A Preliminary Analysis of Circulating Tumor Microemboli from Breast Cancer Patients during Follow-Up Visits



Abstract
1. Introduction
2. Materials and Methods
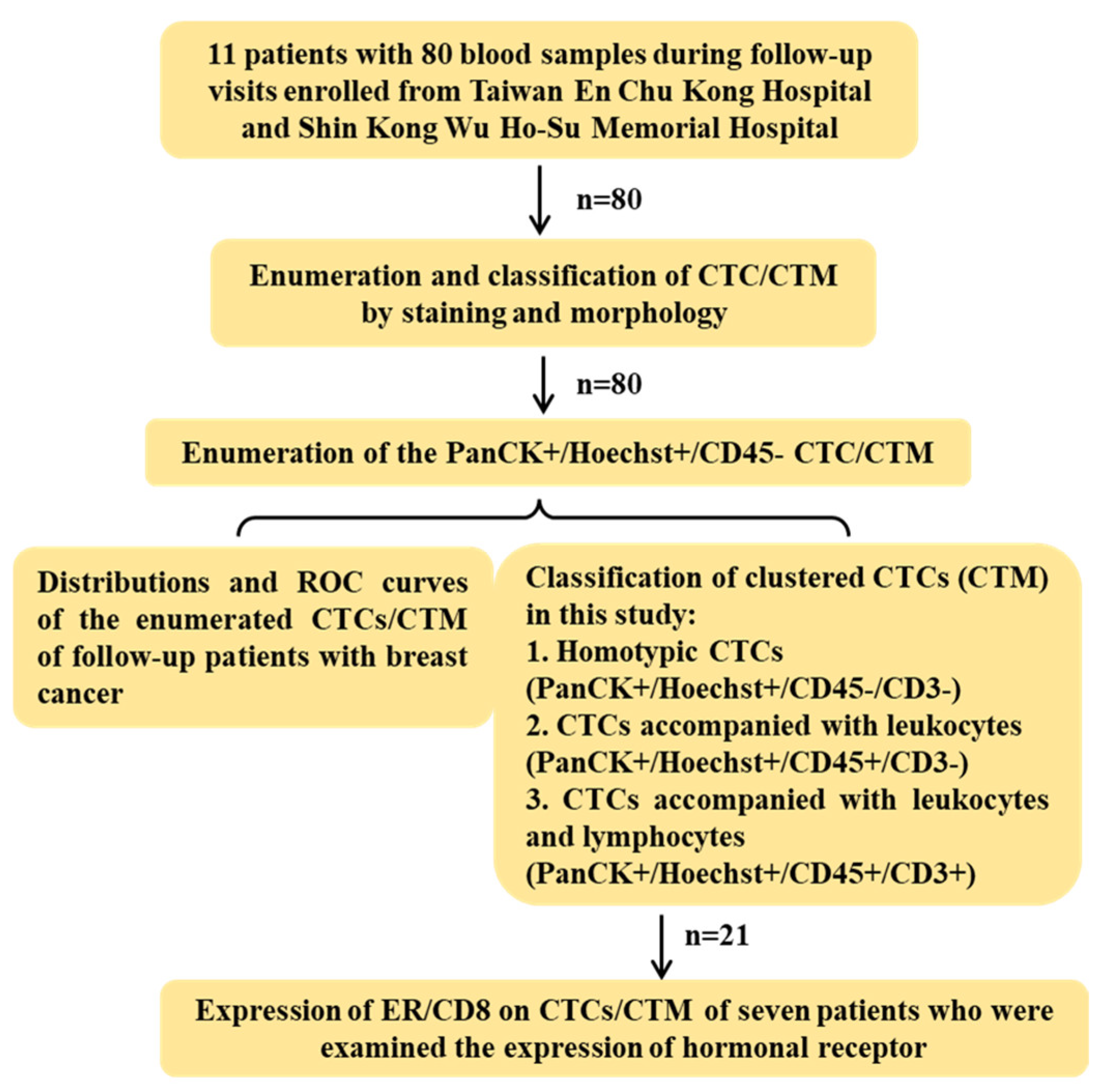
2.1. Enrollment of Clinical Patients
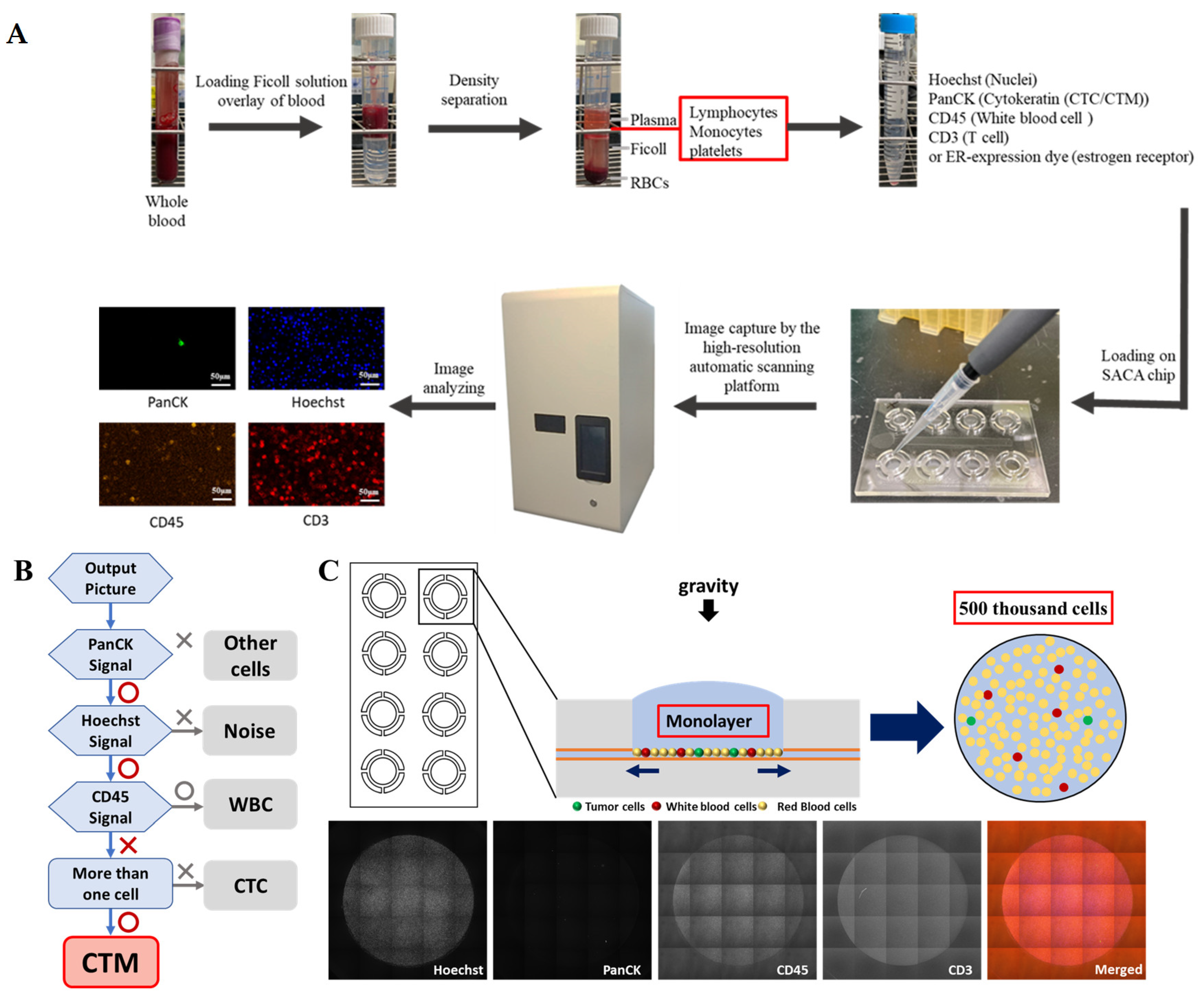
2.2. Image-Based CTC/CTM Detection
2.2.1. Plasma Preparation and Cell Enrichment
2.2.2. Immunofluorescent Staining
2.2.3. CTC/CTM Detection and Enumeration
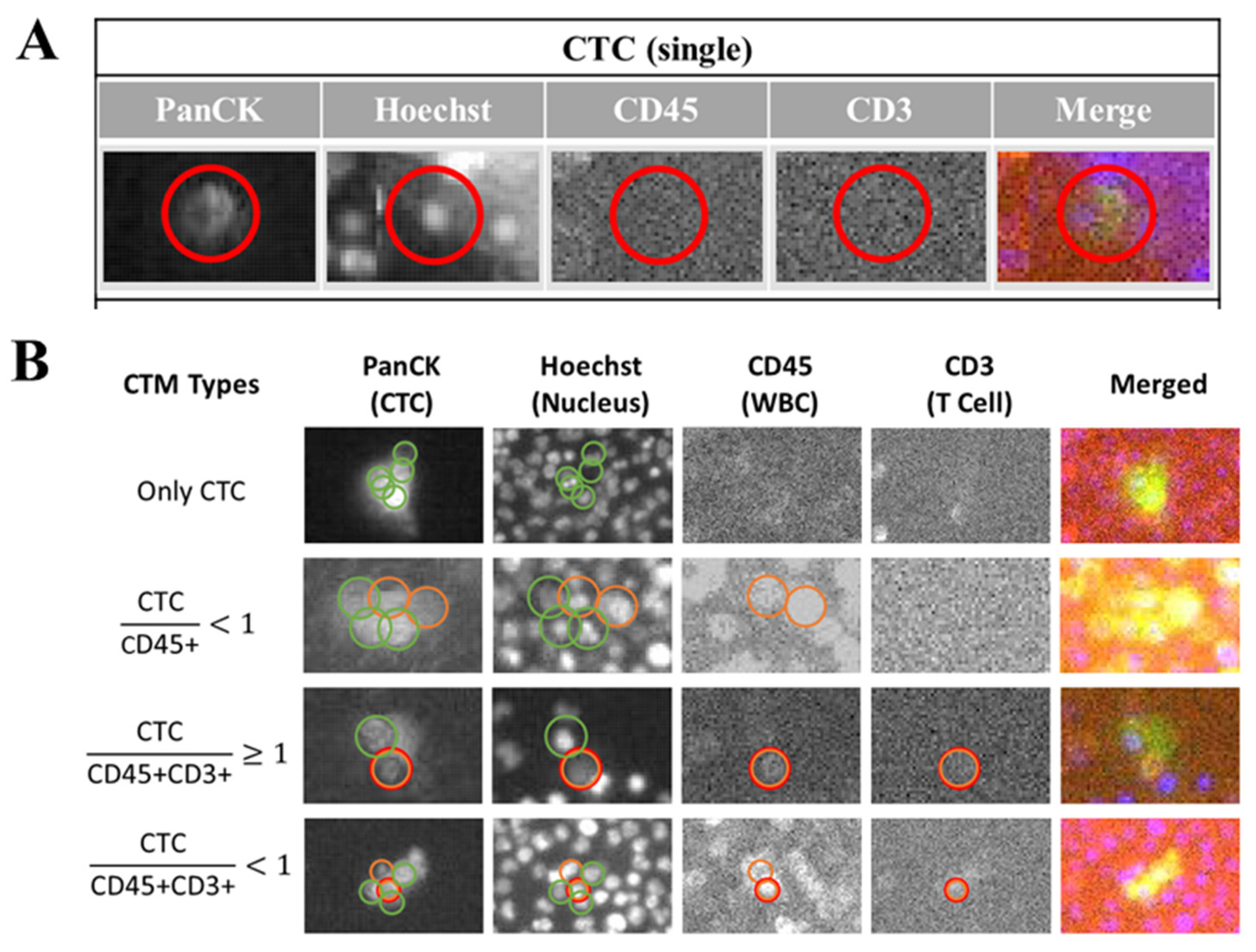
2.2.4. Identification of the Subtypes of CTM with Potential Immune Microenvironment
2.3. Statistical Analysis
3. Results
3.1. The Design of This Study
3.2. The Demography of Patients with Breast Cancer Enrolled in This Study
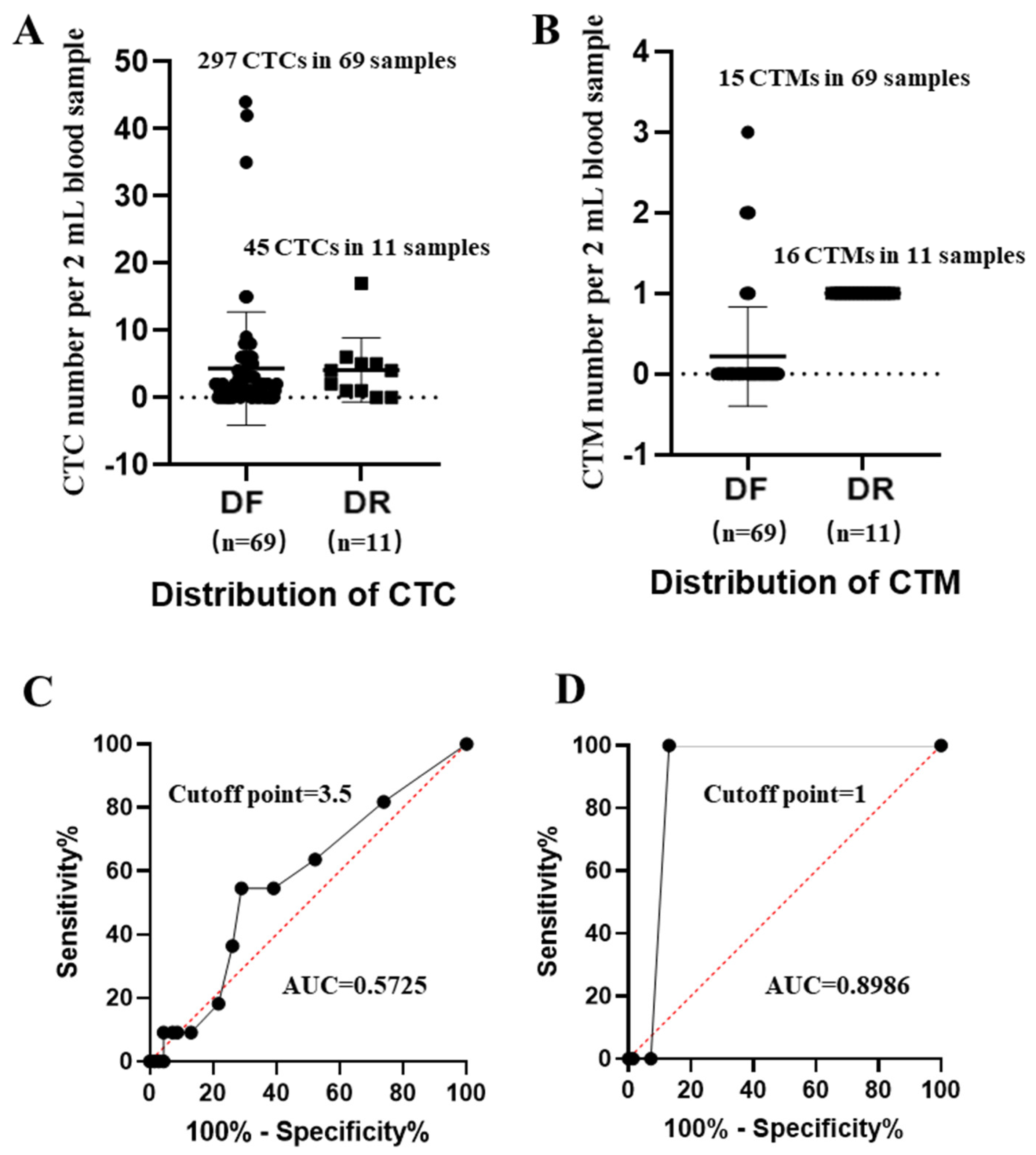
3.3. Distribution and the Receiver-Operating Characteristic (ROC) Curves of CTC/CTM from Patients with Breast Cancer
3.4. Characterization of CTM Subtypes
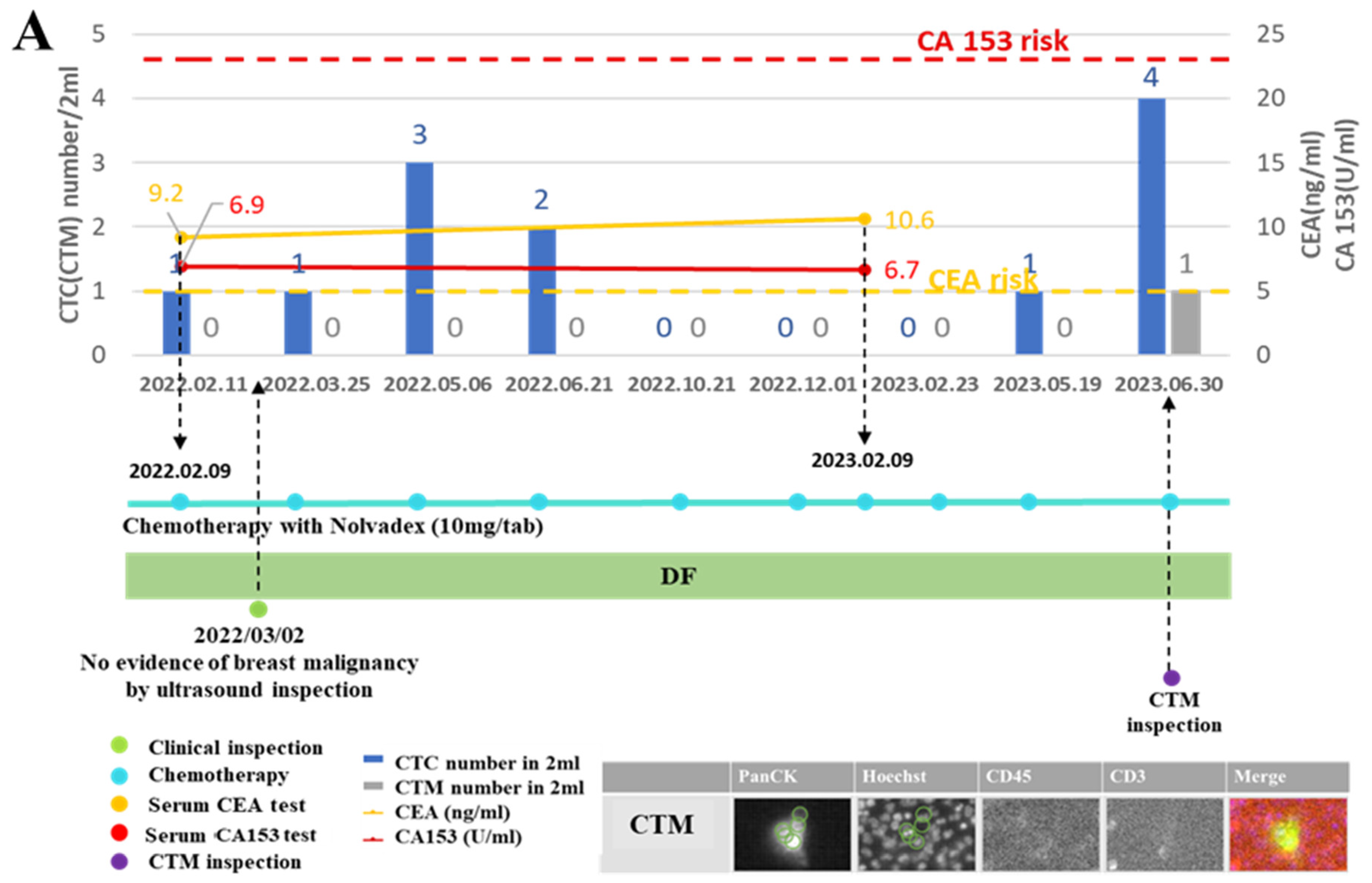
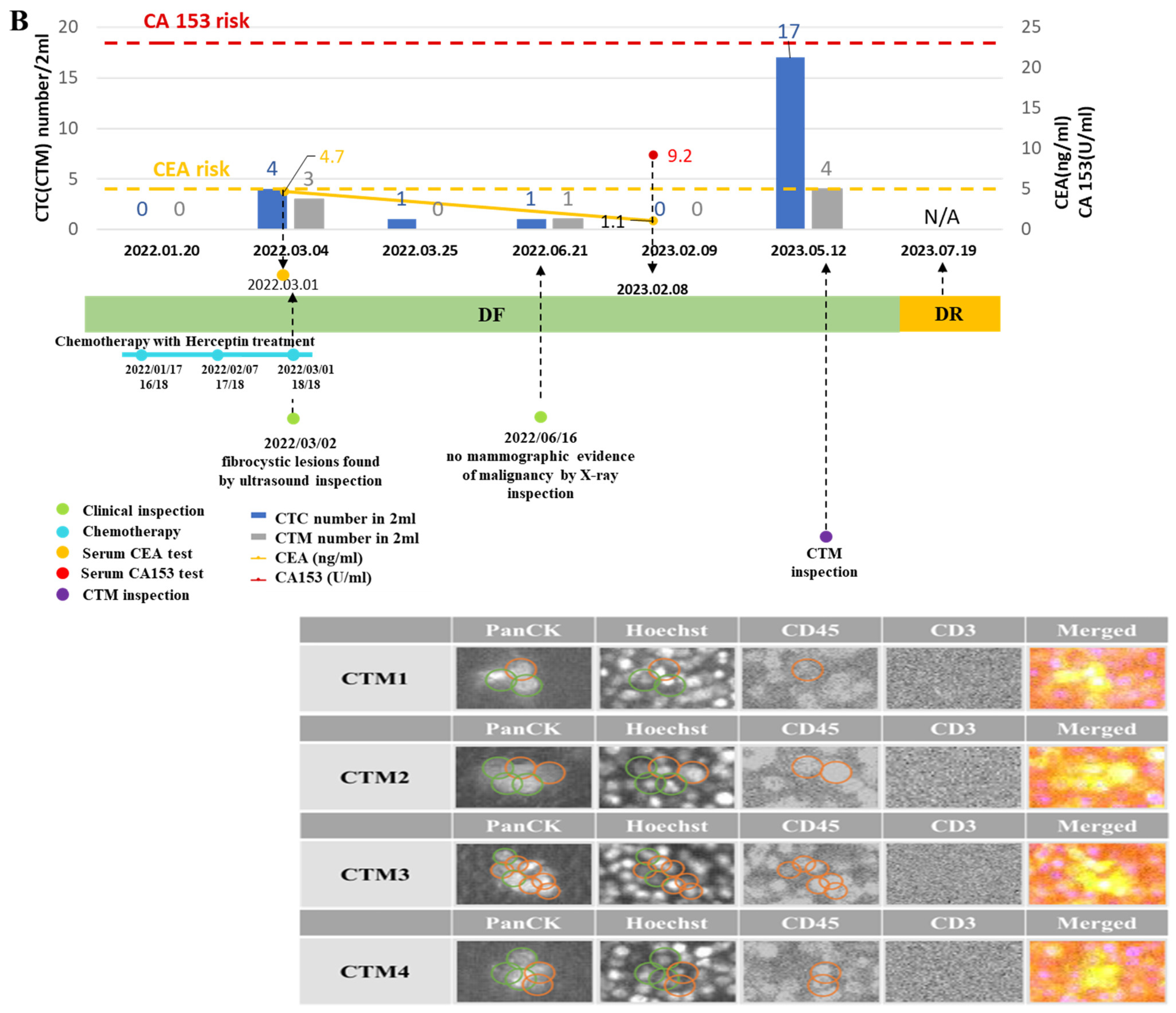
3.5. Patient Management by Monitoring Liquid Biopsy Biomarkers CTC/CTM
3.6. ER Expression in CTC/CTM of Breast Cancer Patients with Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sun, Y.-S.; Zhao, Z.; Yang, Z.-N.; Xu, F.; Lu, H.-J.; Zhu, Z.-Y.; Shi, W.; Jiang, J.; Yao, P.-P.; Zhu, H.-P. Risk factors and preventions of breast cancer. Int. J. Biol. Sci. 2017, 13, 1387. [Google Scholar] [CrossRef] [PubMed]
- Courtney, D.; Davey, M.G.; Moloney, B.M.; Barry, M.K.; Sweeney, K.; McLaughlin, R.P.; Malone, C.M.; Lowery, A.J.; Kerin, M.J. Breast cancer recurrence: Factors impacting occurrence and survival. Ir. J. Med. Sci. (1971-) 2022, 191, 2501–2510. [Google Scholar] [CrossRef] [PubMed]
- Debien, V.; De Caluwé, A.; Wang, X.; Piccart-Gebhart, M.; Tuohy, V.K.; Romano, E.; Buisseret, L. Immunotherapy in breast cancer: An overview of current strategies and perspectives. NPJ Breast Cancer 2023, 9, 7. [Google Scholar] [CrossRef]
- Farkona, S.; Diamandis, E.P.; Blasutig, I.M. Cancer immunotherapy: The beginning of the end of cancer? BMC Med. 2016, 14, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Mohme, M.; Riethdorf, S.; Pantel, K. Circulating and disseminated tumour cells—Mechanisms of immune surveillance and escape. Nat. Rev. Clin. Oncol. 2017, 14, 155–167. [Google Scholar] [CrossRef]
- Nathanson, S.D.; Detmar, M.; Padera, T.P.; Yates, L.R.; Welch, D.R.; Beadnell, T.C.; Scheid, A.D.; Wrenn, E.D.; Cheung, K. Mechanisms of breast cancer metastasis. Clin. Exp. Metastasis 2022, 39, 117–137. [Google Scholar] [CrossRef]
- Leong, S.P.; Naxerova, K.; Keller, L.; Pantel, K.; Witte, M. Molecular mechanisms of cancer metastasis via the lymphatic versus the blood vessels. Clin. Exp. Metastasis 2022, 39, 159–179. [Google Scholar] [CrossRef]
- Ring, A.; Nguyen-Sträuli, B.D.; Wicki, A.; Aceto, N. Biology, vulnerabilities and clinical applications of circulating tumour cells. Nat. Rev. Cancer 2023, 23, 95–111. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Zhong, Z.; Tan, H.-Y.; Wang, N.; Feng, Y. The Significance of circulating tumor cells in patients with hepatocellular carcinoma: Real-time monitoring and moving targets for cancer therapy. Cancers 2020, 12, 1734. [Google Scholar] [CrossRef]
- Nguyen, T.N.A.; Huang, P.-S.; Chu, P.-Y.; Hsieh, C.-H.; Wu, M.-H. Recent progress in enhanced cancer diagnosis, prognosis, and monitoring using a combined analysis of the number of circulating tumor cells (CTCs) and other clinical parameters. Cancers 2023, 15, 5372. [Google Scholar] [CrossRef]
- Lin, D.; Shen, L.; Luo, M.; Zhang, K.; Li, J.; Yang, Q.; Zhu, F.; Zhou, D.; Zheng, S.; Chen, Y.; et al. Circulating tumor cells: Biology and clinical significance. Signal Transduct. Target. Ther. 2021, 6, 404. [Google Scholar] [CrossRef] [PubMed]
- Kahounová, Z.; Pícková, M.; Drápela, S.; Bouchal, J.; Szczyrbová, E.; Navrátil, J.; Souček, K. Circulating tumor cell-derived preclinical models: Current status and future perspectives. Cell Death Dis. 2023, 14, 530. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Chang, E.S.; Kim, J.-Y.; Chelakkot, C.; Sung, M.; Song, J.-Y.; Jung, K.; Lee, J.H.; Choi, J.Y.; Kim, N.Y. c-MET-positive circulating tumor cells and cell-free DNA as independent prognostic factors in hormone receptor-positive/HER2-negative metastatic breast cancer. Breast Cancer Res. 2024, 26, 13. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.-J.; Shu, C.; Yang, H.-Y.; Huang, Z.; Li, Y.-N.; Tao, R.; Chen, Y.-Y.; Chen, Q.; Chen, X.-P.; Xiao, W. The presence of circulating tumor cell cluster characterizes an aggressive hepatocellular carcinoma subtype. Front. Oncol. 2021, 11, 734564. [Google Scholar] [CrossRef] [PubMed]
- Amintas, S.; Bedel, A.; Moreau-Gaudry, F.; Boutin, J.; Buscail, L.; Merlio, J.-P.; Vendrely, V.; Dabernat, S.; Buscail, E. Circulating tumor cell clusters: United we stand divided we fall. Int. J. Mol. Sci. 2020, 21, 2653. [Google Scholar] [CrossRef]
- Cohen, E.N.; Jayachandran, G.; Gao, H.; Peabody, P.; McBride, H.B.; Alvarez, F.D.; Kai, M.; Song, J.; Shen, Y.; Willey, J.S. Phenotypic plasticity in circulating tumor cells is associated with poor response to therapy in metastatic breast cancer patients. Cancers 2023, 15, 1616. [Google Scholar] [CrossRef]
- Micalizzi, D.S.; Maheswaran, S.; Haber, D.A. A conduit to metastasis: Circulating tumor cell biology. Genes Dev. 2017, 31, 1827–1840. [Google Scholar] [CrossRef]
- Yan, M.; Zheng, M.; Niu, R.; Yang, X.; Tian, S.; Fan, L.; Li, Y.; Zhang, S. Roles of tumor-associated neutrophils in tumor metastasis and its clinical applications. Front. Cell Dev. Biol. 2022, 10, 938289. [Google Scholar] [CrossRef]
- Schuster, E.; Taftaf, R.; Reduzzi, C.; Albert, M.K.; Romero-Calvo, I.; Liu, H. Better together: Circulating tumor cell clustering in metastatic cancer. Trends Cancer 2021, 7, 1020–1032. [Google Scholar] [CrossRef]
- Castro-Giner, F.; Aceto, N. Tracking cancer progression: From circulating tumor cells to metastasis. Genome Med. 2020, 12, 31. [Google Scholar] [CrossRef]
- Giuliano, M.; Shaikh, A.; Lo, H.C.; Arpino, G.; De Placido, S.; Zhang, X.H.; Cristofanilli, M.; Schiff, R.; Trivedi, M.V. Perspective on circulating tumor cell clusters: Why it takes a village to metastasize. Cancer Res. 2018, 78, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Fabisiewicz, A.; Grzybowska, E. CTC clusters in cancer progression and metastasis. Med. Oncol. 2017, 34, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Diaz, M.T.d.M.; Abdallah, E.A.; Tariki, M.S.; Braun, A.C.; Dettino, A.L.A.; Nicolau, U.R.; Alves, V.d.S.; Chinen, L.T.D. Circulating tumor cells as marker of poor prognosis in metastatic lung cancer: A pilot study. Appl. Cancer Res. 2018, 38, 8. [Google Scholar] [CrossRef]
- Lawrence, R.; Watters, M.; Davies, C.R.; Pantel, K.; Lu, Y.-J. Circulating tumour cells for early detection of clinically relevant cancer. Nat. Rev. Clin. Oncol. 2023, 20, 487–500. [Google Scholar] [CrossRef]
- Costa, C.; Muinelo-Romay, L.; Cebey-López, V.; Pereira-Veiga, T.; Martínez-Pena, I.; Abreu, M.; Abalo, A.; Lago-Lestón, R.M.; Abuín, C.; Palacios, P. Analysis of a real-world cohort of metastatic breast cancer patients shows circulating tumor cell clusters (CTC-clusters) as predictors of patient outcomes. Cancers 2020, 12, 1111. [Google Scholar] [CrossRef]
- Balakrishnan, A.; Koppaka, D.; Anand, A.; Deb, B.; Grenci, G.; Viasnoff, V.; Thompson, E.W.; Gowda, H.; Bhat, R.; Rangarajan, A. Circulating Tumor Cell cluster phenotype allows monitoring response to treatment and predicts survival. Sci. Rep. 2019, 9, 7933. [Google Scholar] [CrossRef]
- Aceto, N.; Bardia, A.; Miyamoto, D.T.; Donaldson, M.C.; Wittner, B.S.; Spencer, J.A.; Yu, M.; Pely, A.; Engstrom, A.; Zhu, H. Circulating tumor cell clusters are oligoclonal precursors of breast cancer metastasis. Cell 2014, 158, 1110–1122. [Google Scholar] [CrossRef]
- Bailey, P.C.; Martin, S.S. Insights on CTC biology and clinical impact emerging from advances in capture technology. Cells 2019, 8, 553. [Google Scholar] [CrossRef] [PubMed]
- Ju, S.; Chen, C.; Zhang, J.; Xu, L.; Zhang, X.; Li, Z.; Chen, Y.; Zhou, J.; Ji, F.; Wang, L. Detection of circulating tumor cells: Opportunities and challenges. Biomark. Res. 2022, 10, 58. [Google Scholar] [CrossRef]
- Chen, T.-J.; Wu, J.-K.; Chang, Y.-C.; Fu, C.-Y.; Wang, T.-P.; Lin, C.-Y.; Chang, H.-Y.; Chieng, C.-C.; Tzeng, C.-Y.; Tseng, F.-G. High-efficiency rare cell identification on a high-density self-assembled cell arrangement chip. Biomicrofluidics 2014, 8, 036501. [Google Scholar] [CrossRef]
- Goudar, V.S.; Yeh, P.-H.; Wu, S.-Y.; Chu, C.-H.; Lu, L.-S.; Yang, C.-H.; Chiou, T.-J.; Tseng, F.-G. Live circulating tumour cells selection on digitized self-assembled cell array (Digi-saca) chip by in-parallel/in-situ image analysis, cell capture, and cultivation. Sens. Actuators B Chem. 2020, 316, 128002. [Google Scholar] [CrossRef]
- Hao, Y.-J.; Yang, C.-Y.; Chen, M.-H.; Chang, L.-W.; Lin, C.-P.; Lo, L.-C.; Huang, S.-C.; Lyu, Y.-Y.; Jiang, J.-K.; Tseng, F.-G. Potential values of circulating microRNA-21 to predict early recurrence in patients with colorectal cancer after treatments. J. Clin. Med. 2022, 11, 2400. [Google Scholar] [CrossRef] [PubMed]
- Soda, N.; Clack, K.; Shiddiky, M.J. Recent advances in liquid biopsy technologies for cancer biomarker detection. Sens. Diagn. 2022, 1, 343–375. [Google Scholar] [CrossRef]
- Ferro, M.; La Civita, E.; Liotti, A.; Cennamo, M.; Tortora, F.; Buonerba, C.; Crocetto, F.; Lucarelli, G.; Busetto, G.M.; Del Giudice, F. Liquid biopsy biomarkers in urine: A route towards molecular diagnosis and personalized medicine of bladder cancer. J. Pers. Med. 2021, 11, 237. [Google Scholar] [CrossRef] [PubMed]
- Tamminga, M.; De Wit, S.; Hiltermann, T.J.N.; Timens, W.; Schuuring, E.; Terstappen, L.W.; Groen, H.J. Circulating tumor cells in advanced non-small cell lung cancer patients are associated with worse tumor response to checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 173. [Google Scholar] [CrossRef]
- Yan, W.-T.; Cui, X.; Chen, Q.; Li, Y.-F.; Cui, Y.-H.; Wang, Y.; Jiang, J. Circulating tumor cell status monitors the treatment responses in breast cancer patients: A meta-analysis. Sci. Rep. 2017, 7, 43464. [Google Scholar] [CrossRef]
- Cherdyntseva, N.; Litviakov, N.; Denisov, E.; Gervas, P.; Cherdyntsev, E. Circulating tumor cells in breast cancer: Functional heterogeneity, pathogenetic and clinical aspects. Exp. Oncol. 2017, 39, 2–11. [Google Scholar] [CrossRef]
- Murlidhar, V.; Reddy, R.M.; Fouladdel, S.; Zhao, L.; Ishikawa, M.K.; Grabauskiene, S.; Zhang, Z.; Lin, J.; Chang, A.C.; Carrott, P. Poor prognosis indicated by venous circulating tumor cell clusters in early-stage lung cancers. Cancer Res. 2017, 77, 5194–5206. [Google Scholar] [CrossRef]
- Habli, Z.; AlChamaa, W.; Saab, R.; Kadara, H.; Khraiche, M.L. Circulating tumor cell detection technologies and clinical utility: Challenges and opportunities. Cancers 2020, 12, 1930. [Google Scholar] [CrossRef]
- Smit, D.J.; Schneegans, S.; Pantel, K. Clinical applications of circulating tumor cells in patients with solid tumors. Clin. Exp. Metastasis 2024, 41, 403–411. [Google Scholar] [CrossRef]
- Okabe, T.; Togo, S.; Fujimoto, Y.; Watanabe, J.; Sumiyoshi, I.; Orimo, A.; Takahashi, K. Mesenchymal characteristics and predictive biomarkers on circulating tumor cells for therapeutic strategy. Cancers 2020, 12, 3588. [Google Scholar] [CrossRef]
- O’Toole, S.A.; Spillane, C.; Huang, Y.; Fitzgerald, M.C.; Ffrench, B.; Mohamed, B.; Ward, M.; Gallagher, M.; Kelly, T.; O’Brien, C. Circulating tumour cell enumeration does not correlate with Miller–Payne grade in a cohort of breast cancer patients undergoing neoadjuvant chemotherapy. Breast Cancer Res. Treat. 2020, 181, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Tu, Q.; Wu, X.; Le Rhun, E.; Blonski, M.; Wittwer, B.; Taillandier, L.; Bittencourt, M.D.C.; Faure, G.C. CellSearch® technology applied to the detection and quantification of tumor cells in CSF of patients with lung cancer leptomeningeal metastasis. Lung Cancer 2015, 90, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Ffrench, B.; Kashdan, E.; Huang, Y.; Spillane, C.; Cocchiglia, S.; Charmsaz, S.; Varešlija, D.; O’Brien, C.; Scholz, D.; Martin, C. CTC-5: A novel digital pathology approach to characterise circulating tumour cell biodiversity. Heliyon 2023, 9, e13044. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.L.; Stefansson, S.; Haudenschild, C.; Martin, S.S.; Charpentier, M.; Chumsri, S.; Cristofanilli, M.; Tang, C.M.; Alpaugh, R.K. Cytometric characterization of circulating tumor cells captured by microfiltration and their correlation to the cellsearch® CTC test. Cytom. Part A 2015, 87, 137–144. [Google Scholar] [CrossRef]
- Jansson, S.; Bendahl, P.-O.; Larsson, A.-M.; Aaltonen, K.E.; Rydén, L. Prognostic impact of circulating tumor cell apoptosis and clusters in serial blood samples from patients with metastatic breast cancer in a prospective observational cohort. BMC Cancer 2016, 16, 433. [Google Scholar] [CrossRef]
- Marrinucci, D.; Bethel, K.; Bruce, R.H.; Curry, D.N.; Hsieh, B.; Humphrey, M.; Krivacic, R.T.; Kroener, J.; Kroener, L.; Ladanyi, A. Case study of the morphologic variation of circulating tumor cells. Hum. Pathol. 2007, 38, 514–519. [Google Scholar] [CrossRef]
- Lozar, T.; Jesenko, T.; Kloboves Prevodnik, V.; Cemazar, M.; Hosta, V.; Jericevic, A.; Nolde, N.; Grasic Kuhar, C. Preclinical and clinical evaluation of magnetic-activated cell separation technology for CTC isolation in breast cancer. Front. Oncol. 2020, 10, 554554. [Google Scholar] [CrossRef] [PubMed]
- Kolostova, K.; Spicka, J.; Matkowski, R.; Bobek, V. Isolation, primary culture, morphological and molecular characterization of circulating tumor cells in gynecological cancers. Am. J. Transl. Res. 2015, 7, 1203. [Google Scholar]
- Song, Q.; Liu, H.; Wang, W.; Chen, C.; Cao, Y.; Chen, B.; Cai, B.; He, R. Carboxyl graphene modified PEDOT: PSS organic electrochemical transistor for in situ detection of cancer cell morphology. Nanoscale 2024, 16, 3631–3640. [Google Scholar] [CrossRef]
- Carneiro, A.; Piairo, P.; Matos, B.; Santos, D.A.; Palmeira, C.; Santos, L.L.; Lima, L.; Diéguez, L. Minimizing false positives for CTC identification. Anal. Chim. Acta 2024, 1288, 342165. [Google Scholar] [CrossRef] [PubMed]
- Umer, M.; Vaidyanathan, R.; Nguyen, N.-T.; Shiddiky, M.J. Circulating tumor microemboli: Progress in molecular understanding and enrichment technologies. Biotechnol. Adv. 2018, 36, 1367–1389. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Zhao, L.; Zhou, P.; Ma, H.; Huang, F.; Jin, M.; Dai, X.; Zheng, X.; Huang, S.; Zhang, T. Circulating tumor microemboli (CTM) and vimentin+ circulating tumor cells (CTCs) detected by a size-based platform predict worse prognosis in advanced colorectal cancer patients during chemotherapy. Cancer Cell Int. 2017, 17, 6. [Google Scholar] [CrossRef] [PubMed]
- Lopresti, A.; Acquaviva, C.; Boudin, L.; Finetti, P.; Garnier, S.; Aulas, A.; Liberatoscioli, M.L.; Cabaud, O.; Guille, A.; de Nonneville, A. Identification of atypical circulating tumor cells with prognostic value in metastatic breast cancer patients. Cancers 2022, 14, 932. [Google Scholar] [CrossRef] [PubMed]
- Tao, J.; Zhu, L.; Yakoub, M.; Reißfelder, C.; Loges, S.; Schölch, S. Cell–cell interactions drive metastasis of circulating tumor microemboli. Cancer Res. 2022, 82, 2661–2671. [Google Scholar] [CrossRef]
- Leone, K.; Poggiana, C.; Zamarchi, R. The interplay between circulating tumor cells and the immune system: From immune escape to cancer immunotherapy. Diagnostics 2018, 8, 59. [Google Scholar] [CrossRef]
- Duda, D.G.; Duyverman, A.M.; Kohno, M.; Snuderl, M.; Steller, E.J.; Fukumura, D.; Jain, R.K. Malignant cells facilitate lung metastasis by bringing their own soil. Proc. Natl. Acad. Sci. USA 2010, 107, 21677–21682. [Google Scholar] [CrossRef]
- Aceto, N. Bring along your friends: Homotypic and heterotypic circulating tumor cell clustering to accelerate metastasis. Biomed. J. 2020, 43, 18–23. [Google Scholar] [CrossRef]
- Herath, S.; Razavi Bazaz, S.; Monkman, J.; Ebrahimi Warkiani, M.; Richard, D.; O’Byrne, K.; Kulasinghe, A. Circulating tumor cell clusters: Insights into tumour dissemination and metastasis. Expert Rev. Mol. Diagn. 2020, 20, 1139–1147. [Google Scholar] [CrossRef]
- Ward, M.P.; Kane, L.E.; Norris, L.A.; Mohamed, B.M.; Kelly, T.; Bates, M.; Clarke, A.; Brady, N.; Martin, C.M.; Brooks, R.D. Platelets, immune cells and the coagulation cascade; friend or foe of the circulating tumour cell? Mol. Cancer 2021, 20, 59. [Google Scholar] [CrossRef]
- Wolff, A.C.; Somerfield, M.R.; Dowsett, M.; Hammond, M.E.H.; Hayes, D.F.; McShane, L.M.; Saphner, T.J.; Spears, P.A.; Allison, K.H. Human epidermal growth factor receptor 2 testing in breast cancer. Arch. Pathol. Lab. Med. 2023, 147, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Babayan, A.; Hannemann, J.; Spoetter, J.; Mueller, V.; Pantel, K.; Joosse, S.A. Heterogeneity of estrogen receptor expression in circulating tumor cells from metastatic breast cancer patients. PLoS ONE 2013, 8, e75038. [Google Scholar] [CrossRef] [PubMed]
- Ningsi, R.; Elazezy, M.; Stegat, L.; Laakmann, E.; Peine, S.; Riethdorf, S.; Müller, V.; Pantel, K.; Joosse, S.A. Detection and characterization of estrogen receptor α expression of circulating tumor cells as a prognostic marker. Cancers 2022, 14, 2621. [Google Scholar] [CrossRef] [PubMed]
- Clusan, L.; Ferrière, F.; Flouriot, G.; Pakdel, F. A basic review on estrogen receptor signaling pathways in breast cancer. Int. J. Mol. Sci. 2023, 24, 6834. [Google Scholar] [CrossRef]
- Moisand, A.; Madéry, M.; Boyer, T.; Domblides, C.; Blaye, C.; Larmonier, N. Hormone receptor signaling and breast cancer resistance to anti-tumor immunity. Int. J. Mol. Sci. 2023, 24, 15048. [Google Scholar] [CrossRef]
- Chu, H.Y.; Yang, C.Y.; Yeh, P.H.; Hsu, C.J.; Chang, L.W.; Chan, W.J.; Lin, C.P.; Lyu, Y.Y.; Wu, W.C.; Lee, C.W.; et al. Highly correlated recurrence prognosis in patients with metastatic colorectal cancer by synergistic consideration of circulating tumor cells/microemboli and tumor Markers CEA/CA19-9. Cells 2021, 10, 1149. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Age | TNM Stage | ER/PR/HER2 Expression | Ki-67 Value | Breast Cancer Diagnosed at the First Visit | Condition of Disease during Follow-Up Visits | Number of Follow-Up Visits | Hospital |
|---|---|---|---|---|---|---|---|---|
| 1 | 50 | IIA | +/+/− | 50% | Left breast cancer, invasive ductal carcinoma | disease free | 11 | En Chu Kong |
| 2 | 45 | IIA | −/−/− | 90% | Left breast cancer, malignant neoplasm of unspecified site | disease free | 7 | En Chu Kong |
| 3 | 62 | IA | +/+/− | 5% | Left breast cancer, intraductal carcinoma in situ | disease free | 9 | En Chu Kong |
| 4 | 48 | IA | +/+/− | 30% | Right breast cancer, malignant neoplasm of unspecified site | disease free | 3 | En Chu Kong |
| 5 | 47 | IIA | +/+/− | 30% | Left breast cancer, malignant neoplasm of unspecified site | disease free | 10 | En Chu Kong |
| 6 | 48 | IIA | +/+/+ | 50% | Right breast cancer, malignant neoplasm of unspecified site | disease free | 8 | En Chu Kong |
| 7 | 59 | IA | −/−/+ | 60% | Left breast cancer, invasive ductal carcinoma, positive resection margin | disease recurrence | 7 | En Chu Kong |
| 8 | 48 | IIA | +/+/+ | 80% | Left breast cancer, invasive ductal carcinoma, metastatic liver, luminal B | disease free | 6 | En Chu Kong |
| 9 | 51 | IIA | +/+/− | 20% | Right breast cancer, malignant neoplasm of unspecified site, luminal B | disease free | 7 | En Chu Kong |
| 10 | 49 | IIB | −/+/+ | 20% | Left breast cancer, malignant neoplasm of unspecified site | disease free | 8 | En Chu Kong |
| 11 | 44 | IV | −/−/− | 80% | Left breast cancer, invasive ductal carcinoma, metastatic bilateral lung | disease recurrence | 8 | Shin Kong Wu Ho-Su |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, H.-C.; Huang, H.-H.; Hao, Y.-J.; Lee, H.-L.; Wang, C.-C.; Ling, T.-Y.; Wu, J.-K.; Tseng, F.-G. A Preliminary Analysis of Circulating Tumor Microemboli from Breast Cancer Patients during Follow-Up Visits. Curr. Oncol. 2024, 31, 5677-5693. https://doi.org/10.3390/curroncol31090421
Lai H-C, Huang H-H, Hao Y-J, Lee H-L, Wang C-C, Ling T-Y, Wu J-K, Tseng F-G. A Preliminary Analysis of Circulating Tumor Microemboli from Breast Cancer Patients during Follow-Up Visits. Current Oncology. 2024; 31(9):5677-5693. https://doi.org/10.3390/curroncol31090421
Chicago/Turabian StyleLai, Hung-Chih, Hsing-Hua Huang, Yun-Jie Hao, Hsin-Ling Lee, Chiao-Chan Wang, Thai-Yen Ling, Jen-Kuei Wu, and Fan-Gang Tseng. 2024. "A Preliminary Analysis of Circulating Tumor Microemboli from Breast Cancer Patients during Follow-Up Visits" Current Oncology 31, no. 9: 5677-5693. https://doi.org/10.3390/curroncol31090421
APA StyleLai, H.-C., Huang, H.-H., Hao, Y.-J., Lee, H.-L., Wang, C.-C., Ling, T.-Y., Wu, J.-K., & Tseng, F.-G. (2024). A Preliminary Analysis of Circulating Tumor Microemboli from Breast Cancer Patients during Follow-Up Visits. Current Oncology, 31(9), 5677-5693. https://doi.org/10.3390/curroncol31090421