The Relationship Between Obesity and Cancer: Epidemiology, Pathophysiology, and the Effect of Obesity Treatment on Cancer

 and
and
Abstract
1. Background
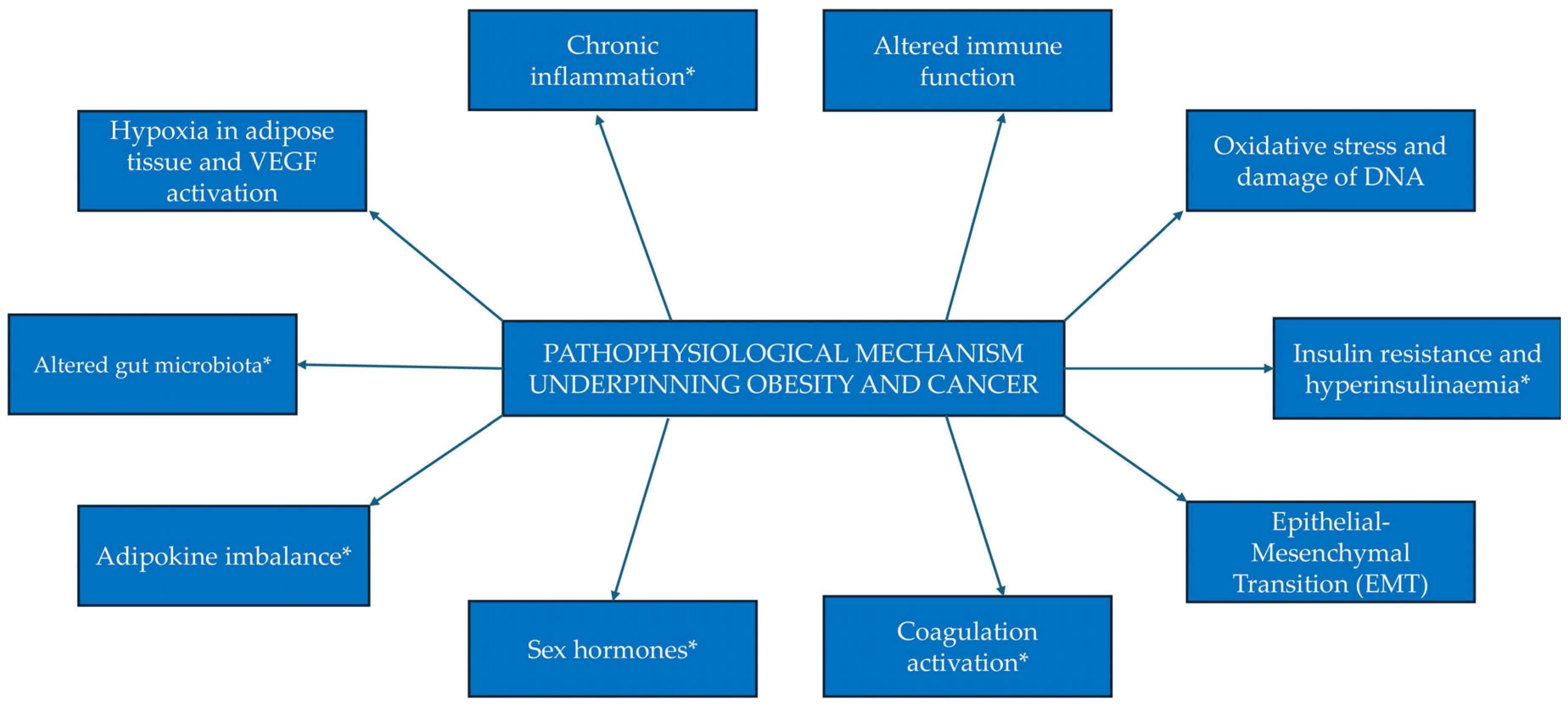
2. Pathophysiology
2.1. Sex Hormones
2.2. Insulin and IGF
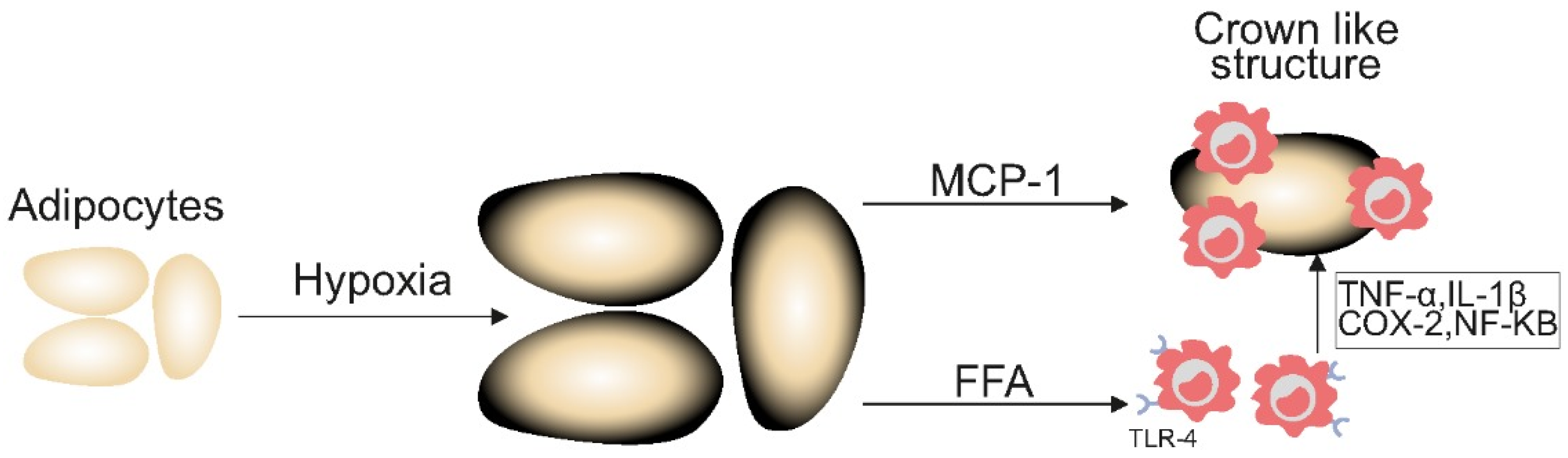
2.3. Chronic Inflammation
2.4. Adipokine Imbalance
2.5. Coagulation System
2.6. Gut Microbiota
3. Obesity and Cancer Outcomes
3.1. Obesity and Cancer Survival and Recurrence
3.2. Obesity and Cancer Treatment-Related Adverse Effects

{kind=link}
{kind=link}
{kind=link}
| Cancer Treatment Side Effect | Impact of Obesity | Underlying Mechanism |
|---|---|---|
| Lymphoedema | Increased risk proportional to BMI [63] | |
| Chemotherapy associated peripheral neuropathy | More common in patients with obesity [65,66] | |
| Cardiotoxicity | 47% increased risk in women receiving Trastuzamab and anthracyclines [68] | |
| Radiation-related dermatitis | 11% increased risk in those with BMI > 25 kg/m2 [69] |
|
| Urinary and Bowel Incontinence (post-radiation) | Increased risk in prostate and gynaecological cancers [70,71] | Excess skin folds, friction, and moisture accumulation [71,72]
|
| Surgical complications | Increased risk of infection and wound dehiscence [73] |
|
4. Efficacy and Toxicity of Cancer Treatments in Patients with Obesity
4.1. Chemotherapy
4.2. Molecular Targeted Therapies
4.3. Immune Checkpoint Inhibitors
5. Weight Loss Interventions and Cancer Risk
5.1. Bariatric Surgery and Cancer Risk
5.2. Use of GLP-1 Receptor Agonists in Obesity and Association with Cancer
6. Obesity as a Presenting Feature of Cancer
7. Conclusions and Future Directions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 21 October 2024).
- Rubino, F.; Cummings, D.E.; Eckel, R.H.; Cohen, R.V.; Wilding, J.P.H.; Brown, W.A.; Stanford, F.C.; Batterham, R.L.; Farooqi, I.S.; Farpour-Lambert, N.J.; et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025, 13, 221–262. [Google Scholar] [CrossRef] [PubMed]
- Schulze, M.B.; Stefan, N. Metabolically healthy obesity: From epidemiology and mechanisms to clinical implications. Nat. Rev. Endocrinol. 2024, 20, 633–646. [Google Scholar] [CrossRef] [PubMed]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D. Special Report Body Fatness and Cancer—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef]
- Pati, S.; Irfan, W.; Jameel, A.; Ahmed, S.; Shahid, R.K. Obesity and Cancer: A Current Overview of Epidemiology, Pathogenesis, Outcomes, and Management. Cancers 2023, 15, 485. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Douglas, I.; Forbes, H.; dos-Santos-Silva, I.; Leon, D.A.; Smeeth, L. Body-mass index and risk of 22 specific cancers: A population-based cohort study of 5·24 million UK adults. Lancet 2014, 384, 755–765. [Google Scholar] [CrossRef]
- Arnold, M.; Leitzmann, M.; Freisling, H.; Bray, R.I.; Renehan, A.; Soerjomataram, I. Global burden of cancer attributable to high body-mass index in 2012: A population-based study. Lancet Oncol. 2016, 17, 36–46. [Google Scholar] [CrossRef]
- Park, S.Y.; Boushey, C.J.; Wilkens, L.R.; Haiman, C.A.; Le Marchand, L.; Setiawan, V.W. Body mass index and risk of colorectal cancer by race and sex: The Multiethnic Cohort Study. Cancer Epidemiol. Biomarkers Prev. 2017, 26, 902–909. [Google Scholar] [CrossRef]
- Arnold, M.; Luohua, J.; Stefanick Marcia, L.; Johnson, K.C.; Lane, D.S.; LeBlanc, E.S.; Prentice, R.; Rohan, T.E.; Snively, B.M.; Vitolins, M.; et al. Duration of Adulthood Overweight, Obesity, and Cancer Risk in the Women’s Health Initiative: A Longitudinal Study from the United States. PLoS Med. 2016, 13, e1002081. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Schiborn, C.; Machann, J.; Birkenfield, A.L.; Schulze, M. Impact of higher BMI on cardiometabolic risk: Does height matter? Lancet Diabetes Endocrinol. 2024, 12, 514–515. [Google Scholar] [CrossRef]
- Stefan, N.; Haring, H.-U.; Hu, F.B.; Schulze, M.B. Divergent associations of height with cardiometabolic disease and cancer: Epidemiology, pathophysiology, and global implications. Lancet Dibaetes Endocrinol. 2016, 4, 457–467. [Google Scholar] [CrossRef]
- Peng, Y.; Zhao, L.; Li, M.; Liu, Y.; Shi, Y.; Zhnag, J. Plasticity of Adipose Tissues:Interconversion among White, Brown, and Beige Fat in its Role in Energy Homeostasis. Biomolecules 2024, 14, 483. [Google Scholar] [CrossRef] [PubMed]
- Trayhurn, P.; Wood, I.S. Adipokines: Inflammation and the pleiotropic role of white adipose tissue. Br. J. Nutr. 2004, 92, 1135–1142. [Google Scholar] [CrossRef] [PubMed]
- Verras, G.; Tchabashvili, L.; Chlorogiannis, D.; Mulita, F.; Argentou, M. Updated Clinical Evidence on the Role of Adipokines and Breast Cancer: A Review. Cancers 2023, 15, 1572. [Google Scholar] [CrossRef]
- Kim, J.; Kim, J.; Lee, Y. The Role of Adipokines in Tumor Progression and Its Association with Obesity. Biomedicines 2024, 12, 97. [Google Scholar] [CrossRef] [PubMed]
- Seldin, M.; Shinoda, K.; Rajbhandari, P. Editorial: Crosstalk between adipose tissue and immune cells. Front. Endocrinol. 2022, 13, 1036737. [Google Scholar] [CrossRef]
- Parra-Soto, S.; Boonpor, J.; Lynskey, N.; Araya, C.; Ho, F.; Pell, J.P.; Celis-Morales, C. Association between visceral adiposity index and cancer risk in the UK Biobank cohort. Cancer 2025, 131, e35576. [Google Scholar] [CrossRef]
- Hunter, G.R.; Gower, B.A.; Kane, B.L. Age Related Shift in Visceral Fat. Int. J. Body Compos. Res. 2010, 8, 103–108. [Google Scholar]
- Bu , T.; Popovic , S.; Huang, H.; Fu , T.; Gardasevic , J. Relationship Between National Economic Development and Body Mass Index in Chinese Children and Adolescents Aged 5-19 From 1986 to 2019. Front Pediatr. 2021, 9. [Google Scholar] [CrossRef]
- Wells, J.C.; Sawaya, A.L.; Wibaek, R.; Mwangome, M.; Poullas, M.S. The double burden of malnutrition:aetiological pathways and consequences for health. Lancet 2020, 395, 75–88. [Google Scholar] [CrossRef]
- Simpson, E.R.; Clyne, C.; Rubin, G.; Boon, W.C.; Robertson, K.; Britt, K.; Speed, C.; Jones, M. Sources of estrogen and their importance. J. Steroid Biochem. Mol. Biol. 2003, 86, 225–230. [Google Scholar] [CrossRef]
- Key, T.J. Hormones and cancer in humans. Mutat. Res. 1995, 333, 59–67. [Google Scholar] [CrossRef]
- Khatpe, A.; Adebayo, A.; Herodotou, C.; Kumar, B.; Nakshatri, H. Nexus between P13K/AKT and Estrogren Receptor Signalling in Breast Cancer. Cancers 2021, 13, 369. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; Li, J.; Xu, H.; Melcher, K.; Yong, E. Androgen receptor:structure, role in prostate cancer and drug discovery. Acute Pharmacol. Sin. 2015, 36, 3–23. [Google Scholar] [CrossRef]
- Lindqvist, J.; Imanishi, S.Y.; Torvaldson, E.; Malinen, M.; Remes, M.; Örn, F.; Palvimo, J.J.; Eriksson, J.E. Cyclin-dependent kinase 5 acts as a critical determinant of AKT-dependent proliferation and regulates dif-ferential gene expression by the androgen receptor in prostate cancer cells. Mol. Biol. Cell 2015, 26, 1971–1984. [Google Scholar] [CrossRef]
- Tian, J.; Ran, B.; Zhang, C.; Yan, D.; Li, X. Estrogen and progesterone promote breast cancer cell proliferation by inducing cyclin G1 expression. Med. Biol. Res. 2018, 51, e5612. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Cheng, D.; Li, P. Androgen receptor dynamics in prostate cancer: From disease progression to treatment resistance. Front. Oncol. 2025, 15, 1542811. [Google Scholar] [CrossRef]
- Gupta, N.; Mayer, D. No TitInteraction of JAK with steroid receptor function. JAKSTAT 2013, 2, e24911. [Google Scholar]
- de Boer, M.C.; Wörner, E.A.; Verlaan, D.; van Leeuwen, P.A.M. The mechanisms and effects of physical activity on breast cancer. Clin. Breast Cancer 2017, 17, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.J.; Kenfield, S.A.; Jimenez, A. Exercise-induced biochemical changes and their potential influence on cancer: A scientific review. Br. J. Sports Med. 2017, 51, 640–644. [Google Scholar] [CrossRef]
- Pasquali, R.; Oriolo, C. Obesity and Androgens in women. Front. Horm. Res. 2019, 53, 120–134. [Google Scholar]
- Chandrasekar, T.; Yang, J.C.; Gao, A.C.; Evans, C.P. Mechanisms of resistance in castration-resistant prostate cancer (CRPC). Transl. Androl. Urol. 2015, 4, 365–380. [Google Scholar]
- Dimitrakakis, C. Androgens and breast cancer in men and women. Endocrinol. Metab. Clin. N. Am. 2011, 40, 533–547. [Google Scholar] [CrossRef] [PubMed]
- Boyle, P.; Koechlin, A.; Bota, M.; d’Onofrio, A.; Zaridze, D.G.; Perrin, P.; Fitzpatrick, J.; Burnett, A.L.; Boniol, M. Endogenous and exogenous testosterone and the risk of prostate cancer and increased prostate-specific antigen (PSA) level: A meta-analysis. BJU Int. 2016, 118, 731–741. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Ryder-burbidge, C.; Mcneil, J. Physical activity, obesity and sedentary behavior in cancer etiology: Epidemiologic evidence and biologic mechanisms. Mol. Oncol. 2021, 15, 790–800. [Google Scholar] [CrossRef]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metab. Clin. Exp. 2019, 92, 121–135. [Google Scholar] [CrossRef]
- Iyengar, N.M.; Gucalp, A.; Dannenberg, A.J.; Hudis, C.A. Obesity and Cancer Mechanisms: Tumor Microenvironment and Inflammation. J. Clin. Oncol. 2016, 34, 4270–4276. [Google Scholar] [CrossRef]
- Wright, S.C.E.; Vasilevski, N.; Serra, V.; Rodon, J.; Eichhorn, P.J.A. Mechanisms of Resistance to PI3K Inhibitors in Cancer: Adaptive Responses, Drug Tolerance and Cellular Plasticity. Cancers 2021, 13, 1538. [Google Scholar] [CrossRef]
- Schaefer, E.L.; Tsuboi, S.; Salerno, E.A. The integrative role of leptin, oestrogen and the insulin family in obesity-associated breast cancer: Potential effects of exercise. Obes. Rev. 2015, 16, 473–487. [Google Scholar]
- Mason, C.; Xiao, L.; Duggan, C.; Imayama, I.; Foster-Schubert, K.E.; Kong, A.; Campbell, K.L.; Wang, C.Y.; Alfano, C.M.; Blackburn, G.L.; et al. Effects of dietary weight loss and exercise on insulin-like growth factor-I and insulin-like growth factor-binding protein-3 in postmenopausal women: A randomized controlled trial. Cancer Epidemiol. Biomarkers Prev. 2013, 22, 1457–1463. [Google Scholar] [CrossRef]
- Hadgraft, N.T.; Winkler, E.; Climie, R.E.; Grace, M.S.; Romero, L.; Owen, N.; Dunstan, D.; Healy, G.; Dempsey, P.C. Effects of sedentary behaviour interventions on biomarkers of cardiometabolic risk in adults: Systematic review with meta-analyses. Br. J. Sports Med. 2020, 54, 514–521. [Google Scholar] [CrossRef] [PubMed]
- ISWood FPde Heredia BWang, P.T. Cellular hypoxia and adipose tissue dysfunction in obesity: Symposium on “Frontiers in Adipose Tissue Biology”. Proc. Nutr. Soc. 2009, 68, 435–443. [Google Scholar]
- Wu, P.-Y.; Lin, S.-H.; Hong, T.-M.; Hsu, K.-F. Omental Macrophagic “Crown-like Structures” Are Associated with Poor Prognosis in Advanced-Stage Serous Ovarian Cancer. Curr. Oncol. 2021, 28, 4234–4246. [Google Scholar]
- Lee, J.Y.; Sohn, K.H.; Rhee, S.H.; Hwang, D. Saturated fatty acids, but not unsaturated fatty acids, induce the expression of cyclooxygenase-2 mediated through toll-like receptor 4. J. Biol. Chem. 2001, 276, 16683–16689. [Google Scholar] [CrossRef]
- Gomez, J.C.; Gonzalez, P.G.; Fernandez, T.F.G.; Bueno, S.C.; Calvo, N.B.; Cardoso, B.S.; Lorido, J.C.A.L. Bioelectrical impedance-derived phase angle (PhA) in people living with obesity: Role in sarcopenia and comorbidities. Nutr. Metab. Cardiovasc. Dis. 2024, 34, 2511–2518. [Google Scholar] [CrossRef]
- Prete, M.; Ballarin, G.; Poriciello, G.; Arianna, A.; Luongo, A.; Belli, V.; Scalfi, L.; Celentano, E. Bioelectrical impedance analysis—Derived phase angle (PhA) in lung cancer patients: A systematic review. BMC Cancer 2024, 24, 608. [Google Scholar] [CrossRef]
- Lal, I.; Dittus, K.; Holmes, C. Platelets, coagulation and fibrinolysis in breast cancer progression. Breast Cancer Res. 2013, 15, 207. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, Z.; Zhang, J.; Mafa, T.; Zhang, J.; Zhu, H. Fibrinogen: A new player and target on the formation of pre-metastatic niche in tumor metastasis. Crit. Rev. Oncol. Hematol. 2025, 207, 105625. [Google Scholar] [CrossRef]
- Alexander, E.T.; Gilmour, S.K. Immunomodulatory role of thrombin in cancer progression. Mol. Carcinog. 2022, 61, 527–536. [Google Scholar] [CrossRef]
- Falanga, A.; Marchetti, M.; Vignoli, A. Coagulation and cancer: Biological and clinical aspect. J. Thromb. Haemost. 2013, 11, 223–233. [Google Scholar] [CrossRef]
- Wu, X.; Yu, X.; Chen, C.; Chen, C.; Wang, Y.; Su, D.; Zhu, L. Fibrinogen and tumors. Front. Oncol. 2024, 14, 1393599. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Malagón, A.; Rodríguez-Sojo, M.; Redondo, E.; Rodríguez-Cabezas, M.; Gálvez, J. Rodríguez-Nogales A systematic review: The gut microbiotaas a link between colorectal cancer and obesity. Obes. Rev. 2025, 26, e13872. [Google Scholar] [CrossRef] [PubMed]
- Rumyantsev, K.; Polyakova, V.; Sorokina, I.; Feoktistova, P.; Khatkov, I.; Bodunova, N. The Gut Microbiota Impacts Gastrointestinal Cancers through Obesity, Diabetes and Chronic Inflammation. Life 2024, 14, 1219. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Alcoholado, L.; Ordonez, R.; Otero, A.; Plaza-Andrade, I.; Laborda-Illanes, A.; Medina, J.A.; Ramos-Molina, B. Gut Microbiota-Mediated Inflammation and Permeability in Patients with Obesity and Colorectal Cancer. Int. J. Mol. Sci. 2020, 21, 6782. [Google Scholar] [CrossRef]
- Petrelli, F.; Cortellini, A.; Indini, A.; Tomasello, G.; Ghidini, M.; Nigro, O.; Salati, M.; Dottorini, L.; Iaculli, A.; Varricchio, A.; et al. Association of Obesity With Survival Outcomes in Patients With Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open. 2021, 4, e213520. [Google Scholar] [CrossRef]
- Hakimi, A.A.; Furberg, H.; Zabor, E.C.; Jacobsen, A.; Schultz, N.; Ciriello, G.; Mikklineni, N.; Fiegoli, B.; Kim, P.H.; Voss, M.H.; et al. An epidemiologic and genomic investigation into the obesity paradox in renal cell carcinoma. J. Natl. Cancer Inst. 2013, 105, 1862–1870. [Google Scholar] [CrossRef]
- Schlesinger, S.; Siegert, S.; Koch, M.; Walter, J.; Heits, N.; Hinz, S.; Jacobs, G.; Hampe, J.; Schafmayer, C.; Nöthlings, U. Postdiagnosis body mass index and risk of mortality in colorectal cancer survivors: A prospective study and meta-analysis. Cancer Causes Control 2014, 25, 1407–1418. [Google Scholar] [CrossRef]
- Li, S.; Wang, Z.; Huang, J.; Fan, J.; Du, H.; Liu, L.; Che, G. Systematic review of prognostic roles of body mass index for patients undergoing lung cancer surgery: Does the “obesity paradox” really exist? Eur. J. Cardiothorac. Surg. 2017, 51, 817–828. [Google Scholar] [CrossRef]
- Banack, H.; Kaufman, J. The “Obesity Paradox” Explained. Epidemiology 2013, 24, 461–462. [Google Scholar] [CrossRef]
- Tönnies, T.; Kahl, S.; Kuss, O. Collider bias in observational studies: Consequences for medical research. Part 30 of a series on evaluation of scientific publications. Dtsch. Arztebl. Int. 2022, 119, 107–112. [Google Scholar] [CrossRef]
- Holmberg, M.; Anderson, L. Collider Bias. JAMA 2022, 327, 1282–1283. [Google Scholar] [CrossRef]
- Butt, J.; Petrie, M.; Jhund, P.; Sattar, N.; Desai, A.; Kober, L. Anthropometric measures and adverse outcomes in heart failure with reduced ejection fraction:revisiting the obesity paradox. Eur. Heart J. 2023, 44, 1136–1153. [Google Scholar] [CrossRef]
- Helyer, L.K.; Varnic, M.; Le, L.W.; Leong, W.; McCready, D. Obesity is a risk factor for developing postoperative lymphedema in breast cancer patients. Breast J. 2010, 16, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Antoniak, K.; Hansdorfer-Korzon, R.; Mrugacz, M.; Zorena, K. Adipose Tissue and Biological Factors. Possible Link between Lymphatic System Dysfunction and Obesity. Metabolites 2021, 11, 617. [Google Scholar] [CrossRef]
- Mizrahi, D.; Park, S.B.; Li, T.; Timmins, H.C.; Trinh, T.; Au, K.; Battaglini, E.; Wyld, D.; Henderson, R.D.; Grimison, P.; et al. Hemoglobin, Body Mass Index, and Age as Risk Factors for Paclitaxel- and Oxaliplatin-Induced Peripheral Neuropathy. JAMA Netw. Open. 2021, 4, e2036695. [Google Scholar] [CrossRef] [PubMed]
- Timmins, H.C.; Li, T.; Goldstein, D.; Trinh, T.; Mizrahi, D.; Harrison, M.; Horvath, L.G.; Friedlander, M.; Kiernan, M.C.; Park, S.B. The impact of obesity on neuropathy outcomes for paclitaxel- and oxaliplatin-treated cancer survivors. J. Cancer Surviv. 2022, 16, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Ross, K.H.; Gogineni, K.; Subhedar, P.D.; Lin, J.Y.; McCullough, L.E. Obesity and cancer treatment efficacy: Existing challenges and opportunities. Cancer 2019, 125, 1588–1592. [Google Scholar] [CrossRef]
- Guenancia, C.; Lefebvre, A.; Cardinale, D.; Yu, A.F.; Ladoire, S.; Ghiringhelli, F.; Zeller, M.; Rochette, L.; Cottin, Y.; Vergely, C. Obesity As a Risk Factor for Anthracyclines and Trastuzumab Cardiotoxicity in Breast Cancer: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2016, 34, 3157–3165. [Google Scholar] [CrossRef]
- Xie, Y.; Wang, Q.; Hu, T.; Chen, R.; Wang, J.; Chang, H.; Cheng, J. Risk Factors Related to Acute Radiation Dermatitis in Breast Cancer Patients After Radiotherapy: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 738851. [Google Scholar] [CrossRef]
- Wichmann, I.A.; Cuello, M.A. Obesity and gynecological cancers: A toxic relationship. Int. J. Gynaecol. Obs. 2021, 155, 123–134. [Google Scholar] [CrossRef]
- Wilson, R.L.; Taaffe, D.R.; Newton, R.U.; Hart, N.H.; Lyons-Wall, P.; Galvão, D.A. Obesity and prostate cancer: A narrative review. Crit. Rev. Oncol. Hematol. 2022, 169, 103543. [Google Scholar] [CrossRef] [PubMed]
- Delaye, M.; Rousseau, A.; Mailly-Giacchetti, L.; Assoun, S.; Sokol, H.; Neuzillet, C. Obesity, cancer, and response to immune checkpoint inhibitors: Could the gut microbiota be the mechanistic link? Pharmacol. Ther. 2023, 247. [Google Scholar] [CrossRef]
- Amri, R.; Bordeianou, L.G.; Sylla, P. BD Obesity, outcomes and quality of care: Body mass index increases the risk of wound-related complications in colon cancer surgery. Am. J. Surg. 2014, 207, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Lennon, H.; Sperrin, M.; Badrick, E.; Renehan, A.G. The Obesity Paradox in Cancer: A Review. Curr. Oncol. Rep. 2016, 18, 56. [Google Scholar] [CrossRef]
- Johnson, D.B.; Nebhan, C.A.; Moslehi, J.J.; Balko, J.M. Immune-checkpoint inhibitors: Long-term implications of toxicity. Nat. rev Clin. Oncol. 2022, 19, 254–267. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, A.; Bersanelli, M.; Buti, S.; Cannita, K.; Santini, D.; Perrone, F.; Giusti, R.; Tiseo, M.; Michiara, M.; Di Marino, P.; et al. A multicenter study of body mass index in cancer patients treated with anti-PD-1/PD-L1 immune checkpoint inhibitors: When overweight becomes favorable. J. Immunother. Cancer. 2019, 1, 57. [Google Scholar] [CrossRef]
- McQuade, J.L.; Daniel, C.R.; Hess, K.R.; Mak, C.; Wang, D.Y.; Rai, R.R.; Park, J.J.; Haydu, L.E.; Spencer, C.; Wongchenko, M.; et al. Association of body-mass index and outcomes in patients with metastatic melanoma treated with targeted therapy, immunotherapy, or chemotherapy: A retrospective, multicohort analysis. Lancet Oncol. 2018, 19, 310–322. [Google Scholar] [CrossRef]
- Heidelberger, V.; Goldwasser, F.; Kramkimel, N.; Jouinot, A.; Huillard, O.; Boudou-Rouquette, P.; Chanal, J.; Arrondeau, J.; Franck, N.; Alexandre, J.; et al. Sarcopenic overweight is associated with early acute limiting toxicity of anti-PD1 checkpoint inhibitors in melanoma patients. Investig. New Drugs. 2017, 35, 436–441. [Google Scholar] [CrossRef]
- Lyman, G.; Sparreboom, A. Chemotherapy dosing in overweight and obese patients with cancer. Nat. Rev. Clin. Oncol. 2013, 10, 451–459. [Google Scholar] [CrossRef]
- Colleoni, M.; Li, S.; Gelber, R.D.; Price, K.N.; Coates, A.S.; Castiglione-Gertsch, M.; Goldhirsch, A. Relation between chemotherapy dose, oestrogen receptor expression, and body-mass index. Lancet 2005, 366, 1108–1110. [Google Scholar] [CrossRef]
- Rosner, G.L.; Hargis, J.B.; Hollis, D.R.; Budman, D.R.; Weiss, R.B.; Henderson, I.C.; Schilsky, R.L. Relationship between toxicity and obesity in women receiving adjuvant chemotherapy for breast cancer: Results from Cancer and Leukemia Group B Study 8541. J. Clin. Oncol. 1996, 14, 3000–3008. [Google Scholar] [CrossRef] [PubMed]
- Griggs, J.J.; Bohlke, K.; Balaban, E.P.; Dignam, J.J.; Hall, E.T.; Donald Harvey, R.; Hecht, D.P.; Klute, K.A.; Morrison, V.A.; Pini , T.M.; et al. Appropriate Systemic Therapy Dosing for Obese Adult Patients With Cancer: ASCO Guideline Update. J. Clin. Oncol. 2021, 39, 2037–2048. [Google Scholar] [CrossRef] [PubMed]
- Laviano, A.; Rianda, S.; Fanelli, F. Sarcopenia and chemotherapy dosing in obese patients. Nat. Rev. Clin. Oncol. 2013, 10, 664. [Google Scholar] [CrossRef]
- Liu, C.; Liu, T.; Deng, L.; Zhang, Q.; Song, M.; Shi, J.; Liu, C.; Xie, H.; Chen, Y.; Lin, S.; et al. Sarcopenic Obesity and Outcomes for Patients With Cancer. JAMA Netw. Open. 2024, 7, e2417115. [Google Scholar] [CrossRef]
- Min, H.-Y.; Lee, H.-Y. Molecular targeted therapy for anticancer treatment. Exp. Mol. Med. 2022, 54, 1670–1694. [Google Scholar] [CrossRef] [PubMed]
- Dauccia, C.; Franzoni, M.A.; Martel, S.; Agbor-Tarh, D. Body mass index and weight changes in patients with HER2-positive early breast cancer: A sub-analysis of the APHINITY trial. Eur. J. Cancer 2025, 8, 115489. [Google Scholar] [CrossRef]
- Lang, X.; Tong, C.; Yu, Y.; Li, H. Effect of body mass index on survival in patients with metastatic colo-rectal cancer receiving chemotherapy plus bevacizumab: A systematic review and met-analysis. Front. Nutr. 2024, 16, 1399569. [Google Scholar]
- Siringo, M.; Gentile, G.; Caponnetto, S.; Sperduti, I. Evaluation of Efficacy of ALK Inhibitors According to Body Mass Index in ALK Rearranged NSCLC Patients-A Retrospective Observational Study. Cancers 2023, 15, 3422. [Google Scholar] [CrossRef]
- Boi, S.K.; Orlandella, R.M.; Gibson, J.T.; Turbitt, W.J.; Wald, G.; Thomas, L.; Rosean, C.B.; Norris, K.E.; Bing, M.; Bertrand, L.; et al. Obesity diminishes response to PD-1-based immunotherapies in renal cancer. J. Immunother. Cancer. 2020, 8, e000725. [Google Scholar] [CrossRef]
- Guzman-Prado, Y.; Ben Shimol, J. SO Body mass index and immune-related adverse events in patients on immune checkpoint inhibitor therapies: A systematic review and meta-analysis. Cancer Immunol. Immunother. 2021, 70, 89–100. [Google Scholar] [CrossRef]
- Yeung, C.; Kartolo, A.; Holstead, R.; Moffat, G.T.; Hanna, L.; Hopman, W.; Baetz, T. Immunotoxicity or Clinical Outcomes for Immune Checkpoint Inhibitors. Immunotherapy 2022, 14, 765–776. [Google Scholar] [CrossRef]
- Tee, M.C.; Cao, Y.; Warnock, G.L.; Hu, F.B. CJ Effect of bariatric surgery on oncologic outcomes: A systematic review and meta-analysis. Surg. Endosc. 2013, 27, 4449–4456. [Google Scholar] [CrossRef]
- Aminian, A.; Wilson, A.; Al-Kurd, A.; Tu, C.; Milinovich, A.; Kroh, M.; Rosenthal, R.J.; Brethauer Stacy, A.; Philip, R.S.; Michael, W.K.; et al. Association of Bariatric Surgery with Cancer Risk and Mortality in Adults with Obesity. JAMA 2022, 327, 2423–2433. [Google Scholar] [CrossRef] [PubMed]
- Adam, S.; Ho, J.H.; Liu, Y.; Siahmansur, T.T.; Siddals, K.; Iqbal, Z.; Azmi, S.; Senapati, S.; New, J.; Jeziorska, M.; et al. Bariatric Surgery-induced High-density Lipoprotein Functionality Enhancement Is Associated With Reduced Inflammation. J. Clin. Endocrinol. Metab. 2022, 207, 2182–2194. [Google Scholar] [CrossRef]
- Birks, S.; Peeters, A.; Backholer, K.; O’Brien, P.; Brown, W. A systematic review of the impact of weight loss on cancer incidence and mortality. Obes. Rev. 2012, 13, 868–891. [Google Scholar] [CrossRef] [PubMed]
- Suna, M.; da Silva, M.; Bjørgeb, T.; Fritza, J.; Mboya, I.B.; Jerkeman, M.; Stattin, P.; Wahlström, J.; Michaëlsson, K.; van Guelpen, B.; et al. Body mass index and risk of over 100 cancer forms and subtypes in 4.1 million individuals in Sweden: The Obesity and Disease Development Sweden (ODDS) pooled cohort study. Lancet Reg. Health 2024, 45. [Google Scholar] [CrossRef] [PubMed]
- Sjöström, L.; Gummesson, A.; Sjöström, C.D.; Narbro, K.; Peltonen, M.; Wedel, H.; Bengtsson, C.; Bouchard, C.; Carlsson, B.; Dahlgren, S.; et al. Effects of bariatric surgery on cancer incidence in obese patients in Sweden (Swedish Obese Subjects Study): A prospective, controlled intervention trial. Lancet Oncol. 2009, 10, 653–662. [Google Scholar] [CrossRef]
- Ard, J.; Fitch, A.; Fruh, S.; Herman, L. Weight Loss and Maintenance Related to the Mechanism of Action of Glucagon-Like Peptide 1 Receptor Agonists. Adv. Ther. 2021, 38, 2821–2839. [Google Scholar] [CrossRef]
- Wang, L.; Wang, W.; Kaelber, D.C.; Xu, R.; Berger, N.A. GLP-1 Receptor Agonists and Colorectal Cancer Risk in Drug-Naive Patients With Type 2 Diabetes, With and Without Overweight/Obesity. JAMA Oncol. 2023, 10, 256–258. [Google Scholar] [CrossRef]
- Wang, L.; Xu, R.; Kaelber, D.C.; Berger, N.A. Glucagon-Like Peptide 1 Receptor Agonists and 13 Obesity-Associated Cancers in Patients With Type 2 Diabetes. JAMA Netw. Open 2024, 7, e2421305. [Google Scholar] [CrossRef]
- Knudsen, L.B.; Madsen, L.W.; Andersen, S.; Almholt, K.; De Boer, A.S.; Drucker, D.J.; Gotfredsen, C.; Egerod, F.L.; Hegelund, A.C.; Jacobsen, H.; et al. Glucagon-like peptide-1 receptor agonists activate rodent thyroid C-cells causing calcitonin release and C-cell proliferation. Endocrinology 2010, 151, 1473–1486. [Google Scholar] [CrossRef] [PubMed]
- Bezin, J.; Gouverneur, A.; Pénichon, M.; Mathieu, C.; Garrel, R.; Hillaire-Buys, D.; Pariente, A.; Faillie, J.-L. GLP-1 Receptor Agonists and the Risk of Thyroid Cancer. Diabetes Care 2022, 46, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.A.; Stüurmer, T. Putting GLP-1 RAs and Thyroid Cancer in Context: Additional Evidence and Remaining Doubts. Diabetes Care 2023, 46, 249–251. [Google Scholar] [CrossRef]
- Cao, C.; Yang, S.; Zhou, Z. GLP-1 receptor agonists and risk of cancer in type 2 diabetes: An updated meta-analysis of randomized controlled trials. Endocrine 2019, 66, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Richa, C.; Saad, K.; Halabi, G.; Gharios, E. Case-series of paraneoplastic Cushing syndrome in small-cell lung cancer. Endocrinol. Diabetes Metab. Case Rep. 2018, 18, 0004. [Google Scholar] [CrossRef]
- Service, F.; Dale, A.; Elveback, L.; Jiang, N. Insulinoma: Clinical and diagnostic features of 60 consecutive cases. Mayo Clin. Proc. 1976, 51, 417–429. [Google Scholar]
- Chiejina, M.; Kudaravalli, P.; Samant, H. Ascites; StatPearls: Treasure Island, FL, USA, 2023; (accessed on 2 June 2025). [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ingram, Y.; Olujide, O.; Sheikh, N.; Robinson, A.; Ho, J.H.; Syed, A.A.; Adam, S. The Relationship Between Obesity and Cancer: Epidemiology, Pathophysiology, and the Effect of Obesity Treatment on Cancer. Curr. Oncol. 2025, 32, 362. https://doi.org/10.3390/curroncol32060362
Ingram Y, Olujide O, Sheikh N, Robinson A, Ho JH, Syed AA, Adam S. The Relationship Between Obesity and Cancer: Epidemiology, Pathophysiology, and the Effect of Obesity Treatment on Cancer. Current Oncology. 2025; 32(6):362. https://doi.org/10.3390/curroncol32060362
Chicago/Turabian StyleIngram, Yasmin, Oluwasegun Olujide, Nabiha Sheikh, Alice Robinson, Jan Hoong Ho, Akheel A. Syed, and Safwaan Adam. 2025. "The Relationship Between Obesity and Cancer: Epidemiology, Pathophysiology, and the Effect of Obesity Treatment on Cancer" Current Oncology 32, no. 6: 362. https://doi.org/10.3390/curroncol32060362
APA StyleIngram, Y., Olujide, O., Sheikh, N., Robinson, A., Ho, J. H., Syed, A. A., & Adam, S. (2025). The Relationship Between Obesity and Cancer: Epidemiology, Pathophysiology, and the Effect of Obesity Treatment on Cancer. Current Oncology, 32(6), 362. https://doi.org/10.3390/curroncol32060362