Psychedelic-Assisted Therapies for Psychosocial Symptoms in Cancer: A Systematic Review and Meta-Analysis

 , ,
, ,  ,
,  and
and 
Simple Summary
Abstract
“Life can only be understood backwards; but it must be lived forwards.”—Søren Kierkegaard
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- Population: Adults (≥18 years) with active cancer (any stage) or cancer survivors (off active treatment), experiencing psychosocial symptoms (e.g., anxiety, depression, existential distress).
- Intervention: Psychedelic agents (psilocybin, ketamine, LSD, or MDMA) administered in therapeutic settings, with or without structured psychotherapy.
- Comparator: Placebo (e.g., saline, niacin) or active control (e.g., low-dose psychedelic, midazolam).
- Outcomes: Quantitative psychosocial outcomes (e.g., validated depression/anxiety scales)
- Study Design:
- RCTs: Prioritized for meta-analysis due to reduced bias.
- Non-RCTs: Open-label, single-arm, mixed-methods, or cohort studies with pre-post assessments were included in the narrative synthesis to capture feasibility, safety, and preliminary efficacy data.
- Language: Studies available in English.
2.2. Information Sources and Search Strategy
- Terms for psychedelic therapies (e.g., “psychedelic*”, “psychedelic therapy*”, “psilocybin”, “ketamine”, “MDMA”, “LSD” and “ayahuasca”)
- Terms for psychosocial symptoms (e.g., “anxiety”, “depression”, “psychological distress”, “emotional distress”).
- Terms for cancer patients (e.g., “oncology”, “cancer survivor*”, “cancer patient*”).
- Example Search Strategy (specific to one database):
- “psychedelic*”.ab,ti.
- “psychedelic therapy*”.ab,ti.
- “hallucinogen*”.ab,ti.
- psilocybin.ab,ti.
- ketamine.ab,ti.
- ayahuasca.ab,ti.
- MDMA.ab,ti.
- anxiety.ab,ti.
- depression.ab,ti.
- “cancer patient*”.ab,ti.
- “cancer survivor*”.ab,ti.
- 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7
- 8 OR 9
- 10 OR 11
- 12 AND 13 AND 14
2.3. Study Selection
2.4. Data Extraction
- Participant Information: Sample size, mean age and standard deviation, sex distribution, cancer type, cancer stage (e.g., advanced/metastatic), and treatment context (e.g., perioperative, palliative, curative).
- Intervention Details: Psychedelic agent (e.g., psilocybin, ketamine, MDMA, LSD), dose and dosing regimen, administration route, frequency, setting, and presence or absence of structured psychotherapeutic support (e.g., preparation, integration).
- Comparator (for RCTs): Nature of the control condition (e.g., placebo, active comparator such as niacin or midazolam).
- Outcome Measures: Primary and secondary outcomes related to psychosocial distress (e.g., depression, anxiety, existential distress), including validated measurement instruments and timing of assessments (e.g., Day 1, 1 week, 6 months).
- Results: Mean and standard deviation at each timepoint for experimental and control groups (if applicable), effect estimates (e.g., Hedges’ g), response/remission rates, and p-values.
- Adverse Events: Any reported serious or non-serious adverse effects, including dropouts related to tolerability or safety.
2.5. Risk of Bias Assessment
2.6. Meta-Analyses of Controlled Psychedelic Trials
2.6.1. Study Selection and Outcome Measures
2.6.2. Data Extraction for Meta-Analysis
2.6.3. Meta-Analytic Procedures
2.6.4. Sensitivity Considerations
3. Results
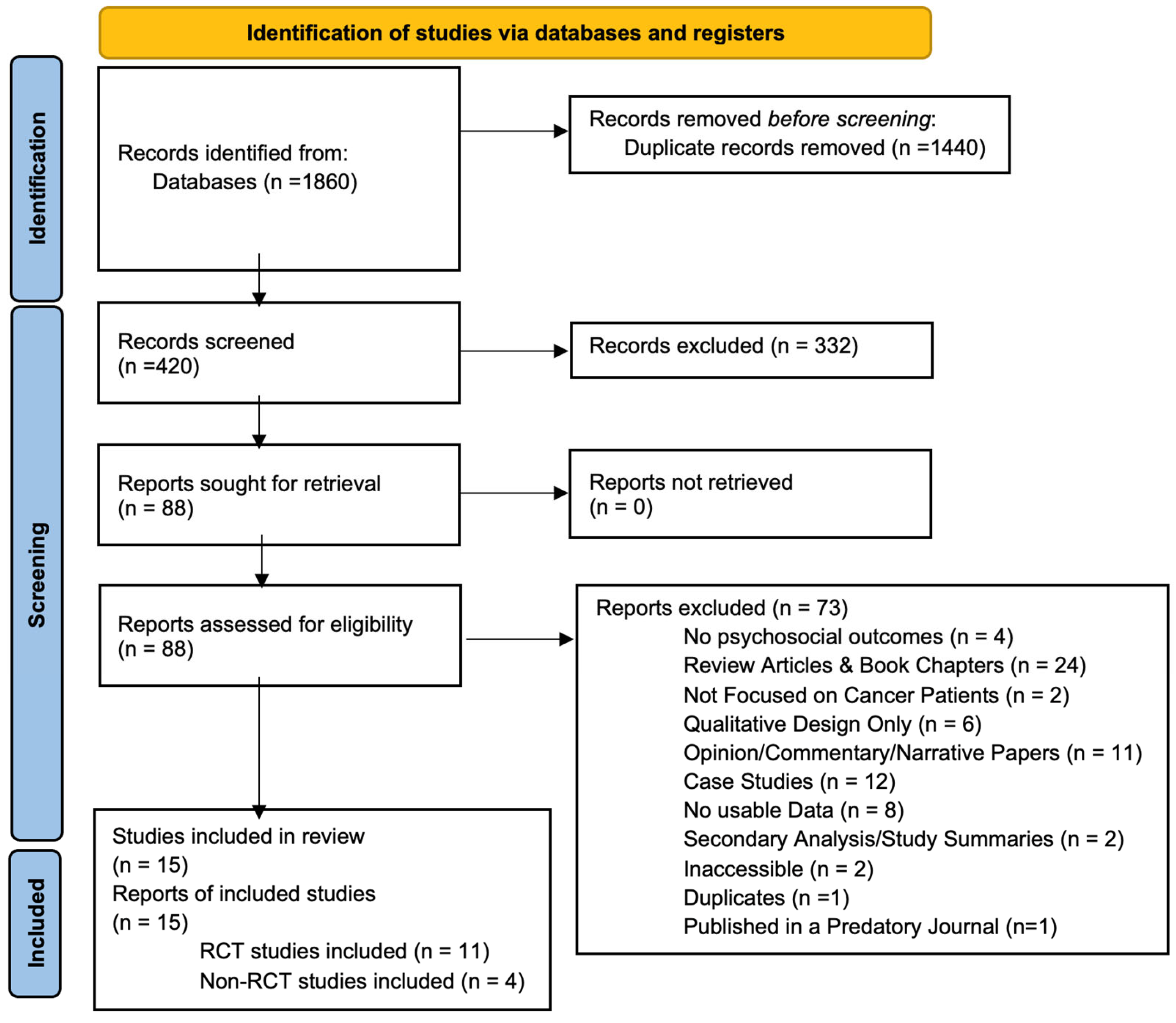
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias Assessments
3.4. Narrative Synthesis of Non-Randomized Studies and Exploratory Studies
3.4.1. Psilocybin-Assisted Therapy (Open-Label Studies)
3.4.2. Long-Term Follow-Up
3.4.3. Ketamine-Assisted Therapy (Open-Label Study)
3.4.4. Exploratory Evidence: MDMA and LSD
MDMA-Assisted Therapy
LSD-Assisted Therapy
3.5. Meta-Analytic Results
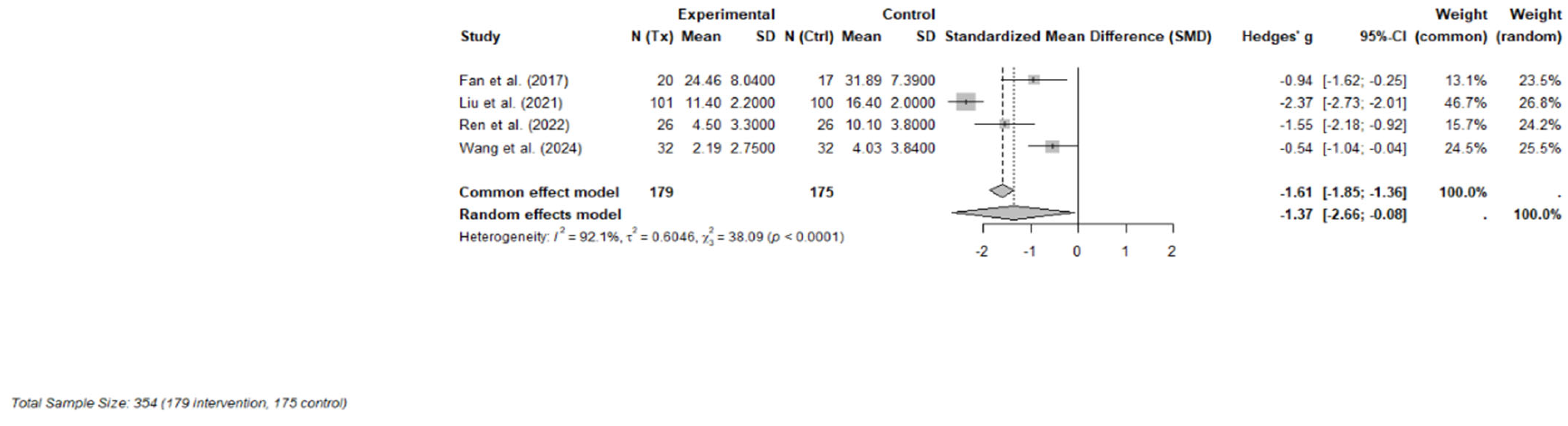
3.5.1. Ketamine
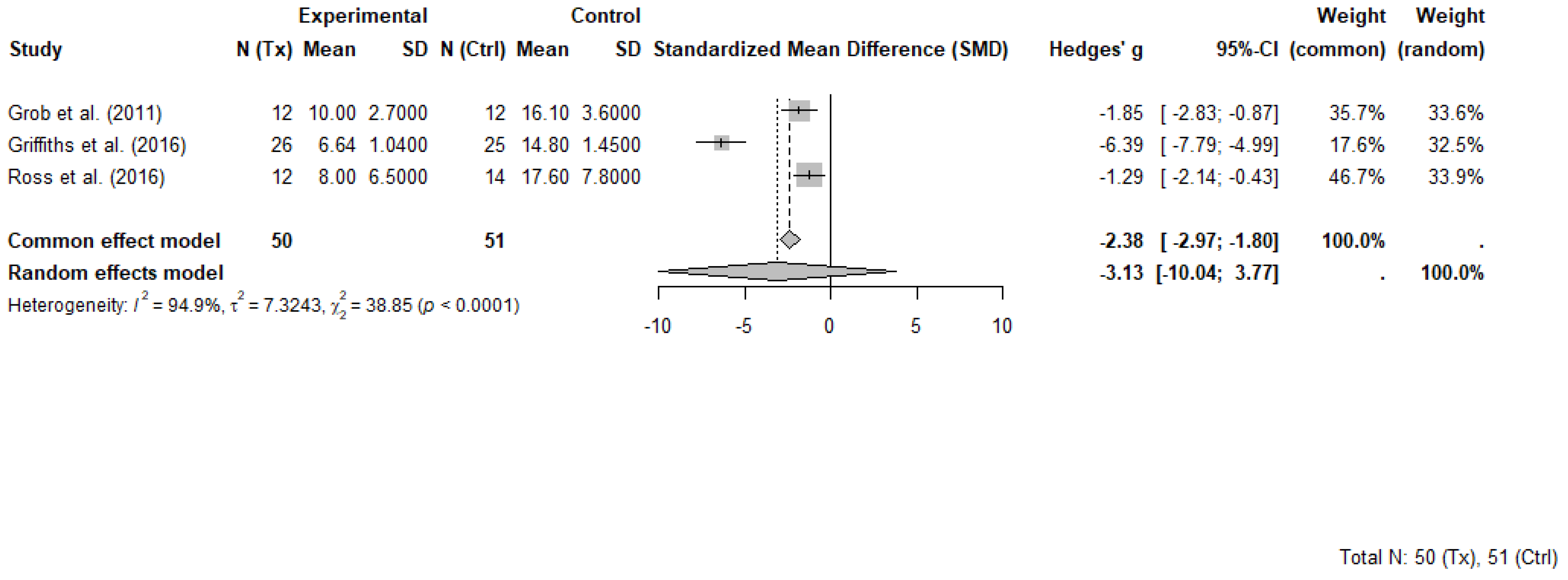
3.5.2. Psilocybin
3.6. Adverse Events Across Studies
3.7. Therapeutic Support Across Trials
4. Discussion
4.1. Divergent Therapeutic Paradigms: Experiential vs. Pharmacologic Models
4.2. The Therapeutic Container as a Mediator of Outcomes
4.3. Blinding Challenges and Comparator Heterogeneity
4.4. Clinical Implications and Context-Specific Implementation
4.5. Comparison with Existing Reviews
4.6. Limitations
4.7. Future Research Directions
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BDI | Beck Depression Inventory |
| BSI | Beck Scale for Suicidal Ideation |
| CI | Confidence Intervals |
| FACIT-Sp | Functional Assessment of Chronic Illness Therapy-Spiritual Well-Being Scale |
| FDA | U.S. Food and Drug Administration |
| GRADE | Grading of Recommendation Assessment, Development and Evaluation |
| GRID-HAMD-17 | GRID-Hamilton Depression Rating Scale |
| HAD-D | Hospital Anxiety and Depression Scale—Depression subscale |
| HADS-T | The Hospital Anxiety and Depression Scale—Total |
| HAM-D | Hamilton Depression Rating Scale |
| HAM-D-17 | 17-item Hamilton Depression Rating Scale |
| LSD | lysergic acid diethylamide |
| LTI | Life-threatening illness |
| MADRS | Montgomery-Asberg Depression Rating Scale |
| MADRS-SI | Montgomery–Åsberg Depression Rating Scale—Suicidal Ideation |
| MAPS | Multidisciplinary Association for Psychedelic Studies |
| MDD | Major Depressive Disorder |
| MDMA | 3,4-methylenedioxymethamphetamine |
| MDPI | Multidisciplinary Digital Publishing Institute |
| MEQ-30 | Mystical Experience Questionnaire |
| NIH | National Institute of Health |
| NIH-HEALS | National Institute of Health—Healing Experience of All Life Stressors |
| NMDA | N-methyl-D-aspartate |
| PAT | Psychedelic-assisted therapy |
| PHQ-9 | Patient-reported depression |
| PLWC | People living with cancer |
| PRISMA | preferred reporting items for systematic reviews and meta-analyses |
| RCT | Randomized controlled trials |
| RoB | Risk of bias |
| STAI | State-Trait Anxiety Inventory |
Appendix A
Appendix A.1. Search Strategy
- Search Words
| Concept | Synonyms |
| Psychedelic-Based Therapy | Psychedelic * [Keyword]; “psychedelic therap *” [Keyword]; “psychedelic-assisted therap *” [Keyword]; hallucinogen * [Keyword]; hallucinogens [MeSH]; psychotomimetic * [Keyword]; psilocybin [Keyword, MeSH]; ketamine [Keyword, MeSH]; ayahuasca [Keyword]; banisteriopsis [Keyword, MeSH]; LSD [Keyword]; “lysergic acid diethylamide” [Keyword, MeSH]; MDMA [Keyword]; N-Methyl-3,4-methylenedioxyamphetamine [MeSH]; DMT [Keyword]; N, N-dimethyltrptamine [MeSH]; |
| Psychosocial Symptoms | Distress [Keyword]; “psychosocial symptom *” [Keyword]; “psychological distress” [Keyword, MeSH]; “emotional distress” [Keyword]; “emotional stress” [Keyword]; anxiety [Keyword, MeSH]; “social anxiety” [Keyword]; “anxiety disorder *” [Keyword]; anxiety disorders [MeSH]; depression [Keyword, MeSH]; demoralization [Keyword, MeSH]; |
| Cancer Patients/ Survivors | Cancer [Keyword]; neoplasm * [Keyword]; neoplasms [MeSH]; carcinoma [Keyword, MeSH]; tumor * [Keyword]; tumour * [Keyword]; oncology [Keyword]; “medical oncology” [Keyword, MeSH]; “cancer survivor *” [Keyword]; cancer survivors [MeSH]; “cancer patient *” [Keyword]; patient * adj3 cancer |
| where appropriate, cancer search filter, Oncology Ovid MEDLINE 06_27_2017—Google Docs, will also be used. | |
Appendix A.2. Suggested Search Strings
Appendix A.3. MEDLINE (Ovid) Search Strategy
- 20.
- “psychedelic*”.ab,ti.
- 21.
- “psychedelic therap*”.ab,ti.
- 22.
- “psychedelic-assisted therap*”.ab,ti.
- 23.
- “hallucinogen*”.ab,ti.
- 24.
- exp Hallucinogens/
- 25.
- “psychotomimetic*”.ab,ti.
- 26.
- psilocybin.ab,ti.
- 27.
- exp Psilocybin/
- 28.
- exp Ketamine/
- 29.
- ketamine.ab,ti.
- 30.
- ayahuasca.ab,ti.
- 31.
- banisteriopsis.ab,ti.
- 32.
- exp Banisteriopsis/
- 33.
- exp Lysergic Acid Diethylamide/
- 34.
- LSD.ab,ti.
- 35.
- “lysergic acid diethylamide”.ab,ti.
- 36.
- MDMA.ab,ti.
- 37.
- exp N-Methyl-3,4-methylenedioxyamphetamine/
- 38.
- exp N,N-Dimethyltryptamine/
- 39.
- DMT.ab,ti.
- 40.
- 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20
- 41.
- distress.ab,ti.
- 42.
- “psychosocial symptom*”.ab,ti.
- 43.
- “psychological distress”.ab,ti.
- 44.
- exp Psychological Distress/
- 45.
- “emotional distress”.ab,ti.
- 46.
- “emotional stress”.ab,ti.
- 47.
- anxiety.ab,ti.
- 48.
- exp Anxiety/
- 49.
- “social anxiety”.ab,ti.
- 50.
- “anxiety disorder*”.ab,ti.
- 51.
- exp Anxiety Disorders/
- 52.
- exp Depression/
- 53.
- depression.ab,ti.
- 54.
- exp Demoralization/
- 55.
- demoralization.ab,ti.
- 56.
- 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36
- 57.
- 38. exp Neoplasms/or (oncolog* or cancer* or carcinoma* or tumor* or tumour* or neoplasm* or metasta* or malignan*).mp.
- 58.
- exp Cancer Survivors/
- 59.
- “cancer survivor*”.ab,ti.
- 60.
- “cancer patient*”.ab,ti.
- 61.
- (patient* adj3 cancer).mp. [mp = title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms, population supplementary concept word, anatomy supplementary concept word]
- 62.
- 38 or 39 or 40 or 41 or 42
- 63.
- 21 and 37 and 43
- 64.
- 21 and 43
- 65.
- 44 or 45
- 66.
- limit 46 to (english language and yr = “2000 − Current” and “all adult (19 plus years)”)
- 67.
- limit 47 to (comment or editorial or letter)
- 68.
- 47 not 48
- 69.
- remove duplicates from 49
Appendix A.4. Databases
- MEDLINE (Ovid); PsycINFO; PubMed; Cochrane Library; CINAHL; MEDLINE (Ebsco).
Appendix A.5. Limits
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Substance | Trial Type | Therapy Included | Psychotherapeutic Approach 1 | Support Type | Setting |
|---|---|---|---|---|---|---|
| Griffiths et al. (2016) [8] | Psilocybin | RCT | Yes | Non-directive supportive therapy 2 | Preparatory sessions; meeting with session monitors, monitored dosing; post-dose integration. | Academic medical center |
| Ross et al. (2016) [9] | Psilocybin | RCT | Yes | Non-directive supportive therapy 2 | Manualized prep (preparatory psychotherapy) and integration with therapist support. | Academic medical center |
| Grob et al. (2011) [31] | Psilocybin | RCT | Yes | Non-directive supportive therapy 2 | Prep sessions; therapeutic support during and after dosing. | Academic medical center |
| Fan et al. (2017) [32] | Ketamine | RCT | No | Not applicable | None | Inpatient hospital (psychiatry) |
| Liu et al. (2020) [10] | S-Ketamine | RCT | No | Not applicable | None | Post-operative ward University Hospital |
| Ren et al. (2022) [33] | Ketamine | RCT | No | Not applicable | None | Surgical ward |
| Wang et al. (2024) [34] | Esketamine | RCT | No | Not applicable | Clinical monitoring only. | Surgical unit |
| Wolfson et al. (2020) [37] | MDMA | RCT | Yes | MAPS protocol 3 | Three preparatory sessions (90 min) with co-therapy team, 2 MDMA sessions, non-directive therapy throughout sessions, 3 integration sessions. | Outpatient therapy psychiatric clinic |
| Gasser et al. (2014) [35] | LSD | RCT | Yes | Psycholytic therapy 4 | Two- prep psychotherapy sessions, 2 LSD sessions, three follow-up integration sessions. | Psychiatric outpatient clinic |
| Holze et al. (2023) [36] | LSD | RCT | Yes | Non-directive supportive therapy 2 | Prep, supported dosing, follow-up visits. | University Hospital |
| Lewis et al. (2023) [24] | Psilocybin | Open-label | Yes | Group therapy | Three group prep sessions, group dosing, and three group integration sessions; therapists on 1:1 dyad within group. | Hospital outpatient unit |
| Shnayder et al. (2023) [23] | Psilocybin | Open-label | Yes | Individual + group therapy | Prep (group + 1:1)., individual dosing, and integration (group + 1:1). | Psycho-oncology clinic |
| Agrawal et al. (2024) [25] | Psilocybin | Open-label | Yes | Group therapy with 1:1 support | Group dosing with 1:1 therapists; structured prep/integration (group + 1:1). | Community oncology center |
| Rosenblat et al. (2023) [12] | Ketamine | Open-label | No | Not applicable | Clinical monitoring; supportive check-ins. | Palliative care unit |
References
- Carlson, L.E.; Toivonen, K.; Subnis, U. Integrative Approaches to Stress Management. Cancer J. 2019, 25, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Andersen, B.L.; Lacchetti, C.; Ashing, K.; Berek, J.S.; Berman, B.S.; Bolte, S.; Dizon, D.S.; Given, B.; Nekhlyudov, L.; Pirl, W.; et al. Management of Anxiety and Depression in Adult Survivors of Cancer: ASCO Guideline Update. J. Clin. Oncol. 2023, 41, 3426–3453. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.E.; Ismaila, N.; Addington, E.L.; Asher, G.N.; Atreya, C.; Balneaves, L.G.; Bradt, J.; Fuller-Shavel, N.; Goodman, J.; Hoffman, C.J.; et al. Integrative Oncology Care of Symptoms of Anxiety and Depression in Adults With Cancer: Society for Integrative Oncology-ASCO Guideline. J. Clin. Oncol. 2023, 41, 4562–4591. [Google Scholar] [CrossRef] [PubMed]
- Lowe, H.; Toyang, N.; Steele, B.; Valentine, H.; Grant, J.; Ali, A.; Ngwa, W.; Gordon, L. The Therapeutic Potential of Psilocybin. Molecules 2021, 26, 2948. [Google Scholar] [CrossRef]
- Bahji, A.; Lunsky, I.; Gutierrez, G.; Vazquez, G. Efficacy and Safety of Four Psychedelic-Assisted Therapies for Adults with Symptoms of Depression, Anxiety, and Posttraumatic Stress Disorder: A Systematic Review and Meta-Analysis. J. Psychoact. Drugs 2025, 57, 1–16. [Google Scholar] [CrossRef]
- De Gregorio, D.; Aguilar-Valles, A.; Preller, K.H.; Heifets, B.D.; Hibicke, M.; Mitchell, J.; Gobbi, G. Hallucinogens in Mental Health: Preclinical and Clinical Studies on LSD, Psilocybin, MDMA, and Ketamine. J. Neurosci. 2021, 41, 891–900. [Google Scholar] [CrossRef]
- Yao, Y.; Guo, D.; Lu, T.S.; Liu, F.L.; Huang, S.H.; Diao, M.Q.; Li, S.X.; Zhang, X.J.; Kosten, T.R.; Shi, J.; et al. Efficacy and safety of psychedelics for the treatment of mental disorders: A systematic review and meta-analysis. Psychiatry Res. 2024, 335, 115886. [Google Scholar] [CrossRef]
- Griffiths, R.R.; Johnson, M.W.; Carducci, M.A.; Umbricht, A.; Richards, W.A.; Richards, B.D.; Cosimano, M.P.; Klinedinst, M.A. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: A randomized double-blind trial. J. Psychopharmacol. 2016, 30, 1181–1197. [Google Scholar] [CrossRef]
- Ross, S.; Bossis, A.; Guss, J.; Agin-Liebes, G.; Malone, T.; Cohen, B.; Mennenga, S.E.; Belser, A.; Kalliontzi, K.; Babb, J.; et al. Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: A randomized controlled trial. J. Psychopharmacol. 2016, 30, 1165–1180. [Google Scholar] [CrossRef]
- Liu, P.; Li, P.; Li, Q.; Yan, H.; Shi, X.; Liu, C.; Zhang, Y.; Peng, S. Effect of Pretreatment of S-Ketamine On Postoperative Depression for Breast Cancer Patients. J. Investig. Surg. 2020, 34, 883–888. [Google Scholar] [CrossRef]
- Guo, J.; Qiu, D.; Gu, H.W.; Wang, X.M.; Hashimoto, K.; Zhang, G.F.; Yang, J.J. Efficacy and safety of perioperative application of ketamine on postoperative depression: A meta-analysis of randomized controlled studies. Mol. Psychiatry 2023, 28, 2266–2276. [Google Scholar] [CrossRef]
- Rosenblat, J.D.; Leon-Carlyle, M.; Ali, S.; Husain, M.I.; McIntyre, R.S. Antidepressant Effects of Psilocybin in the Absence of Psychedelic Effects. Am. J. Psychiatry 2023, 180, 395–396. [Google Scholar] [CrossRef] [PubMed]
- Ko, K.; Knight, G.; Rucker, J.J.; Cleare, A.J. Psychedelics, Mystical Experience, and Therapeutic Efficacy: A Systematic Review. Front. Psychiatry 2022, 13, 917199. [Google Scholar] [CrossRef] [PubMed]
- Roseman, L.; Haijen, E.; Idialu-Ikato, K.; Kaelen, M.; Watts, R.; Carhart-Harris, R. Emotional breakthrough and psychedelics: Validation of the Emotional Breakthrough Inventory. J. Psychopharmacol. 2019, 33, 1076–1087. [Google Scholar] [CrossRef] [PubMed]
- Rucker, J.J.H.; Iliff, J.; Nutt, D.J. Psychiatry & the psychedelic drugs. Past, present & future. Neuropharmacology 2018, 142, 200–218. [Google Scholar] [CrossRef]
- Kucsera, A.; Suppes, T.; Haug, N.A. Psychologists’ and psychotherapists’ knowledge, attitudes, and clinical practices regarding the therapeutic use of psychedelics. Clin. Psychol. Psychother. 2023, 30, 1369–1379. [Google Scholar] [CrossRef]
- Schipper, S.; Nigam, K.; Schmid, Y.; Piechotta, V.; Ljuslin, M.; Beaussant, Y.; Schwarzer, G.; Boehlke, C. Psychedelic-assisted therapy for treating anxiety, depression, and existential distress in people with life-threatening diseases. Cochrane Database Syst. Rev. 2024, 9, Cd015383. [Google Scholar] [CrossRef]
- Maia, L.O.; Beaussant, Y.; Garcia, A.C.M. The Therapeutic Potential of Psychedelic-assisted Therapies for Symptom Control in Patients Diagnosed With Serious Illness: A Systematic Review. J. Pain Symptom Manag. 2022, 63, e725–e738. [Google Scholar] [CrossRef]
- Schimmers, N.; Breeksema, J.J.; Smith-Apeldoorn, S.Y.; Veraart, J.; van den Brink, W.; Schoevers, R.A. Psychedelics for the treatment of depression, anxiety, and existential distress in patients with a terminal illness: A systematic review. Psychopharmacology 2022, 239, 15–33. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- National Heart Lung and Blood Institute. Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 10 February 2025).
- Shnayder, S.; Ameli, R.; Sinaii, N.; Berger, A.; Agrawal, M. Psilocybin-assisted therapy improves psycho-social-spiritual well-being in cancer patients. J. Affect. Disord. 2023, 323, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Lewis, B.R.; Garland, E.L.; Byrne, K.; Durns, T.; Hendrick, J.; Beck, A.; Thielking, P. HOPE: A Pilot Study of Psilocybin Enhanced Group Psychotherapy in Patients With Cancer. J. Pain Symptom Manag. 2023, 66, 258–269. [Google Scholar] [CrossRef]
- Agrawal, M.; Richards, W.; Beaussant, Y.; Shnayder, S.; Ameli, R.; Roddy, K.; Stevens, N.; Richards, B.; Schor, N.; Honstein, H.; et al. Psilocybin-assisted group therapy in patients with cancer diagnosed with a major depressive disorder. Cancer 2024, 130, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- PlotDigitizer. PlotDigitizer: Version 3.1.6. PlotDigitizer.com 2025. Available online: https://plotdigitizer.com (accessed on 27 January 2025).
- Schwarzer, G. Meta: An R Package for Meta-Analysis, 8.0-2; CRAN: Vienna, Austria, 2025. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023. [Google Scholar]
- RStudio Team. RStudio: Integrated Development for R; RStudio, PBC: Boston, MA, USA, 2020. [Google Scholar]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Grob, C.S.; Danforth, A.L.; Chopra, G.S.; Hagerty, M.; McKay, C.R.; Halberstad, A.L.; Greer, G.R. Pilot study of psilocybin treatment for anxiety in patients with advanced-stage cancer. Arch. Gen. Psychiatry 2011, 68, 71–78. [Google Scholar] [CrossRef]
- Fan, W.; Yang, H.; Sun, Y.; Zhang, J.; Li, G.; Zheng, Y.; Liu, Y. Ketamine rapidly relieves acute suicidal ideation in cancer patients: A randomized controlled clinical trial. Oncotarget 2017, 8, 2356–2360. [Google Scholar] [CrossRef]
- Ren, Q.; Hua, L.; Zhou, X.; Cheng, Y.; Lu, M.; Zhang, C.; Guo, J.; Xu, H. Effects of a Single Sub-Anesthetic Dose of Ketamine on Postoperative Emotional Responses and Inflammatory Factors in Colorectal Cancer Patients. Front. Pharmacol. 2022, 13, 818822. [Google Scholar] [CrossRef]
- Wang, H.; Te, R.; Zhang, J.; Su, Y.; Zhou, H.; Guo, N.; Chi, D.; Huang, W. Effects of a single subanesthetic dose of esketamine on postoperative subthreshold depressive symptoms in patients undergoing unilateral modified radical mastectomy: A randomised, controlled, double-blind trial. BMC Psychiatry 2024, 24, 315. [Google Scholar] [CrossRef]
- Gasser, P.; Holstein, D.; Michel, Y.; Doblin, R.; Yazar-Klosinski, B.; Passie, T.; Brenneisen, R. Safety and efficacy of lysergic acid diethylamide-assisted psychotherapy for anxiety associated with life-threatening diseases. J. Nerv. Ment. Dis. 2014, 202, 513–520. [Google Scholar] [CrossRef]
- Holze, F.; Gasser, P.; Müller, F.; Dolder, P.C.; Liechti, M.E. Lysergic Acid Diethylamide-Assisted Therapy in Patients With Anxiety With and Without a Life-Threatening Illness: A Randomized, Double-Blind, Placebo-Controlled Phase II Study. Biol. Psychiatry 2023, 93, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, P.E.; Andries, J.; Feduccia, A.A.; Jerome, L.; Wang, J.B.; Williams, E.; Carlin, S.C.; Sola, E.; Hamilton, S.; Yazar-Klosinski, B.; et al. MDMA-assisted psychotherapy for treatment of anxiety and other psychological distress related to life-threatening illnesses: A randomized pilot study. Sci. Rep. 2020, 10, 20442. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, M.; Emanuel, E.; Richards, B.; Richards, W.; Roddy, K.; Thambi, P. Assessment of Psilocybin Therapy for Patients With Cancer and Major Depression Disorder. JAMA Oncol. 2023, 9, 864–866. [Google Scholar] [CrossRef] [PubMed]
- Ross, S.; Agin-Liebes, G.; Lo, S.; Zeifman, R.J.; Ghazal, L.; Benville, J.; Franco Corso, S.; Bjerre Real, C.; Guss, J.; Bossis, A.; et al. Acute and Sustained Reductions in Loss of Meaning and Suicidal Ideation Following Psilocybin-Assisted Psychotherapy for Psychiatric and Existential Distress in Life-Threatening Cancer. ACS Pharmacol. Transl. Sci. 2021, 4, 553–562. [Google Scholar] [CrossRef]
- Agin-Liebes, G.I.; Malone, T.; Yalch, M.M.; Mennenga, S.E.; Ponté, K.L.; Guss, J.; Bossis, A.P.; Grigsby, J.; Fischer, S.; Ross, S. Long-term follow-up of psilocybin-assisted psychotherapy for psychiatric and existential distress in patients with life-threatening cancer. J. Psychopharmacol. 2020, 34, 155–166. [Google Scholar] [CrossRef]
- Griffiths, R.R.; Richards, W.A.; McCann, U.; Jesse, R. Psilocybin can occasion mystical-type experiences having substantial and sustained personal meaning and spiritual significance. Psychopharmacology 2006, 187, 268–283. [Google Scholar] [CrossRef]
- FDA. FDA Briefing Document: NDA 215455—Midomafetamine (MDMA) for PTSD; FDA: Silver Spring, MD, USA, 2024.
- Carhart-Harris, L.R.; Bolstridge, M.; Day, J.M.C.; Rucker, J.; Watts, R.; Erritzoe, E.D.; Kaelen, M.; Giribaldi, B.; Bloomfield, M.; Pilling, S.; et al. Psilocybin with psychological support for treatment-resistant depression: Six-month follow-up. Psychopharmacology 2018, 235, 399–408. [Google Scholar] [CrossRef]
- Pedro, J.; Monteiro-Reis, S.; Carvalho-Maia, C.; Henrique, R.; Jerónimo, C.; Silva, E.R. Evidence of psychological and biological effects of structured Mindfulness-Based Interventions for cancer patients and survivors: A meta-review. Psychooncology 2021, 30, 1836–1848. [Google Scholar] [CrossRef]
- Yaden, D.B.; Potash, J.B.; Griffiths, R.R. Preparing for the Bursting of the Psychedelic Hype Bubble. JAMA Psychiatry 2022, 79, 943–944. [Google Scholar] [CrossRef]
- Pallavicini, C.; Vilas, M.G.; Villarreal, M.; Zamberlan, F.; Muthukumaraswamy, S.; Nutt, D.; Carhart-Harris, R.; Tagliazucchi, E. Spectral signatures of serotonergic psychedelics and glutamatergic dissociatives. Neuroimage 2019, 200, 281–291. [Google Scholar] [CrossRef]
- Marguilho, M.; Figueiredo, I.; Castro-Rodrigues, P. A unified model of ketamine’s dissociative and psychedelic properties. J. Psychopharmacol. 2023, 37, 14–32. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, P.; Vaid, G. Ketamine-assisted psychotherapy, psychedelic methodologies, and the impregnable value of the subjective-a new and evolving approach. Front. Psychiatry 2024, 15, 1209419. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, A.; Moghaddam, B. Licit use of illicit drugs for treating depression: The pill and the process. J. Clin. Investig. 2024, 134, e180217. [Google Scholar] [CrossRef] [PubMed]
- Sholevar, R.; Peteet, J.; Sanders, J.; Beaussant, Y. Disruption as an opportunity or threat: A qualitative analysis of factors influencing the attitudes of experts in serious illness care toward psychedelic-assisted therapies. Palliat. Support. Care 2023, 21, 967–972. [Google Scholar] [CrossRef]
- Muthukumaraswamy, S.D.; Anna, F.; Lumley, T. Blinding and expectancy confounds in psychedelic randomized controlled trials. Expert Rev. Clin. Pharmacol. 2021, 14, 1133–1152. [Google Scholar] [CrossRef]
- Aday, J.S.; Simonsson, O.; Schindler, E.A.D.; D’Souza, D.C. Addressing blinding in classic psychedelic studies with innovative active placebos. Int. J. Neuropsychopharmacol. 2025, 28, pyaf023. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Goodwin, G.M. The Therapeutic Potential of Psychedelic Drugs: Past, Present, and Future. Neuropsychopharmacology 2017, 42, 2105–2113. [Google Scholar] [CrossRef]
- Bogenschutz, M.P.; Ross, S.; Bhatt, S.; Baron, T.; Forcehimes, A.A.; Laska, E.; Mennenga, S.E.; O’Donnell, K.; Owens, L.T.; Podrebarac, S.; et al. Percentage of Heavy Drinking Days Following Psilocybin-Assisted Psychotherapy vs Placebo in the Treatment of Adult Patients With Alcohol Use Disorder: A Randomized Clinical Trial. JAMA Psychiatry 2022, 79, 953–962. [Google Scholar] [CrossRef]
- Wilkinson, S.T.; Farmer, C.; Ballard, E.D.; Mathew, S.J.; Grunebaum, M.F.; Murrough, J.W.; Sos, P.; Wang, G.; Gueorguieva, R.; Zarate, C.A., Jr. Impact of midazolam vs. saline on effect size estimates in controlled trials of ketamine as a rapid-acting antidepressant. Neuropsychopharmacology 2019, 44, 1233–1238. [Google Scholar] [CrossRef]
- Sener, S.; Eken, C.; Schultz, C.H.; Serinken, M.; Ozsarac, M. Ketamine with and without midazolam for emergency department sedation in adults: A randomized controlled trial. Ann. Emerg. Med. 2011, 57, 109–114.e102. [Google Scholar] [CrossRef]
- Suzuki, M.; Tsueda, K.; Lansing, P.S.; Tolan, M.M.; Fuhrman, T.M.; Sheppard, R.A.; Hurst, H.E.; Lippmann, S.B. Midazolam attenuates ketamine-induced abnormal perception and thought process but not mood changes. Can. J. Anaesth. 2000, 47, 866–874. [Google Scholar] [CrossRef] [PubMed]
- Lii, T.R.; Smith, A.E.; Flohr, J.R.; Okada, R.L.; Nyongesa, C.A.; Cianfichi, L.J.; Hack, L.M.; Schatzberg, A.F.; Heifets, B.D. Randomized trial of ketamine masked by surgical anesthesia in patients with depression. Nat. Ment. Health 2023, 1, 876–886. [Google Scholar] [CrossRef] [PubMed]
- Carbonaro, T.M.; Bradstreet, M.P.; Barrett, F.S.; Maclean, K.A.; Jesse, R.; Johnson, M.W.; Griffiths, R.R.; Griffiths, R. Survey study of challenging experiences after ingesting psilocybin mushrooms: Acute and enduring positive and negative consequences HHS Public Access. J. Psychopharmacol. 2016, 30, 1268–1278. [Google Scholar] [CrossRef]
- Johnson, M.W.; MacLean, K.A.; Reissig, C.J.; Prisinzano, T.E.; Griffiths, R.R. Human psychopharmacology and dose-effects of salvinorin A, a kappa opioid agonist hallucinogen present in the plant Salvia divinorum. Drug Alcohol. Depend. 2011, 115, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Earleywine, M.; Ueno, L.F.; Mian, M.N.; Altman, B.R. Cannabis-induced oceanic boundlessness. J. Psychopharmacol. 2021, 35, 841–847. [Google Scholar] [CrossRef]
- Reissig, C.J.; Carter, L.P.; Johnson, M.W.; Mintzer, M.Z.; Klinedinst, M.A.; Griffiths, R.R. High doses of dextromethorphan, an NMDA antagonist, produce effects similar to classic hallucinogens. Psychopharmacology 2012, 223, 1–15. [Google Scholar] [CrossRef]
- Urrutia, J.; Anderson, B.T.; Belouin, S.J.; Berger, A.; Griffiths, R.R.; Grob, C.S.; Henningfield, J.E.; Labate, B.C.; Maier, L.J.; Maternowska, M.C.; et al. Psychedelic Science, Contemplative Practices, and Indigenous and Other Traditional Knowledge Systems: Towards Integrative Community-Based Approaches in Global Health. J. Psychoact. Drugs 2023, 55, 523–538. [Google Scholar] [CrossRef]
- Palitsky, R.; Kaplan, D.M.; Peacock, C.; Zarrabi, A.J.; Maples-Keller, J.L.; Grant, G.H.; Dunlop, B.W.; Raison, C.L. Importance of Integrating Spiritual, Existential, Religious, and Theological Components in Psychedelic-Assisted Therapies. JAMA Psychiatry 2023, 80, 743–749. [Google Scholar] [CrossRef]
- Wen, A.; Singhal, N.; Jones, B.D.M.; Zeifman, R.J.; Mehta, S.; Shenasa, M.A.; Blumberger, D.M.; Daskalakis, Z.J.; Weissman, C.R. A Systematic Review of Study Design and Placebo Controls in Psychedelic Research. Psychedelic Med. 2024, 2, 15–24. [Google Scholar] [CrossRef]
- Riggs, L.M.; Gould, T.D. Ketamine and the Future of Rapid-Acting Antidepressants. Annu. Rev. Clin. Psychol. 2021, 17, 207–231. [Google Scholar] [CrossRef]
- Wilkinson, S.T.; Toprak, M.; Turner, M.S.; Levine, S.P.; Katz, R.B.; Sanacora, G. A Survey of the Clinical, Off-Label Use of Ketamine as a Treatment for Psychiatric Disorders. Am. J. Psychiatry 2017, 174, 695–696. [Google Scholar] [CrossRef] [PubMed]
- FDA. FDA Warns Patients and Health Care Providers About Potential Risks Associated with Compounded Ketamine Products, Including Oral Formulations, for the Treatment of Psychiatric Disorders; FDA: Silver Spring, MD, USA, 2023.
- Aslam, A.M.; Shinozuka, K.; Muir, O.; Tabaac, B.J. Mapping the Use of Ketamine in Treatment-Resistant Depression and Other Psychiatric Disorders: A Scoping Review of Practice Patterns, Efficacy, and Patient Demographic Trends. Am. J. Ther. 2025, 32, e242–e246. [Google Scholar] [CrossRef] [PubMed]
- Chrenek, C.; Duong, B.; Khullar, A.; McRee, C.; Thomas, R.; Swainson, J. Use of ketamine for treatment resistant depression: Updated review of literature and practical applications to a community ketamine program in Edmonton, Alberta, Canada. Front. Psychiatry 2023, 14, 1283733. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.; Gale, C.; Sarma, S.; Smith, J.; Bayes, A.; Loo, C. Royal Australian and New Zealand College of Psychiatrists professional practice guidelines for the use of ketamine in psychiatric practice. Aust. N. Z. J. Psychiatry 2025, 59, 576–587. [Google Scholar] [CrossRef]
- Mills, C. The Status of Ketamine Therapy in Canada. Available online: https://diplomatconsulting.com/the-status-of-ketamine-therapy-in-canada/ (accessed on 15 April 2025).
- Health, F.T. Ketamine Therapy Cost in Canada: Exploring Affordable Options. Available online: https://fieldtriphealth.ca/ketamine-therapy-cost-in-canada/ (accessed on 15 April 2025).
- Clinic, N.K.W. Ketamine Therapy Pricing. Available online: https://neuconnectionswellness.com/ketamine-therapy-pricing/ (accessed on 15 April 2025).
- Kim, K.; Yusuf, A.; Sud, A.; Persaud, N.; Kirubarajan, A.; Moller, M.; Lloyd, T.; O’Neill, B. Critical appraisal of evidence supporting prescription of psychedelics from clinic websites in Ontario, Canada. PLoS ONE 2024, 19, e0309911. [Google Scholar] [CrossRef]
- Ross, S. Therapeutic use of classic psychedelics to treat cancer-related psychiatric distress. Int. Rev. Psychiatry 2018, 30, 317–330. [Google Scholar] [CrossRef]
- Grof, S.; Halifax, J. The Human Encounter with Death; Souvenir Press: London, UK, 1978. [Google Scholar]
- Grof, S.; Goodman, L.E.; Richards, W.A.; Kurland, A.A. LSD-assisted psychotherapy in patients with terminal cancer. Int. Pharmacopsychiatry 1973, 8, 129–144. [Google Scholar] [CrossRef]

| Criteria | Rosenblat et al., 2023 [12] | Shnayder et al., 2023 [23] | Lewis et al., 2023 [24] | Agrawal et al., 2024 [25] |
|---|---|---|---|---|
| Study objectives stated | Yes | Yes | Yes | Yes |
| Study population defined | Yes | Yes | Yes | Yes |
| Study participants representative of clinical populations of interest | Yes | Yes | Yes | Yes |
| All eligible participants enrolled | No | No | No | No |
| Sample size sufficient and/or described | No | No | No | No |
| Intervention clearly described | Yes | Yes | Yes | Yes |
| Outcome measures clearly described, valid, reliable | Yes | Yes | Yes | Yes |
| Blinding of outcome assessors | No | No | No | No |
| Follow-up rate | Yes | Yes | Yes | Yes |
| Statistical analysis | Yes | Yes | Yes | Yes |
| Multiple outcome measures | No | No | No | No |
| Group-level interventions and individual-level outcome efforts | N.A. | N.A. | N.A. | N.A. |
| Overall rating | Fair | Fair | Fair | Fair |
| Outcome | No. of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Overall Certainty | Effect Estimate (SMD [95% CI]) |
|---|---|---|---|---|---|---|---|---|
| Reduction in psychosocial symptoms (e.g., depression, anxiety) with ketamine or esketamine vs. Control. | 4 | RCTs | Moderate 1 | Serious 2 | Not serious | Serious 3 | Low | −1.37 [−2.66 to −0.08] |
| Reduction in psychosocial symptoms (e.g., depression, anxiety, existential distress) with psilocybin vs. Control. | 3 | RCTs | Moderate 4 | Serious 5 | Not serious | Serious 6 | Low | −3.13 [−10.04 to 3.77] |
| Study (Author, Year) | Sample Size (N) | Male (%) | Mean Age (SD) | Condition | Psychedelic Agent & Dose | Comparator | Therapy Included | Primary Outcome Measures | Evaluation Timepoints | Key Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| Grob et al., 2011 [31] | 12 | 8% | 36–58 | Advanced cancer-related anxiety | Psilocybin 0.2 mg/kg | Niacin (Vitamin B3) | Yes | BDI, POMS, STAI | 6 months | Reduction in anxiety sustained at 6 months. |
| Griffiths et al., 2016 [8] | 51 | 51% | 56.3 (±1.4) | Cancer-related depression/ anxiety | Psilocybin 1 or 3 mg/70 kg (low) & 22 or 30 mg/70 kg (high) | Low-dose Psilocybin | Yes | GRID-HAM-D-17, HAM-A | 6 months | Large effect size for depression & anxiety reduction (p < 0.001). |
| Ross et al., 2016 [9] | 29 | 38% | 56.28 (±12.93) | Cancer-related depression/ anxiety | Psilocybin 0.3 mg/kg | Niacin 250 mg | Yes | HADS, BDI, STAI | 6.5 months | 60–80% sustained reduction in anxiety & depression. |
| Fan et al., 2017 [32] | 39 | 32% | 45.78 (±14.4) | Cancer with suicidal ideation | Ketamine 0.5 mg/kg IV | Midazolam 0.05 mg/kg | No | BSI, MADRS-SI | Day 1, 3, 7 | Significant reduction in suicidal ideation (p < 0.001). |
| Liu et al., 2020 [10] | 303 | 0% | 47.43 (±9.4) | Breast cancer and depression | S-Ketamine 0.125 mg/kg IV | Saline | No | HAMD-17, BDNF, 5-HT | 3 days, 1 week, 1 month | Lower depression scores & higher BDNF & 5-HT levels. |
| Ren et al., 2022 [33] | 104 | 51% | 61.35 (±7.24) | Colorectal cancer surgery | Ketamine 0.1–0.3 mg/kg IV | Saline | No | HADS, QoR-40, IL-6, IL-8 | 24, 48, 72 h | Improvement in anxiety, depression, and inflammatory markers. |
| Wang et al., 2024 [34] | 64 | 0% | 42.05 (±5.81) | Breast cancer and depressive symptoms | Esketamine 0.2 mg/kg IV | Saline | No | PHQ-9, VAS | 1, 3, 7, 30 days | PHQ-9 significantly lower at post-op day 1 (p = 0.047). |
| Gasser et al., 2014 [35] | 12 | 50% | 51.7 (±9.1) | Life-threatening illness with anxiety | LSD 200 µg | LSD 20 µg (active placebo) | Yes | STAI, EORTC-QLQ-30, HADS | 2 months, 12 months | Large effect size for anxiety reduction (p = 0.033). |
| Holze et al., 2023 [36] | 42 | 52% | 45 (±12) | Anxiety (with/without life-threatening illness) | LSD 200 µg | Placebo | Yes | STAI-G, BDI, HAM-D-21 | 16 weeks | Significant reductions in anxiety (p = 0.007) & depression (p = 0.0004). |
| Wolfson et al., 2020 [37] | 18 | 22.2% | 54.9 (±7.9) | Life-threatening illness with anxiety | MDMA 125 mg | Placebo | Yes | STAI, BDI-II, PSQI | 1 month, 2 months | Reduction in anxiety sustained at 2-month follow-up. |
| Lewis et al., 2023 [24] | 12 | 33% | 48.2 (±11.5) | Cancer patients with DSM-5 depressive disorder | Psilocybin 25 mg oral, group session | None (open-label, single-arm study) | Yes | HAMD-17 | Baseline; 2 weeks; 26 weeks | HAM-D dropped from 21.5 to 10.1 (2 weeks) and 14.8 (26 weeks) (p < 0.001, p = 0.006). |
| Shnayder et al., 2023 [23] | 30 | 30% | 56 (±12) | Cancer patients with MDD | Psilocybin 25 mg oral | None (open-label, single-arm study) | Yes | NIH-HEALS | Baseline; 1, 3, 8 weeks | NIH-HEALS increased by ~16.4 points at 8 weeks (p < 0.001). |
| Agrawal et al., 2024 [25] | 30 | 30% | 56 (±12) | Curable/metastatic cancer with MDD | Psilocybin 25 mg oral, group session | None (open-label, single-arm study) | Yes | MADRS | Baseline; 1-week; 8 weeks | MADRS reduced by 19.1 points by Week 8 (p < 0.0001). |
| Rosenblat et al., 2023 [12] | 20 | 35% | 58.4 (±17.2) | Advanced cancer with MDD (palliative care) | Intranasal Ketamine was administered in three flexible doses (50–150 mg) over one week | None (open-label, single-arm study) | No | MADRS | Baseline; Day 8; Day 14 | 70% response, 45% remission; MADRS fell ~20 points by Day 8 (p < 0.001). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schuman, H.D.M.; Savard, C.; Mina, R.; Barkova, S.; Conradi, H.S.W.; Deleemans, J.M.; Carlson, L.E. Psychedelic-Assisted Therapies for Psychosocial Symptoms in Cancer: A Systematic Review and Meta-Analysis. Curr. Oncol. 2025, 32, 380. https://doi.org/10.3390/curroncol32070380
Schuman HDM, Savard C, Mina R, Barkova S, Conradi HSW, Deleemans JM, Carlson LE. Psychedelic-Assisted Therapies for Psychosocial Symptoms in Cancer: A Systematic Review and Meta-Analysis. Current Oncology. 2025; 32(7):380. https://doi.org/10.3390/curroncol32070380
Chicago/Turabian StyleSchuman, Haley D. M., Chantal Savard, Raèf Mina, Sofia Barkova, Hanna S. W. Conradi, Julie M. Deleemans, and Linda E. Carlson. 2025. "Psychedelic-Assisted Therapies for Psychosocial Symptoms in Cancer: A Systematic Review and Meta-Analysis" Current Oncology 32, no. 7: 380. https://doi.org/10.3390/curroncol32070380
APA StyleSchuman, H. D. M., Savard, C., Mina, R., Barkova, S., Conradi, H. S. W., Deleemans, J. M., & Carlson, L. E. (2025). Psychedelic-Assisted Therapies for Psychosocial Symptoms in Cancer: A Systematic Review and Meta-Analysis. Current Oncology, 32(7), 380. https://doi.org/10.3390/curroncol32070380