Epidemiology, Treatment Patterns, Survival, Healthcare Resource Utilization, and Costs of Dedifferentiated Liposarcoma (DDLPS) in Canada: A Retrospective Cohort Study Using Administrative Databases in Ontario

 ,
,
Abstract
1. Introduction and Objectives
2. Methodology
2.1. Study Design, Population, and Data Sources
2.2. Study Population and Follow-Up
2.3. Outcomes
2.3.1. Baseline Characteristics
2.3.2. Incidence and Prevalence
2.3.3. Treatment Patterns
- -
- DOXO: doxorubicin alone or with ifosfamide, cisplatin, or olaratumab.
- -
- GEM: gemcitabine alone or with cisplatin or docetaxel.
- -
- OTHER: not DOXO and GEM; includes carboplatin and paclitaxel with radiotherapy, dacarbazine, epirubicin, and ifosfamide; paclitaxel (weekly), pazopanib, vincristine, dactinomycin, and cyclophosphamide; ifosfamide, olaratumab (maintenance), paclitaxel, and carboplatin; and durvalumab.
2.3.4. Overall Survival (OS)
2.3.5. Healthcare Resource Utilization and Costs
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Incidence and Prevalence of DDLPS
3.3. Treatment Patterns
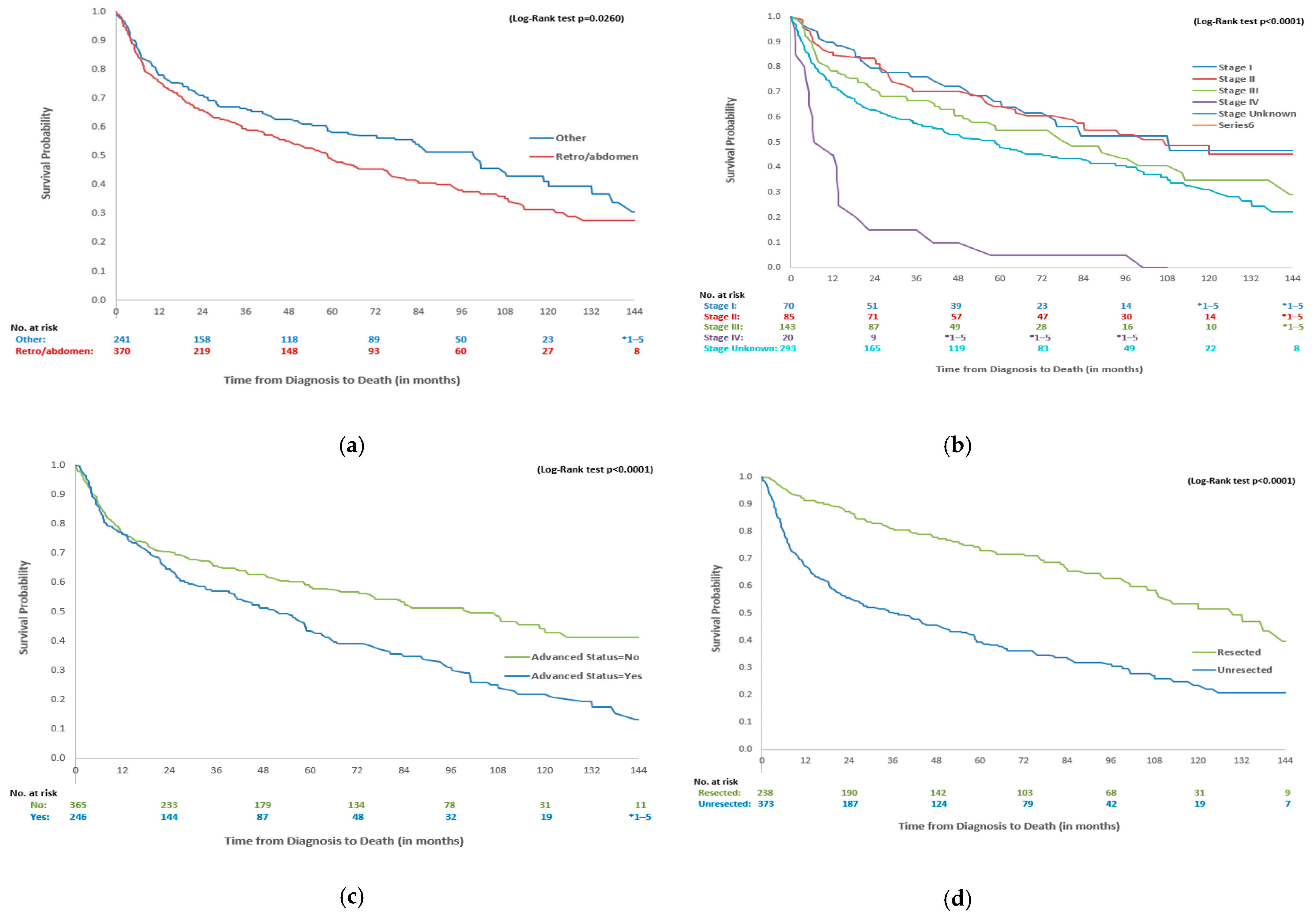
3.4. Survival Outcomes for Overall Cohort and Stratifications
3.5. All-Cause Healthcare Resource Utilization (HCRU) and Costs
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schöffski, P.; Lahmar, M.; Lucarelli, A.; Maki, R.G. Brightline-1: Phase II/III trial of the MDM2–p53 antagonist BI 907828 versus doxorubicin in patients with advanced DDLPS. Future Oncol. 2023, 19, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.T.J.; Thway, K.; Huang, P.H.; Jones, R.L. Clinical and molecular spectrum of liposarcoma. J. Clin. Oncol. 2018, 36, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Gootee, J.; Aurit, S.; Curtin, C.; Silberstein, P. Primary anatomical site, adjuvant therapy, and other prognostic variables for dedifferentiated liposarcoma. J. Cancer Res. Clin. Oncol. 2018, 145, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Bock, S.; Hoffmann, D.G.; Jiang, Y.; Chen, H.; Il’yasova, D. Increasing Incidence of Liposarcoma: A Population-Based Study of National Surveillance Databases, 2001–2016. Int. J. Environ. Res. Public Health 2020, 17, 2710. [Google Scholar] [CrossRef] [PubMed]
- Haddox, C.L.; Riedel, R.F. Recent advances in the understanding and management of liposarcoma. Fac. Rev. 2021, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Amer, K.M.; Congiusta, D.V.; Thomson, J.A.; Elsamna, S.T.; Chaudhry, I.; Bozzo, A.; Amer, R.; Siracuse, B.; Ghert, M.; Beebe, K.S. Epidemiology and survival of liposarcoma and its subtypes: A dual database analysis. J. Clin. Orthop. Trauma. 2020, 11 (Suppl. S4), S479–S484. [Google Scholar] [CrossRef] [PubMed]
- Nishio, J.; Nakayama, S.; Nabeshima, K.; Yamamoto, T. Biology and management of dedifferentiated liposarcoma: State of the art and perspectives. J. Clin. Med. 2021, 10, 3230. [Google Scholar] [CrossRef] [PubMed]
- Bozzo, A.; Seow, H.; Pond, G.; Ghert, M. Changes in soft-tissue sarcoma treatment patterns over time: A population-based study in a country with universal and centralized healthcare. Sarcoma 2019, 2019, 8409406. [Google Scholar] [CrossRef] [PubMed]
- Alkazemi, B.; Ghazawi, F.M.; Lagacé, F.; Nechaev, V.; Zubarev, A.; Litvinov, I.V. Investigation of the incidence and geographic distribution of bone and soft tissue sarcomas in Canada: A national population-based study. Curr. Oncol. 2023, 30, 5631–5651. [Google Scholar] [CrossRef] [PubMed]
- Jönsson, L.; Justo, N.; Musayev, A.; Krishna, A.; Burke, T.; Pellissier, J.; Judson, I.; Staddon, A.; Blay, J.Y. Cost of treatment in patients with metastatic soft tissue sarcoma who respond favourably to chemotherapy: The Sarcoma treatment and Burden of Illness in North America and Europe (SABINE) study. Eur. J. Cancer Care 2015, 25, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Wodchis, W.P.; Bushmeneva, K.; Nikitovis, M.; McKillop, I. Guidelines on Person-Level Costing Using Administrative Databases in Ontario. Work. Pap. Ser. 2013, 1, 1–70. Available online: https://tspace.library.utoronto.ca/bitstream/1807/87373/1/Wodchis%20et%20al_2013_Guidelines%20on%20Person-Level%20Costing.pdf (accessed on 12 December 2024).
- Bacon, A.; Wong, K.; Fernando, M.S.; Rous, B.; Hill, R.J.W.; Collins, S.D.; Broggio, J.; Strauss, S.J. Incidence and survival of soft tissue sarcoma in England between 2013 and 2017, an analysis from the National Cancer Registration and Analysis Service. Int. J. Cancer 2023, 152, 1789–1803. [Google Scholar] [CrossRef] [PubMed]
- Italiano, A.; Toulmonde, M.; Cioffi, A.; Penel, N.; Bompas, E.; Isambert, N.; Duffaud, F.; Patrikidou, A.; Lortal, B.; Le Cesne, A.; et al. Advanced well-differentiated/dedifferentiated liposarcomas: Role of chemotherapy and survival. Ann. Oncol. 2012, 23, 1601–1607. [Google Scholar] [CrossRef] [PubMed]
- Rugge, M.; Buja, A.; Tropea, S.; Girardi, G.; Franzese, L.C.; Cozzolino, C.; Zorzi, M.; Vecchiato, A.; Del Fiore, P.; Brunello, A.; et al. Direct costs of care for adults with soft tissue sarcomas: A population-based study. Cancers 2022, 14, 3109. [Google Scholar] [CrossRef] [PubMed]
- Livingston, J.A.; Bugano, D.; Barbo, A.; Lin, H.; Madewell, J.E.; Wang, W.L.; Lazar, A.J.; Tseng, W.W.; Roland, C.L.; Feig, B.W.; et al. Role of chemotherapy in dedifferentiated liposarcoma of the retroperitoneum: Defining the benefit and challenges of the standard. Sci. Rep. 2017, 7, 10733. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Baseline Characteristics | Total DDLPS Cohort | Advanced DDLPS | Unresected Status | ||||
|---|---|---|---|---|---|---|---|
| N = 611 | Yes N = 246 | No N = 365 | p-Value | Yes N = 373 | No N = 238 | p-Value | |
| Age at Index Date, Years | |||||||
| Mean (SD) | 66.2 (13.3) | 64.8 (12.8) | 67.1 (13.6) | 0.0408 | 67.0 (13.2) | 64.8 (13.3) | 0.0485 |
| Median (IQR) | 67 (57–76) | 66 (56–73) | 67 (57–77) | 0.0573 | 68 (57–77) | 66 (56–75) | 0.0856 |
| Min–max | 21–96 | 21–91 | 26–96 | 26–96 | 21–93 | ||
| Age Group at Index Date (N, %) | |||||||
| 18–50 years | 76 (12.4%) | 34 (13.8%) | 42 (11.5%) | 0.1523 | 41 (11.0%) | 35 (14.7%) | 0.4137 |
| 51–64 years | 186 (30.4%) | 76 (30.9%) | 110 (30.1%) | 110 (29.5%) | 76 (31.9%) | ||
| 65–74 years | 173 (28.3%) | 77 (31.3%) | 96 (26.3%) | 110 (29.5%) | 63 (26.5%) | ||
| 75+ years | 176 (28.8%) | 59 (24.0%) | 117 (32.1%) | 112 (30.0%) | 64 (26.9%) | ||
| Sex (N, %) | |||||||
| Female | 218 (35.7%) | 80 (32.5%) | 138 (37.8%) | 0.1809 | 136 (36.5%) | 82 (34.5%) | 0.6135 |
| Male | 393 (64.3%) | 166 (67.5%) | 227 (62.2%) | 237 (63.5%) | 156 (65.5%) | ||
| Residence (N, %) | |||||||
| Urban | 531 (86.9%) | 209 (85.0%) | 322 (88.2%) | 0.2414 | 318 (85.3%) | 213 (89.5%) | 0.1297 |
| Rural | 80 (13.1%) | 37 (15.0%) | 43 (11.8%) | 55 (14.7%) | 25 (10.5%) | ||
| Treatment facility in one of five cancer centres *** (N, %) | |||||||
| Yes | 317 (51.9%) | 133 (54.1%) | 184 (50.4%) | 0.3753 | 166 (44.5%) | 151 (63.4%) | <0.0001 |
| Type of Centre for Diagnosis (N, %) | |||||||
| Community | 207 (33.9%) | 75 (30.5%) | 132 (36.2%) | 0.1460 | 147 (39.4%) | 60 (25.2%) | 0.0003 |
| Academic | 404 (66.1%) | 171 (69.5%) | 233 (63.8%) | 226 (60.6%) | 178 (74.8%) | ||
| Income Quintile (N, %) | |||||||
| 1 (lowest) | 104 (17.0%) | 34 (13.8%) | 70 (19.2%) | 0.1139 | 61 (16.4%) | 43 (18.1%) | 0.9894 |
| 2- | 119 (19.5%) | 59 (24.0%) | 60 (16.4%) | 73 (19.6%) | 46 (19.3%) | ||
| 3- | 151 (24.7%) | 56 (22.8%) | 95 (26.0%) | 93 (24.9%) | 58 (24.4%) | ||
| 4- | 115 (18.8%) | 47 (19.1%) | 68 (18.6%) | 71 (19.0%) | 44 (18.5%) | ||
| 5 (highest) | 122 (20.0%) | 50 (20.3%) | 72 (19.7%) | 75 (20.1%) | 47 (19.7%) | ||
| Charlson Co-Morbidity Index Score (N, %) | |||||||
| Score = 0 | 419 (68.6%) | 173 (70.3%) | 246 (67.4%) | 0.2855 | 251 (67.3%) | 168 (70.6%) | 0.1533 |
| Score = 1 | 23 (3.8%) | 11 (4.5%) | 12 (3.3%) | 15 (4.0%) | 8 (3.4%) | ||
| Score = 2 | 102 (16.7%) | 42 (17.1%) | 60 (16.4%) | 58 (15.5%) | 44 (18.5%) | ||
| Score ≥ 3 | 67 (11.0%) | 20 (8.1%) | 47 (12.9%) | 49 (13.1%) | 18 (7.6%) | ||
| Disease Stage (N, %) | |||||||
| Stage I | 70 (11.5%) | 11 (4.5%) | 59 (16.2%) | NA | ** 38–42 | ** 28–32 | 0.0008 |
| Stage II | 85 (13.9%) | 12 (4.9%) | 73 (20.0%) | 43 (11.5%) | 42 (17.6%) | ||
| Stage III | 143 (23.4%) | 143 (58.1%) | - | 75 (20.1%) | 68 (28.6%) | ||
| Stage IV | 20 (3.3%) | 20 (8.1%) | - | ** 15–19 | * 1–5 | ||
| Unknown/missing | 293 (48.0%) | 60 (24.4%) | 233 (63.8%) | 198 (53.1%) | 95 (39.9%) | ||
| Topography (N, %) | |||||||
| Retroperitoneum/ abdomen | 370 (60.6%) | 166 (67.5%) | 204 (55.9%) | 0.0578 | 257 (68.9%) | 113 (47.5%) | <0.0001 |
| Extremities | 121 (19.8%) | 42 (17.1%) | 79 (21.6%) | 27 (7.2%) | 94 (39.5%) | ||
| Thorax or trunk | 40 (6.5%) | 12 (4.9%) | 28 (7.7%) | ** 19–23 | ** 17–21 | ||
| Pelvis | 54 (8.8%) | 16 (6.5%) | 38 (10.4%) | 45 (12.1%) | 9 (3.8%) | ||
| Other or unknown | 26 (4.3%) | 10 (4.1%) | 16 (4.4%) | ** 21–25 | * 1–5 | ||
| Years of Follow-up Time (from Index Date to Death or Censored Date) | |||||||
| Mean (SD) | 4.1 (3.5) | 3.6 (3.3) | 4.4 (3.6) | 0.0027 | 3.3 (3.2) | 5.4 (3.5) | <0.0001 |
| Median (IQR) | 3.1 (1.1–6.6) | 2.5 (1.1–5.2) | 3.6 (1.1–7.3) | 0.0100 | 2.0 (0.6–5.3) | 4.9 (2.2–8.2) | <0.0001 |
| Treatment after DDLPS Diagnosis Anytime During Follow-up (N, %) | |||||||
| Surgical status | 321 (52.5%) | 123 (50.0%) | 198 (54.2%) | 0.3026 | 83 (22.3%) | 238 (100.0%) | <0.0001 |
| Radiation status | 398 (65.1%) | 181 (73.6%) | 217 (59.5%) | 0.0003 | 226 (60.6%) | 172 (72.3%) | 0.0031 |
| Systemic therapy (ALR/NDFP data only) | 117 (19.1%) | 117 (47.6%) | - | NA | 85 (22.8%) | 32 (13.4%) | 0.0042 |
| Crude Incidence Rate per 100,000 | Crude Prevalence Rate per 100,000 | |
|---|---|---|
| Overall cohort (2010–2022) | 0.46 | 1.99 |
| Age | ||
| 18–50 | 0.10 | 0.56 |
| 51–64 | 0.58 | 2.81 |
| 65–74 | 1.15 | 4.86 |
| 75+ | 1.56 | 5.17 |
| Sex | ||
| Female | 0.32 | 1.31 |
| Male | 0.62 | 2.72 |
| Line of Treatment | Drug Type | Frequency (%) |
|---|---|---|
| 1L treatment (N = 117) | DOXO | 95 (81.2) |
| GEM | 16 (13.7) | |
| OTHER | 6 (5.1) | |
| Mean time from DDLPS diagnosis to 1L treatment in days (SD) Median time from DDLPS diagnosis to 1L treatment in days (IQR) | 624.7 (862.1) 222 (70–899) | |
| Mean time spent on 1L treatment in days (SD) Median time spent on 1L treatment in days (IQR) | 85.3 (123.2) 50 (22–113) | |
| Mean time from 1L to 2L (SD) Median time from 1L to 2L (IQR) | 156.4 (292.4) 28 (21–87) | |
| 2L treatment (N = 41) | GEM | 22 (53.7) |
| OTHER or DOXO * | 19 (46.3) | |
| Mean time spent on 2L treatment in days (SD) Median time spent on 2L treatment in days (IQR) | 84.8 (121.4) 45 (22–90) | |
| Variable | Details | No. (%) Patients at Index | 1-Year Survival % (95% CI) | 5-Year Survival % (95% CI) | 10-Year Survival % (95% CI) | Median OS Months (IQR) |
|---|---|---|---|---|---|---|
| Overall cohort | All DDLPS patients | 611 (100.0%) | 76.6 (73.2–80.0) | 52.4 (48.2–56.7) | 35.0 (29.7–40.3) | 69 (15–151) |
| Age | <65 years | 262 (42.9%) | 83.2 (78.7–87.7) | 67.3 (61.3–73.3) | 51.5 (43.5–59.4) | 122 (28–NA) |
| ≥65 years | 349 (57.1%) | 71.6 (66.9–76.4) | 41.2 (35.6–46.8) | 21.7 (15.0–28.5) | 47 (11–114) | |
| Topography | Retroperitoneum/abdomen | 370 (60.6%) | 75.7 (71.3–80.0) | 48.5 (43.0–54.1) | 31.4 (24.9–38.0) | 60 (14–151) |
| Other | 241 (39.4%) | 78.0 (72.8–83.2) | 58.3 (51.7–64.9) | 40.1 (31.4–48.9) | 101 (17–NA) | |
| Disease Stage | Stage I | 70 (11.5%) | 90.0 (83.0–97.0) | 64.2 (51.8–76.6) | * 1–5 | 85 (43–NA) |
| Stage II | 85 (13.9%) | 85.9 (78.5–93.3) | 64.3 (54.1–74.6) | 46.0 (33.7–58.4) | 103 (30–NA) | |
| Stage III | 143 (23.4%) | 78.3 (71.6–85.1) | 55.4 (45.9–64.8) | 34.5 (21.4–47.6) | 79 (19–145) | |
| Stage IV | 20 (3.3%) | 45.0 (23.2–66.8) | * 1–5 | 0.0% | 8 (6–NA) | |
| Unknown/missing | 293 (48.0%) | 72.0 (66.9–77.2) | 48.0 (41.9–54.1) | 31.3 (23.9–38.7) | 60 (12–134) | |
| Advanced DDLPS | Yes | 246 (40.3%) | 76.4 (71.1–81.7) | 43.7 (36.8–50.6) | 21.9 (14.7–29.1) | 53 (15–108) |
| No | 365 (59.7%) | 76.7 (72.4–81.0) | 57.9 (52.6–63.3) | 43.6 (36.5–50.6) | 103 (16–NA) | |
| Resected Status | Resected | 238 (39.0%) | 91.2 (87.6–94.8) | 73.2 (67.1–79.3) | 52.1 (43.1–61.1) | 131 (57–NA) |
| Not resected | 373 (61.0%) | 67.3 (62.5–72.1) | 39.1 (33.8–44.5) | 23.8 (17.5–30.0) | 38 (9–115) | |
| 1L Drug Treatment | All patients with 1L treatment (based on drug group) | 117 | 16 (6–58) | |||
| 2L Drug Treatment | All patients with 2L treatment (based on drug group) | 41 | 9 (5–16) |
| Healthcare Resource Utilization | Total No. Patients Who Used Resource | Mean HCRU Use per Person-Year (95% CI) | |
|---|---|---|---|
| All years | Year 1 ** | ||
| Specialist visits | 611 (100%) | 22.1 (20.2–23.7) | 47.6 (44.7–50.5) |
| Medical oncologist visits | 295 (48.3%) | 2.5 (1.9–3.1) | 3.6 (2.9–4.4) |
| Therapeutic radiologist visits | 506 (82.8%) | 1.8 (1.7–2.0) | 6.1 (5.6–6.7) |
| Inpatient hospitalizations | 584 (95.6%) | 0.8 (0.8–0.9) | 2.2 (2.0–2.4) |
| Length of stay (days) | 584 (95.6%) | 8.9 (7.8–10.2) | 27.1 (23.6–30.9) |
| Homecare visits | 502 (82.2%) | 19.0 (15.6–22.9) | 29.5 (25.5–33.8) |
| Cancer clinic visits | 453 (74.1%) | 5.2 (4.7–5.6) | 17.8 (16.5–19.0) |
| Advanced Status N = 246 | Non-Advanced Status N = 365 | p-Value | |||
|---|---|---|---|---|---|
| Healthcare Resource Utilization | Total No. (%) Patients Who Used HCRU | Mean HCRU Use PPY (95% CI) | Total No. (%) Patients Who Used HCRU | Mean HCRU Use PPY (95% CI) | |
| Specialist visits | 246 (100.0%) | 30.1 (27.2–33.2) | 365 (100.0%) | 17.7 (16.2–19.5) | <0.0001 |
| Medical oncologist visits | 159 (64.6%) | 5.9 (4.5–7.4) | 136 (37.3%) | 0.6 (0.4–0.9) | <0.0001 |
| Therapeutic radiologist visits | 213 (86.6%) | 2.29 (2.0–2.6) | 293 (80.3%) | 1.6 (1.4–1.8) | 0.0411 |
| Inpatient hospitalizations | * 241–245 | 1.1 (1.0–1.3) | * 339–343 | 0.7 (0.6–0.8) | 0.0002 |
| Length of stay (days) | * 241–245 | 11.3 (9.4–13.5) | * 339–343 | 7.7 (6.4–9.2) | 0.1432 |
| Homecare visits | 216 (87.8%) | 25.0 (19.1–32.1) | 286 (78.4%) | 15.8 (11.7–20.3) | 0.2018 |
| Cancer clinic visits | 218 (88.6%) | 7.4 (6.6–8.4) | 235 (64.4%) | 4.0 (3.6–4.4) | <0.0001 |
| Healthcare Resource Utilization | Total No. Patients Who Used Resource | Mean Cost per Person-Year (95% CI) | |
|---|---|---|---|
| All years | Year 1 ** | ||
| Total costs | 611 (100%) | CAD 34,448 (CAD 31,394–CAD 37,863) | CAD 86,840 (CAD 80,120–CAD 94,236) |
| Specialist visits | 611 (100%) | CAD 4895 (CAD 4564–CAD 5249) | CAD 12,566 (CAD 11,756–CAD 13,379) |
| Medical oncologist visits | 295 (48.3%) | CAD 201 (CAD 159–CAD 251) | CAD 336 (CAD 273–CAD 406) |
| Therapeutic radiologist visits | 506 (82.8%) | CAD 334 (CAD 305–CAD 365) | CAD 1137 (CAD 1053–CAD 1216) |
| Inpatient hospitalizations | 584 (95.6%) | CAD 14,522 (CAD 12,804–CAD 16,505) | CAD 43,373 (CAD 37,757–CAD 49,882) |
| Homecare visits | 502 (82.2%) | CAD 2122 (CAD 1796–CAD 2486) | CAD 3921 (CAD 3409–CAD 4492) |
| Cancer clinic visits | 453 (74.1%) | CAD 4314 (CAD 3860–CAD 4801) | CAD 12,345 (CAD 11,378–CAD 13,298) |
| Mean Cost PPY (95% CI) | Advanced Status | Unresected Status | ||||
|---|---|---|---|---|---|---|
| Yes (N = 246) | No (N = 365) | p-Value | Yes (N = 373) | No (N = 238) | p-Value | |
| Total cost | CAD 45,221 (CAD 40,113–CAD 51,133) | CAD 28,599 (CAD 24,965–CAD 32,824) | <0.05 | CAD 41,186 (CAD 36,727–CAD 46,474) | CAD 28,0701 (CAD 24,180–CAD 32,588) | <0.05 |
| Specialist visits | CAD 6260.4 (CAD 5645–CAD 6940) | CAD 4154 (CAD 3783–CAD 4560) | <0.05 | CAD 5718 (CAD 5194–CAD 6298) | CAD 4116 (CAD 3727–CAD 4543) | <0.05 |
| Medical oncologist visits | CAD 465 (CAD 357–CAD 587) | CAD 58 (CAD 40–CAD 80) | <0.05 | CAD 303 (CAD 228–CAD 393) | CAD 105 (CAD 74–CAD 141) | <0.05 |
| Therapeutic radiologist visits | CAD 447 (CAD 392–CAD 510) | CAD 273 (CAD 241–CAD 307) | <0.05 | CAD 398 (CAD 352–CAD 449) | CAD 274 (CAD 240–CAD 313) | <0.05 |
| Inpatient hospitalization | CAD 18,779 (CAD 15,601–CAD 22,804) | CAD 12,202 (CAD 10,264–CAD 14,456) | <0.05 | CAD 18,954 (CAD 16,168–CAD 22,257) | CAD 10,319 (CAD 8440–CAD 12,666) | <0.05 |
| Homecare visits | CAD 2839 (CAD 2290–CAD 3482) | CAD 1732 (CAD 1346–CAD 2165) | <0.05 | CAD 2721 (CAD 2207–CAD 3290) | CAD 1555 (CAD 1160–CAD 2009) | <0.05 |
| Cancer clinic visits | CAD 7477 (CAD 6462–CAD 8591) | CAD 2590 (CAD 2264–CAD 2947) | <0.05 | CAD 5226 (CAD 4485–CAD 6066) | CAD 3450 (CAD 2965–CAD 3982) | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seung, S.J.; Wong, A.; Milan, R.; Chandran, N.; Razak, A.R.A. Epidemiology, Treatment Patterns, Survival, Healthcare Resource Utilization, and Costs of Dedifferentiated Liposarcoma (DDLPS) in Canada: A Retrospective Cohort Study Using Administrative Databases in Ontario. Curr. Oncol. 2025, 32, 273. https://doi.org/10.3390/curroncol32050273
Seung SJ, Wong A, Milan R, Chandran N, Razak ARA. Epidemiology, Treatment Patterns, Survival, Healthcare Resource Utilization, and Costs of Dedifferentiated Liposarcoma (DDLPS) in Canada: A Retrospective Cohort Study Using Administrative Databases in Ontario. Current Oncology. 2025; 32(5):273. https://doi.org/10.3390/curroncol32050273
Chicago/Turabian StyleSeung, Soo Jin, Anisia Wong, Raymond Milan, Nisha Chandran, and Albiruni R. Abdul Razak. 2025. "Epidemiology, Treatment Patterns, Survival, Healthcare Resource Utilization, and Costs of Dedifferentiated Liposarcoma (DDLPS) in Canada: A Retrospective Cohort Study Using Administrative Databases in Ontario" Current Oncology 32, no. 5: 273. https://doi.org/10.3390/curroncol32050273
APA StyleSeung, S. J., Wong, A., Milan, R., Chandran, N., & Razak, A. R. A. (2025). Epidemiology, Treatment Patterns, Survival, Healthcare Resource Utilization, and Costs of Dedifferentiated Liposarcoma (DDLPS) in Canada: A Retrospective Cohort Study Using Administrative Databases in Ontario. Current Oncology, 32(5), 273. https://doi.org/10.3390/curroncol32050273