical–Pathological Characteristics and Immune Microenvironment. Curr. Oncol. 2025, 32, 403. https://doi.org/10.3390/curroncol32070403
Xue Q, Wang Y, Zheng Q, Huang Z, Lin Y, Jin Y, Li Y. MET Exon 14 Skipping Mutations in Lung Cancer: Clinical–Pathological Characteristics and Immune Microenvironment. Current Oncology. 2025; 32(7):403. https://doi.org/10.3390/curroncol32070403
Chicago/Turabian StyleXue, Qianqian, Yue Wang, Qiang Zheng, Ziling Huang, Yicong Lin, Yan Jin, and Yuan Li. 2025. "MET Exon 14 Skipping Mutations in Lung Cancer: Clinical–Pathological Characteristics and Immune Microenvironment" Current Oncology 32, no. 7: 403. https://doi.org/10.3390/curroncol32070403
APA StyleXue, Q., Wang, Y., Zheng, Q., Huang, Z., Lin, Y., Jin, Y., & Li, Y. (2025). MET Exon 14 Skipping Mutations in Lung Cancer: Clinical–Pathological Characteristics and Immune Microenvironment. Current Oncology, 32(7), 403. https://doi.org/10.3390/curroncol32070403